

Abstract
Background: Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC) is a drug delivery technique with superior pharmacological properties for treating peritoneal metastasis (PM). Adding electrostatic loading (ePIPAC) as an adjunct to aerosol and artificial hydrostatic pressure improved tissue uptake in a preclinical model.
Methods: We report the first ePIPAC use in 3 patients with PM of hepatobiliary-pancreatic (HBP) origin. All 3 patients received concomitant palliative systemic chemotherapy that was discontinued in two patients. PIPAC with cisplatin 7.5 mg/m2 and doxorubicin 1.5 mg/m2 was applied intraperitoneally at a pressure of 12 mmHg and a temperature of 37% °C for 30 min. Additionally, a voltage 7,500–9,500 V and a current≤10 µA were applied over a stainless steel brush electrode emitting a stream of electrons.
Results: ePIPAC was technically feasible. No intraoperative complication was noted. The procedures were well tolerated with no adverse event CTCAE > 2. Patient 1 with PM of unknown origin (CUP with HBP phenotype) showed an objective histological and radiological response and survived 11 months. Patient 2 with ductal pancreatic cancer underwent secondary resection after ePIPAC with no residual PM; however, tumor recurred 5 months later. Patient 3 with adenocarcinoma of the gallbladder showed a radiological regression of liver infiltration and is alive after 22 months without histological evidence of PM.
Conclusion: ePIPAC is technically feasible, is well tolerated and can induce tumor regression of PM in HBP cancers with and without concomitant systemic chemotherapy. These preliminary results justify prospective clinical studies with ePIPAC.
Keywords: aerosol, cisplatin, doxorubicin, electrostatic precipitation, gallbaldder cancer, intraperitoneal chemotherapy, pancreatic cancer, peritoneal metastasis, PIPAC, pressure
Introduction
The metastatic seeding of tumors into the peritoneal cavity remains an unmet medical need. Prognosis is poor with limited options for an effective treatment. Treatments offered are mainly limited to palliative systemic therapy and best supportive care [1]. Although intraperitoneal chemotherapy has been shown to have pharmacological advantages in this situation, its use remains limited [2]. Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC) is an innovative drug delivery system developed for treating PM [3]. PIPAC takes advantage of the physical properties of the combination of gas and pressure in order to overcome pharmacological limitations of intraperitoneal chemotherapy such as limited exposure of peritoneal surfaces and poor drug diffusion into the tumor nodes [4]. There is substantial evidence in vitro [5], in vivo [6], ex vivo [7] and in human patients [8] that PIPAC has superior pharmacological properties compared to fluid-based intraperitoneal application of chemotherapy. Since the therapeutic ratio between local and systemic drug concentration is increased by PIPAC, enhanced local efficacy together with low systemic toxicity was expected and has been confirmed clinically [9]. Retrospective analysis of first patient cohorts in ovarian [10], gastric [11] and colorectal [12] cancer have shown encouraging results of PIPAC in the palliative situation, with relatively high efficacy and favorable safety profiles. A first prospective phase-2 trial with low-dose doxorubicin and cisplatin in recurrent, platinum-resistant ovarian cancer applied as PIPAC has confirmed these results with a clinical benefit rate (CBR) of 62% and an objective histological regression rate of 76%, coupled with a low incidence of severe adverse events (15% CTCAE grade 3, no CTCAE grade 4 and 5) [13]. Further prospective clinical trials are ongoing to evaluate the efficacy and the safety of PIPAC with various drugs and in various indications [14–16].
In theory, adding electrostatic loading of the aerosolized particles as an adjunct to PIPAC should further improve the pharmacological properties of PIPAC, since it should induce precipitation of the aerosolized drug, enhancing thereby the ratio between the dose applied and the dose in the target tissue. This enhanced PIPAC procedure, so-called electrostatic precipitation PIPAC (ePIPAC), might allow further dose reduction – or dose escalation in tumor nodes. A dedicated medical application of electrostatic precipitation has recently been developed for clearing surgical smoke from the operative field of view during laparoscopy. The performance and safety of this approach has been demonstrated in bench studies, preclinical, and clinical studies including a randomized clinical trial with 30 patients undergoing laparoscopic cholecystectomy [17]. In particular, no adverse events such as cardiac arrhythmia, modification of ECG, bowel perforations, or skin burning were reported.
