

Abstract
Background:
Tendon overuse injuries are an issue in elite footballers (soccer players) and may affect tendon function. Achilles and patellar tendinopathy are the most frequent pathologies. Tendon stiffness, the relationship between the force applied to a tendon and the displacement exerted, may help represent tendon function. Stiffness is affected by training and pathology. Nevertheless, information regarding this mechanical property is lacking for elite soccer athletes.
Hypothesis:
Achilles and patellar tendon stiffness assessed using myotonometric measurements will be greater in elite soccer athletes than in control participants.
Study Design:
Cross-sectional study.
Level of Evidence:
Level 4.
Methods:
Forty-nine elite soccer athletes and 49 control participants were evaluated during the 2017 preseason. A handheld device was used to measure Achilles and patellar tendon stiffness. Dominant and nondominant limbs were assessed for both groups.
Results:
A significantly stiffer patellar tendon was found for both the dominant and the nondominant limb in the elite soccer athletes compared with the control group. Nevertheless, no differences were found in Achilles tendon stiffness between groups. When comparing between playing positions in soccer athletes, no significant differences were found for both tendons.
Conclusion:
Greater patellar tendon stiffness may be related to an improvement in force transmission during muscle contraction. On the other hand, it seems that after years of professional training, Achilles tendon stiffness does not change, conserving the storing-releasing function of elastic energy. The nonsignificant differences between positions may be attributable to the years of homogeneous training that the players underwent.
Clinical Relevance:
The present study shows another technique for measuring mechanical properties of tendons in soccer athletes that could be used in clinical settings. In the future, this technique may help clinicians choose the best exercise protocol to address impairments in tendon stiffness.
Keywords: tendon stiffness, elite soccer athletes, soccer, myotonometric measurements, patellar tendon, Achilles tendon
Football (soccer) is the world’s most popular sport, with approximately 265 million players worldwide.13 Injuries in soccer are common, with a rate of 2.6 injuries per match being reported during international elite tournaments.23 Particularly, overuse injuries are a major problem in soccer, accounting for almost one-third of the injury incidence.37 A prevalence of 13.5% for patellar tendinopathy has been reported in soccer athletes, possibly resulting from the high demands on speed and power for the leg extensors30; ankle and knee sprains and hamstrings strains show a higher prevalence (32.2% and 18.1%, respectively).1 Patellar tendinopathy can result from long-standing absence from competition.5 On the other hand, Achilles tendon (AT) injuries are also common, and it has been shown that 96% of AT injuries correspond with tendinopathy.17,22 Thus, tendon pathology appears to be of importance in elite soccer athletes.
Tendons are responsible for transmitting force produced by muscles and for storing and releasing elastic energy during movement.34 This double function is highly important during the muscle-tendon interaction, allowing for efficient functioning of the muscle-tendon complex (MTC) in human movements.16,33 Tendon function can be assessed mechanically through the use of dynamometry combined with ultrasonography, known as “in vivo” assessment.42 Stiffness, the relationship between the force applied to a tissue and the displacement exerted, is one of the mechanical properties most reported in tendon function assessment in either passive15 or active conditions.25 Tendon stiffness has been widely used to represent changes in the mechanical properties of tendons after training or in the presence of pathology. Greater stiffness values have been found in participants who underwent short-term–specific load-training programs.3,43 Moreover, stiffer tendons have been found in athletes who have been training for years (ie, long-term training), highlighting that tendons adapt to short- or long-term training regimens.20 Alterations of mechanical properties have also been found in pathological stages such as tendinopathy. Patellar tendon (PT) and AT pathologies have shown lower stiffness values than those for normal tendons, which affects the transmission of force through the tendon.2,7 Although muscle force production may be normal, altered transmission may affect motor output.40 Therefore, assessment of tendon stiffness is needed to understand tendon function during training adaptation and to optimize rehabilitation in pathological stages.
