

Abstract
Aim:
The aim of this study is to determine the clinicopathologic trends in oral pathological biopsies in children aged 14 years and below received for histopathological diagnosis in the institution.
Materials and Methods:
The archives of the Department of Oral Pathology and Microbiology were retrospectively analyzed. Biopsy records of all oral lesions from pediatric patients, aged 0–14 years, in the files of the Department of Oral Pathology and Microbiology, A B Shetty Memorial Institute of Dental Sciences, Mangalore, DK, from 2007 to 2017 were considered. Descriptive statistical analysis and Pearson's Chi-square test using computer software were performed.
Results:
About 3,590 biopsies were received during the period of which 93 (2.6%) belonged to pediatric population. Prevalence was more in males (58%) compared to females (42%). Commonly affected age group was 10–14 years. The most common category of lesions diagnosed was cysts, and pulp pathologies were the least. The most common location was the jaws of which mandible was more common compared to maxilla followed by the lower lip and buccal mucosa. Histopathologically, radicular cysts (11%) were the most common followed by equal frequency of dentigerous cysts, mucoceles, and odontomes (9%). A statistically significant association of age and gender was seen with the category of the lesion.
Conclusion:
This study shows a blend of similarities and contradictions as compared to other similar studies, which could be attributed to geographical diversity, and a number of biopsies received each year which needs to be further explored.
Keywords: Cysts, mucocele, odontomes, oral biopsies, pediatric
Introduction
Oral and maxillofacial pathologies in pediatric population have always been an arena for major concern, and early detection and rapid treatment has been the goal for provision of better health services. Majority of literature have been published on common pathologies affecting this age group which includes caries, malocclusion, dental trauma, and periodontal disease. There are limited studies on the data available on the lesions such as jaw cysts, odontogenic tumors, benign and malignant neoplasms, and salivary gland pathologies.[1] Previous international studies have reported the frequency of such lesions in different countries, where Skinner et al. documented epidemiological information from 1525 biopsied oral lesions over a 14-year-old period in the age group of 0–19 years;[2] however, Jones and Franklin reported the highest number of lesions (4406) with the longest follow-up data (30 years) in the age group of 0–16 years.[3] In India, few studies have investigated pediatric oral lesions which include one from Salem, Tamil Nadu, where Krishnan et al. analyzed 97 cases in 0–15-year age group for 10-year period[4] and other from South Kerala by Heera et al. with 540 cases aged 0–12 years over 10-year period.[5] However, there are no studies reported to date in Karnataka, India, with regard to this matter. The present study was carried out with the aim of contributing data toward the incidence of common pediatric oral lesions in Dakshina Kannada population which could help pediatric dentists and pathologists in diagnosing and managing such lesions appropriately.
Materials and Methods
Archives of biopsy request form of pediatric patients between 0 and 14 years' age group were retrieved from the Department of Oral Pathology and Microbiology, A B Shetty Memorial Institute of Dental Sciences, Mangalore, Dakshina Kannada, during the time period from 2007 to 2017. Data regarding the age, gender, location, and provisional and histopathological diagnosis were evaluated. Biopsies were grouped under eight categories, namely jaw cysts, odontogenic tumors, nonodontogenic tumors, reactive/inflammatory, fibro-osseous, developmental, pulp pathology, and salivary gland pathology. Cases reported as normal dental follicle were discarded and not considered under pathologies. Children were categorized under three age groups, i.e. <5 years, 5–10 years, and >10 years, respectively. Data were tabulated and analyzed by descriptive statistics using the IBM, SPSS 20.0, Chicago, USA.