The practical feasibility of electrostatic precipitation Pressurized IntraPeritoneal Aerosol Chemotherapy (ePIPAC) was recently evaluated in the preclinical model [18]. ePIPAC was technically feasible in all animals. The aerosol was cleared completely from the visual field within 15 s in the ePIPAC group. The peritoneal surface was homogeneously stained. Toluidine blue in the peritoneal fluid was greatly reduced after ePIPAC but remained present after PIPAC. After 30 min 1.5% remaining DT01 was measured in samples of ePIPAC treated peritoneal fluid vs. 15% in PIPAC animals (p=0.01). Tissue concentration was increased after ePIPAC vs. PIPAC (p=0.06). Thus, ePIPAC met the theoretical expectations by improving tissue drug delivery.
We decided to investigate the feasibility of adding electrostatic precipitation to our usual PIPAC protocol for treating human patients. For this purpose, we selected patients with aggressive, lethal disease without curative option and decided to first treat peritoneal metastasis of hepatobiliary-pancreatic (HBP) origin. We now report on the first observations collected with ePIPAC in these patients, in particular concerning feasibility and tolerability of the procedure, and provide first preliminary efficacy data.
Patients and methods
Study design
Observational feasibility study on the 3 first patients treated with ePIPAC.
Regulatory framework
PIPAC and ePIPAC were performed as off-label use of approved drugs (cisplatin and doxorubicin), using CE-certified medical devices. All patients had a severe, lethal disease without curative option. Data collection into a prospective PIPAC registry has been authorized by the Institutional Review Board of the Ruhr-University Bochum (Reg. 15–5280). All procedures were performed according to the principles of the Helsinki declaration. All patients were extensively informed and signed a consent form for each procedure.
Patient selection
Indication to (e)PIPAC therapy was decided on an individual basis by the interdisciplinary tumor conference of our institution. Three patients with histologically verified PM of hepatobiliary-pancreatic (HBP) origin were selected. All patients received or had received systemic palliative chemotherapy. No patient had extraperitoneal disease. Cytoreductive surgery and Hyperthermic IntraPEritoneal Chemotherapy (HIPEC) was not indicated in these patients.
Surgical procedure
All interventions were performed under general anesthesia with a single-shot of ceftriaxone 1.5 g iv administered 30 min prior to surgery. A venous thromboembolism prophylaxis was given the night before surgery using certoparin 3,000 IE 1 × s.c. The technical setup for the ePIPAC procedure is shown in Figure 1 After insufflation of a 12 mmHg CO2 pneumoperitoneum with open access or with Veres needle, two balloon safety trocars (5 and 12 mm, Applied Medical, Düsseldorf, Germany) were inserted into the abdominal wall. Extent of peritoneal carcinomatosis (PCI score) was determined based on lesion size and distribution [19]. Peritoneal biopsies were taken in all 4 quadrants for histological examination, and a local partial peritonectomy of several square centimeters was performed routinely to improve accuracy of anatomopathology. An 9-mm aerosolizer (Capnopen®, Capnomed, Villigendorf, Germany) was connected to an intravenous high-pressure injector (Arterion Mark 7, Medrad, Bayer,, Germany) and inserted into the abdomen through an access port. A IonWand® brush electrode (Alesi Surgical Ltd, Cardiff, UK) was inserted through the abdominal wall. Following safety measures were taken to exclude any exposure of the operating team [20, 21]. First, tightness of the abdomen was documented via a zero-flow of CO2. Second, the procedure was performed in an operating room equipped with laminar air flow. Third, chemotherapy injection was remote-controlled and nobody remained in the operating room during the application. A pressurized aerosol containing doxorubicin at a dose of 1.5 mg/m2 body surface in a 50 mL NaCl 0.9% solution followed by cisplatin at a dose of 7.5 mg/m2 body surface in a 150 mL NaCl 0.9% solution was applied via aerosolizer and injector. Flow rate was 30 mL/min and maximal upstream pressure was 200 psi. Electrostatic loading was activated at this timepoint. The charged therapeutic capnoperitoneum was then maintained for 30 min at 37%°C. Then, the chemotherapy aerosol was exsufflated via a closed line over two sequential microparticle filters into the airwaste system of the hospital. Finally, trocars were retracted and laparoscopy ended. No drainage of the abdomen was applied. When possible, the ePIPAC procedure was repeated after 6 weeks.
Figure 1:
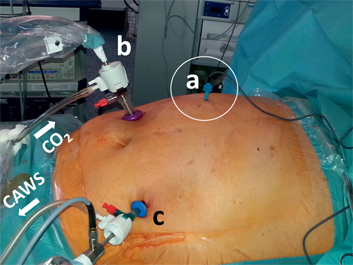
Technical setup for ePIPAC.
