

Abstract
Objective
To develop a new measure of caregiver strain for use in caregivers of individuals with TBI, TBI-CareQOL Caregiver Strain.
Design
Qualitative data, literature reviews, and cross-sectional survey study.
Setting
Three TBI Model Systems rehabilitation hospitals, an academic medical center, and a military medical treatment facility.
Participants
Five-hundred-sixty caregivers of civilians (n=344) or service members/veterans (SMVs) with TBI (n=216).
Interventions
Not applicable.
Main Outcome Measure
TBI-CareQOL Caregiver Strain Item Bank
Results
Exploratory and confirmatory factor analyses, a graded response model (GRM) and differential item functioning supported the retention of 33 items in the final measure. GRM calibration data was used to inform the selection of a 6-item static short form, and to program the TBI-CareQOL Caregiver Strain computer-adaptive test (CAT). CAT simulation analyses indicated a 0.97 correlation between the CAT scores and the full item-bank. Three-week test-retest reliability was strong (r = 0.83).
Conclusions
The new TBI-CareQOL Caregiver Strain CAT and corresponding 6-item short form were developed using established rigorous measurement development standards; this is the first self-reported measure developed to evaluate caregiver strain in caregivers of individuals with TBI.
Keywords: Health-related quality of life, PROMIS, TBI-CareQOL, traumatic brain injury, caregiver, caregiver strain, caregiver burden, patient reported outcome
Over the past 30 years, many studies have documented significant distress for caregivers of persons with traumatic brain injury (TBI). Caregivers may experience emotional distress, including depression and anxiety, from as early as three months to as long as seven years after injury and beyond.1–9 While this has been mostly described in those caring for individuals with more severe TBI, it can also occur in those caring for individuals with mild or moderate TBI, especially in the context of significant comorbid physical injuries or emotional trauma.10–15 Caregiver distress often increases over time, as caregivers are faced with persistent impairments in the person with injury.16,17 Pre-existing emotional distress is present in about a third of caregivers of persons with TBI and can predispose them to difficulty coping with the effects of injury.18,19
Strain on caregivers may be attributed to the fact that they are often the primary source of assistance for financial, functional, and social components of daily living.20 About one-third of persons with more severe TBI require supervision at one year post-injury in both civilian21 and service member/veteran (SMV)22 samples; over one-fourth still require assistance at 2-9 years post-injury.23 Unemployment is a major problem for individuals with TBI, with 30-40% of civilians returning to work24–26 and only 20.5% of SMVs working at one year post-injury.27 Reduced independence and community participation in the person with TBI contributes substantially to distress in family caregivers.9 Caregivers often feel isolated and perceive discrimination and stigma associated with the caregiving role,28 and they report a variety of unmet emotional and instrumental/practical needs for at least two years post-injury.29–31 Loneliness and less contact with friends contribute to caregivers’ feelings of stress.32,33
Caregiver stress has historically been conceptualized under the term “burden”, which refers to stress directly associated with injury-related changes.34 The concept of caregiver burden is not well-conceptualized, nor is there a clear consensus definition of this term.35,36 Early research distinguished between objective burden (perceived changes in the person with injury) and subjective burden (distress experienced by caregivers as a result of injury-related changes).37 Initially, subjective burden was rated on a single, 7-point Likert scale to assess stress resulting from the TBI.2,3,38 Over time, the multidimensional nature of caregiver burden39 was recognized, and attempts were made to assess it, often via homegrown questionnaires with unknown psychometric properties.40 Others adapted existing measures other disorders, including dementia and multiple sclerosis (Caregiver Burden Inventory,41 Caregiver Burden Scale,42 Zarit Burden Interview,43 Caregiver Appraisal Scale44,45). While these measures have shown utility for investigating some aspects of the caregiving role following TBI, other issues specific to TBI caregivers are neglected. For example, the young age of many persons with TBI means they will need care for a longer period of time compared to persons with dementia.46–49 Cognitive and behavioral changes also differ between severe TBI and dementia or multiple sclerosis.50,51 Therefore, a measure of stress or burden specific to TBI caregivers is warranted.
Recent efforts have been devoted to developing patient-reported outcome (PRO) assessments through the Patient-Report Outcomes Measurement Information System (PROMIS).52,53 PROMIS is a dynamic measurement system for physical, mental, and social well-being offering several advantages: measures are brief, administration can include a computer-adaptive test (CAT; a smart test in which items are selected based on the respondents’ previous response—therefore, only the most relevant items in the bank are administered to each respondent) or fixed-length short form (SF), and measures are available across multiple domains of functioning. However, PROMIS does not include any caregiver-specific content or content that is specific to caring for someone with a TBI. To address this need, the TBI-CareQOL measurement system was developed using the established PROMIS methodology.54–57 This paper describes the development of a PRO measure of caregiver-reported HRQOL; TBI-CareQOL Caregiver Strain is designed to capture feelings of being overwhelmed or stressed by the caregiver role.
Methods
Study Participants
A total of 560 caregivers of individuals with TBI participated in this study (n=344 caregivers of civilians and n=216 caregivers of SMVs); some (56 civilian, 89 SMV) also completed a retest approximately 3 weeks after the initial visit. A detailed study description is reported elsewhere in this issue (Carlozzi et al., Under Review58). Briefly, recruitment targeted existing hospital- and community-based initiatives, TBI caregiver databases, and medical record data capture systems (MiChart and the Electronic Medical Record Search Engine59). Participants were recruited through University of Michigan, TIRR Memorial Hermann, Rehabilitation Institute of Michigan, Kessler Foundation, and Walter Reed National Military Medical Center; retest participants were recruited solely through the University of Michigan. Caregivers were ≥18 years of age and able to read/understand English. For the civilian sample, caregivers were caring for an individual with a medically documented complicated mild, moderate, or severe TBI (according to TBI Model System criteria60). For the SMV sample, caregivers were caring for an individual with a TBI that was documented by a Department of Defense or Veteran Affairs treatment facility. For both groups, the person with the TBI was ≥16 years of age at the time of injury and ≥1 year post injury. All caregivers were required to indicate that they provided physical assistance, financial assistance, or emotional support to an individual with a TBI. Data were collected with local institutional review boards; all participants provided consent prior to study participation.
Study Measures
The TBI-CareQOL Caregiver Strain Item Pool
An initial pool of 75 questions was designed to evaluate caregiver strain, using the PROMIS methodology.54,61 Specific item content was based on focus group discussions nine groups each with caregivers of civilians and nine groups with caregivers of SMVs with TBI.62,63 Items were further refined by expert review (n=11 Ph.D. and n=3 masters’-level investigators with expertise in TBI, caregivers of TBI, and measurement development), evaluation of item literacy level (to ensure ≤6th grade reading level), and participant cognitive review to ensure adequate content coverage and appropriate reading and comprehension levels. The final item pool was comprised of 66 items that examined feelings of being overwhelmed, stressed, self-defeated, down trodden, or beat down as a consequence of undertaking the role of caregiver for a person with TBI.