Results
In the study period of 10 years, 3,590 biopsies were received of which 93 (2.6%) belonged to pediatric population. Prevalence was observed more in males (54) compared to females (39) [Figure 1]. Mandible was most commonly affected site for intraosseous lesions followed by lower lip and buccal mucosa [Figure 2]. Majority of oral lesions are seen in the age group of 10–14 years and the least below 5 years [Figure 3]. The most common pathologies which were received had provisional diagnosis of odontome followed by mucoceles, dentigerous cysts, pyogenic granuloma, radicular cysts, and fibromas. Overall, histopathologically, the cysts formed majority of the cases (39%), followed by reactive/inflammatory lesions (19.4%) and nonodontogenic tumors (19.4%) equally, odontogenic tumors (14%), fibro-osseous lesions (3%), developmental disorders (3%), and pulp pathology and salivary neoplasms (2%) [Figure 4]. Periapical cysts formed majority that were diagnosed among cysts, followed by dentigerous cysts and odontogenic keratocysts (OKCs). Mucoceles were commonly diagnosed compared to pyogenic granulomas in reactive/inflammatory category while fibromas were the most common in the neoplasm category. Among odontogenic tumors, odontomes comprised majority of cases. Fibrous dysplasias and developmental disorders (2 cases) were seen in the same proportion, whereas pulp pathology and salivary gland neoplasms were least comprising 1 case each. A significant association was seen between the age and diagnosis where cysts, fibro-osseous lesions, odontogenic tumors, and pulp pathology were seen in participants in 10–14 years' age group, reactive lesions were seen maximum in 5–10 years' age group, while developmental disorders and neoplasms were more common in 0–5 years' and 10–14 years' age group, respectively [Figure 5]. The association of gender and diagnosis was also significant with cysts seen more in females and rest of the pathologies were more common in males. Nine of 93 cases had the clinical details missing as a result of which the location of the lesion could not be recorded.
Figure 1.
Pie chart showing percentage distribution of cases according to gender
Figure 2.
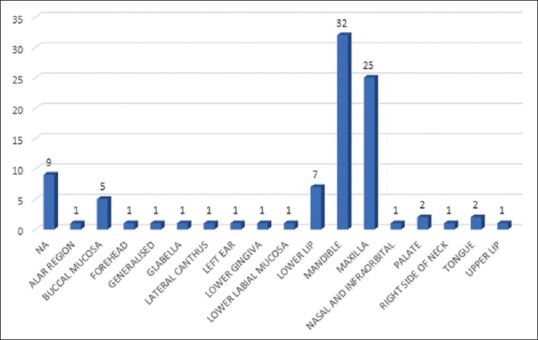
Bar chart showing location of common pediatric lesions in the oral and maxillofacial region
Figure 3.
Pie chart showing percentage distribution of cases according to age
Figure 4.
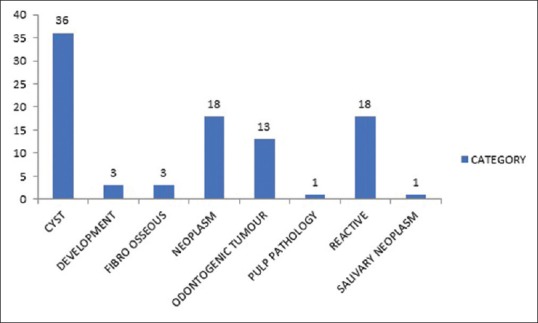
Bar chart showing prevalence of common pediatric oral lesions in different categories
Figure 5.
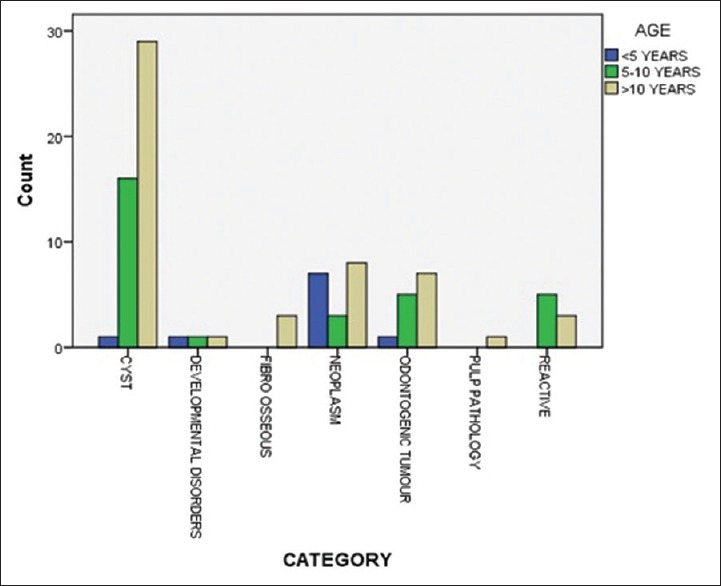
Bar chart showing age distribution among the common oral lesions in pediatric population
Discussion
Data regarding oral and maxillofacial lesions in pediatric population have been documented through many studies done in various parts of the world. Literature on both international and Indian studies are available where pediatric biopsies account for <10% of overall cases referred for histopathology services.[5] However, many other authors have found this prevalence to be between 11% and 27.2%.[6] Our study too showed a similar prevalence (2.67%) as compared to the total number of biopsies referred to the department. These pathologies have been commonly reported in the mixed dentition above 10 years of age as mentioned in previous studies.[4,7,8,9,10,11] In our study, this variable was further simplified into three categories, namely <5 years, 5–10 years, and >10 years where most of the pathologies were seen in the age group of 10–14 years (we have limited the age for pediatric age to be below 14 years). This could be partly because of the fact that there have been variations in the age ranges considered for pediatric pathologies in different studies resulting in difficulties to determine the age interval for occurrence of these pathologies among the population.[5] For the same reason, subdividing the age range further could help with this regard. Although most studies report an equal incidence of these pathologies among males and females,[3,9] the studies reported in India have shown these occurrences to be more in females.[4,5] Our study reports the prevalence of pediatric oral pathologies to be more among males (58%) as compared with females (42%). Mandible was seen to be the most commonly affected site in our study and in accordance with the previous two studies reported in South India.[4,5] Lima et al. and Mouchrek et al. reported maxilla as the most common site in their studies, whereas all other studies including the ones in India have reported mandible to be a common site. Geographical and ethnic variation could be the attributed cause for this finding.
