

Abstract
Background:
Transtheoretical model (TTM) is one of the most commonly used methods in behavioral change modeling. The aim of this study was to conduct a systematic review (SR) to determine research gaps with regard to this template with an emphasis on intervention for patients with chronic diseases (CDs).
Materials and Methods:
ISI-WOS, Scopus, PubMed, SID, and Magiran databases were examined systematically and on the basis of defined criteria. Titles, abstracts, and full texts of articles retrieved were examined for the presence of defined criteria. Then finalized articles were analyzed in consensus meetings. After that, references of selected articles and full text of those meeting the criteria were also analyzed.
Results:
We screened 103 articles, excluded 27 in abstract review and 34 in full-text review, leaving 42 articles for critical appraisal. Then the references of these 42 articles were also screened. Fifty articles were excluded on abstract review and 5 on full-text review, leaving 15 articles. The result of the analysis of 57 final articles of this SR determined that 28 articles were about aspects of TTM and 5 stages of change were the most commonly used aspect. Eight articles used TTM in intervention about CDs. A total of 21 articles examined TTM's pros and cons, most of which were about TTM's pros.
Conclusions:
The majority of studies focused on the effectiveness of TTM on the behavioral change management. This finding supported the hypothesis that TTM can be applied in the prevention of CDs.
Keywords: Health behavior, review, theoretical model
Introduction
Industrialization of societies and an increasingly mechanical lifestyle has led to increased prevalence of chronic diseases (CDs) such as obesity, heart diseases, osteoporosis, and chronic back pain.[1] The increasing prevalence of CDs has serious health implications for individuals especially nurses and may also impact general health and workforce participation.[2] Studies show that obesity in nurses will lead to various problems such as lower back pain, heart diseases, and reduced on-duty times.[3] In prevention of CDs, the main focus is on education and lifestyle improvements. One of the methods of improving lifestyle is changing behavioral patterns.[4,5]
Transtheoretical model (TTM) of behavioral change is one of the behavioral change models which states that changing a behavior is not a coincidence but instead is a process and different people are in different stages of change (SC) and readiness. In this process, people pass through five stages: precontemplation, contemplation, preparation, action, and maintenance.[6]
In this pattern, it is possible to return to a previous level as well. There are three factors controlling the transfer between different stages and the time necessary for change which include the following: process of change (PC), decisional balance (DB), and self-efficiency (SE).[7] Due to its cost and time-effective nature, TTM has been used in prevention interventions for chronic conditions such as diabetes and various forms of cancers. The results of these studies show the effectiveness of TTM in this regard.[8]
Due to the importance of this topic, this study focused on use of TTM especially in the context of healthcare with emphasis on the impacts of TTM on information-seeking behaviors of patients with CDs. The current systematic review (SR) was conducted to present a comprehensive and complete review of the studies for the following research objectives: Which studies have used different aspects of TTM? Why studies have used TTM to improve health behaviors in CDs? What are the pros and cons of TTM in the studies?
Materials and Methods
To start, a literature review coordination session was conducted in May 2015 for the research team to determine the inclusion criteria. The following core national and international databases were searched: Magiran, SID, Scopus, PubMed, and ISI-WOS. Two Persian core databases are the most widely used and reliable Persian databases. There are a lot of interdisciplinary articles in the field of medical sciences in Scopus, PubMed, and ISI-WOS; therefore, they were chosen based on inclusion criteria and their ability to adequately respond to the research team. There was also an overlap between articles of different databases.
The search was carried out with the following search strategies: “Stages of change model" in title, abstract, keywords, subject, or mesh, “Stages of change model" AND “pros OR cons" in title, abstract, keywords, “Trans theoretical model" OR “Stages of change model" AND “chronic diseases" in title, abstract, keywords, subject, or mesh.
All English language articles published between 2009 and 2015 were included if they met the following eligibility criteria: (a) using different aspects of TTM, (b) using TTM in CDs, (c) examining pros and cons of TTM, and (d) being written in English or Persian languages. These articles were screened by title and abstract content for inclusion by AR and MH. The references of the included articles were hand-searched for other eligible articles. Following this comprehensive process, the included articles were distributed for review among all the authors according to their expertise and experience.
All articles were reviewed by AR, MH, and all of coauthors. The authors used a data extraction template [Table 1] based on previous studies of SR team leader (AR).[9] The template kept the extracted information consistent: study types, subject area, results, goals, methods, outputs, society, dimension of data quality, and critical thinking about research. Three consensus meetings were arranged among AR, MH, and each of the coauthors to discuss and achieve final consensus and synthesis of the findings. Table 2 is used as a tool to gather opinions and similarities and differences of reviewers' opinions. Using this method, a total of 57 articles were analyzed.
Table 1.
