

Abstract
OBJECTIVE
The epidemiology of carpal tunnel syndrome (CTS) has been extensively researched. However, data describing the economic burden of CTS is limited. The purpose of this study was to quantify the disease burden of CTS and determine the economic benefit of its surgical management.
METHODS
The authors utilized the PearlDiver database to identify the number of individuals with CTS in the Medicare patient population, and then utilized CPT codes to identify which individuals underwent surgical management. These data were used to calculate the total number of disability-adjusted life years (DALYs) associated with CTS. A human capital approach was employed and gross national income per capita was used to calculate the economic burden.
RESULTS
From 2005 to 2012 there were 1,500,603 individuals identified in the Medicare patient population with the diagnosis of CTS. Without conservative or surgical management, this results in 804,113 DALYs without age weighting and discounting, and 450,235 DALYs with age weighting and a discount rate of 3%. This amounts to between $ 21.8 and $39 billion in total economic burden, or $2.7–$4.8 billion per year. Surgical management of CTS has resulted in the aversion of 173,000–309,000 DALYs. This has yielded between $780 million and $1.6 billion in economic benefit per year. Endoscopic carpal tunnel release provided between $11,683 and $23,186 per patient at 100% success while open carpal tunnel release provided between $10,711 and $22,132 per patient at 100% success. The benefit-cost ratio at its most conservative is 2.7:1, yet could be as high as 6.9:1.
CONCLUSIONS
CTS is prevalent in the Medicare patient population, and is associated with a large amount of economic burden. The surgical management of CTS leads to a large reduction in this burden, yielding extraordinary economic benefit.
Keywords: carpal tunnel release, DALY, economic benefit, utilization, disability-adjusted life year
Carpal tunnel syndrome (CTS) is the most commonly diagnosed peripheral neuropathy in the US, with an incidence of approximately 1–3 people per 1000 per year.3,6,22 Conservative therapy is typically used, but many patients ultimately require surgery. This is one of the most common surgical procedures performed each year with more than 600,000 cases performed annually.22 Given the prominence of this disease, a study determining disease burden and economic benefit of treating the disease is of value. The onset of disease for CTS is reportedly between 40 and 60 years of age, therefore the Medicare patient population would be greatly impacted by this condition.9,21 The authors are unaware of any prior economic analysis performed within the Medicare patient population. The prevalence of CTS in the Medicare patient population leads to a large amount of disease burden that can be averted by surgical management. There is an increased focus on cost effectiveness and cost containment in medicine, and as such an understanding of health care resource utilization and economic burden for CTS would be valuable. The purpose of this study was to describe the disease burden of CTS in the Medicare patient population and to evaluate the benefit of providing surgery from a disease burden aversion model.
Methods
Data Collection
To assess the economic benefit of surgery for CTS, a previously reported utilization study was performed by the authors.13 A retrospective review of a Medicare database within the PearlDiver supercomputer was performed for patients undergoing open carpal tunnel release (OCTR) or endoscopic carpal tunnel release (ECTR) from 2005 to 2012. The PearlDiver database is a publicly available Health Insurance Portability and Accountability Act–compliant national database compiled from a collection of private payer records. This database contains current procedural terminology (CPT) and International Classification of Diseases, Ninth Revision (ICD-9) codes. Patients who underwent OCTR were identified by CPT code 64721 and ICD-9 code 04.43. ECTR was identified by CPT code 29848. CTS was identified by ICD-9 code 354.0.