Although dynamometry combined with ultrasonography is the gold standard to measure passive tendon stiffness, it is an expensive and operator-dependent technique that can only be used in laboratory settings. Recently, another technique has been reported that evaluates the mechanical properties of tendons.9,11 Myotonometric measurement is a noninvasive and painless technique based on free oscillation theory where a brief mechanical impulse is realized over the skin using a probe, and parameters, such as stiffness, can be obtained.12 Nevertheless, studies that used myotonometric measurements have mainly measured muscle properties,19,36 and only a few have measured tendon stiffness.39 Hence, more studies assessing tendon stiffness by myotonometric measurements are needed.
The main aims of this study were to describe the mechanical properties (stiffness) of the PT and AT in elite soccer athletes using myotonometric measurements and to compare the results with a healthy control group. A second aim was to compare PT and AT stiffness between playing positions among the soccer athletes. Data regarding tendon stiffness could be used to improve training program design, to create prevention strategies in overuse tendon injuries, and to optimize rehabilitation in tendon pathology.
Methods
Participants
A total of 49 elite soccer athletes were recruited during the offseason from 3 different soccer clubs. Players underwent a clinical interview to determine eligibility. Participant inclusion criteria included the following: normal training regimen in the past 6 months, and no history or symptoms of PT and AT or surgery. Exclusion criteria were as follows: history of quadriceps and triceps sural muscle strain in the past 6 months, and history of knee or ankle surgery in the past year. A group of 49 healthy participants was also recruited using the following inclusion criteria: not having been an elite athlete, and no history or symptoms of PT and AT. The exclusion criteria for this second group were as follows: history of quadriceps and triceps sural muscle strain in the past 6 months, and history of knee or ankle surgery in the past year. Anthropometric characteristics for each group are provided in Table 1. All participants provided their signed informed consent before participating in this study, which was approved by the bioethics committee of the university and conducted in accordance with the Declaration of Helsinki.
Table 1.
Demographic characteristics by group a
| Elite Soccer Players (n = 49) | Control Group (n = 49) | P | |
|---|---|---|---|
| Age, y | 24.59 (5.22) | 25.90 (3.86) | 0.16 |
| Mass, kg | 73.94 (6.27) | 74.04 (8.19) | 0.94 |
| Height, m | 1.76 (0.06) | 1.75 (0.08) | 0.44 |
| Body mass index, kg/m2 | 23.67 (0.98) | 24.01 (1.76) | 0.24 |
Demographic characteristics by group are presented as mean (SD). No significant intergroup differences (P > 0.05) were observed.
Outcomes
The PT and AT were assessed using myotonometric measurements with the MyotonPRO device (Myoton Ltd). The measuring method of the device is based on the free oscillation technique, where the following steps occur during a single measurement: (1) the device is placed perpendicular to the skin and a constant pre-pressure is applied for compressing the subcutaneous tissue; (2) a brief mechanical impulse is applied, causing damped oscillation of the tissue; and (3) the co-oscillation generated in the tissue is recorded by an accelerometer. The raw signal is then processed to filter the frequencies that are not characteristic of the tissue’s natural oscillation, and finally, the filtered acceleration curve is used to calculate the mechanical and viscoelastic properties of the tissue.18 Further information regarding the free oscillation theory can be found in the study by Ditroilo et al.12
From the obtained filtered signal, stiffness can be mathematically inferred from the filtered curve. Stiffness was obtained as follows:
where a0 is the maximal acceleration of the curve (first negative peak), mProbe is the mass of the measurement mechanism (probe), and ∆l is the maximal displacement of the tissue (Figure 1), obtained by double integration of the acceleration curve. The MyotonPRO has good to excellent test-retest reliability and has been established in previous literature.8,29
Figure 1.