Cystic lesions
Overall, cysts formed the majority of diagnosis (50%), which were seen in children above 10 years. This is in accordance with the studies reported by Krishnan et al. and Heera et al. where cysts formed majority of the diagnosis.[4,5] Among cysts, periapical cyst was seen in majority followed by dentigerous cyst and OKC. Predominance of inflammatory cysts as compared to developmental cysts has been reported in studies by Selvamani et al. and Krishnan et al.[4,12] Other authors like Bodner,[13] Heera et al.,[5] and Padmakumar et al.[14] reported more of dentigerous cysts to have predominated the pediatric pathologies in their studies. These findings in our study are in accordance with the studies by Selvamani et al. and Krishnan et al., which could be attributed to the high incidence of caries seen in the pediatric population. The reason for higher prevalence of developmental cysts compared to inflammatory cysts in few other studies could be due to the underreporting of periapical cysts owing to easy loss of their epithelial lining during specimen handling. OKCs are more common in the second or third decade rather than pediatric age group which could be the reason for its least occurrence in our study as well.
Reactive/inflammatory lesions
This category of pathologies accounted for 19% of total biopsies and the second largest category along with nonodontogenic neoplasms. Mucocele was the most common lesion observed, followed by pyogenic granuloma and one case each of sialocyst, peripheral giant cell granuloma, foreign body granuloma, and granulomatous lesion. The lower lip was the most common site for mucocele, and these findings were seen in majority of previous studies.[2,4,5,7,8,9,11] Gültelkin et al. found peripheral giant cell granulomas to be the most common in their study,[15] whereas Saravani et al. found pyogenic granuloma be the highest in this category.[1] In our study, the only other finding that was different was that this category of lesions was commonly seen in the 5–10 years' age group. An extensive study on oral mucoceles was done by Harrison JD in 1975 where he found that majority of mucoceles were in the birth to 20-year category.[4] Our findings also support the above fact that mucoceles are more common in the younger age group since it lies well within the age range mentioned in the above studies (0–14 years).
Nonodontogenic neoplasms
This group of lesions included only the benign epithelial and connective tissue tumors not of odontogenic origin and comprised about 19% of total cases analyzed. Fibroma was the most common in this category followed by hemangioma and one case each of osteoma, osteoblastoma, neurofibroma, fibromyxoma, melanotic neuroectodermal tumor of infancy, teratoma, pleomorphic adenoma, and eosinophilic granuloma. The risk factors associated with the biopsy of hemangioma may have resulted in less number of hemangiomas been reported histopathologically although the number might have been more clinically. The most common location was the lower lip, followed by buccal mucosa, tongue, palate, and upper lip. Similar observations were found in studies by Heera et al. and Krishnan et al. where fibroma and hemangioma were the most common nonodontogenic neoplasms, respectively.[4,5] Jones and Franklin also mentioned in their analysis that malignant tumors accounted for 1% of the total biopsies which holds true in our case as well.[5]
Odontogenic neoplasms
Odontogenic tumors comprised about 14% of pediatric pathologies of which the most common lesion in our study was odontoma with only one case each of ameloblastoma, adenomatoid odontogenic tumor, and odontogenic fibroma [Figure 2 and Table 1]. This observation was common with most of the international studies[1,2,6,7,8,16,17,18] and studies within India,[5] where odontomas have been majorly reported in the odontogenic category which may be due to the fact that odontomas are routinely encountered during radiographic examinations and might be a reason for more number of these pathologies being surgically excised and reported. Krishnan et al.[4] and Dhanuthai et al.,[18] however, reported ameloblastoma to be the most common in this category. Maxilla was the common location for the odontomas in our study. This location was also seen to be common in the studies reported by Skinner et al. and Heera et al [Figure 4 and Table 2].[2,5] The important fact drawn from this observation is that radiographic reports may play a vital role in the diagnosis of odontomas preoperatively, resulting in high number of odontomes being submitted for histopathological examination.