Reviewers’ critical appraisal template
| Row | Author/title/reference | Type of research | Society studied | Goals | Methods/tools | Subject area | Dimensions of data quality studied/the model presentation for evaluation | Results | Critical thinking about research: about quality of tools and method/relevancy |
|---|---|---|---|---|---|---|---|---|---|
Table 2.
Summary template to summarize critical appraisal differences between reviewers
| Author/title/year | First research analysis | Second research analysis | Third research analysis |
|---|---|---|---|
Ethical consideration
Research ethics confirmation was received from the Ethical Review Board at Isfahan University of Medical Sciences. The approval number of the project is 3995540.
Results
In the first iteration, we identified 103 articles after applying the search strategies, of which 27 were excluded in abstract review because they did not meet inclusion criteria or they were duplicates, leaving 76 articles. After full-text review, 34 articles were excluded which left 42 articles for critical appraisal [Figure 1]. After reviewing references of selected articles in previous round, a total 70 articles were retrieved, of which 50 were excluded in abstract review and 5 in full-text review. Finally, 15 articles were analyzed. Of 57 finalized articles, 28 articles examined different aspects of TTM, 8 articles used TTM in CDs, 21 articles studied pros and cons of TTM, 21 articles were in Persian, and 36 articles were in English [Figure 2].
Figure 1.
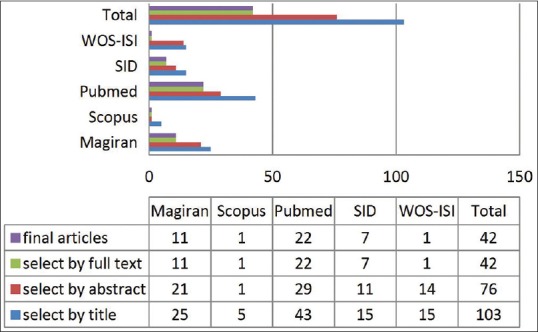
Retrieved articles in searching selected databases in the first iteration
Figure 2.
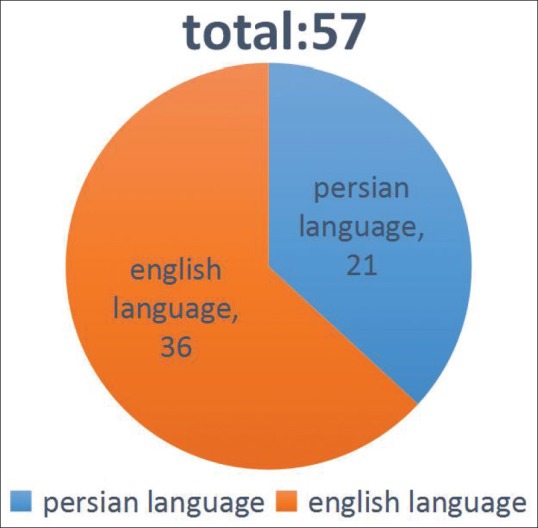
Finalized articles by the language
One article responded to questions a and c at the same time.[8] Articles relevant to first research question were divided based on their subject area in Table 3 which shows various mentioned aspects of TTM such as 5 SC,[4,8,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27] PC,[28] DB,[29,30,31] and SE.[32,33,34,35] However, the results indicated that the majority of studies focused on 5 SC in both Iran and other countries. Therefore, it can be concluded that the most important achievement of the TTM was the change in five-step behavior.
Table 3.