Statistical Analyses
Sample size considerations are reported elsewhere this special issue (Carlozzi et al., Under Review).58
Overview
New measurement development included classical test theory and item response theory (IRT) analyses. First, an essentially unidimensional set of items (using classical test theory approaches described below) were identified, and second, IRT64 analysis was conducted to estimate the item parameters (slopes and thresholds) necessary for CAT administration of the measure. Given that CAT administration includes only the most relevant and informative items for a specific respondent, CATs have the advantage of brevity (typically 4 to 12 items in length), as well as better precision and lower standard errors than more traditional static measures, even when the number of items for a CAT and a static form are identical.65 Initial analyses began with the full 66-item Caregiver Strain item pool. All statistical analyses were conducted in accordance with PROMIS measurement development guidelines.61
Exploratory Factor Analysis (EFA)/Confirmatory Factor Analysis (CFA) Modeling, Initial Item Performance Assessments
Full-sample EFA and CFA was used to examine and then assess the dimensionality of the item pool (using Mplus version 7.466). EFA was employed to determine if the data supported potential unidimensionality. This was done by examining the eigenvalues, a measure of the amount of the variance that is accounted for by each individual factor (the ratio of eigenvalue 1 to eigenvalue 2 >4 and the proportion of variance accounted for by eigenvalue 1 >.40). Next, items were excluded if they had sparse cells (i.e., a response category with n <10 respondents), if their item-adjusted total score correlation was low (<0.40), or if their observed responses were non-monotonic (according to item-rest plots and expected score by latent trait plots obtained from a non-parametric IRT model conducted using Testgraf67). CFA was then used to screen out items with low factor loadings (lx <0.50) and items demonstrating evidence of local dependence (residual correlation >0.20; correlated error modification index ≥100).68–70 An iterative process was employed for both the EFA and CFA analyses, with clinical input elicited at item content decision points.68–70
IRT Modeling, Final Item Performance Assessments, Differential Item Functioning (DIF)Studies, Final CFA Modeling
After an essentially unidimensional item set was identified and refined, item parameters were estimated with Samejima’s graded response model (GRM),71 using IRTPRO (version 3.1.2).72 Items demonstrating good model fit (S-X2, p>.01) were retained, while items displaying significant misfit (S-X2, p<0.01) were excluded. The retained items were assessed for DIF (response bias for a certain group) using a hybrid IRT ability score-ordinal logistic regression framework73 (implemented in the R package LORDIF Version 0.3-274,75). Items were considered to have impactful DIF if: 1) they were flagged for potential DIF, using a flagging criterion of Nagelkerke pseudo-R2 change ≥0.20; and 2) more than 2% of DIF-corrected vs. uncorrected total score differences exceeded uncorrected total score standard errors. Items were removed due to impactful DIF for age, education, or caregiver status (civilian or SMV). Following DIF-based item exclusions, a final CFA model was run to assess overall model fit to the item response data, using standard fit criteria: comparative fit index (CFI) ≥0.95, Tucker-Lewis index (TLI) ≥0.95, and root mean square error of approximation (RMSEA) <0.15.76–79
CAT Simulation, Short Form Development
A CAT simulation (using Firestar software80) was run to estimate scores based on a CAT administration of the Caregiver Strain item bank and examine item usage frequencies and patterns. A 6-item short form was then developed, using item calibration and calibration-related statistics (e.g., item slope, thresholds, average item difficulty, and item information), in combination with input from clinical experts (n=7 Ph.D.– level investigators with expertise in TBI and/or caregivers of persons with TBI) on item content and its range of coverage. Thus, psychometric and clinical considerations were balanced in order to attain item bank representativeness in the short form items.
Results
Study Participants
Detailed descriptive data is provided in Carlozzi et al.58 Briefly, 344 caregivers of civilians with TBI and 216 caregivers of SMVs with TBI participated in this study. Caregivers were primarily female, Caucasian, married, and caring for their spouse. Caregivers of civilians were significantly older than caregivers of SMVs, and were caring for persons who were significantly older. A greater percentage of caregivers of civilians with TBI had a high school education compared to those caring for SMVs. Caregivers of civilians were much more likely to be unmarried than military caregivers.
Unidimensional Modeling and Analyses
EFA/CFA Modeling, Initial Item Performance Assessments
After field testing 66 Caregiver Strain items, EFA, CFA, and supporting analyses identified 40 essentially unidimensional items (Table 1).
Table 1.
Unidimensional Modeling and Analyses
| Unidimensional Modeling | Initial Item Performance |
IRT Modeling |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
||||||||||||
| Domain | Item pool | EFA E1/E2 ratio (criterion >4) |
Proportion of variance for E1 (criterion >0.40) |
1-factor CFA loading (criterion <.50) |
1-factor CFA residual correlation (criterion >.20) |
1-factor CFA modification index (criterion >100) |
Item-adjusted total score correlation (Criterion <.40) 1 1 |
Sparse cells (criterion<10) |
Problems with monotonicity |
IRT item misfit | DIF | Final item bank |
| Caregiver Strain | 66 items | 8.99 | 0.51 | 0 items | 3 items | 9 items | 1 item | 13 items | 0 items | 7 items | 0 items | 33 items |
Note. CFA = Confirmatory Factor Analysis; EFA = Exploratory Factor Analysis, IRT = Item Response Theory
IRT Modeling, Final Item Performance Assessments, DIF Studies, Final CFA Modeling
Next, an IRT model (GRM) indicated seven items with significant misfit (S-X2, p<0.01; Table 1). After assessing the remaining items, no items were flagged for age or education-related DIF; three items (“I feel like I am the only one who can care for the person with the injury,” “I feel stressed about the medical care the person I care for is receiving,” “I feel frustrated with my situation”) were flagged for potential civilian vs. military DIF. However, since these items did not exhibit impactful DIF (i.e., <2% of DIF-corrected vs. uncorrected score differences exceeded uncorrected score standard errors) and were retained (see Table 2). A final CFA model was run; results suggest good overall model fit to the item response data (Table 2). The final item bank item parameters are reported in Table 3. On a measurement continuum from theta=−2.8 (T-score=22) to +2.8 (T-score=78), score-level information was excellent from theta=−2.0 to +2.8, with expected score-level reliability ≥.90; score-level reliability at theta=−2.4 was also very good (≥.80; Figure 1).
Table 2.
Caregiver Strain Final Item Parameters
| Domain | Item Bank | CFI (criterion >95) | TLI (criterion >.95) | CFA-based RMSEA (criterion < .15) | Alpha Reliability (criterion > .80) | IRT-based RMSEA (criterion < .15) | Response Pattern Reliability (criterion > .80) |
|---|---|---|---|---|---|---|---|
| Caregiver Strain | 33 items | .95 | .95 | .096 | .98 | .08 | .98 |
Note. CFI = Comparative Fit Index, TLI = Tucker-Lewis Index, RMSEA: Root Mean Square Error of Approximation
Table 3.