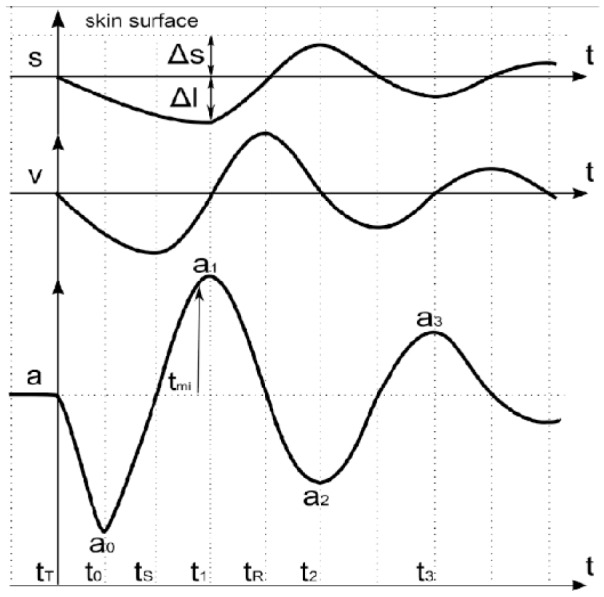
Obtained filtered acceleration curve. Displacement and velocity curves are obtained by double integrating the acceleration curve. (Reproduced with permission from MyotonPRO User Manual.)
Design and Procedures
Measures were performed during the preseason (January-February 2017), and all measurements were conducted at the MEDS Clinic. The anatomical landmark for the PT stiffness assessment was 3 cm below the inferior pole of the patella. The participants sat with their knees flexed to 90° (Figure 2A). For AT, the measure point was 4 cm above the distal insertion of the tendon (ie, calcaneal tuberosity). The participants lay prone with their ankles in a neutral position (approximately 90°) (Figure 2B). For both tendons, the myotonometric evaluation was repeated 3 times per extremity. Only measures that had a coefficient of variation lower than 3% were considered; otherwise, the measured was repeated. The dominant limb was selected as the one used for kicking the ball.4
Figure 2.

Patellar tendon and Achilles tendon assessment. (a) Position of the participant during stiffness assessment of the patellar tendon. Players were relaxed and sat with their knees in 90° of flexion. (b) Position of the participant during stiffness assessment of the Achilles tendon. Players were relaxed and lay on a stretcher with their ankles in neutral position (approximately 90°).
Statistical Analysis
Sample size was calculated based on a difference of 139 N/m in PT stiffness between athletes and control participants from previous studies that took place in our laboratory. This is equivalent to a moderate effect size (0.75) using an α = 0.05 and β = 0.20, and a sample size of 30 participants per group was required.38 Since estimates on this outcome were not available in the literature, we decided to be conservative, and thus we recruited 49 participants per group.
Statistical analyses were performed using SPSS v 20.0 software (IBM Corp). The Shapiro-Wilk test was applied to determine the normality of data. Means and SDs were used to describe the obtained data. Unpaired t tests were used for between-group comparisons, and paired t tests were used for within-group comparisons. A 1-way analysis of variance was performed to compare AT and PT stiffness between playing positions of the soccer athletes. The Bartlett test was applied to analyze the equality of the variance. Goalkeepers were excluded from this analysis because of the small sample size. The level of significance was set at α = 0.05.
Results
PT Stiffness
PT stiffness in elite soccer athletes was 1138.0 ± 215.5 and 1118.0 ± 199.1 N/m for the dominant and nondominant limbs, respectively (Figure 3). PT stiffness for healthy controls was 897.7 ± 190.1 and 871.1 ± 178.5 N/m for the dominant and nondominant limbs, respectively (Figure 3). Significant differences were found between groups for the dominant (P = 0.0001) and nondominant limbs (P = 0.0001). No significant differences were found for the within-limb comparison in each group (elite soccer athletes, P = 0.336; healthy controls, P = 0.210).
Figure 3.

Patellar tendon and Achilles tendon stiffness for both groups, football (soccer athlete) and control. Significant intergroup differences (*P < 0.05) can be observed.
AT Stiffness
AT stiffness in elite soccer athletes was 1075.0 ± 100.8 and 1031.0 ± 115.9 N/m for the dominant and nondominant limbs, respectively (Figure 3). AT stiffness for healthy controls was 1098.0 ± 139.5 and 1072.0 ± 112.3 N/m for the dominant and nondominant limbs, respectively (Figure 3). No significant differences were found in the between-group comparison for the dominant (P = 0.220) and nondominant limbs (P = 0.054) (Figure 3). Additionally, no significant differences were found in the within-limb comparison in each group (elite soccer athletes, P = 0.051; healthy controls, P = 0.096).