The aspects of TTM in various contexts
| Aspects | Subject area | Results |
|---|---|---|
| SC1/DB2 | Eating behavior | TTM3 has had positive results for understanding the PC4 in eating behaviors[29] |
| SC/SE5 | Physical activities in housewives | SE and SC play important roles in physical activities[32] |
| DB | Using vegetable and fruits | DB has increased by going from initial to final SC[31] |
| SC/DB/SE | Using contraceptives | There was a direct relation between using contraceptives and three factors of sexual behavior[30] |
| SC | Care methods for elderly | Most of the participants were in the stages of precontemplation, action, and maintenance[10] |
| SC | Physical activity in adults | People in action and maintenance stages had more positive than negative scores in different dimensions[11] |
| SC | Sleep in laborers | There is a direct relation between stages of change and sleep quality[12] |
| PC | Physical activity in college students | TTM is effective for changing the pattern of physical activity[28] |
| SC | Diet in students | Using vegetables and fruits was in line with SC[13] |
| SC/SE | Exercise behavior in students | The score for SE and advancement in SC had increases in participants after study[33] |
| SC | Exercise behavior in female students | Perceived SE, benefits, and use of PC increases by advancing through the SC[14] |
| SC | Using vegetable and fruit in elderly | Educational intervention showed significant results in using fruit and vegetables[15] |
| SC | Physical activity in pregnant women | The participants in test group showed positive and significant improvement in physical activities after intervention[16] |
| SC | Physical activities of operation room nurses | People in final SC had higher scores and perceived benefits[17] |
| SC | Using dairy products in students | The majority of participants were in the stage of contemplation and a small number were in the stage of precontemplation[18] |
| SC | Addictive behaviors | The majority of participants were in the stage of contemplation and a small number were in the stage of action[19] |
| SC | Quitting smoking in pregnant women | The desire for quitting smoking was reduced by advancing through the stages[20] |
| SE | Dental health in students | The SE score of women was higher than men; the majority of participants brush their teeth twice a day[35] |
| SC | Protection against the sun | After intervention, the advancement of participants through the stages increased[21] |
| SC | Physical activities in low-income population | People with better income situations are more likely to advance in the stages[27] |
| SC/SE/DB | Exercise behavior in nurses and midwives | The smallest number of participants were in the action and the majority were in the contemplation stage[34] |
| SC | Physical activity in mothers | There is a relation between physical activity and SC[22] |
| SC | Physical activity in pregnant women | The majority of participants were in the action and very few were in precontemplation stage[23] |
| SC | Chronic pain in children and teenagers | The parent version of the questionnaire was supported by four factors of precontemplation, contemplation, action, and maintenance, whereas the children version was supported by three factors mixing the scales for action and maintenance[24] |
| Motivational interview | Physical condition of nurses | SE and physical condition improved in intervention group compared with the control group[4] |
| SC | Physical activity | The scores of SC, SE, and DB increase in experiment group after intervention[25] |
| SC | Exercise behavior of students | The effectiveness of patterns in changing exercise behavior was proved[8] |
| SC | Physical activity in disabled individuals | There is a weak but meaningful relation between barriers of physical activity in disabled individuals and SC[26] |
1Stages of change, 2Decisional balance, 3Transtheoretical model, 4Process of change, 5Self-efficiency
Table 4a shows the extensive use of TTM in healthcare. These results show that the majority of studies applied TTM specifically for some chronic conditions such as inflammatory bowel disease,[36] type 2 diabetes,[37] cancer,[38] AIDS,[39] breast cancer,[40] osteoporosis,[41] high blood pressure,[42] and anorexia nervosa.[43] The results reported that TTM was used more in healthcare context than treatment and prevention of CDs. In healthcare context, TTM was used to change exercise behaviors,[8,44,45,46,47,48,49] change the attitude of diet behaviors,[50,51,52,53,54] addiction treatment behaviors,[55,56,57,58] air pollution prevention behaviors,[43] and oral health behaviors.[59]
Table 4a.
Use of TTM in changing the behavior of chorionic patients
| Disease | Pattern use | Results |
|---|---|---|
| IBD1 | Dividing the samples into experiment and control groups and using educational program for changing behavioral pattern in experiment group | Physical activities of experiment group increased after intervention[36] |
| Type 2 diabetes | Dividing the samples into intervention and control groups and routine care for intervention group based on TTM and SC | At the end of 47th week, blood sugar of the intervention group improved[37] |
| Cancer | Using a behavioral change questionnaire in healthy adults to determine the predictors of cancer prevention stages | There is a relation between cancer prevention behavior and SE[38] |
| HIV | Using behavioral change questionnaire to determine the addiction to antiretroviral drugs in HIV+patients | People in the initial stages had lower dependencies compared with patients in later stages[39] |
| Breast cancer | Using questionnaire to determine SC in self-examination of breast and dividing the samples into intervention and control groups and conducting educational program for the intervention group | The effectiveness of TTM-based educational program was confirmed[40] |
| Osteoporosis | Dividing the samples into intervention and control groups and using a questionnaire for calcium intake behavioral changes and TTM-based interviews with intervention group | The intervention was effective in improving the knowledge of intervention group about osteoporosis and calcium intake[41] |
| Hypertension | Dividing the samples into intervention and control groups and conducting motivational TTM interviews for intervention group | TTM-based motivational interviews are effective in reducing BP2[42] |
| Anorexia nervous | Using a checklist of SC, psychotherapy sessions, music therapy, etc. | Checklist can determine the danger of relapse to previous stages; contemplation stage is a positive predictor[43] |
1Irritated bowl syndrome, 2Blood pressure
Table 4b also describes some studies focusing on pros and cons of TTM.[8,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63] The results of these studies show evidence of TTM's success in treatment[54] and prevention of CDs.[59] However, few studies show some weakness of TTM effectiveness in various healthcare context such as quitting smoking,[62] diet intervention in diabetic patients,[60] and physical activities of youth.[63] Hence, it can be said that this pattern can be implemented in other areas and diseases with successful results.
Table 4b.