Disability-Adjusted Life Years
The disability-adjusted life year (DALY) was created in the early 1990s as a health measure that extended beyond deaths avoided. It encompasses healthy years of life lost as a result of disability as well as years of life lost due to premature death.19 The DALY itself is calculated by assigning a particular health state with a corresponding disability weight ranging from 0 to 1 (0 = perfect health, 1 = death). The value of a DALY is impacted based on adjustments made to discounting and age weighting. Discounting arises from the belief that individuals value a healthy year of life at the present, decreasing the value of a life year in the future. Age weighting places more value on a year of middle life compared to those at the beginning or end of life. Due to the debate over the accuracy of these principles, calculations were made with and without age weighting and discounting.20
Calculating DALYs
DALYs were calculated and converted to US dollars by means of the human capital approach. The human capital approach assumes that the individual is valued at their contribution to the economy. The notation DALY (r,K,C) represents the adjustments to the DALY based on discount-weighting, age weighting, and the age-weighting factor, respectively. For the human capital approach, DALYs (3,1,0.04) were calculated under the conditions of 3% discounting + age weighting. Additionally, DALYs (0,0,0) were calculated under the conditions without discounting or age weighting. DALYs were calculated using the following equation used in previous studies:5,20,26
in which “L” is the country-specific life expectancy in the US (www.worldbank.org), “a” represents the age of onset of disease, and “DW” represents the disability weight for carpal tunnel syndrome.7 Age of disease onset was set at 65 years of age to avoid overestimating the disability within the Medicare patient population. “K” is the age-weighting modulation constant (0 = no age weighting, 1 = age weighting), “C” is the age-weighting disability constant (0.04), “x” is the age integrated over the duration of disease and/or years of life lost, and “r” is the discount rate (3%).14
Valuing DALYs
The human capital approach values averted DALYs at a lower bound of DALYs (3,1,0.04) × gross national income (GNI) per capita and an upper bound of DALYs (0,0,0) × GNI per capita. The GNI per capita was calculated by averaging the US GNI per capita reported by the World Bank (data.worldbank.org) from the years included in this study. 26
Determining Economic Benefit
The DALY calculations allow one to interpret and quantify multiple health states. Importantly, this allows for the calculations of DALYs averted due to an intervention by establishing two scenarios that reflect the course of disease with and without intervention. In the first scenario, the assumption is made that no surgical intervention is performed, and DALYs are calculated. In the second scenario, DALYs are calculated when surgical intervention is conducted. The difference obtained by subtracting total DALYs in scenario 2 from scenario 1 is representative of the DALYs averted due to the intervention, and is representative of the improved health care state as a consequence. Economic benefit is the value of this difference in US dollars (USD). 26 The assumption is that surgery for CTS relieves the disability weight associated with the condition. Calculations for economic benefit were made for 100%, 90%, 80%, and 70% success rate, representing the proportion of DALYs averted by means of surgery.
Results
Medicare Utilization
Our query returned 1,500,603 patients with CTS of which 507,924 (33.8%) and 68,768 (4.6%) were managed surgically with OCTR and ECTR, respectively (Fig. 1A). Surgeries for CTS were performed most frequently in the < 65 age group. Both procedures were performed most commonly in females (64%) compared with males (36%; Fig. 1C). OCTR and ECTR were performed the most in the Southern region (36.1% and 37.6%) and the least in the Western region (12.9% and 14.7%; Fig. 1B). Mean annual charges were significantly higher in the OCTR group ($3820) than ECTR ($2952). Conversely, reimbursements paid by Medicare were higher in ECTR ($1643) than OCTR ($1312; Fig. 2).
FIG. 1.
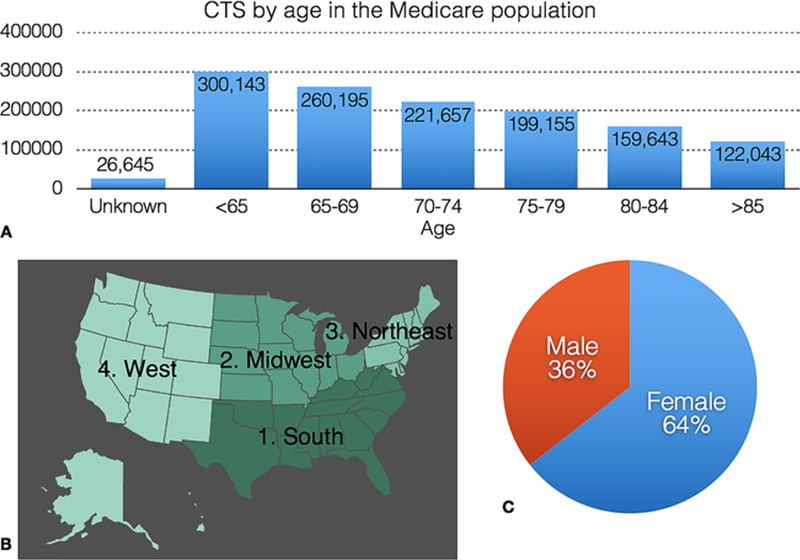
A: Bar graph demonstrating the number of patients with CTS according to age group. B: Geographic representation of total CTS surgeries following US Census Bureau data. C: Pie chart demonstrating total CTS surgeries by sex.