TBI-CareQOL Caregiver Strain Item Parameters
| Item | Slope | Threshold 1 | Threshold 2 | Threshold 3 | Threshold 4 |
|---|---|---|---|---|---|
| I feel like there is no rest when it comes to providing care for the person with the injury. | 2.14 | −1.25 | −0.36 | 0.65 | 1.51 |
| I have trouble giving the same level of care that I did in the past. | 1.52 | −0.43 | 0.58 | 2.30 | 3.17 |
| Small things stress me out more than they should when it comes to caring for the person with the injury. | 1.92 | −1.28 | −0.31 | 1.08 | 2.06 |
| I feel like I am the only one who can care for the person with the injury. | 1.42 | −1.32 | −0.58 | 0.37 | 1.28 |
| When it comes to caring for the person with the injury, I feel like there is no way out. | 1.88 | −0.24 | 0.42 | 1.59 | 2.27 |
| I have trouble doing general household chores (i.e., taking out the trash) due to the responsibilities I have as a caregiver. | 2.10 | −0.19 | 0.63 | 1.71 | 2.38 |
| I have too much to do because of the responsibilities I have as a caregiver. | 3.07 | −0.58 | 0.08 | 0.95 | 1.71 |
| I wish I had help with the responsibilities I have as a caregiver. | 2.37 | −1.04 | −0.28 | 1.05 | 1.71 |
| I feel angry about the amount of help I get with the responsibilities I have as a caregiver. | 2.66 | −0.18 | 0.49 | 1.45 | 1.94 |
| I am getting more and more tired of my caregiving responsibilities. | 2.59 | −0.25 | 0.55 | 1.52 | 2.16 |
| I cannot handle any more responsibility when it comes to providing care for the person with the injury. | 2.24 | −0.32 | 0.61 | 1.44 | 2.39 |
| I cannot do everything that needs to be done for the person I care for. | 1.76 | −0.54 | 0.46 | 1.72 | 2.73 |
| I feel stressed when it comes to providing care for the person with the injury. | 3.03 | −1.09 | −0.28 | 0.94 | 1.63 |
| I feel so stressed that I am not taking care of myself. | 2.83 | −0.37 | 0.34 | 1.30 | 1.90 |
| I feel drained by my responsibilities as a caregiver. | 3.72 | −0.69 | 0.02 | 1.04 | 1.60 |
| I feel that stress makes me forget things more easily. | 2.59 | −0.85 | −0.10 | 0.95 | 1.65 |
| I feel that stress is making me age faster. | 2.67 | −0.81 | −0.16 | 0.79 | 1.44 |
| I feel like I am never going to stop feeling stressed. | 3.14 | −0.62 | −0.09 | 0.83 | 1.46 |
| I feel stressed about how the person I care for might act. | 1.77 | −1.02 | −0.21 | 1.01 | 1.82 |
| I feel stressed about the medical care the person I care for is receiving. | 1.58 | −0.76 | 0.05 | 1.03 | 1.80 |
| I feel stressed out when interacting with the person I care for. | 1.63 | −0.74 | 0.20 | 1.94 | 2.78 |
| I have to limit my social activity because I have too much to do. | 2.43 | −0.81 | −0.15 | 0.74 | 1.41 |
| I feel that stress makes it difficult to start anything new. | 3.48 | −0.64 | −0.04 | 0.88 | 1.50 |
| I feel that stress makes me feel tired. | 3.40 | −1.18 | −0.63 | 0.42 | 1.10 |
| I feel that there are not enough hours in the day to get everything done. | 2.52 | −1.24 | −0.69 | 0.35 | 0.94 |
| I feel that stress makes it more difficult to concentrate. | 3.02 | −1.16 | −0.36 | 0.68 | 1.40 |
| I feel like I am under too much pressure when it comes to providing care for the person with the injury. | 2.87 | −0.47 | 0.34 | 1.44 | 2.14 |
| I feel so stressed that I am not sure where to begin. | 2.86 | −0.64 | 0.15 | 1.28 | 1.98 |
| I feel like I can never take a break from my caregiver responsibilities. | 2.56 | −0.79 | −0.06 | 0.68 | 1.40 |
| I feel alone in my caregiving duties. | 2.59 | −0.63 | −0.05 | 0.71 | 1.36 |
| I feel frustrated with my situation. | 2.85 | −0.77 | −0.08 | 1.02 | 1.55 |
| I feel so stressed that I want to remove myself from the situation. | 1.64 | 0.03 | 0.84 | 2.17 | 2.98 |
| I feel burdened with the responsibility of caring for the person with the injury. | 2.10 | −0.21 | 0.55 | 1.75 | 2.54 |
Note. Items that are indicated in bold were selected for inclusion on the 6-item Caregiver Strain short form
Figure 1. Caregiver Strain Test Information Plot.
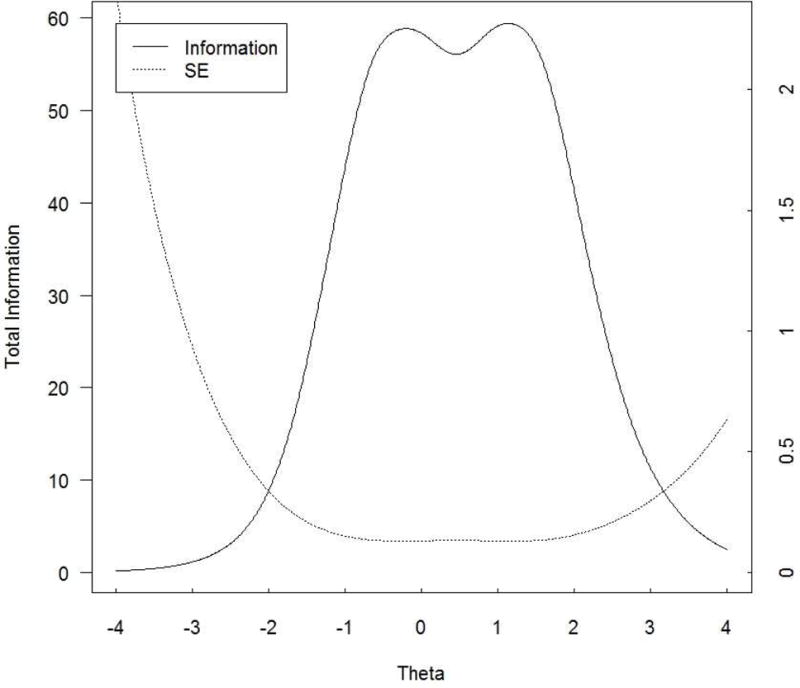
In general, total information should be ≥ 10.0 and the standard error should be ≤ 0.32 (this provides a reliability of 0.9). This figure shows excellent total information and standard errors for Caregiver Strain scale scores between −2.0 and +2.8.