Advantages and disadvantages of TTM
| Pros | Cons | Pattern use method | Results |
|---|---|---|---|
| Positive influence of TTM on marijuana, cocaine, and opium addicts | - | An interview created based on five SC | People in precontemplation, contemplation, and preparation are more erratic[55] |
| Positive influence of TTM on predicting patterns of preventing confrontation with polluted air in pregnant women | - | Using a questionnaire to determine SC, advantages, barriers, and SE | SC, advantages, barriers, and SE are great predictors for prevention of confrontation with polluted air[61] |
| Positive influence of TTM on exercise behavior of students | - | Using a questionnaire to determine physical activity, SC, SE, and DB | There was a positive and significant relation between TTM patterns and exercise behavior[8] |
| Positive influence of TTM on improving physical activity and physical strength | - | Dividing the samples into intervention and control groups, using questionnaires and educational sessions | Physical activity and strength of intervention group increased after intervention[44] |
| - | Lack of effect of TTM on quitting smoking | Using SC questionnaire and educational pamphlets | No evidence of TTM being effective in people in the first three stages was observed[62] |
| - | Lack of effectiveness of TTM on diet intervention in diabetic patients | SR1 of Cochran, Sinhal, Medline, Sai Info, and UBase databases | Evidence of effectiveness of TTM on diet intervention of diabetic patients was not observed[60] |
| Positive influence of TTM in quitting smoking | - | Using SC questionnaire and selecting people in precontemplation, contemplation, and preparation stages | By advancing through the stages, the desire to smoke is reduced[56] |
| Positive influence of TTM on food fat intake | - | Using TTM questionnaire to determine all factors of the model | Evidence of predictive power and repeatability of TTM was gathered[50] |
| Positive influence of TTM on using vegetable and fruit in elderly | - | Dividing people into intervention and control groups, using TTM questionnaire and educational sessions | Average usage of vegetables, perceived benefits, and SE was increased[51] |
| Positive influence of TTM on physical activity | - | Using TTM questionnaire in telephone interviews | TTM patterns are useful for predicting SC[45] |
| Positive influence of TTM in physical activity of medical students | - | Dividing the samples into intervention and control groups, using TTM questionnaire, training sessions, and pamphlets | The scores of SC, DB, SE, and PC increased[46] |
| Positive influence of TTM on diet intervention | - | Using TTM questionnaire, dividing people into intervention and control groups, and conducting training sessions | Evidence of mediation role of TTM in diet interventions was provided[52] |
| Positive influence of TTM on physical activities | - | Using TTM questionnaire | By advancing through SC, the scores of perceived benefits and desire for physical activity increased[47] |
| Positive influence of TTM on physical activities | - | Using TTM questionnaire | The reasons for moving from precontemplation to contemplation are experience change and behavioral change, the reasons for moving from contemplation to preparation are PC and DB, the reason for moving from preparation to action stage is self-sufficiency; no factor affects moving from action to maintenance[48] |
| Positive influence of TTM on using vegetables of fruits | - | Using TTM questionnaire in a telephone interview | People were in the final stages of behavioral change processes[53] |
| Positive influence of TTM on changing smoking behavior | - | Using Iranian version of TTM questionnaire | This questionnaire is a credible tool for quitting smoking in Iranians[57] |
| Positive influence of TTM on physical activity behavior | - | SR of Sai Info, Science Direct, Web of Science, Scopus, and Sports Discus databases | Results showed significant effect of TTM on intervention group[49] |
| Positive influence of TTM on using dental floss in students | - | Using TTM questionnaire | Using dental floss is directly influenced by perceived benefits and SE[59] |
| Positive influence of TTM on smoking in male students | - | Using TTM questionnaire | People in the precontemplation stage were the least prepared for quitting smoking; the average SE and perceived benefit scores are related to advancement in stages[58] |
| Positive influence of TTM in behavioral change in eating disorders | - | SR of Google Scholar and Sai Info databases | There is a defined relation between initial SC and treatment results for eating disorders[54] |
| - | Lack of effectiveness of TTM on physical activities of youth | Using TTM questionnaire and educational sessions | Using TTM pattern was not effective for change in this population[63] |
1Systematic review
Discussion
The aim of this study was to conduct an SR on utility of the TTM in health behavioral change. Overall, the result of this study indicated the applicability of TTM for creating strong change in human behavior and increasing SE which can be applied in the prevention of CDs and can also corroborate the extended use of five SC. The results not only confirmed previous results but also lead to new information in this area which are mentioned below.
Applying different aspects of TTM
A large number of retrieved articles have used one of the aspects of TTM including SC, PC, DB, and SE. Noia et al. in their SR of selected databases showed the use for different aspects of this model in different subject areas. The results of their study showed that the most common aspect was the five SC.[29] Moattari et al. reported an increase in scores of SC, DB, and SE in nursing and midwifery students.[34] The results of this study also confirm the extended use of five SC.