FIG. 2.
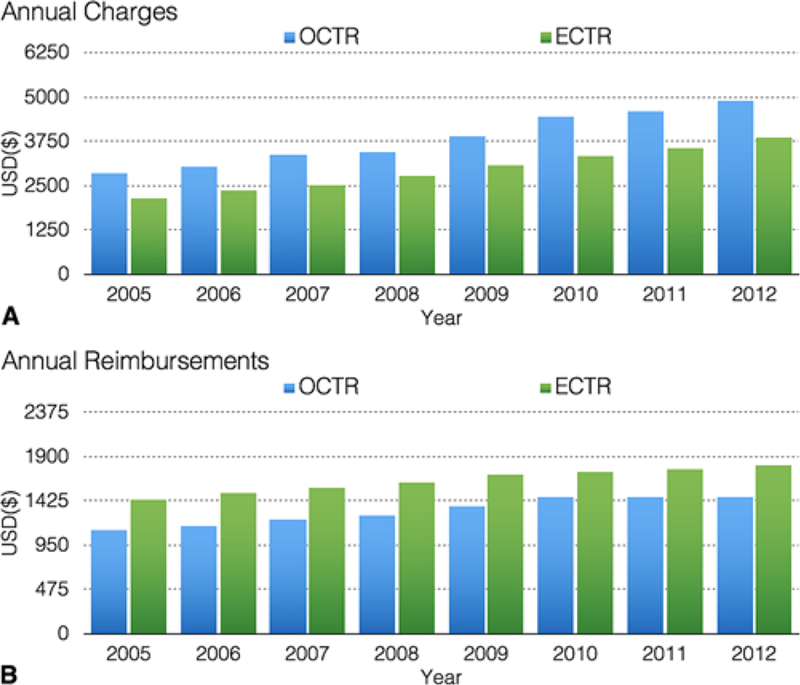
Bar graphs demonstrating annual charges (A) and annual reimbursements (B) for OCTR and ECTR from 2005 to 2012.
DALYs
DALYs were calculated for all 1,500,603 patients with CTS within the Medicare patient population. This resulted in a total of 450,235 DALYs calculated using age weighting and discounting, and a total of 804,113 DALYs calculated without age weighting and discounting (Table 1). CTS results in an average loss of 78,375 DALYs per year. Converting DALYs into USD, the total disease burden of carpal tunnel syndrome ranged from $2.7 to $4.8 billion annually or between $21.8 and $39 billion during the study period (Table 2).
TABLE 1.
DALYs calculated using a human capital approach
| DALY | 3% Discounting DALY (3,K,C) | No Discounting DALY (0,K,C) |
|---|---|---|
| Age weighting (r,1,0.04) | 450,235 | 544,703 |
| No age weighting (r,0,0) | 661,313 | 804,113 |
(r,K,C) = (discount rate, age weighting modulation constant, age weighting disability constant)
TABLE 2.
Disease burden of CTS in the Medicare patient population
| Variable | DALY (3,1,0.04) | DALY (0,0,0) |
|---|---|---|
| DALYs | 450,235 | 804,113 |
| Annual economic burden | $2.7 billion | $4.8 billion |
| Total economic burden | $21.8 billion | $39 billion |
(r,K,C) = (discount rate, age weighting modulation constant, age weighting disability constant)
Economic Benefit
In scenario 1, a total of 1,500,603 patients with CTS experienced a health state equivalent to 450,000–804,000 total DALYs. In scenario 2, 576,692 of these patients underwent surgical management that resulted in an improved health care state of 277,000–495,000 total DALYs. Subtracting scenario 2 from scenario 1 resulted in a total of 173,000–309,000 total DALYs averted due to both OCTR and ECTR.