Table 1.
Percentage distribution of biopsies according to different locations
| Location | n (%) |
|---|---|
| No clinical details available | 9 (9.7) |
| Alar region | 1 (1.1) |
| Buccal mucosa | 5 (5.4) |
| Forehead | 1 (1.1) |
| Generalized | 1 (1.1) |
| Glabella | 1 (1.1) |
| Lateral canthus | 1 (1.1) |
| Left ear | 1 (1.1) |
| Lower gingiva | 1 (1.1) |
| Lower labial mucosa | 1 (1.1) |
| Lower lip | 7 (7.5) |
| Mandible | 32 (34.4) |
| Maxilla | 25 (26.9) |
| Nasal and infraorbital | 1 (1.1) |
| Palate | 2 (2.2) |
| Right side of neck | 1 (1.1) |
| Tongue | 2 (2.2) |
| Upper lip | 1 (1.1) |
| Total | 93 (100) |
Table 2.
Percentage distribution of biopsies according to various categories
| Category | n (%) |
|---|---|
| Cyst | 36 (38.7) |
| Developmental disorders | 3 (3.2) |
| Fibro-osseous | 3 (3.2) |
| Neoplasm | 18 (19.4) |
| Odontogenic tumor | 13 (14) |
| Pulp pathology | 1 (1.1) |
| Reactive | 18 (19.4) |
| Salivary neoplasm | 1 (1.1) |
| Total | 93 (100) |
Fibro-osseous lesions and developmental disorders
These both minor categories accounted for totally 6% of pathologies with majority of fibrous dysplasias and one of the juvenile ossifying fibromas. Among the developmental disorders, one case each of natal teeth, dentinogenesis imperfecta, and vascular malformation were reported. These findings have also been noted by Skinner et al. and Heera et al.[2,5] Since these lesions are more common in the second and third decades of life and developmental anomalies are commonly encountered in permanent dentition, it could be a reason for lesser number of these lesions being observed in children below 14 years of age.
Pulpal pathology
The only pulpal pathology seen in our case was pulp polyp which has also been reported by Heera et al. in their study.[5] The fact that pulpal pathologies have been documented as the least in our study could be because of the fact that most of the pulpal pathologies may have progressed to periapical lesion. This is highlighted by the finding of majority of periapical cysts in our study. This also could be explained by the fact that anatomy of primary teeth could help faster progression of pulp pathology into the periapex and another reason could be dental phobias in this age group resulting in delay in dental treatment.
The tissues reported as dental follicle were not considered in our study as they were seen to be devoid of any specific pathology. The other important point that needs to be considered is the classification of the pathologies into respective categories which could be subjective. Mucoceles have been categorized into cysts in some studies, whereas various other authors have classified them into reactive lesions.[11,14] Similarly, ossifying fibromas have been grouped into bone pathologies in some studies and benign odontogenic neoplasms in others.[5,8] Such variations with a combination of missing/incomplete clinical details may have affected the prevalence of common lesions in pediatric age group.
Conclusion
The geographical and racial variations seen in the population worldwide could greatly influence the prevalence of various pediatric pathologies. Most of the data available on pediatric pathologies in India have been based on South Indian population. Our study thus aims to further contribute to these data which could help researchers, surgeons, pedodontists, and general dentists adopt better diagnostic and treatment strategies for common oral lesions to seek better health care.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to extend my sincere thanks to our postgraduate Dr. Varshini M who helped us with the data compilation from the archives and Dr. Srikant N who helped with the statistical analysis and graphical presentation of data in this study.