The usage of TTM in CDs
The results of the review showed that only a small number of studies used this model for CDs. Despite this small number, these studies have led to positive and meaningful results. Lower popularity of this model for CDs can be due to unfamiliarity with this model and its use in medicine. Karimzadeh et al. in an intervention based on TTM on osteoporosis patients reported improved knowledge about increasing calcium levels and disease prevention.[39] It might be possible that the reason behind the low number of results regarding CDs is the fact that this study does not specifically target use of TTM in CDs.
The mentioned pros and cons of TTM
A small number of studies had led to negative results after using this model. Sanna Salmela et al. reported negative results in their SR of studies using TTM in diet studies for diabetic patients.[60] Most retrieved articles reported positive and significant results. Although many studies have been conducted on TTM and its uses, no study had specifically investigated the pros and cons of this model despite the fact that pros can lead to improved behavioral changes, whereas cons can lead to stagnation. Therefore, such studies seem necessary in this field. By knowing the possible cons of this model, it is possible to predict areas where this model is ineffective and knowing, different advantages this model can help determine what aspects of the model are useful in which condition. Restrictions existed on the full access to some databases such as Wiley and Ovid. Therefore, the research team selected the core and comprehensive databases that were used continuously and were readily accessible.
Based on the result of this study, there are insufficient studies in the application of TTM in health context. This study has also determined that few studies have used TTM in the prevention of CDs. The findings showed that TTM was not used at all for the prevention and treatment of obesity in children.
Conclusion
This review provided strong evidences for extended and effective use of TTM for changing health behaviors. According to the results, a large number of studies were about five SC, PC, DB, and SE. The majority of the current studies had investigated the five SC. Expertise behavior and physical activities were the areas in which the model was used most. Therefore, the effectiveness of TTM was proved in numerous studies while a small number of studies had reported some weakness of TTM.
Only a small number of studies had used TTM in CDs, but despite this low number, all these articles had reported positive results. Given the fact that chronic conditions are among important issues in society, it is suggested that this model can be used for areas such as obesity, multiple sclerosis, and problems in groups such as nurses who are in a greater danger of chronic conditions due to their occupation. Investigations showed that very few studies investigate the use of TTM in these areas. Therefore, it is suggested that more studies should be conducted in these subjects.
Financial support and sponsorship
Isfahan University of Medical Sciences
Conflicts of interest
Nothing to declare.
Acknowledgement
The authors would like to thank Dr. Gholamreza Asghari for comments on drafts.
References
- 1.Moradi A, Seyed Amini B, Malek, Ebrahimi M. Social problems in obese and overweight children. J Nur Mid. 2007;5:36–40. [Google Scholar]
- 2.Bogossian F, Hepworth J, Leong GM, Flaws DF, Gibbons KS, Benefer CA, et al. A cross-sectional analysis of patterns of obesity in a cohort of working nurses and midwives in Australia, New Zealand, and the United Kingdom. Int J Nurs Stud. 2012;49:727–38. doi: 10.1016/j.ijnurstu.2012.01.003. [DOI] [PubMed] [Google Scholar]
- 3.Kyle RG, Neall RA, Atherton IM. Prevalence of overweight and obesity among nurses in Scotland: A cross-sectional study using the Scottish Health Survey. Int J Nurs Stud. 2016;53:126–33. doi: 10.1016/j.ijnurstu.2015.10.015. [DOI] [PubMed] [Google Scholar]
- 4.Moazzami Z, Soltanian Ar. Correct body posture in nurse: An application of motivational interviewing. J Res Health. 2013;3:466–73. [Google Scholar]
- 5.Peikani FA, Shahgholian N, Kazemi A. The effect of health -beliefmodel based training on behaviors preventing peritonitis in patients on peritoneal dialysis. Int J Prev Med. 2018;9:49. doi: 10.4103/ijpvm.IJPVM_566_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Prochaska JO, Diclemente CC. Transtheoretical therapy: Toward a more integrative model of change. Psychother Theory Res Pract. 1982;19:276–88. [Google Scholar]
- 7.Prochaska JO, Velicer WF, Rossi JS, Goldstein MG, Marcus BH, Rakowski W, et al. Stages of change and decisional balance for 12 problem behavior. Health Psychol. 1994;13:39–46. doi: 10.1037//0278-6133.13.1.39. [DOI] [PubMed] [Google Scholar]