The abdomen is insufflated as usual with CO2 at 12 mmHg and 37%°C. Two trocars and a brush electrode (a) are inserted into the abdomen. The aerosolizing device (b) is inserted into a trocar under videoscopic control (c) and the pressurized therapeutic aerosol installed. After electrostatic loading and precipitation, the abdomen is exsufflated over a closed aerosol waste system (CAWS).
Electrostatic precipitation
The system (Ultravision™, Alesi Surgical Ltd, Cardiff, UK) integrates the following components: a generator unit (Voltage 7,500–9,500 V, current ≤ 10 µA), and an active cable terminating in an atraumatic stainless steel brush electrode (Ionwand™) that is responsible for the electrostatic charging of aerosol particles, and a return electrode with a solid patient return plate. The IonwandTM emits a stream of electrons, resulting in the creation of negative gas ions. The gas ions collide with particulate matter passing on the negative charge. The return electrode confers a weak positive charge on the subject which results in the electrostatic attraction of the negatively charged aerosol particles to the tissue surfaces of the contained space, i. e. the peritoneum.
Patient follow-up
Survival follow-up data were regularly updated by telephone calls. Patients were followed up until 16 February 2016 or until death. Clinical, laboratory and anatomopathology data were documented according to GCP rules, including electronic microfilm archiving and digital video recording of the surgical procedures. Tumor response was graded by independent pathologists considering fibrosis overgrowth and proportion of vital tumor cells, as described elsewhere [22]. Adverse events were classified according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0 [23].
Statistics
This is an exploratory report on individual cases, with the aim of generating preliminary data for designing later studies. Only descriptive statistics are provided. No sample size was calculated. No comparative statistics nor survival statistics were calculated.
Results
Between 29 July 2014 and 6 October 2015, ten PIPAC and four ePIPAC procedures were performed in 3 patients. Patient characteristics are summarized in Table 1.
Table 1:
Patients characteristics.
| Patient | Age, years | Sex | Origin of peritoneal metastasis | PCI | Number of (e)PIPAC | Systemic chemotherapy | Radiological response (RECIST) | Histological response of PM (PRGS) | Adverse events (CTCAE) | Survival (months) from diagnosis | Survival (months) from (e)PIPAC #1 |
| 1 AL | 72 | M | CUP (HBP) | 17 | 2 PIPAC 2 ePIPAC | 3 cycles Cisplatin + Gemcitabin weekly, discontinued | Partial response(PM) | PRGS 2 Major regression | 2 (AP) | 11,1 | 9,1 |
| 2 BC | 68 | W | Pancreas | 3 | 2 PIPAC 1 ePIPAC | 7 cycles Nab-paclitaxel + Gemcitabin, discontinued | N/A (PM); Stable disease (primary) | PRGS 1 Complete regression | 1 (AP) | 11,7 | 8,6 |
| 3 ER | 59 | W | Gallbladder | 3 | 6 PIPAC 1 ePIPAC | 13 cycles Cisplatin + Gemcitabin | N/A (PM); Partial response (primary) | PRGS 1 Complete regression | 1 (AP) | >22 (alive) | >18 (alive) |
PM, peritoneal metastasis; PCI, peritoneal carcinomatosis index (Sugarbaker); CUP, cancer unknown origin; HBP, hepatobiliarypancreatic; RECIST, Response Evaluation Criteria In Solid Tumors Version 1.1; PRGS, Peritoneal Regression Grading Score; CTCAE, Common Terminology Criteria for Adverse Events v. 4.03; AP, abdominal pain; (e)PIPAC, (electrostatic precipitation) PIPAC (Pressurized IntraPeritoneal Aerosol Chemotherapy).
