

Abstract
Objectives:
Previous research has shown that e-cigarette use is rising among young adults, but it is unknown whether the dual use of alcohol and marijuana is associated with e-cigarette use in a U.S.A. nationally representative sample.
Methodology:
Secondary analysis of the Population Assessment of Tobacco and Health 2013–2014 nationally representative sample of young adults (aged 18–24) was conducted to examine the relationships between dual ever and dual current use of alcohol and marijuana with e-cigarette use. Multiple logistic regression models were used to explore the associations between dual ever and dual current use alcohol and marijuana with two outcomes: Past 30 days and former experimental e-cigarette use. Covariates included sex, race/ethnicity, education level, household income, and the total number of tobacco products ever used.
Results:
Dual ever use of alcohol and marijuana was significantly associated with past 30 days use (adjusted odds ratio [AOR] = 2.20; 95% confidence interval [CI] = 1.67–2.91) and former experimental e-cigarette use (AOR = 2.82; 95% CI = 2.23–3.57). Exclusive ever marijuana use was also significantly associated with each outcome, while exclusive ever alcohol use was associated with former experimental e-cigarette use. Exclusive current marijuana use, exclusive current alcohol use, and dual current use of both substances were significantly associated with past 30-day e-cigarette use, but not former experimental e-cigarette use.
Conclusions:
These findings indicate that young adult dual users of marijuana and alcohol have increased odds of e-cigarette use. In addition, exclusive current and ever marijuana users had the highest odds e-cigarette use, higher than young adult dual users of alcohol and marijuana, indicating that marijuana users may be an important group to target with intervention programs.
Keywords: Alcohol, electronic cigarettes, marijuana, non-cigarette tobacco products, young adults
Introduction
Combustible cigarette use has decreased among young adults (ages 18–24), but non-cigarette tobacco product (NCTP) usage has increased in the United States among this age group since 2011.[1-3] NCTPs include cigars, pipes, hookah, smokeless tobacco, and electronic cigarettes (e-cigarettes),[4] which generate inhalable nicotine aerosol by heating a nicotine solution when they are used as intended.[1] In 2014, data from the National Adult Tobacco Survey found that, among U.S. adults (aged 18–24 years), the prevalence of ever e-cigarette use more than doubled from the previous year to 35.8% and the prevalence of past 30-day e-cigarette use was 13.6%, while among adults 25 and older, 16.4% reported ever e-cigarette use and 5.7% reported past 30-day e-cigarette use.[1] In addition, the prevalence of ever e-cigarette use among students in grades 6–12 was 8.1%, as shown by data from the National Youth Tobacco Survey.[1,5] These findings show that young adults in the U.S.A. exhibit the highest rates of e-cigarette use, and research is needed to determine what other substance-use behaviors influence this trend.
The emerging adulthood hypothesis claims that young adulthood (ages 18–25) is a distinct developmental period that features independent role exploration and identity exploration.[6] Some of the strongest evidence for the emerging adulthood hypothesis comes from trends in psychoactive substance use, as young adulthood is characterized by an increase in the use of many different psychoactive substances that have potential negative health consequences.[2,7,8] A survey conducted by the Substance Abuse and Mental Health Services Administration found that, in 2014, the prevalence of past 30-day alcohol use among young adults (aged 18–25) was 59.6% and the prevalence of past 30-day marijuana use in young adults was 19.6%,[2] which were higher than the prevalence’s among other age groups studied, including adolescents aged 12–17 and adults aged 26 and older.[2]
Previous research has established that the couse of alcohol with tobacco products, marijuana with tobacco products, as well as alcohol and marijuana use are all common substance use behavior patterns in young adults.[2,3,7,9-12] Researchers are now starting to generate evidence on the association between alcohol and marijuana use with e-cigarette use, but the evidence is mixed, and dual use of both substances has not been explored. Using data from 2013, researchers examined the link between alcohol and marijuana use with e-cigarette use in a U.S.A. nationally representative sample of young adults (ages 18–24).[11] They found that after controlling for covariates, current (past 30-day) alcohol use was significantly associated with increased odds of past 30-day e-cigarette use (adjusted odds ratio [AOR] = 9.03) and that current marijuana use was significantly associated with increased odds of past 30-day e-cigarette use (AOR= 2.31).[11] However, a different U.S.A. nationally representative study found no association between current marijuana use and NCTP use, which included e-cigarettes, snus, dissolvables, chewing tobacco, dip, or snuff.[3] Finally, a convenience sample of college students in New York found that past year marijuana use was significantly associated with past 30-day e-cigarette use (AOR = 2.37), but the association between past 30-day alcohol use and past 30-day e-cigarette use was not significant.[7] More research using different study samples and research approaches is needed to further clarify these mixed findings exploring if alcohol and marijuana use is associated with e-cigarette use in the United States.