References
- 1.Saravani S, Kadeh H, Amirabadi F, Keramati N. Clinical and histopathological profiles of pediatric and adolescent oral and maxillofacial biopsies in a Persian population. Int J Pediatr. 2015;3:381–90. [Google Scholar]
- 2.Skinner RL, Davenport WD, Jr, Weir JC, Carr RF. A survey of biopsied oral lesions in pediatric dental patients. Pediatr Dent. 1986;8:163–7. [PubMed] [Google Scholar]
- 3.Jones AV, Franklin CD. An analysis of oral and maxillofacial pathology found in children over a 30-year period. Int J Paediatr Dent. 2006;16:19–30. doi: 10.1111/j.1365-263X.2006.00683.x. [DOI] [PubMed] [Google Scholar]
- 4.Krishnan R, Ramesh M, Paul G. Retrospective evaluation of pediatric oral biopsies from a dental and maxillofacial surgery centre in Salem, Tamil Nadu, India. J Clin Diagn Res. 2014;8:221–3. doi: 10.7860/JCDR/2014/6805.3930. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Heera R, Bharathan R, Padmakumar SK, Rajeev R, Sivakumar R. Oral and maxillofacial biopsy reports of children in south Kerala population: A 20-year retrospective study. Int J Sci Stud. 2016;4:104–8. [Google Scholar]
- 6.Mouchrek MM, Gonçalves LM, Bezerra-Júnior JR, Maia ED, Silva RA, Cruz MC. Oral and maxillofacial biopsied lesions in Brazilian pediatric patients: A 16-year retrospective study. Rev Odonto Cienc. 2011;26:222–6. [Google Scholar]
- 7.Lima Gda S, Fontes ST, de Araújo LM, Etges A, Tarquinio SB, Gomes AP. A survey of oral and maxillofacial biopsies in children: A singlecenter retrospective study of 20 years in Pelotas-Brazil. J Appl Oral Sci. 2008;16:397–402. doi: 10.1590/S1678-77572008000600008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lei F, Chen J, Lin L, Wang W, Huang H, Chen C, et al. Retrospective study ofbiopsied oral and maxillofacial lesions in pediatric patients from Southern Taiwan. J Dent Sci. 2014;9:351–8. [Google Scholar]
- 9.Das S, Das AK. A review of pediatric oral biopsies from a surgical pathology service in a dental school. Pediatr Dent. 1993;15:208–11. [PubMed] [Google Scholar]
- 10.Hussein AA, Darwazeh AM, Al-Jundi SH. Prevalence of oral lesions among Jordanian children. Saudi J Oral Sci. 2017;4:12–7. [Google Scholar]
- 11.Vale EB, Ramos-Perez FM, Rodrigues GL, Carvalho EJ, Castro JF, Perez DE, et al. Areview of oral biopsies in children and adolescents: A clinicopathological study of a case series. J Clin Exp Dent. 2013;5:e144–9. doi: 10.4317/jced.51122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Selvamani M, Donoghue M, Basandi PS. Analysis of 153 cases of odontogenic cysts in a South Indian sample population: A retrospective study over a decade. Braz Oral Res. 2012;26:330–4. doi: 10.1590/s1806-83242012005000007. [DOI] [PubMed] [Google Scholar]
- 13.Bodner L. Cystic lesions of the jaws in children. Int J Pediatr Otorhinolaryngol. 2002;62:25–9. doi: 10.1016/s0165-5876(01)00583-3. [DOI] [PubMed] [Google Scholar]
- 14.Padmakumar SK, Beena VT, Aloka D, Lav R, Sivakumar R. Cysts of the jaws in pediatric population: A 12-year institutional study. Oral Maxillofac Pathol J. 2015;6:532–6. [Google Scholar]
- 15.Gültelkin SE, Tokman B, Türkseven MR. A review of paediatric oral biopsies in turkey. Int Dent J. 2003;53:26–32. doi: 10.1111/j.1875-595x.2003.tb00652.x. [DOI] [PubMed] [Google Scholar]
- 16.Saxena S, Kumar S, Pundir S. Pediatric jaw tumors: Our experience. J Oral Maxillofac Pathol. 2012;16:27–30. doi: 10.4103/0973-029X.92969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Arotiba GT. A study of orofacialtumors in Nigerian children. J Oral Maxillofac Surg. 1996;54:34–8. doi: 10.1016/s0278-2391(96)90299-2. [DOI] [PubMed] [Google Scholar]
- 18.Dhanuthai K, Banrai M, Limpanaputtajak S. A retrospective study of paediatric oral lesions from Thailand. Int J Paediatr Dent. 2007;17:248–53. doi: 10.1111/j.1365-263X.2007.00828.x. [DOI] [PubMed] [Google Scholar]