Converting averted DALYs to USD amounts to $8.39– $14.98 billion in total gross economic benefit for both OCTR and ECTR assuming a 100% success rate, $7.54– $13.48 billion assuming a 90% success rate, $6.71–$11.98 billion assuming an 80% success rate, and $5.87–$10.48 assuming a 70% success rate. OCTR was responsible for the greatest amount of gross benefit due to a greater number of procedures performed compared to ECTR.
OCTR and ECTR costs were generated from the average charges billed to Medicare at $3820 and $2952, respectively. The product of the average cost and the total number of procedures resulted in total costs of $1.94 billion and $203 million for OCTR and ECTR, respectively (Tables 3 and 4). Average annual costs amounted to $242.5 million/year and $25.4 million/year for OCTR and ECTR, respectively. These costs were used to determine the cost-benefit ratio for surgical intervention for CTS.
TABLE 3.
Net economic benefit of OCTR
| Variable | DALY (3,1,0.04) | DALY (0,0,0) |
|---|---|---|
| Gross economic benefit | 8,386,905,542 | 14,978,888,306 |
| OCTR economic benefit | 7,380,476,877 | 13,181,421,709 |
| Cost per OCTR* | 3820 | |
| Total cost OCTR* | 1,940,000,000 | |
| Net economic benefit of OCTR | 5,440,476,877 | 11,241,421,709 |
| Net economic benefit per patient† | ||
| 100% | 10,711 | 22,132 |
| 90% | 9640 | 19,919 |
| 80% | 8569 | 17,706 |
| 70% | 7498 | 15,492 |
All values given in USD.
Reported by Medicare.
100%, 90%, 80%, and 70% surgical efficacy to avert DALYs.
TABLE 4.
Net economic benefit of ECTR
| Variable | DALY (3,1,0.04) | DALY (0,0,0) |
|---|---|---|
| Gross economic benefit | 8,386,905,542 | 14,978,888,306 |
| ECTR economic benefit | 1,006,428,665 | 1,797,466,597 |
| Cost per ECTR* | 2952 | |
| Total cost ECTR* | 203,000,000 | |
| Net economic benefit of ECTR | 803,428,665 | 1,594,466,597 |
| Net economic benefit per patient† | ||
| 100% | 11,683 | 23,186 |
| 90% | 10,515 | 20,868 |
| 80% | 9347 | 18,549 |
| 70% | 8178 | 16,230 |
All values given in USD.
Reported by Medicare.
100%, 90%, 80%, and 70% surgical efficacy to avert DALYs.
Subtracting total costs from total gross economic benefit yields the net economic benefit of surgeries for procedures performed within the Medicare patient population. Net economic benefit totaled between $6.2 and $12.8 billion, or an average between $780 million and $1.60 billion per year. Total net economic benefit for OCTR ranged between $5.4 and $11.2 billion (Table 3), while for ECTR it ranged between $803 million and $1.59 billion (Table 4). ECTR was associated with lower costs, therefore the net economic benefit was greater per patient. ECTR provided between $11,683 and $23,186 per patient at 100% success while OCTR provided between $10,711 and $22,132 per patient at 100% success. The most conservative estimate for CTS surgery was at a surgical success rate of 70%. This success rate equaled $7498 to $15,492 per patient for OCTR and $8178 to $16,230 per patient for ECTR (Tables 3 and 4). The benefit-cost ratio at its most conservative is 2.7:1, yet could be as high as 6.9:1 with greater surgical success.
Discussion
This study is the first to analyze the utilization, cost of treatment, disease burden, and economic benefit of treating CTS in the Medicare patient population. CTS is the most common peripheral neuropathy in the US and no treatment leads to mild to moderate disability. This study attempted to quantify that disability and the long-term benefit of surgical intervention.