AT and PT Stiffness by Position
No significant differences were found for PT and AT stiffness values between playing positions of the soccer players (Table 2).
Table 2.
Patellar tendon and Achilles tendon stiffness by position a
| Tendon | Dominance | Goalkeepers (n = 4) | Defenders (n = 17) | Midfielders (n = 16) | Strikers (n = 12) | F | P |
|---|---|---|---|---|---|---|---|
| Patellar tendon stiffness (N/m) | Dominant | 1349 (163.2) | 1143 (241.3) | 1051 (179.9) | 1179 (193.4) | 1.46 | 0.24 |
| Nondominant | 1120 (130.3) | 1128 (189.4) | 1074 (226.7) | 1163 (201.9) | 0.67 | 0.51 | |
| Achilles tendon stiffness (N/m) | Dominant | 1136 (76.7) | 1107 (117.5) | 1043 (87.27) | 1052 (84.8) | 2.01 | 0.14 |
| Nondominant | 1086 (99.7) | 1042 (126.9) | 1000 (114.2) | 1039 (109.2) | 0.62 | 0.54 |
All values are presented as mean (SD). No significant differences (P > 0.05) can be observed for the comparison between playing positions.
Discussion
The aim of this study was to describe PT and AT stiffness in elite soccer athletes and to compare these results with a control group. The results indicate that elite soccer athletes have stiffer PTs than controls in both limbs—dominant and nondominant. However, AT stiffness seems to be similar for both groups. Previous studies have evaluated AT stiffness in karate competitors and reported lower AT stiffness values than those obtained in the present study.39 A possible reason for this may be the different mechanical demands exerted in karate and soccer. Thus, mechanical adaptation of tendons may be different.
PT Stiffness
Elite soccer athletes showed greater PT stiffness values than the control group. This could be explained by the well-documented phenomenon of tendon adaptation to training.3,43 Previous studies using in vivo assessment have shown stiffer PT values after short-term training regimens (12 weeks).26,35 Similar results have been reported in long-term training.20 Although there is no clear training modality (eg, resistance, plyometric, or endurance) that contributes less/more to this stiffening process, it seems to be a homogeneous adaptation over time. Moreover, the PT has been described as a transmission force tendon rather than an elastic energy store-release tendon.6 Elite soccer athletes are subjected to long-term training, including the aforementioned different training modalities. Thus, PT stiffening seems to be an adaptation process that may enhance force transmission and sports performance. Therefore, myotonometric measuring seems to show a sensitivity to changes in PT stiffness, and the presented adaptations were similar to those reported in the literature.
AT Stiffness
No differences were found in AT stiffness between groups. Evidence related to AT adaptation after training (short term or long term) and its relationship with performance in different disciplines is controversial. A few studies have reported that long-distance runners with the best records in a 5000-m race presented lower AT stiffness values than those with the worst records.27,28 Nevertheless, other studies have shown that middle- and long-distance runners with the best running economy or the best records had stiffer ATs.14,41 Thus, there is no clear relationship between AT stiffness and performance. Because of the nature of the triceps sural MTC and its function in the storing and releasing of elastic energy, no difference in AT stiffness may facilitate this function, and it could be explained by the interaction between muscle and tendon during movement.
The interaction of muscle and tendon during human movement is complex. To understand the nature of the MTC it is necessary to distinguish the changes in the fascicle and tendon length through different movements.16 In particular, the triceps sural MTC has been widely studied in different tasks, such as gait, running, and jumping. During the stance phase of gait, an isometric contraction of the gastrocnemius fascicle was observed along with elongation of the AT.21,24 Also, during the stance phase of running and a squat-jump task, shortening of the gastrocnemius fascicles (ie, concentric contraction) and AT elongation have been observed.31,32 These behaviors optimize the mechanical function of the triceps surae MTC by 2 mechanisms: (1) AT elongation allows efficient storage and release of elastic energy, and (2) no elongation of muscular fascicles enables them to work in the most efficient zone of the force-velocity curve.16 Hence, no changes in AT stiffness for the elite soccer athletes compared with controls may mean that this mechanism of interaction is maintained between fascicles and tendinous tissue. Thus, other adaptations (eg, neuromuscular adaptations) may play a key role in the maintenance of this mechanism.