Patient 1
This 72-years old male patient was diagnosed during laparoscopy with PM from an adenocarcinoma (G2) of unknown origin (CUP). Tumor cells were positive for CK7 and negative for CK20, CDX2 and TTF1, suggesting an origin in the upper gastrointestinal tract. CT showed PM but no primary tumor. Upper GI endoscopy showed no pathology so that HBP origin was assumed. The patient received 3 cycles of intravenous palliative chemotherapy with cisplatin and gemcitabine. This therapy was discontinued because of poor tolerability. Subsequently, 2 months after the initial diagnosis, the first low-dose PIPAC with cisplatin 7.5 mg/m2 and doxorubicin 1.5 mg/m2 was applied. Karnofsky Index was 80%, Peritoneal Carcinomatosis Index (PCI) was 17 with a diffuse small bowel involvement. No ascites was documented. Biopsies showed high-grade regressive changes after systemic chemotherapy. The first ePIPAC was applied 6 weeks later, Karnofsky was 80%, intraoperatively PCI was 13, 50 mL ascites fluid was aspirated and multiple peritoneal biopsies showed no tumor cells (complete intraperitoneal regression). A third PIPAC was applied 6 weeks later, patient had improved quality of life with a Karnofsky of 90%. PCI was 13, ascites volume was 100 mL and multiple biopsies showed moderate regressive changes. CT-scan showed objective regression according to RECIST criteria (Figure 2). Six weeks later, the KI was 90% and a second ePIPAC was administered. The PCI was 16 and histology still showed moderate regressive changes. The patient was hospitalized 2 months later with an obstructive icterus and a squirrhous stenosis of the proximal duodenum preventing stent placement into the bile duct. General condition was so reduced that the patient was referred to a palliative care unit. He died 3 months later or 11 months after the histological diagnosis of PM (12.5 months after the radiological diagnosis).
Figure 2:
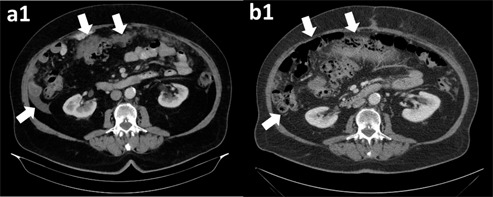
72-years old male patient with peritoneal metastasis (PM) from an adenocarcinoma (G2) unknown origin (CUP) with hepatobiliarypancreatic (HBP) immunohistochemical profile.
CT scan shows an objective regression of PM (arrows) after systemic chemotherapy, 2 conventional PIPAC and 1 ePIPAC. Histology showed major tumor regression (PRGS 2).
Patient 2
A 68-years old women was diagnosed with a 5 mm mass of the pancreatic tail (5 mm diameter mass in the CT-scan). The KI was 90%. Staging laparoscopy showed synchronous PM and therefore resection was performed. Peritoneal biopsies confirmed a ductal adenocarcinoma of the pancreas, moderately differentiated (G2). The patient received thereafter one cycle of palliative systemic chemotherapy with oxaliplatin and gemcitabine, followed by 6 cycles INN-paclitaxel and gemcitabine. Three months after diagnosis, the first ePIPAC with low-dose cisplatin (7.5 mg/m2 body surface) and doxorubicin (1.5 mg/m2 body surface) was applied. PCI was 3 and no tumor cells were found in multiple peritoneal biopsies. The patient recovered well and was scheduled 2 weeks later for a curative pancreatic tail resection and splenectomy. Histology showed a ypT3 pN1 (2/15), M0, L0, V0, Pn0 tumor, UICC-Stage IIB, R0-resection. The patient developed postoperatively a systemic inflammatory response syndrome (SIRS) and a bilateral pneumonia and could leave the hospital on postoperative day (POD) 12. Five months later, a second-look laparoscopy was scheduled, which showed again PM with a PCI of 16 and 50 mL of ascites. The second low-dose PIPAC with cisplatin and doxorubicin was applied. One month later, the patient was admitted again to the hospital because of bilateral hydronephrosis that was drained endoscopically with ureteral double-J stents. The third PIPAC was administered showing 800 mL ascites and a PCI of 23. Peritoneal biopsies were tumor-free with the exception of one centimetric piece of peritonectomy showing tumor with moderate regressive changes. Two weeks later, the patient was admitted again for symptomatic ascites drainage. She died 12 months after diagnosis.
Patient 3
The third patient was a 59-years old women with adenocarcinoma of the gallbladder diagnosed incidentally during cholecystectomy. A second-look laparotomy was scheduled 2 months later in order to complete the resection but PM was diagnosed intraoperatively and confirmed by histologyten so that no resection was performed. CT scan showed an infiltration of the liver in the hilus region, but the patient developed no icterus. She was treated with 2 cycles of systemic palliative chemotherapy with cisplatin and gemcitabine. Two months after the diagnosis of PM, she was treated with the first low-dose PIPAC with cisplatin and doxorubicin. Intraoperatively, the PCI was < 3, no ascites was documented and multiple peritoneal biopsies were tumor-free. The KI was 90%. The patient received then combined systemic and intraperitoneal chemotherapy. She was treated with ePIPAC after 6 weeks, and then with PIPAC after 3, 6, 9, 12 months and 15 months. All peritoneal biopsies remained negative. Repeated abdominal CT-scans showed objective tumor regression according to RECIST criteria (Figure 3). The patient received 13 cycles of systemic chemotherapy and 7 ePIPAC cycles. The patient is alive 18 months after the first PIPAC or 22 months after the diagnosis of gallbladder cancer without evidence of intraperitoneal disease.