CAT Simulation, Short Form Development
The correlation between full item bank and CAT scores was 0.97. The standard deviation of the differences between these scores was 0.26, while the root mean square deviation (RMSD) of the two scores was also 0.26 (both statistics in the theta metric). The four most common CAT lengths were four items (n=349, 62.3%), five items (n=93, 16.6%), six items (n=48, 8.6%), and 12 items (n=47, 8.4%); CATs 7 to 11 items long occurred infrequently (n=23, 4.1%). The mean CAT length was 5.2 items. For 4-item CATs, observed thetas ranged from −1.05 to +1.67; theta ranges for 5- and 6-item CATs were similar to those observed for 4-item CATs, though slightly wider (5 items: −1.23 to +1.82; 6 items: −1.33 to +2.05). Observed thetas for 12-item CATs were bimodal: Low thetas ranged from −2.30 to −1.34, while high thetas ranged from 2.68 to 2.77. Thus, 12-item CATs occurred when extreme low and extreme high levels of Caregiver Strain were measured. Overall, fewer items were required to estimate scores for the majority of individuals, whose caregiver strain levels ranged from moderately low to moderately high; individuals with either very low or very high levels of caregiver strain required the administration of additional items. The average administration time for a 6-item version was 42 seconds.
Figure 2 shows the number of CAT items used for different scale scores at standard deviation units: at <−1.4 SD units, the CAT tended to use the maximum of 12 items from the item bank; from −1.1 to +1.7 SD units, the CAT tended to use the minimum number of four items from the item bank, with some longer-length CATs occurring, though considerably less frequently than 4-item CATs; and at >2.0 SD units the CAT tended to use the maximum of 12 items from the item bank.
Figure 2. Caregiver Strain Number of CAT Items by CAT Theta.
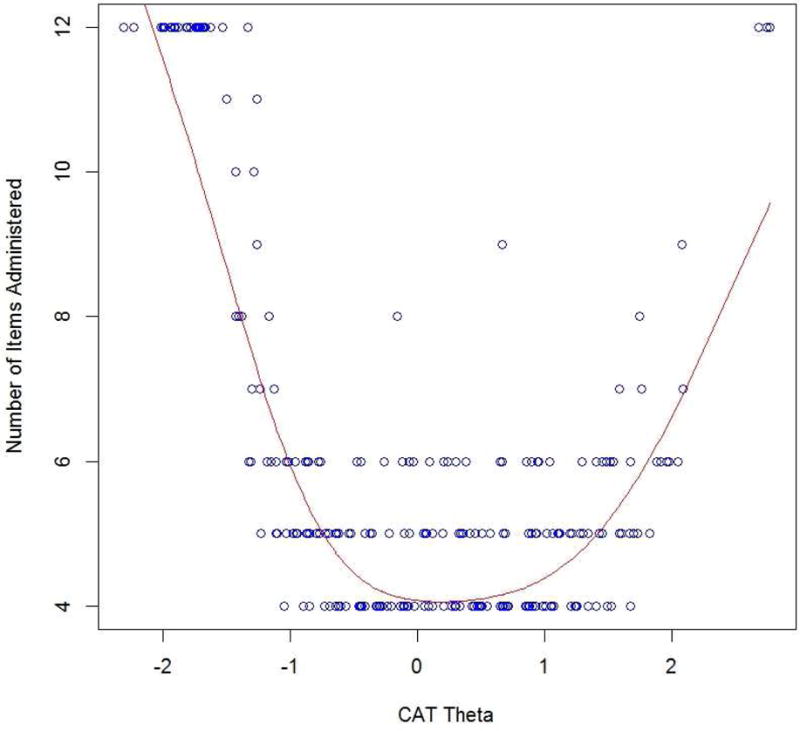
This figure shows the number of CAT items used for different scale scores in standard deviation units: at < −1.4 SD units, the CAT tended to use the maximum of 12 item bank items; from −1.1 to +1.7 SD units, the CAT tended to use the minimum number of 4 item bank items; and at > +2.0 units the CAT tended to use the maximum of 12 item bank items.
Clinical experts approved the Caregiver Strain 6-item short form item content, its representativeness, and its range of coverage. On a measurement continuum from theta = −2.8 (T-score=22) to +2.8 (T-score=78), score-level information was excellent in the theta range from −0.8 to +1.6, with expected score-level reliability ≥ .90; in the extended theta range from −1.6 to +2.4, score-level reliability was very good or excellent (i.e., ≥.80), while in the further extended theta range from −1.6 to +2.8, score-level reliability was good, very good, or excellent (i.e., ≥.70). Three-week test-retest for this short form was very good (r=0.83). Table 4 provides a summed score to t score conversion.
Table 4.
Caregiver Strain Short Form Summed Score to t Score Conversion Table
| Raw Score | T-score | SE * |
|---|---|---|
| 6 | 32.13 | 5.08 |
| 7 | 36.93 | 3.71 |
| 8 | 39.21 | 3.46 |
| 9 | 41.34 | 3.11 |
| 10 | 43.14 | 2.94 |
| 11 | 44.78 | 2.83 |
| 12 | 46.31 | 2.78 |
| 13 | 47.78 | 2.78 |
| 14 | 49.23 | 2.80 |
| 15 | 50.67 | 2.82 |
| 16 | 52.09 | 2.84 |
| 17 | 53.48 | 2.85 |
| 18 | 54.85 | 2.85 |
| 19 | 56.22 | 2.84 |
| 20 | 57.61 | 2.83 |
| 21 | 59.01 | 2.80 |
| 22 | 60.40 | 2.78 |
| 23 | 61.81 | 2.78 |
| 24 | 63.25 | 2.81 |
| 25 | 64.76 | 2.90 |
| 26 | 66.40 | 3.04 |
| 27 | 68.22 | 3.24 |
| 28 | 70.26 | 3.53 |
| 29 | 72.57 | 3.87 |
| 30 | 76.12 | 4.62 |
SE = Standard error
Discussion
This study developed a new PRO to evaluate the caregiver strain component of HRQOL in caregivers of individuals with TBI (the Caregiver Strain item bank and corresponding short form are available at www.assessmentcenter.net). The TBI-CareQOL Caregiver Strain item bank is the first measure to focus on a single, unidimensional and well-defined aspect of caregiver HRQOL—feelings of being overwhelmed, stressed, self-defeated, down trodden, or beat down as a consequence of undertaking the role of caregiver for a person with TBI. This item bank was developed using a well-established, mixed methodology that included critical input from the caregivers themselves, qualitative methods, classical test theory approaches, and item response theory.61 Items are devoid of bias (age, gender, and education) and are equally relevant to civilian- and military-TBI caregivers. This homogenous item set also exhibits excellent reliability that meets or exceeds established measurement development standards.61 This is also the first time that a CAT administration format has been available for use in caregivers. CAT has the advantages of efficiency (only the most relevant items are administered) and sensitivity (predetermined stopping rules for maximal acceptable standard error are implemented). Furthermore, the calibrated short form includes items selected using IRT, and thus scores can be generated, theoretically, from a single item. As a result, missing data are less problematic compared to a measure developed solely using classical test theory. Furthermore, as seen in Figure 2, the CAT administration typically requires fewer than 12 items for most participants, highlighting both test brevity and precision of this measure.
Caregiver Strain is scored using a T metric that indicates how a caregiver is functioning relative to other caregivers of individuals with TBI; higher scores indicate more self-reported strain. Such standardized scores have the advantage of aiding in score interpretation. For example, T scores that are one standard deviation above the mean (i.e., T scores ≥60) suggest clinically significant levels of strain since this is worse than 84% of the larger caregiver population. Scores ≥70 or above indicate extremely significant problems with strain (i.e., their concerns exceed 95.45% of caregivers). This scoring approach can help guide clinical decision making and referrals.