AT and PT Stiffness by Position
Statistical analysis showed no significant differences in AT and PT stiffness between playing positions among the soccer athletes. Physical demands and position characteristics have been reported to be different from one another. It has been shown that midfield players cover significantly greater distances and display higher work rates than players in other positions.10 Although players in other positions may display different physical demands, the loads and the training dosage that they were subjected to during years of professional training would be the same. This means that, from a purely mechanical perspective, it can be hypothesized that both tendons adapted to similar mechanical demands after long-term training.20 Therefore, the observed stiffness values may be enough to fulfill the physical demands of soccer, even if there are differences in work rates between playing positions. Overall, the differences in physical demands of each position (ie, different loads and workrates) may not influence the stiffness of both tendons, resulting in similar tendon stiffness throughout the different playing positions.
Strengths and Limitations
Nowadays, the widely accepted methods for measuring tendon mechanical properties are dynamometry and ultrasonography.42 The present study shows another technique that could be used in the clinical setting and may help clinicians in deciding the best exercise protocol to address impairments in tendon stiffness. Moreover, the obtained AT and PT stiffness values could be used as normative values, especially to compare pathological stages (ie, tendinopathy).
There are 2 main limitations to the present study. First, the cross-sectional study design did not allow measurement of PT and AT adaptation to training and changes associated with pathology. Prospective studies using this method are needed for a better understanding of the mechanical properties of the tendon. Second, the estimated sample size may influence the results of the present study. No previous study has measured PT or AT stiffness in elite soccer athletes; thus, the estimated sample size may influence the obtained nonsignificant differences for the within-limb comparisons as well as those between playing positions. Future studies should use a larger sample size.
Conclusion
A stiffer PT may be related to an improvement in force transmission during human movement. This adaptation could be associated with the long-term practices that soccer players undergo during years of professional training. Conversely, no difference was found in AT stiffness between groups. The AT storing-releasing of elastic energy is a main function during human movements; thus, an increase in AT stiffness is not needed to preserve this function after years of training. No differences were found in PT and AT stiffness with regard to playing position, which may be explained by the standardized and long-term training that the soccer athletes endured. More studies assessing tendon stiffness using myotonometric measurements are needed.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Aoki H, O’Hata N, Kohno T, Morikawa T, Seki J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am J Sports Med. 2012;40:1006-1014. [DOI] [PubMed] [Google Scholar]
- 2. Arya S, Kulig K. Tendinopathy alters mechanical and material properties of the Achilles tendon. J Appl Physiol (1985). 2010;108:670-675. [DOI] [PubMed] [Google Scholar]
- 3. Bohm S, Mersmann F, Arampatzis A. Human tendon adaptation in response to mechanical loading: a systematic review and meta-analysis of exercise intervention studies on healthy adults. Sports Med Open. 2015;1:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Brophy R, Silvers HJ, Gonzales T, Mandelbaum BR. Gender influences: the role of leg dominance in ACL injury among soccer players. Br J Sports Med. 2010;44:694-697. [DOI] [PubMed] [Google Scholar]