Figure 3:
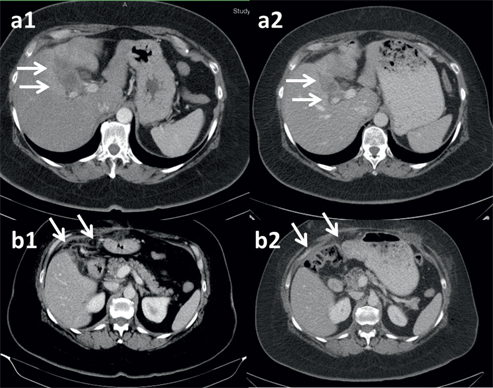
Fifty nine-years old woman with histologically verified peritoneal metastasis of a gallbladder cancer after cholecystectomy.
Postoperative CT-scan showed a residual tumor with central necrosis in the liver hilus (a1) as well as peritoneal metastasis with small nodular diffuse infiltration of fatty tissue (b1). After repeated (e)PIPAC combined with palliative systemic chemotherapy, significant regression of the solid tumor component (a2) and complete regression of the peritoneal metastasis (b2) were documented. Multiple and repeated peritoneal biopsies remained tumor free (complete histological regression, PRGS 1). Patient is alive 22 months after diagnosis and 18 months after first PIPAC.
ePIPAC procedures
As in the preclinical model, application of ePIPAC in human patients was easy and uneventful. Mean operating time was 105±41 min for ePIPAC vs. 87±21 min for PIPAC. No intraoperative technical difficulty or intraoperative complication was noted. No aberrant electrical currents were detected and no alarm activated. The electrostatic precipitation system was turned on at the end of the phase of aerosol production. This time point of activation was arbitrary and has still to be optimized. The electroprecipitation system was turned off after 30 min steady-state. In contrast to conventional PIPAC where the aerosol remains visible on the intraoperative videomonitoring after 30 min, the aerosol vanished optically within 30 s after activation of the electrostatic precipitation system (Supplementary Material, Video).
Safety and tolerability
Blood chemistry after ePIPAC showed no significant liver (Supplementary Material, Figure S1) or renal (data on file) toxicity and this toxicity did not appear to differ grossly from the profile observed after PIPAC. As after PIPAC, a significant postoperative systemic inflammatory response syndrome was documented by increased C-reactive protein (CRP) on PODs 1–3, with a peak on POD 2 (Figure 4). A causal hypothesis is that this reaction might be due to the chemical peritonitis induced by the toxic therapeutic aerosol. Patients reported transient, non-disabling postoperative abdominal pain that was controlled with oral medication. However, local toxicity of the bowel was well controlled, the patients did not report about gastrointestinal symptoms such as nausea/vomiting, diarrhea, constipation, or appetite loss. Importantly, no bowel perforation was registered in the postoperative phase. No significant bowel adhesions were detected at re-laparoscopy. Thus, peritonitis induced by ePIPAC does not appear to cause postoperative adhesions and the reason for this remains unclear at this research stage.
Figure 4:
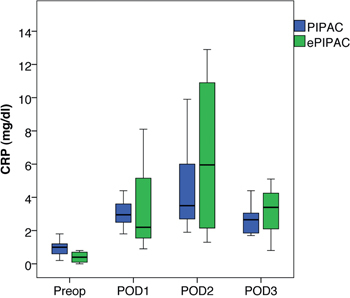
A significant postoperative inflammatory response syndrome was documented by an increase in C-reactive protein (CRP) culminating on postoperative day 2.
Discussion
The additional physical principle applied during ePIPAC as an adjunct to aerosol nature and pressure is old: electrostatic precipitation of particles in an aerosol has been first described at the beginning of the nineteenth century by M. Hohlfeld in Leipzig [24]. Two centuries later, electrostatic precipitation systems are widely used for air purification in the industry and in sterile working environments since they allow highly efficient capture of dry particles and of aerosol droplets [25]. Electrostatic precipitation technology has recently been applied for clearing surgical smoke during laparoscopy. However to our knowledge, this is the first report of the application of chemotherapy as a pressurized aerosol enhanced by electrostatic precipitation technology within the abdomen of human patients. These preliminary data show that ePIPAC was feasible, easy to perform, and safe for the patient. Moreover, ePIPAC, combined or not with PIPAC and intravenous chemotherapy, could induce tumor response in peritoneal metastasis of HBP origin, which have the reputation of being biologically aggressive and therapy-resistant.