Study Limitations
While this calibration sample included a diverse caregiver cohort, there were not enough parents to assess item bias relative to spouses. Furthermore, there were not enough male caregivers (n=81) to examine item bias by sex (DIF analysis requires ~200 per group81). While all participants required medical record documentation to be included in this study, TBI severity data were lacking for individuals with TBI in the military sample (these data were missing for 60.3% of the military sample). However, these individuals were recruited from the community, and based on existing prevalence rates of TBI severity in the military,82 it can be reasonably assumed that most of this sample (i.e., >80%) falls in the mild TBI classification. Additional work is needed to establish test-retest reliability, validity, and responsiveness to change data for this measure. Preliminary support for reliability and validity are reported elsewhere in this special issue.58
Conclusions
The Caregiver Strain item bank is the first computer adaptive test of caregiver strain to be developed that is relevant to caregivers of both civilians and SMVs with TBI. Since this measure was developed explicitly for use in caregivers of TBI, it should be more sensitive than existing generic measures of caregiver burden. This type of brief measure (taking less than one minute to complete), could potentially be integrated into outpatient visits where patients are often accompanied by caregivers, helping to generate appropriate referrals for caregivers in greatest need of additional services/support. This is especially important given that improvements in caregiver HRQOL have the potential benefit of improving the HRQOL of the person with the TBI (which would be consistent with research that links caregiver and care-recipient outcomes83–90). Finally, while this measure was developed for use in caregivers of individuals with TBI, it may be relevant and clinically useful in other trauma or neurological caregiver populations.
Highlights.
The TBI-CareQOL measurement system includes new and existing self-report measures
Measures were developed specific to caring for someone with traumatic brain injury
Generic measures also evaluate important quality of life constructs for caregivers
Acknowledgments
Work on this manuscript was supported by the National Institutes of Health (NIH)- National Institute of Nursing Research (R01NR013658), the National Center for Advancing Translational Sciences (UL1TR000433), and the Defense and Veterans Brain Injury Center (DVBIC). We thank the investigators, coordinators, and research associates/assistants who worked on this study, the study participants, and organizations who supported recruitment efforts. The University of Michigan Research Team would also like to thank the Hearts of Valor and the Brain Injury Association of Michigan for assistance with community outreach for recruitment efforts at this site.
TBI-CareQOL Site Investigators and Coordinators: Noelle Carlozzi, Anna Kratz, Amy Austin, Mitchell Belanger, Micah Warschausky, Siera Goodnight, Jennifer Miner (University of Michigan, Ann, Arbor, MI); Angelle Sander (Baylor College of Medicine and TIRR Memorial Hermann, Houston, TX), Curtisa Light (TIRR Memorial Hermann, Houston, TX); Robin Hanks, Daniela Ristova-Trendov (Wayne State University/Rehabilitation Institute of Michigan, Detroit, MI); Nancy Chiaravalloti, Dennis Tirri, Belinda Washington (Kessler Foundation, West Orange, NJ); Tracey Brickell, Rael Lange, Louis French, Rachel Gartner, Megan Wright, Angela Driscoll, Diana Nora, Jamie Sullivan, Nicole Varbedian, Johanna Smith, Lauren Johnson, Heidi Mahatan, Mikelle Mooney, Mallory Frazier, Zoe Li, and Deanna Pruitt (Walter Reed National Military Medical Center/Defense and Veterans Brain Injury Center, Bethesda, MD)
List of Abbreviations
- CAT
Computer Adaptive Test
- CFA
Confirmatory Factor Analysis
- CFI
Confirmatory Fit Index
- DIF
Differential Item Functioning
- EFA
Exploratory Factor Analysis
- GRM
Graded Response Model
- HRQOL
Health-Related Quality of Life
- PRO
Patient-Reported Outcome
- PROMIS
Patient-Reported Outcomes Measurement Information System
- RMSD
Root Mean Square Deviation
- RMSEA
Root Mean Squared Error of Approximation
- SE
Standard Error
- SF
Short Form
- SMV
Service Member/Veteran
- TBI
Traumatic Brain Injury
- TBI-CareQOL
Traumatic Brain Injury Caregiver Quality of Life
- TLI
Tucker Lewis Index
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclaimer:
The identification of specific products or scientific instrumentation does not constitute endorsement or implied endorsement on the part of the author, DoD, or any component agency. While we generally exercise reference to products companies, manufacturers, organizations etc. in government produced works, the abstracts produced and other similarly situated research presents a special circumstance when such a product inclusions become an integral part of the scientific endeavor.
References
- 1.Ponsford J, Schonberger M. Family functioning and emotional state two and five years after traumatic brain injury. J Int Neuropsychol Soc. 2010;16(2):306–317. doi: 10.1017/S1355617709991342. [DOI] [PubMed] [Google Scholar]
- 2.Brooks N, Campsie L, Symington C, Beattie A, McKinlay W. The five year outcome of severe blunt head injury: a relative’s view. J Neurol Neurosurg Psychiatry. 1986;49(7):764–770. doi: 10.1136/jnnp.49.7.764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brooks N, Campsie L, Symington C, Beattie A, McKinlay W. The effects of severe head injury on patient and relatives within seven years of injury. Journal of Head Trauma Rehabilitation. 1987;2:1–13. [Google Scholar]
- 4.Kreutzer JS, Gervasio AH, Camplair PS. Primary caregivers’ psychological status and family functioning after traumatic brain injury. Brain Injury. 1994;8(3):197–210. doi: 10.3109/02699059409150973. [DOI] [PubMed] [Google Scholar]