CTS management has evolved over time with trends shifting from an open toward an endoscopic approach.22 Although many studies have reported similar outcomes, the endoscopic approach is being utilized at a greater rate over the past two decades.8,10,17 This growth might be influenced by patient preference due to a reduction in scar tenderness and increase in grip and pinch strength.17,23 Interestingly, financial factors might be present as well. Our study found that ECTR charges were lower, which is corroborated by the study of Trumble et al. who found that the average cost of OCTR was $3940 compared with $3750 for ECTR.24 These financial factors may impact patient and physician preference, but they also impact the net economic benefit provided to the population affected by CTS. Our study found higher net economic benefit provided by ECTR compared with OCTR, due to the lower charges.
Defining the surgical success rate can be difficult due to variations in both surgeon and patient factors across the Medicare population. For this reason, benefit was calculated at varying ranges of surgical success ranging from 70% to 100% success. Importantly, factors such as complication rate, reoperation rate, and patient satisfaction should be considered. Atroshi et al. reported the outcomes of 128 patients, 12.8 years following a randomized controlled trial for open versus endoscopic carpal tunnel release. There was similar efficacy in reduction of symptom severity between the two approaches, with a reoperation rate of 6%.2 In a recent meta-analysis, Vasiliadis reported an overall complication rate of 3.84% over 7227 patient-years.25 Additionally, a meta-analysis by Zuo et al. utilized four studies to estimate patient subjective satisfaction at 87.96% and 87.97% for ECTR and OCTR, respectively. 27
Overall, both OCTR and ECTR provide successful surgical management of CTS. In 1998, Katz et al. suggested a surgical success rate of > 70%, which was later supported by Bland in 2007 who reported a rate of 75%. 4,12 Subsequent studies suggested that CTS surgery appears to be corrective or obtain adequate relief of symptoms in 70%– 90%.15,16,18 The authors believe that a surgical success rate of 70%–80% can be used to conservatively estimate the economic benefit of OCTR and ECTR. Therefore, the most conservative estimate of CTS surgery (70%) would provide between $3.73 and $8.34 billion in net economic benefit. This amounts to a benefit-cost ratio of 2.7:1 to 4.9:1.
Our study found a large economic burden of CTS within the Medicare population. CTS disease burden is greater than the annual burden of peptic ulcer disease, but less than conditions such as periodontal disease or benign prostatic hypertrophy (Fig. 3).11
FIG. 3.
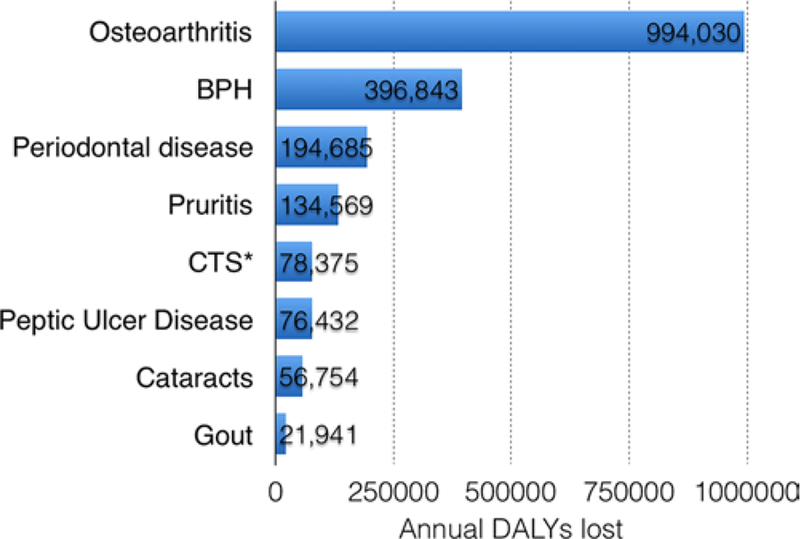
Horizontal bar chart demonstrating annual disease burden in DALYs/year of various medical conditions. BPH = benign prostatic hypertrophy.