The combination of chemotherapy drugs (cisplatin and doxorubicin) applied during ePIPAC was determined in analogy to PIPAC [8] and thus remains largely arbitrary. The chemotherapy dose applied was also derived from PIPAC protocols and an order of magnitude (10x) lower than the regular dose applied during HIPEC or for a single regimen of systemic chemotherapy. A dose-finding study is currently ongoing in order to determine the optimal dose to be applied during PIPAC [26] and the results might by extrapolated later to ePIPAC.
The limited chemotherapy dose applied was probably responsible for the good tolerability of ePIPAC, another reason being the minimally-invasive surgical access. Taken together, these results suggest that safety of ePIPAC might not differ grossly from the results reported after conventional PIPAC [13]. Thus, both PIPAC and ePIPAC may have significant advantages over existing chemotherapy techniques. Of course, safety of ePIPAC has now to be determined in an adequate prospective phase-2 trial.
It can not be expected from this report of the first use of ePIPAC in three patients to deliver reliable efficacy data. However, CT-scans showed an objective tumor regression in 2 patients and stable disease in the third patient according to RECIST criteria, which all were unexpected in this kind and stage of peritoneal disease. Further evidence for a potential efficacy of ePIPAC in PM of HBP origin was delivered by repeated histology, which showed complete regression of peritoneal disease in 2 patients and major regression in the third one according to PRGS [22]. After (e)PIPAC, secondary curative surgery (R0) could be performed in one patient with metastatic cancer of the pancreas tail and no evidence of peritoneal metastasis was found during surgery, all peritoneal histologies remaining negative. Under combined (e)PIPAC and systemic chemotherapy, 2 patients with HBP cancer survived for 11 months after diagnosis of peritoneal metastasis, the third one is alive 22 months after diagnosis without evidence of intraperitoneal disease: Recent publications report on a median overall survival is 4.0 months in stage 4 pancreatic cancer [27] and 4.4 months in gallbladder cancer [28]. It has to be noted that all 3 patients received ePIPAC combined with systemic chemotherapy. Thus, interpretation of these first data should remain most cautious and the results presented in this first preliminary report should not be extrapolated to other patients.
Interestingly, the patient with complete regression of PM of pancreatic origin after systemic and locoregional chemotherapy developed early peritoneal recurrence after surgery, suggesting that this procedure was not useful and might have even stimulated tumor progression by creating peritoneal wounds [29, 30] and generating favorable conditions for tumor cell implantation and growth [31] in this biologically aggressive tumor.
There might also be practical advantages of ePIPAC over PIPAC: since the therapeutic aerosol vanished within seconds after activation of the electroprecipitation system, application time might be considerably reduced with ePIPAC vs. conventional PIPAC technology. Next research step will be to perform repeated pharmacological measurements over time in the preclinical model to determine the absorption and drug tissue uptake curve during the procedure. Should this experiment confirm equivalent of superior drug tissue uptake concentrations as compared to PIPAC [18] immediately after activation of the electroprecipitation system, then operating time could be reduced in the clinical setting. This would not only reduce the operating time and the costs of the procedure, but also lower the risk of occupational exposure to toxic aerosols since the potential inhaled dose is proportional to the time of exposure [32].
In conclusion, ePIPAC is a novel procedure providing another potential means of delivering drugs into the peritoneal cavity. These early data in the human patient suggest that ePIPAC can be safe and can induce regression of PM even in biologically aggressive tumors such as hepatobiliary and pancreatic adenocarcinoma. Both PIPAC and ePIPAC are generic therapeutic approaches allowing delivery of a large range of molecules into the abdominal cavity, the thoracic cavity (data on file) or into hollow organs [33]. Several challenges have now to be overcome including proper selection of drugs, optimization of physicochemical administration parameters including possible use of hyperthermia [34], development of advanced formulations, and the design of proper clinical trials.