- 5.Kreutzer JS, Rapport LJ, Marwitz JH, et al. Caregivers’ well-being after traumatic brain injury: a multicenter prospective investigation. Arch Phys Med Rehabil. 2009;90(6):939–946. doi: 10.1016/j.apmr.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 6.Livingston MG, Brooks DN, Bond MR. Patient outcome in the year following severe head injury and relatives’ psychiatric and social functioning. Journal of Neurology, Neurosurgery, and Psychiatry. 1985;48(9):876–881. doi: 10.1136/jnnp.48.9.876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Marsh NV, Kersel DA, Havill JA, Sleigh JW. Caregiver burden during the year following severe traumatic brain injury. Journal of clinical and experimental neuropsychology. 2002;24(4):434–447. doi: 10.1076/jcen.24.4.434.1030. [DOI] [PubMed] [Google Scholar]
- 8.Gillen R, Tennen H, Affleck G, Steinpreis R. Distress, depressive symptoms, and depressive disorder among caregivers of patients with brain injury. J Head Trauma Rehabil. 1998;13(3):31–43. doi: 10.1097/00001199-199806000-00004. [DOI] [PubMed] [Google Scholar]
- 9.Winstanley J, Simpson G, Tate R, Myles B. Early indicators and contributors to psychological distress in relatives during rehabilitation following severe traumatic brain injury: findings from the Brain Injury Outcomes Study. J Head Trauma Rehabil. 2006;21(6):453–466. doi: 10.1097/00001199-200611000-00001. [DOI] [PubMed] [Google Scholar]
- 10.Sayer NA, Chiros CE, Sigford B, et al. Characteristics and rehabilitation outcomes among patients with blast and other injuries sustained during the Global War on Terror. Arch Phys Med Rehabil. 2008;89(1):163–170. doi: 10.1016/j.apmr.2007.05.025. [DOI] [PubMed] [Google Scholar]
- 11.Pugh MJ, Finley EP, Copeland LA, et al. Complex comorbidity clusters in OEF/OIF veterans: the polytrauma clinical triad and beyond. Medical Care. 2014;52(2):172–181. doi: 10.1097/MLR.0000000000000059. [DOI] [PubMed] [Google Scholar]
- 12.Dillahunt-Aspillaga C, Powell-Cope G. Community Reintegration, Participation, and Employment Issues in Veterans and Service Members With Traumatic Brain Injury. Arch Phys Med Rehabil. 2018;99(2S):S1–S3. doi: 10.1016/j.apmr.2017.04.013. [DOI] [PubMed] [Google Scholar]
- 13.Grandhi R, Tavakoli S, Ortega C, Simmonds MJ. A Review of Chronic Pain and Cognitive, Mood, and Motor Dysfunction Following Mild Traumatic Brain Injury: Complex, Comorbid, and/or Overlapping Conditions? Brain Sci. 2017;7(12) doi: 10.3390/brainsci7120160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Howrey BT, Graham JE, Pappadis MR, Granger CV, Ottenbacher KJ. Trajectories of Functional Change After Inpatient Rehabilitation for Traumatic Brain Injury. Arch Phys Med Rehabil. 2017;98(8):1606–1613. doi: 10.1016/j.apmr.2017.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sashika H, Takada K, Kikuchi N. Rehabilitation needs and participation restriction in patients with cognitive disorder in the chronic phase of traumatic brain injury. Medicine (Baltimore) 2017;96(4):e5968. doi: 10.1097/MD.0000000000005968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Perlesz A, Kinsella G, Crowe S. Psychological distress and family satisfaction following traumatic brain injury: injured individuals and their primary, secondary, and tertiary carers. J Head Trauma Rehabil. 2000;15(3):909–929. doi: 10.1097/00001199-200006000-00005. [DOI] [PubMed] [Google Scholar]
- 17.Ponsford J, Olver J, Ponsford M, Nelms R. Long-term adjustment of families following traumatic brain injury where comprehensive rehabilitation has been provided. Brain Injury. 2003;17(6):453–468. doi: 10.1080/0269905031000070143. [DOI] [PubMed] [Google Scholar]
- 18.Sander AM, Sherer M, Malec JF, et al. Preinjury emotional and family functioning in caregivers of persons with traumatic brain injury. Archives of Physical Medicine and Rehabilitation. 2003;84(2):197–203. doi: 10.1053/apmr.2003.50105. [DOI] [PubMed] [Google Scholar]
- 19.Davis LC, Sander AM, Struchen MA, Sherer M, Nakase-Richardson R, Malec JF. Medical and psychosocial predictors of caregiver distress and perceived burden following traumatic brain injury. J Head Trauma Rehabil. 2009;24(3):145–154. doi: 10.1097/HTR.0b013e3181a0b291. [DOI] [PubMed] [Google Scholar]
- 20.Jacobs HE. The Los Angeles Head Injury Survey: procedures and initial findings. Arch Phys Med Rehabil. 1988;69(6):425–431. [PubMed] [Google Scholar]
- 21.Hart T, Millis S, Novack T, Englander J, Fidler-Sheppard R, Bell KR. The relationship between neuropsychologic function and level of caregiver supervision at 1 year after traumatic brain injury. Arch Phys Med Rehabil. 2003;84(2):221–230. doi: 10.1053/apmr.2003.50023. [DOI] [PubMed] [Google Scholar]
- 22.Bailey EK, Nakase-Richardson R, Patel N, et al. Supervision Needs Following Veteran and Service Member Moderate to Severe Traumatic Brain Injury: A VA TBI Model Systems Study. J Head Trauma Rehabil. 2017 doi: 10.1097/HTR.0000000000000317. [DOI] [PubMed] [Google Scholar]
- 23.Hall KM, Bushnik T, Lakisic-Kazazic B, Wright J, Cantagallo A. Assessing traumatic brain injury outcome measures for long-term follow-up of community-based individuals. Arch Phys Med Rehabil. 2001;82(3):367–374. doi: 10.1053/apmr.2001.21525. [DOI] [PubMed] [Google Scholar]
- 24.Doctor JN, Castro J, Temkin NR, Fraser RT, Machamer JE, Dikmen SS. Workers’ risk of unemployment after traumatic brain injury: a normed comparison. J Int Neuropsychol Soc. 2005;11(6):747–752. doi: 10.1017/S1355617705050836. [DOI] [PubMed] [Google Scholar]
- 25.Malec JF, Moessner AM. Replicated positive results for the VCC model of vocational intervention after ABI within the social model of disability. Brain Inj. 2006;20(3):227–236. doi: 10.1080/02699050500488124. [DOI] [PubMed] [Google Scholar]
- 26.Murphy L, Chamberlain E, Weir J, Berry A, Nathaniel-James D, Agnew R. Effectiveness of vocational rehabilitation following acquired brain injury: preliminary evaluation of a UK specialist rehabilitation programme. Brain Inj. 2006;20(11):1119–1129. doi: 10.1080/02699050600664335. [DOI] [PubMed] [Google Scholar]