- 5. Cook J, Khan K, Harcourt P, Grant M, Young D, Bonar S. A cross sectional study of 100 athletes with jumper’s knee managed conservatively and surgically. The Victorian Institute of Sport Tendon Study Group. Br J Sports Med. 1997;31:332-336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Couppe C, Hansen P, Kongsgaard M, et al. Mechanical properties and collagen cross-linking of the patellar tendon in old and young men. J Appl Physiol (1985). 2009;107:880-886. [DOI] [PubMed] [Google Scholar]
- 7. Chang YJ, Kulig K. The neuromechanical adaptations to Achilles tendinosis. J Physiol. 2015;593:3373-3387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Chuang LL, Lin KC, Wu CY, et al. Relative and absolute reliabilities of the myotonometric measurements of hemiparetic arms in patients with stroke. Arch Phys Med Rehabil. 2013;94:459-466. [DOI] [PubMed] [Google Scholar]
- 9. Chuang LL, Wu CY, Lin KC. Reliability, validity, and responsiveness of myotonometric measurement of muscle tone, elasticity, and stiffness in patients with stroke. Arch Phys Med Rehabil. 2012;93:532-540. [DOI] [PubMed] [Google Scholar]
- 10. Di Salvo V, Baron R, Tschan H, Montero FC, Bachl N, Pigozzi F. Performance characteristics according to playing position in elite soccer. Int J Sports Med. 2007;28:222-227. [DOI] [PubMed] [Google Scholar]
- 11. Ditroilo M, Cully L, Boreham CA, De Vito G. Assessment of musculo-articular and muscle stiffness in young and older men. Muscle Nerve. 2012;46:559-565. [DOI] [PubMed] [Google Scholar]
- 12. Ditroilo M, Watsford M, Murphy A, De Vito G. Assessing musculo-articular stiffness using free oscillations: theory, measurement and analysis. Sports Med. 2011;41:1019-1032. [DOI] [PubMed] [Google Scholar]
- 13. Faude O, Junge A, Kindermann W, Dvorak J. Injuries in female soccer players: a prospective study in the German national league. Am J Sports Med. 2005;33:1694-1700. [DOI] [PubMed] [Google Scholar]
- 14. Fletcher JR, Esau SP, MacIntosh BR. Changes in tendon stiffness and running economy in highly trained distance runners. Eur J Appl Physiol. 2010;110:1037-1046. [DOI] [PubMed] [Google Scholar]
- 15. Fouré A, Nordez A, McNair P, Cornu C. Effects of plyometric training on both active and passive parts of the plantarflexors series elastic component stiffness of muscle-tendon complex. Eur J Appl Physiol. 2011;111:539-548. [DOI] [PubMed] [Google Scholar]
- 16. Fukunaga T, Kawakami Y, Kubo K, Kanehisa H. Muscle and tendon interaction during human movements. Exerc Sport Sci Rev. 2002;30:106-110. [DOI] [PubMed] [Google Scholar]
- 17. Gajhede-Knudsen M, Ekstrand J, Magnusson H, Maffulli N. Recurrence of Achilles tendon injuries in elite male football players is more common after early return to play: an 11-year follow-up of the UEFA Champions League injury study. Br J Sports Med. 2013;47:763-768. [DOI] [PubMed] [Google Scholar]
- 18. Gapeyeva H, Vain A. Methodical Guide: Principles of Applying Myoton in Physical Medicine and Rehabilitation. Tartu, Estonia: Muomeetria; 2008. [Google Scholar]
- 19. Gervasi M, Sisti D, Amatori S, et al. Muscular viscoelastic characteristics of athletes participating in the European Master Indoor Athletics Championship. Eur J Appl Physiol. 2017;117:1739-1746. [DOI] [PubMed] [Google Scholar]
- 20. Heinemeier K, Kjaer M. In vivo investigation of tendon responses to mechanical loading. J Musculoskelet Neuronal Interact. 2011;11:115-123. [PubMed] [Google Scholar]
- 21. Ishikawa M, Komi PV, Grey MJ, Lepola V, Bruggemann GP. Muscle-tendon interaction and elastic energy usage in human walking. J Appl Physiol (1985). 2005;99:603-608. [DOI] [PubMed] [Google Scholar]
- 22. Järvinen TA, Kannus P, Maffulli N, Khan KM. Achilles tendon disorders: etiology and epidemiology. Foot Ankle Clin. 2005;10:255-266. [DOI] [PubMed] [Google Scholar]