References
- 1.Lambert LA. Looking up: Recent advances in understanding and treating peritoneal carcinomatosis. CA Cancer J Clin 2015 Jul–Aug;65:284–98. [DOI] [PubMed]
- 2.Chemotherapy MM. Limited use of the intraperitoneal route for ovarian cancer-why? Nat Rev Clin Oncol 2015 Nov;12:628–30. [DOI] [PubMed]
- 3.Reymond MA, Hu B, Garcia A, Reck T, Köckerling F, Hess J, et al. Feasibility of therapeutic pneumoperitoneum in a large animal model using a microvaporisator. Surg Endosc 2000 Jan;14:51–5. [DOI] [PubMed]
- 4.Dedrick RL, Flessner MF. Pharmacokinetic problems in peritoneal drug administration: tissue penetration and surface exposure. J Natl Cancer Inst 1997;89:480–7. [DOI] [PubMed]
- 5.Haidira A, Pocard M. Nouveau mode d’administration en intrapéritonéal d’une chimiothérapie dans le traitement de la carcinose péritonéale: PIPAC (Pressurized Intraperitoneal Aerosol Chemotherapy). Master Thesis, University Paris 13, 2015.
- 6.Solaß W, Hetzel A, Nadiradze G, Sagynaliev E, Reymond MA. Description of a novel approach for intraperitoneal drug delivery and the related device. Surg Endosc 2012;26:1849–55. [DOI] [PubMed]
- 7.Solass W, Herbette A, Schwarz T, Hetzel A, Sun JS, Dutreix M, et al. Therapeutic approach of human peritoneal carcinomatosis with Dbait in combination with capnoperitoneum: proof of concept. Surg Endosc 2012;26:847–52. [DOI] [PMC free article] [PubMed]
- 8.Solass W, Kerb R, Mürdter T, Giger-Pabst U, Strumberg D, Tempfer C, et al. Intraperitoneal chemotherapy of peritoneal carcinomatosis using pressurized aerosol as an alternative to liquid solution: first evidence for efficacy. Ann Surg Oncol 2014 Feb;21:553–9. [DOI] [PMC free article] [PubMed]
- 9.Blanco A, Giger-Pabst U, Solass W, Zieren J, Reymond MA. Renal and hepatic toxicities after pressurized intraperitoneal aerosol chemotherapy (PIPAC). Ann Surg Oncol 2013 Jul;20:2311–16. [DOI] [PMC free article] [PubMed]
- 10.Tempfer CB, Celik I, Solass W, Buerkle B, Pabst UG, Zieren J, et al. Activity of Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) with cisplatin and doxorubicin in women with recurrent, platinum-resistant ovarian cancer: preliminary clinical experience. Gynecol Oncol 2014 Feb;132:307–11. [DOI] [PubMed]
- 11.Nadiradze G, Giger-Pabst U, Zieren J, Strumberg D, Solass W, Reymond MA. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) with Low-Dose Cisplatin and Doxorubicin in Gastric Peritoneal Metastasis. J Gastrointest Surg 2015 Oct 28. [Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 12.Demtröder C, Solass W, Zieren J, Strumberg D, Giger-Pabst U, Reymond MA. Pressurized intraperitoneal aerosol chemotherapy (PIPAC) with oxaliplatin in colorectal peritoneal metastasis. Colorectal Dis 2015 Sep 24. [Epub ahead of print]. [DOI] [PubMed]
- 13.Tempfer CB, Winnekendonk G, Solass W, Horvat R, Giger-Pabst U, Zieren J, et al. Pressurized intraperitoneal aerosol chemotherapy in women with recurrent ovarian cancer: A phase 2 study. Gynecol Oncol 2015 May;137:223–8. [DOI] [PubMed]
- 14.Study of Efficacy and Safety of Laparoscopic Intra-abdominal Chemotherapy (PIPAC) Performed in Patients With Peritoneal Carcinomatosis From Colorectal, Ovarian, Gastric Cancer and Primary Peritoneal Tumors (PI-CaP). NCT0260478, www.clincialtrials.gov, Accessed Feb 22, 2016.
- 15.Treating Peritoneal Carcinomatosis With PIPAC, NCT02320448, www.clincialtrials.gov, Accessed Feb 22, 2016.
- 16.Intraperitoneal Aerosol Chemotherapy in Gastric Cancer (PIPAC-GA01), NCT01854255, www.clincialtrials.gov, Accessed Feb 22, 2016.