OCTR and ECTR have provided a remarkable amount of benefit within the Medicare patient population. In the future, cost of treatment will likely be a main driver to utilization. This study indicated that surgical management is providing a large amount of benefit with a very low cost/ DALYs. Cost/DALYs was optimized when ECTR was utilized, however, this is functioning under the assumption that both procedures are providing equivalent improvement in the health state. Future studies may provide further insight into the optimal treatment modality and will be able to delineate which approach is most cost-effective.
Limitations
This study is not without limitations. The PearlDiver database is reliant on accurate CPT or ICD coding, which creates the potential for a reporting bias. In addition, we investigated charges and reimbursements rather than direct costs because this was not available within the Pearl-Diver database. Finally, patient comorbidities were not stratified within the scope of this study.
The limitations of DALYs are well described in previous literature.1 The DALY was not intentioned to quantify reduction of the burden of disease.26 The authors believe that this model is a reasonable assessment of the economic benefit in treating CTS, as surgical management has an established efficacy. The disability weight was established in surveying 30,660 people, which is likely representative of the patient perception of healthy years of life loss due to the condition. This analysis is limited in the fact that a large number of Medicare patients incorporated were subject to surgical management by two different modalities. Each modality may be performed by a litany of different techniques and/or systems, by many different surgeons. We attempted to account for this variability by calculating the economic benefit across increasing proportions of surgical success.
Conclusions
This study indicates there is a great amount of economic benefit provided by performing OCTR and ECTR for CTS within the Medicare patient population. The total annual DALYs for CTS are comparable to that of peptic ulcer disease, pruritus, and cataracts. Each patient treated provides $7498 to $22,132 in benefit for OCTR and $8178 to $23,186 in benefit for ECTR depending on the surgical success rate. The cost-benefit ratio, therefore, is 2.7:1 with most conservative estimates, and potentially as high as 6.9:1.
ABBREVIATIONS
- CPT
current procedural terminology
- CTS
carpal tunnel syndrome
- DALY
disability-adjusted life year
- ECTR
endoscopic carpal tunnel release
- GNI
gross national income
- OCTR
open carpal tunnel release
- USD
US dollars
Footnotes
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
- 1.Anand S, Hanson K: Disability-adjusted life years: a critical review. J Health Econ 16:685–702, 1997 [DOI] [PubMed] [Google Scholar]
- 2.Atroshi I, Hofer M, Larsson GU, Ranstam J: Extended follow-up of a randomized clinical trial of open vs endoscopic release surgery for carpal tunnel syndrome. JAMA 314:1399–1401, 2015 [DOI] [PubMed] [Google Scholar]
- 3.Beck JD, Deegan JH, Rhoades D, Klena JC: Results of endoscopic carpal tunnel release relative to surgeon experience with the Agee technique. J Hand Surg Am 36:61–64, 2011 [DOI] [PubMed] [Google Scholar]
- 4.Bland JD: Treatment of carpal tunnel syndrome. Muscle Nerve 36:167–171, 2007 [DOI] [PubMed] [Google Scholar]
- 5.Devleesschauwer B, Havelaar AH, Maertens de Noordhout C, Haagsma JA, Praet N, Dorny P, et al. : Calculating disability-adjusted life years to quantify burden of disease. Int J Public Health 59:565–569, 2014 [DOI] [PubMed] [Google Scholar]
- 6.Fajardo M, Kim SH, Szabo RM: Incidence of carpal tunnel release: trends and implications within the United States ambulatory care setting. J Hand Surg Am 37:1599–1605, 2012 [DOI] [PubMed] [Google Scholar]
- 7.Haagsma JA, Maertens de Noordhout C, Polinder S, Vos T, Havelaar AH, Cassini A, et al. : Assessing disability weights based on the responses of 30,660 people from four European countries. Popul Health Metr 13:10, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hansen TB, Majeed HG: Endoscopic carpal tunnel release. Hand Clin 30:47–53, 2014 [DOI] [PubMed] [Google Scholar]