- 27.Dillahunt-Aspillaga C, Nakase-Richardson R, Hart T, et al. Predictors of Employment Outcomes in Veterans With Traumatic Brain Injury: A VA Traumatic Brain Injury Model Systems Study. J Head Trauma Rehabil. 2017 doi: 10.1097/HTR.0000000000000275. [DOI] [PubMed] [Google Scholar]
- 28.Phelan SM, Griffin JM, Hellerstedt WL, et al. Perceived stigma, strain, and mental health among caregivers of veterans with traumatic brain injury. Disabil Health J. 2011;4(3):177–184. doi: 10.1016/j.dhjo.2011.03.003. [DOI] [PubMed] [Google Scholar]
- 29.Kreutzer J, Serio C, Bergquist S. Family needs after brain injury: A quantitative analysis. Journal of Head Trauma Rehabilitation. 1994;9:104–115. [Google Scholar]
- 30.Witol AD, Sander AM, Kreutzer JS. A longitudinal analysis of family needs following traumatic brain injury. NeuroRehabilitation. 1996;7(3):175–187. doi: 10.3233/NRE-1996-7303. [DOI] [PubMed] [Google Scholar]
- 31.Serio C, Kreutzer J, Gervasio A. Predicting family needs after traumatic brain injury: Implications for intervention. Journal of Head Trauma Rehabilitation. 1995;10(2):32–45. [Google Scholar]
- 32.Manskow US, Friborg O, Roe C, Braine M, Damsgard E, Anke A. Patterns of change and stability in caregiver burden and life satisfaction from 1 to 2 years after severe traumatic brain injury: A Norwegian longitudinal study. NeuroRehabilitation. 2017;40(2):211–222. doi: 10.3233/NRE-161406. [DOI] [PubMed] [Google Scholar]
- 33.Manskow US, Sigurdardottir S, Roe C, et al. Factors Affecting Caregiver Burden 1 Year After Severe Traumatic Brain Injury: A Prospective Nationwide Multicenter Study. Journal of Head Trauma Rehabilitation. 2015;30(6):411–423. doi: 10.1097/HTR.0000000000000085. [DOI] [PubMed] [Google Scholar]
- 34.Brooks DN, Aughton ME. Psychological consequences of blunt head injury. Int Rehabil Med. 1979;1(4):160–165. doi: 10.3109/03790797909164037. [DOI] [PubMed] [Google Scholar]
- 35.Chou K-R, Chu H, Tseng C, Lu R-B. The measurement of caregiver burden. Journal of Medical Sciences. 2003;23:73–82. [Google Scholar]
- 36.Bastawrous M. Caregiver burden-A critical discussion. International Journal of Nursing Studies. 2013;50(3):431–441. doi: 10.1016/j.ijnurstu.2012.10.005. [DOI] [PubMed] [Google Scholar]
- 37.Brooks DN. The Head-Injured Family. Journal of clinical and experimental neuropsychology. 1991;13(1):155–188. [Google Scholar]
- 38.McKinlay W, Brooks D, Bond M. The short term outcome of severe blunt head injury as reported by the relatives of the injured person. Journal of Neurology, Neurosurgery, & Psychiatry. 1981;44:527–533. doi: 10.1136/jnnp.44.6.527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.George LK, Gwyther LP. Caregiver well-being: a multidimensional examination of family caregivers of demented adults. Gerontologist. 1986;26(3):253–259. doi: 10.1093/geront/26.3.253. [DOI] [PubMed] [Google Scholar]
- 40.Marsh NV, Kersel DA, Havill JH, Sleigh JW. Caregiver burden at 6 months following severe traumatic brain injury. Brain Injury. 1998;12(3):225–238. doi: 10.1080/026990598122700. [DOI] [PubMed] [Google Scholar]
- 41.Novak M, Guest C. Application of a multidimensional caregiver burden inventory. Gerontologist. 1989;29(6):798–803. doi: 10.1093/geront/29.6.798. [DOI] [PubMed] [Google Scholar]
- 42.Montgomery RJV, Gonyea JG, Hooyman NR. Caregiving and the experience of subjective and objective burden. Family Relations. 1985;34(1):19–26. [Google Scholar]
- 43.Zarit SH, Reever KE, Bach-Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontologist. 1980;20(6):649–655. doi: 10.1093/geront/20.6.649. [DOI] [PubMed] [Google Scholar]
- 44.Lawton MP, Kleban MH, Moss M, Rovine M, Glicksman A. Measuring caregiving appraisal. Journal of gerontology. 1989;44(3):P61–71. doi: 10.1093/geronj/44.3.p61. [DOI] [PubMed] [Google Scholar]
- 45.Struchen MA, Atchison TB, Roebuck TM, Caroselli JS, Sander AM. A multidimensional measure of caregiving appraisal: validation of the Caregiver Appraisal Scale in traumatic brain injury. J Head Trauma Rehabil. 2002;17(2):132–154. doi: 10.1097/00001199-200204000-00005. [DOI] [PubMed] [Google Scholar]
- 46.Taylor CA, Bell JM, Breiding MJ, Xu L. Traumatic Brain Injury-Related Emergency Department Visits, Hospitalizations, and Deaths - United States, 2007 and 2013. MMWR Surveill Summ. 2017;66(9):1–16. doi: 10.15585/mmwr.ss6609a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Faul M, Coronado V. Epidemiology of traumatic brain injury. Handb Clin Neurol. 2015;127:3–13. doi: 10.1016/B978-0-444-52892-6.00001-5. [DOI] [PubMed] [Google Scholar]
- 48.Faul M, Xu L, Wald MM, Coronado VG. Traumatic brain injury in the United States: Emergency department visits, hospitalizations and deaths. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2010. pp. 2002–2006. [Google Scholar]
- 49.Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, Ferri CP. The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement. 2013;9(1):63–75 e62. doi: 10.1016/j.jalz.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 50.Zakzanis KK, Leach L, Kaplan E. Studies on neuropsychology, development, and cognition Neuropsychological differential diagnosis. Lisse, Netherlands: Swets & Zeitlinger Publishers; 1999. [Google Scholar]
- 51.Lezak MD, Howieson DB, Loring DW. Neuropsychological assessment. 4th. NY, NY: Oxford University Press; 2004. [Google Scholar]
- 52.Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested in its first wave of adult self-reported health outcome item banks: 2005-2008. Journal of Clinical Epidemiology. 2010;63:1179–1194. doi: 10.1016/j.jclinepi.2010.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cella D, Yount S, Rothrock N, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): 567 Progress of an NIH Roadmap cooperative group during its first two years. Medical Care. 2007;45(Suppl 1):S3. doi: 10.1097/01.mlr.0000258615.42478.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.PROMIS® Instrument Development and Psychometric Evaluation Scientific Standards. http://www.nihpromis.org/Documents/PROMIS_Standards_050212.pdf.