- 8.Farmanbar R, Niknami SH, R Lubans D, Hidarnia A. predicting exercise behavior in iranian college students: Utility of an integrated model of health behavior based on the transtheoretical model and self-determination theory. Health Educ J. 2011;72:56–69. [Google Scholar]
- 9.Rahimi A, Liaw ST, Ray P, Taggart J, Yu H. Ontological specification of quality of chronic disease data in EHRs to support decision analytics: A realist review. Decision Analytics. 2014:1. [Google Scholar]
- 10.Fried TR, Redding CA, Robbins ML, Paiva A, Oleary JR, Lannone L. Stages of change for the component behaviors of advance care planning. J Am Geriatr Soc. 2010;58:2329–36. doi: 10.1111/j.1532-5415.2010.03184.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parker PD, Martin AJ, Martinez C, Marsh HW, Jackson SA. Stages of change in physical activity: A validation study in late adolescence. Health Educ Behav. 2010;37:318–29. doi: 10.1177/1090198109333281. [DOI] [PubMed] [Google Scholar]
- 12.Hui SK, Grandner MA. associations between poor sleep quality and stages of change of multiple health behaviors among participants of employee wellness program. Prev Med Rep. 2015;1:292–99. doi: 10.1016/j.pmedr.2015.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Di Noia J, Mauriello L, Byrd-Bredbenner C, Thompson D. Validity and reliability of a dietary stages of change measure among economically disadvantaged African-American adolescents. Am J Health Promot. 2012;26:381–89. doi: 10.4278/ajhp.100903-QUAN-302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Khaniyan H, Hosseini M, Atashzadeh shorideh F, Chaibakhsh S. Understanding exercise behavior among Tehran adolescent girls according to stage of change model. Adv Nurs Midwifery. 2014;24:11–20. [Google Scholar]
- 15.Khezeli M, Ramezankhani A, Bakhtiyari M. Effect of education on nutritional knowledge and stages of fruit and vegatable intake in geriatrics according to stages of change model. JMUMS. 2012;22:88–98. [Google Scholar]
- 16.Solhi M, Ahmadi L, Taghdisi MH, Haghani H. The effect of transtheoretical model on exercise behavior in pregnant women reffered to dehaghan rural health center in. IJME. 2012;11:942–95. [Google Scholar]
- 17.Moazzami Z, Dehdari T, Taghdisi M, Soltanian A. Readiness to adapting correct posture in operating room nurses based on transtheoretical model in Hamadan city in 2011. JRJE. 2013;9:66–74. [Google Scholar]
- 18.Jafari F, Beladian Behbahan SE, Samadpour M, Kholdi N. Application of the stage of change model to dairy consumption among students of Shahrekord University of Medical Science. JSHUMS. 2013;15:65–74. [Google Scholar]
- 19.Campbell S, Bohanna I, Swinbourne A, Cadet-James Y, McKeown D, McDermott R. Stages of change, smoking behaviour and readiness to quit in a large sample of indigenous Australians living in eight remote north Queensland communities. Int J Environ Res Public Health. 2013;10:1562–71. doi: 10.3390/ijerph10041562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Buja A, Guarnieri E, Forza G, Tognazzo F, Sandra P, Zampieron A. Socio-demographic factors and processes associated with stages of change for smoking cessation in pregnant versus non-pregnant women. BMC Women's Health. 2011:11. doi: 10.1186/1472-6874-11-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Santiago-Rivas M, Velicer WF, Redding CA, Prochaska JO, Paiva AL. Outcomes of cluster profiles within stages of change for sun protection behavior. Psychol Health Med. 2013;18:471–81. doi: 10.1080/13548506.2012.748206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carlie J, Jancey J, Howat P, Dhaliwal S, Burns SH, Mcmanus A, et al. Utility of stages of change construct in the planning of physical interventions among playgroup mothers. BMC Res Notes. 2013:300. doi: 10.1186/1756-0500-6-300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Haakstad LAH, Voldner N, Bo K. Stages of change model for participation in physical activity during pregnancy. J Pregnancy. 2013 doi: 10.1155/2013/193170. doi: 10.1155/2013/193170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Guite JW, Logan DE, Simons LE, Blood EA, Kerns RD. Readiness to change in pediatric chronic pain: Initial validation of adolescent and parent versions of the pain stages of change questionnaire. Pain. 2011;152:2301–11. doi: 10.1016/j.pain.2011.06.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moeini B, Rahimi M, Hazaveie SM, Allahverdipour H, Moghim Beigi A, Mohammadfam I. Effect of education based on transtheoretical model on promoting physical activity and increasing physical work capacity. J Mill Med. 2012;12:123–30. [Google Scholar]