- 17.Ansell J, Warren N, Wall P, Cocks K, Goddard S, Whiston R, et al. Electrostatic precipitation is a novel way of maintaining visual field clarity during laparoscopic surgery: a prospective double-blind randomized controlled pilot study. Surg Endosc 2014 Jul;28:2057–65. [DOI] [PubMed]
- 18.Kakchekeeva T, Demtröder C, Herath NI, Griffiths D, Torkington J, Solaß W, et al. In Vivo Feasibility of Electrostatic Precipitation as an Adjunct to Pressurized Intraperitoneal Aerosol Chemotherapy (ePIPAC). Ann Surg Oncol 2016 Feb 2. [Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 19.Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal metastasis. In: Sugarbaker PH, editor. Peritoneal metastasis: principles of management. Boston: Kluwer Academic Publishers, 1996:359–74. [DOI] [PubMed]
- 20.Solass W, Giger-Pabst U, Zieren J, Reymond MA. Pressurized intraperitoneal aerosol chemotherapy (PIPAC): occupational health and safety aspects. Ann Surg Oncol 2013 Oct;20:3504–11. [DOI] [PMC free article] [PubMed]
- 21.Oyais A, Solass W, Zieren J, Reymond MA, Giger-Pabst U. Occupational health aspects of Pressurised Intraperitoneal Aerosol Chemotherapy (PIPAC): confirmation of harmlessness. Zentralbl Chir 2014 Feb 4. [Epub ahead of print]. [DOI] [PubMed]
- 22.Solass W, Sempoux C, Carr NY, Detlefsen S, Bibau F. Peritoneal sampling procedures and histological assessment of therapeutic response: Proposal of the Peritoneal Regression Grading Score (PRGS). Pleura Peritoneum 2016. [Epub ahead of print]. [DOI] [PMC free article] [PubMed]
- 23.Common Terminology Criteria for Adverse Events (CTCAE) version 4.0; published: May 28, 2009 v4.03. U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute; June 14 2010.
- 24.Hohlfeld M. Das Niederschlagen des Rauches durch Elektricitat. Kastner Arch Gesammte Naturl 1824;2:205–6.
- 25.Parker KR, editor. Applied electrostatic precipitation. Springer: Netherlands, 1997, ISBN 978-94-009-1553-4.
- 26.A Study With Intraperitoneal Cisplatin and Doxorubicin in Recurrent Ovarian Cancer and Peritoneal Carcinomatosis. NCT02475772. www.clinicaltrials.gov, Accessed Nov 4, 2015.
- 27.Kim HW, Lee JC, Paik KH, Lee YS, Hwang JH, Kim J. Initial metastatic site as a prognostic factor in patients with stage IV pancreatic ductal adenocarcinoma. Medicine (Baltimore) 2015 Jun;94:e1012. [DOI] [PMC free article] [PubMed]
- 28.Ji JH, Song HN, Kim RB, Oh SY, Lim HY, Park JO, et al. Natural history of metastatic biliary tract cancer (BTC) patients with good performance status (PS) who were treated with only best supportive care (BSC). Jpn J Clin Oncol 2015 Mar;45:256–60. [DOI] [PubMed]
- 29.Antonio N, Bønnelykke-Behrndtz ML, Ward LC, Collin J, Christensen IJ, Steiniche T, et al. The wound inflammatory response exacerbates growth of pre-neoplastic cells and progression to cancer. EMBO J 2015 Sep 2;34:2219–36. [DOI] [PMC free article] [PubMed]
- 30.Elias D, Goéré D. Treat the peritoneum with respect! It’s our first line of defense against carcinomatosis. J Chir (Paris) 2007 Jul-Aug;144:275–6. [DOI] [PubMed]
- 31.Reymond MA, Köckerling F, Bonjer J, editors. Port site and wound recurrences in cancer surgery. New York, Heidelberg: Springer, 2001.
- 32.Reymond L, Solass W, Tempfer CB, Reymond MA. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC): occupational health and safety management. In: Berhardt L.V. editor,Advances in medicine and biology. Volume 87. Hauppauge, NY: Nova Science Publishers, 2015.
- 33.Khalili-Harbi N, Herath N, Solass W, Giger-Pabst U, Dutreix M, Reymond MA. Pressurized intraluminal aerosol chemotherapy with Dbait in the distal esophagus of swine. Endoscopy 2016 Feb;48:184–7. [DOI] [PubMed]
- 34.Jung DH, Son SY, Oo AM, Park YS, Shin DJ, Ahn SH, et al. Feasibility of hyperthermic pressurized intraperitoneal aerosol chemotherapy in a porcine model. Surg Endosc 2015 Dec 29. [Epub ahead of print]. [DOI] [PubMed]