- 55.Reeve BB, Hays RD, Bjorner JB, et al. Psychometric evaluation and calibration of health-related quality of life item banks: plans for the Patient-Reported Outcomes Measurement Information System (PROMIS) Medical Care. 2007;45(5 Suppl 1):S22–31. doi: 10.1097/01.mlr.0000250483.85507.04. [DOI] [PubMed] [Google Scholar]
- 56.Cella D, Yount S, Rothrock N, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): progress of an NIH Roadmap cooperative group during its first two years. Medical Care. 2007;45(5 Suppl 1):S3–S11. doi: 10.1097/01.mlr.0000258615.42478.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Cook KF, Teal CR, Bjorner JB, et al. IRT health outcomes data analysis project: an overview and summary. Quality of Life Research. 2007;16(Suppl 1):121–132. doi: 10.1007/s11136-007-9177-5. [DOI] [PubMed] [Google Scholar]
- 58.Carlozzi NE, Kallen MA, Hanks R, et al. The TBI-CareQOL Measurement System: Development and validation of health-related quality of life measures for caregivers of civilians and service members/veterans with traumatic brain injury. Archives of Physical Medicine & Rehabilitation. doi: 10.1016/j.apmr.2018.08.175. Under Review, This Issue. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Hanauer DA, Mei Q, Law J, Khanna R, Zheng K. Supporting information retrieval from electronic health records: A report of University of Michigan’s nine-year experience in developing and using the Electronic Medical Record Search Engine (EMERSE) Journal of Biomedical Informatics. 2015;55:290–300. doi: 10.1016/j.jbi.2015.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Corrigan JD, Cuthbert JP, Whiteneck GG, et al. Representativeness of the Traumatic Brain Injury Model Systems National Database. Journal of Head Trauma Rehabilitation. 2012;27(6):391–403. doi: 10.1097/HTR.0b013e3182238cdd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zaider TI, Heimberg RG, Fresco DM, Schneier FR, Liebowitz MR. Evaluation of the clinical global impression scale among individuals with social anxiety disorder. Psychological Medicine. 2003;33(4):611–622. doi: 10.1017/s0033291703007414. [DOI] [PubMed] [Google Scholar]
- 62.Carlozzi NE, Brickell TA, French LM, et al. Caring for our wounded warriors: A qualitative examination of health-related quality of life in caregivers of individuals with military-related traumatic brain injury. Journal of rehabilitation research and development. 2016;53(6):669–680. doi: 10.1682/JRRD.2015.07.0136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Carlozzi NE, Kratz AL, Sander AM, et al. Health-related quality of life in caregivers of individuals with traumatic brain injury: development of a conceptual model. Archives of Physical Medicine & Rehabilitation. 2015;96(1):105–113. doi: 10.1016/j.apmr.2014.08.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.PARSCALE [computer program] Lincolnwood, IL: Scientific Software International Inc.; 2003. [Google Scholar]
- 65.Lai JS, Cella D, Choi S, et al. How item banks and its applications can influence measurement practice in rehabilitation medicine: A PROMIS fatigue item bank example. Arch Phys Med Rehabil. 2011;92(Supp 1):S20–S27. doi: 10.1016/j.apmr.2010.08.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Muthén LK, Muthén BO. Mplus User’s Guide. Los Angeles, CA: Muthén & Muthén;; 2011. [Google Scholar]
- 67.TestGraf [computer program] Canada: McGill University; Aug 1, 2000. [Google Scholar]
- 68.McDonald RP. Test theory: A unified treatment. Mahwah, NJ: Lawrence Erlbaum Associates, Inc; 1999. [Google Scholar]
- 69.Reise SP, Morizot J, Hays RD. The role of the bifactor model in resolving dimensionality issues in health outcomes measures. Quality of Life Research. 2007;16(Suppl 1):19–31. doi: 10.1007/s11136-007-9183-7. [DOI] [PubMed] [Google Scholar]
- 70.Cook KF, Kallen MA, Amtmann D. Having a fit: Impact of number of items and distribution of data on traditional criteria for assessing IRT’s unidimensionality assumption. Quality of Life Research. 2009;18(4):447–460. doi: 10.1007/s11136-009-9464-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Samejima F, van der Liden WJ, Hambleton R. The graded response model. In: van der Liden WJ, editor. Handbook of modern item response theory. NY, NY:: Springer; 1996. pp. 85–100. [Google Scholar]
- 72.IRTPRO for Windows [Computer software] [computer program] Lincolnwood, IL: Scientific Software International; 2015. [Google Scholar]
- 73.Crane PK, Gibbons LE, Jolley L, van Belle G. Differential item functioning analysis with ordinal logistic regression techniques. DIFdetect and difwithpar. Medical Care. 2006;44(11 Suppl 3):S115–123. doi: 10.1097/01.mlr.0000245183.28384.ed. [DOI] [PubMed] [Google Scholar]
- 74.R: A language and environment for statistical computing [computer program] Vienna, Austria: R Foundation for Statistical Computing; 2014. [Google Scholar]
- 75.Choi SW, Gibbons LE, Crane PK. Lordif: An R package for detecting differential item functioning using iterative hybrid ordinal logistic regression/item response theory and monte carlo simulations. Journal of Statistical Software. 2011;39(8):1–30. doi: 10.18637/jss.v039.i08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kline RB. Principles and Practice of Structural Equation Modeling, Second Edition. New York: Guilford Press; 2005. [Google Scholar]
- 77.Bentler PM. Comparative Fit Indexes in Structural Models. Psychological Bulletin. 1990;107(2):238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- 78.Hu LT, Bentler PM. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Structural Equation Modeling-a Multidisciplinary Journal. 1999;6(1):1–55. [Google Scholar]
- 79.Hatcher L. A step-by-step approach to using SAS for factor analysis and structural equation modeling. Cary, NC: SAS Institute, Inc; 1994. [Google Scholar]
- 80.Choi SW. Firestar: Computerized Adaptive Testing Simulation Program for Polytomous Item Response Theory Models. Applied Psychological Measurement. 2009;33(8):644–645. [Google Scholar]
- 81.Clauser BE, Hambleton RK. Review of differential item functioning. Journal of Educational Measurement. 1994;31(1):88–92. [Google Scholar]
- 82.DVBIC. DoD Worldwide Numbers for TBI. 2015 http://dvbic.dcoe.mil/dod-worldwide-numbers-tbi. Accessed 02/10, 2017.
- 83.Smith AM, Schwirian PM. The relationship between caregiver burden and TBI survivors’ cognition and functional ability after discharge. Rehabilitation Nursing. 1998;23(5):252–257. doi: 10.1002/j.2048-7940.1998.tb01795.x. [DOI] [PubMed] [Google Scholar]
- 84.Vangel SJ, Jr, Rapport LJ, Hanks RA. Effects of family and caregiver psychosocial functioning on outcomes in persons with traumatic brain injury. J Head Trauma Rehabil. 2011;26(1):20–29. doi: 10.1097/HTR.0b013e318204a70d. [DOI] [PubMed] [Google Scholar]
- 85.Florian V, Katz S, Lahav V. Impact of traumatic brain damage on family dynamics and functioning: A review. Brain Injury. 1989;3(3):219–233. doi: 10.3109/02699058909029637. [DOI] [PubMed] [Google Scholar]
- 86.McLaughlin AM, Carey JL. The adversarial alliance: developing therapeutic relationships between families and the team in brain injury rehabilitation. Brain Injury. 1993;7(1):45–51. doi: 10.3109/02699059309008155. [DOI] [PubMed] [Google Scholar]
- 87.Pelletier PM, Alfano DP. Depression, social support, and family coping following traumatic brain injury. Brain and Cognition. 2000;44(1):45–49. [Google Scholar]
- 88.Sander AM, Caroselli JS, High WM, Becker C, Neese L, Scheibel R. Relationship of family functioning to progress in a post-acute rehabilitation programme following traumatic brain injury. Brain Injury. 2002;16(8):649–657. doi: 10.1080/02699050210128889. [DOI] [PubMed] [Google Scholar]
- 89.Sander AM, Maestas KL, Sherer M, Malec JF, Nakase-Richardson R. Relationship of caregiver and family functioning to participation outcomes after postacute rehabilitation for traumatic brain injury: a multicenter investigation. Arch Phys Med Rehabil. 2012;93(5):842–848. doi: 10.1016/j.apmr.2011.11.031. [DOI] [PubMed] [Google Scholar]
- 90.Sady MD, Sander AM, Clark AN, Sherer M, Nakase-Richardson R, Malec JF. Relationship of preinjury caregiver and family functioning to community integration in adults with traumatic brain injury. Arch Phys Med Rehabil. 2010;91(10):1542–1550. doi: 10.1016/j.apmr.2010.07.012. [DOI] [PubMed] [Google Scholar]