- 26.Ashrafi S, Kashef SM, Seyed Ameri MH. The relationship between disincentive factors of physical activity and athletic behavior variation in disables and maims in urmia city. Appl Res Sport Manage. 2014;2:115–28. [Google Scholar]
- 27.Callaghan P, Khalil E, Morres I. A prospective evaluation of the transtheoretical model of change applied to exercise in young people. Int J Nurs Stud. 2010;47:3–12. doi: 10.1016/j.ijnurstu.2009.06.013. [DOI] [PubMed] [Google Scholar]
- 28.Dishman RK, Jackson AS, Bray MS. Validity of processes of change in physical activity among college students in the TIGER study. Ann Behav Med. 2010;40:164–75. doi: 10.1007/s12160-010-9208-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Di Noia J, Prochaska JO. Dietary stages of change and decisional balance: A meta-analytic review. Am J Health Behav. 2010;34:618–32. doi: 10.5993/ajhb.34.5.11. [DOI] [PubMed] [Google Scholar]
- 30.Gullette DL, Wright PB, Booth BM, Feldman Z, Stewart KE. Stages of change, decisional balance, and self-efficacy in condom use among rural African-American stimulant users. J Assoc Nurses AIDS Care. 2009;20:428–41. doi: 10.1016/j.jana.2009.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mainvil LA, Lawson R, Horwath CC, Mckenzie JE, Hart I. Validated scales to assess adult decisional balance to eat more fruits and vegetables. Appetite. 2010;55:454–65. doi: 10.1016/j.appet.2010.08.007. [DOI] [PubMed] [Google Scholar]
- 32.Hashemi Z, Rakhshani F, Keykhai R, Tirzir A, Zareban E. Relationship between self- efficacy with physical activity stage of change in housewives. J Res Health. 2013;3:363–69. [Google Scholar]
- 33.Asadpour M, Sheikh Fathollahi M, Goujani R, Razi S, Torkashvand F, Hassanloei B, et al. Survey on physical exercise among paramedical students of rafsanjan University of Medical Science based on stages of change model and its association with self-efficacy in 2011-2012. JRUMS. 2014;13:349–60. [Google Scholar]
- 34.Moattari M, Shafakhah M, Sabet Sarvestani R. Assessing stages of exercise behavior change, self efficacy and decisional balance in Iranian nursing and midwifery students. IJCBNM. 2013:1. [Google Scholar]
- 35.Mizutani S, Ekuni D, Furuta M, Tomofuji T, Irie K, Azuma T, et al. Effects of self-efficacy on oral health behaviors and gingival health in university students aged 18 or 19 year old. J Clin Periodontol. 2012;39:844–9. doi: 10.1111/j.1600-051X.2012.01919.x. [DOI] [PubMed] [Google Scholar]
- 36.Mardani Hamule M, Shahraky Vahed A, Moshtagh Eshgh Z. Assessment of the effect of educational program based on transtheoretical model on physical activity in patients with inflammatory bowel diseases. Sci J Hamadan Univ Med Sci. 2010;17:39–45. [Google Scholar]
- 37.Partapsingh VA, Maharaj RG, Rawlins JM. Applying the stages of change model to type 2 diabetes care in Trinidad: A randomised trial. J Negat Results Biomed. 2011:10. doi: 10.1186/1477-5751-10-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Choi JH, Chung KM, Park K. Psychosocial predictors of four health-promoting behaviors for cancer prevention using the stage of change of transtheoretical model. Psychooncology. 2013;22:2253–61. doi: 10.1002/pon.3278. [DOI] [PubMed] [Google Scholar]
- 39.Genberg BL, Lee Y, Rogers WH, Willey C, Wilson IB. Stages of change for adherence to antiretroviral medications. AIDS Patient Care STDS. 2013;27:567–72. doi: 10.1089/apc.2013.0126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pourhaji F, Vahedian Shahroodi M, Esmaily H, Harooni J. Effects of training program based on stage of change model to promote breast self-examination behavior. Sci J Hamadan Nurs Midwifery Fac. 2013;21:59–68. [Google Scholar]
- 41.Karimzadeh shirazi K, Niknami S, Rahimi E. Using intervention mapping to develop a tailored health education program based on stages of change to prevent osteoporosis. J Res Health. 2014;4:795–802. [Google Scholar]
- 42.Navidian A, Abedi MR, Baghbani I, Fatehizadeh M, Poursharifi H. Effect of motivational interviewing on blood pressure of referents suffering from hypertention. Kowsar Med J. 2010;15:115–21. [Google Scholar]
- 43.Mander J, Teufel M, Keifenheim K, Zipfel S, Giel KE. Stages of change treatment outcome and therapeutic alliance in adult in patients with chronic anorexia nervosa. BMC Psychiatry. 2013:111. doi: 10.1186/1471-244X-13-111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Moeini B, Hazaveie S, Allahverdipour H, Moghimbeygi A, Mohammadfam I. Effect of education based on transtheoretical model on promoting physical activity and increasing physical work capacity. Iran J Mil Med. 2010;12:123–30. [Google Scholar]