- 9.Ibrahim I, Khan WS, Goddard N, Smitham P: Carpal tunnel syndrome: a review of the recent literature. Open Orthop J 6:69–76, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kang HJ, Koh IH, Lee TJ, Choi YR: Endoscopic carpal tunnel release is preferred over mini-open despite similar outcome: a randomized trial. Clin Orthop Relat Res 471:1548–1554, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kassebaum N, Arora M, Barber RM, Bhutta ZA, Brown J, Carter A, et al. : Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388:1603–1658, 2016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Katz JN, Keller RB, Simmons BP, Rogers WD, Bessette L, Fossel AH, et al. : Maine Carpal Tunnel Study: outcomes of operative and nonoperative therapy for carpal tunnel syndrome in a community-based cohort. J Hand Surg Am 23:697–710, 1998 [DOI] [PubMed] [Google Scholar]
- 13.Law TY, Rosas S, Hubbard ZS, Chieng LO, Chim HW: Trends in open and endoscopic carpal tunnel release utilization in the Medicare patient population. J Surg Res 214:9–13, 2017 [DOI] [PubMed] [Google Scholar]
- 14.Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL (eds): Global Burden of Disease and Risk Factors New York: Oxford University Press, 2006 [Google Scholar]
- 15.Louie D, Earp B, Blazar P: Long-term outcomes of carpal tunnel release: a critical review of the literature. Hand (N Y) 7:242–246, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Louie DL, Earp BE, Collins JE, Losina E, Katz JN, Black EM, et al. : Outcomes of open carpal tunnel release at a minimum of ten years. J Bone Joint Surg Am 95:1067–1073, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mintalucci DJ, Leinberry CF Jr: Open versus endoscopic carpal tunnel release. Orthop Clin North Am 43:431–437, 2012 [DOI] [PubMed] [Google Scholar]
- 18.Mosier BA, Hughes TB: Recurrent carpal tunnel syndrome. Hand Clin 29:427–434, 2013 [DOI] [PubMed] [Google Scholar]
- 19.Murray CJ: Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bull World Health Organ 72:429–445, 1994 [PMC free article] [PubMed] [Google Scholar]
- 20.Murray CJ, Acharya AK: Understanding DALYs (disability-adjusted life years). J Health Econ 16:703–730, 1997 [DOI] [PubMed] [Google Scholar]
- 21.Phalen GS: The carpal-tunnel syndrome. Seventeen years’ experience in diagnosis and treatment of six hundred fifty-four hands. J Bone Joint Surg Am 48:211–228, 1966 [PubMed] [Google Scholar]
- 22.Smetana BS, Zhou X, Hurwitz S, Kamath GV, Patterson JM: Effects of hand fellowship training on rates of endoscopic and open carpal tunnel release. J Hand Surg Am 41:e53–e58, 2016 [DOI] [PubMed] [Google Scholar]
- 23.Thoma A, Veltri K, Haines T, Duku E: A meta-analysis of randomized controlled trials comparing endoscopic and open carpal tunnel decompression. Plast Reconstr Surg 114:1137–1146, 2004 [DOI] [PubMed] [Google Scholar]
- 24.Trumble TE, Diao E, Abrams RA, Gilbert-Anderson MM: Single-portal endoscopic carpal tunnel release compared with open release: a prospective, randomized trial. J Bone Joint Surg Am 84-A:1107–1115, 2002 [DOI] [PubMed] [Google Scholar]
- 25.Vasiliadis HS, Nikolakopoulou A, Shrier I, Lunn MP, Brassington R, Scholten RJ, et al. : Endoscopic and open release similarly safe for the treatment of carpal tunnel syndrome. A systematic review and meta-analysis. PLoS One 10:e0143683, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Warf BC, Alkire BC, Bhai S, Hughes C, Schiff SJ, Vincent JR, et al. : Costs and benefits of neurosurgical intervention for infant hydrocephalus in sub-Saharan Africa. J Neurosurg Pediatr 8:509–521, 2011 [DOI] [PubMed] [Google Scholar]
- 27.Zuo D, Zhou Z, Wang H, Liao Y, Zheng L, Hua Y, et al. : Endoscopic versus open carpal tunnel release for idiopathic carpal tunnel syndrome: a meta-analysis of randomized controlled trials. J Orthop Surg Res 10:12, 2015 [DOI] [PMC free article] [PubMed] [Google Scholar]