- 23. Junge A, Dvorak J. Injury surveillance in the world football tournaments 1998-2012. Br J Sports Med. 2013;47:782-788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Kawakami Y, Muraoka T, Ito S, Kanehisa H, Fukunaga T. In vivo muscle fibre behaviour during counter-movement exercise in humans reveals a significant role for tendon elasticity. J Physiol. 2002;540:635-646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kongsgaard M, Nielsen C, Hegnsvad S, Aagaard P, Magnusson S. Mechanical properties of the human Achilles tendon, in vivo. Clin Biomech (Bristol, Avon). 2011;26:772-777. [DOI] [PubMed] [Google Scholar]
- 26. Kubo K, Kanehisa H, Ito M, Fukunaga T. Effects of isometric training on the elasticity of human tendon structures in vivo. J Appl Physiol (1985). 2001;91:26-32. [DOI] [PubMed] [Google Scholar]
- 27. Kubo K, Miyazaki D, Shimoju S, Tsunoda N. Relationship between elastic properties of tendon structures and performance in long distance runners. Eur J Appl Physiol. 2015;115:1725-1733. [DOI] [PubMed] [Google Scholar]
- 28. Kubo K, Tabata T, Ikebukuro T, Igarashi K, Yata H, Tsunoda N. Effects of mechanical properties of muscle and tendon on performance in long distance runners. Eur J Appl Physiol. 2010;110:507-514. [DOI] [PubMed] [Google Scholar]
- 29. Li X, Shin H, Li S, Zhou P. Assessing muscle spasticity with myotonometric and passive stretch measurements: validity of the myotonometer. Sci Rep. 2017;7:44022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Lian ØB, Engebretsen L, Bahr R. Prevalence of jumper’s knee among elite athletes from different sports: a cross-sectional study. Am J Sports Med. 2005;33:561-567. [DOI] [PubMed] [Google Scholar]
- 31. Lichtwark GA, Bougoulias K, Wilson A. Muscle fascicle and series elastic element length changes along the length of the human gastrocnemius during walking and running. J Biomech. 2007;40:157-164. [DOI] [PubMed] [Google Scholar]
- 32. Lichtwark GA, Wilson A. Optimal muscle fascicle length and tendon stiffness for maximising gastrocnemius efficiency during human walking and running. J Theor Biol. 2008;252:662-673. [DOI] [PubMed] [Google Scholar]
- 33. Lichtwark GA, Wilson AM. Interactions between the human gastrocnemius muscle and the Achilles tendon during incline, level and decline locomotion. J Exp Biol. 2006;209(pt 21):4379-4388. [DOI] [PubMed] [Google Scholar]
- 34. Magnusson SP, Narici MV, Maganaris CN, Kjaer M. Human tendon behaviour and adaptation, in vivo. J Physiol. 2008;586:71-81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Malliaras P, Kamal B, Nowell A, et al. Patellar tendon adaptation in relation to load-intensity and contraction type. J Biomech. 2013;46:1893-1899. [DOI] [PubMed] [Google Scholar]
- 36. Park SK, Yang DJ, Kim JH, Heo JW, Uhm YH, Yoon JH. Analysis of mechanical properties of cervical muscles in patients with cervicogenic headache. J Phys Ther Sci. 2017;29:332-335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016;51:410-424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 3rd ed. Englewood Cliffs, NJ: Prentice Hall; 2009. [Google Scholar]
- 39. Pozarowszczyk B, Pawlaczyk W, Smoter M, et al. Effects of karate fights on Achilles tendon stiffness measured by myotonometry. J Hum Kinet. 2017;56:93-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Rio E, Kidgell D, Moseley GL, et al. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. Br J Sports Med. 2016;50:209-215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Rogers SA. Relationships Between Multiple Mechanical Stiffness Assessments and Performance in Middle-Distance Runners [master’s thesis]. Auckland, New Zealand: Auckland University of Technology; 2015. [Google Scholar]
- 42. Seynnes OR, Bojsen-Møller J, Albracht K, et al. Ultrasound-based testing of tendon mechanical properties: a critical evaluation. J Appl Physiol (1985). 2015;118:133-141. [DOI] [PubMed] [Google Scholar]
- 43. Wiesinger H-P, Kösters A, Müller E, Seynnes OR. Effects of increased loading on in vivo tendon properties: a systematic review. Med Sci Sports Exerc. 2015;47:1885-1895. [DOI] [PMC free article] [PubMed] [Google Scholar]