- 45.Dishman RK, Vandenberg RJ, Motl RW, Nigg CR. Using constructs of the transtheoretical model to predict classes of change in regular physical activity: A multi-ethnic longitudinal cohort study. Ann Behav Med. 2010;40:150–63. doi: 10.1007/s12160-010-9196-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Pirasteh A, Davati A, Jouhari Z, Mohamadi L. Predicting physical activity behavior among Iranian medial college students using the transtheoretical model. Daneshvarmed. 2012;19:1–10. [Google Scholar]
- 47.Mohammadi M, Mehri A. Application of the transtheoretical model to predict exercise activties in the students of Islamic Azad University of Sabzevar. AUMS. 2012;1:85–92. [Google Scholar]
- 48.Jeon DJ, Kim KJ, Heo M. Factors related to stages of exercise behavior change among university students based on the transtheoretical model. J Phys Ther Sci. 2014;26:1929–32. doi: 10.1589/jpts.26.1929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hutchison AJ, Breckon JD, Johnston LH. Physical activity behavior change interventions based on the transtheoretical model: A systematic review. Health Educ Behav. 2009;36:829–45. doi: 10.1177/1090198108318491. [DOI] [PubMed] [Google Scholar]
- 50.Wright JA, Velicer WF, Prochaska JO. Testing the predictive power of the transtheoretical model of behavior change applied to dietary fat intake. Health Educ Res. 2009;24:224–36. doi: 10.1093/her/cyn014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Salehi L, Solki S, Montazeri A. Effectiveness of an educational program based on transtheoretical model on fruit and vegetable consumption. PAYESH. 2014;13:51–60. [Google Scholar]
- 52.Di Noia J, Prochaska JO. Mediating variables in a transtheoretical model dietary intervention program. Health Educ Behav. 2010;37:753–62. doi: 10.1177/1090198109334897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Horwath CC, Schembre SM, Motl RW, Dishman RK, Nigg CR. Does the transtheoretical model of behavior change provide a useful basis for interventions to promote fruit and vegetable consumption? Am J Health Promot. 2013;27:351–7. doi: 10.4278/ajhp.110516-QUAN-201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dray J, Wade TD. Is the transtheoretical model and motivational interviewing approach applicable to the treatment of eating disorders? A review. Clin Psychol Rev. 2012;32:558–65. doi: 10.1016/j.cpr.2012.06.005. [DOI] [PubMed] [Google Scholar]
- 55.Harrell PT, Trenz RC, Scherer M, Martins SS, Latimer WW. A latent class approach to treatment readiness corresponds to transtheoretical ("stages of change") model. J Subst Abuse Treat. 2013;45:249–56. doi: 10.1016/j.jsat.2013.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Girma E, Assefa T, Deribew A. Cigarette smokers intention to quit smoking in Dire Dawa town Ethiopia: An assessment using the transtheoretical model. BMC Public Health. 2010:10. doi: 10.1186/1471-2458-10-320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sarbandi F, Niknami SH, Hidarnia A, Hajizadeh E, Montazari A. The transtheoretical model questionnaire for smoking cessation: Psychometric properties of the Iranian version. BMC Public Health. 2013:13. doi: 10.1186/1471-2458-13-1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Sharifi Rad GH, Charkazi A, Shahnazi H, Kouchaki GHM, Orouj MA, Ekrami Z. Smoking behavior among male students based on transtheoretical model. Q J Fundam Mental Health. 2012;13:386–95. [Google Scholar]
- 59.Mazloomi Ma S, Kamali Khah T, Rahmati Najarkolaei F, Karimi M. Assessment of determinant factors of dental flossing based on transtheoretical model in Pakdasht high school students in 2012. TB. 2014;13:12–24. [Google Scholar]
- 60.Salmela S, Poskiparta M, Kasila K, Vähäsarja K, Vanhala M. Transtheoretical model-based dietary interventions in primary care: A review of the evidence in diabetes. Health Educ Res. 2009;24:237–52. doi: 10.1093/her/cyn015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Leonard T, Shuval K, de Oliveira A, Skinner CS, Eckel C, Murdoch JC. Health behavior and behavioral economics: Economic preferences and physical activity stages of change in a low-income African American community. Am J Health Promot. 2013;27:211–21. doi: 10.4278/ajhp.110624-QUAN-264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Araban M, Tavafian SS, Motesaddizarandi S, Hidarnia A, Gohari MR, Labie A, et al. Predictors of air pollution exposure behavior among pregnant women: A transtheoretical model based study. Know Health. 2013;8:83–8. [Google Scholar]
- 63.Aveyard P, Massey L, Parsons A, Manaseki S, Griffin C. The effect of transtheoretical model based interventions on smoking cessation. Soc Sci Med. 2009;68:397–403. doi: 10.1016/j.socscimed.2008.10.036. [DOI] [PubMed] [Google Scholar]