The current study sought to explore patterns of alcohol and marijuana use among e-cigarette users for several reasons. The couse of alcohol and marijuana is well established,[13] so exploring the dual use of both substances as exposure for e-cigarette use is warranted to determine the effect of these risky behaviors on e-cigarette use. Lifetime tobacco use, including cigarettes and NCTPs, is primarily established during emerging adulthood,[14] and there are significant health implications for preventing e-cigarette use among young adults. Furthermore, recent research has shown that e-cigarette users who have never smoked a combustible cigarette exhibit increased risk of cigarette smoking after 1 year of follow-up, indicating that e-cigarette use may be a risk factor for subsequent combustible cigarette use.[15] This trend is concerning because studies of toxicant and carcinogen metabolites have shown that combustible cigarettes are more harmful to health than e-cigarettes.[16] The risks of long-term health consequences, such as chronic obstructive pulmonary disease and lung cancer, which result from nicotine’s effect on the respiratory and cardiovascular systems are elevated when individuals initiate and establish tobacco product use during emerging adulthood.[17] While the long-term effects of e-cigarette use are unknown, the use of any product that contains nicotine should be concerning, and more research is needed exploring the factors that contribute to e-cigarette use in this age group.
The current study conceptualizes dual ever use of alcohol and marijuana, as well as dual past-30 day use (from now on referred to as current use) of alcohol and marijuana as hypothesized exposures for e-cigarette use, above and beyond exclusive use of each substance alone. The primary goal of this study was to explore combinations of substance use (never alcohol nor marijuana use, exclusive ever alcohol use, exclusive ever marijuana use, and ever use of both alcohol and marijuana, as well as non-current alcohol nor marijuana use, exclusive current alcohol use, exclusive current marijuana use, and dual current use of alcohol and marijuana) across e-cigarette use outcomes in the Population Assessment of Tobacco and Health (PATH) 2013–2014 sample of young adults (ages 18–24). By considering both dual and exclusive use of alcohol and marijuana as exposures, as well as both past 30-day and past experimentation with e-cigarettes as outcomes, this study adds to the literature elucidating the role of risky substance-use behaviors in the uptake of an emerging class of tobacco products.
Methods
Study design and participants
The PATH study used a four-stage stratified area probability sampling design to generate a nationally representative sample of U.S. adults in 2013–2014, and its methodology has been described elsewhere[4] with a summary provided here. The target population consisted of the civilian household population of individuals aged 12 and older in all 50 U.S. states, and wave 1 data were collected from September 2013 to December 2014 using Audio Computer-Assisted Self-Interviewing with 32,320 adults (18 and older) completing the study.[4] The overall weighted adult survey response rate was 74.0%, which was based on the household inverse probability of selection and the inverse of the within-household probability of selection. The current study implemented a secondary data cross-sectional analysis of the PATH 2013–2014 young adult sample of participants in the 18–24 year old age category (n = 9.112) because previous research has identified this population as at higher risk of using alcohol and marijuana, as well as e-cigarettes,[1,2,11] and the publicly available PATH data categorizes participants into an age category with this range. This secondary analysis was reviewed by the Committee for the Protection of Human Subjects of the University of Texas Health Science Center at Houston (HSC-SPH-16-1088).
Outcomes
Two outcome variables concerning e-cigarette use classified participants as different types of e-cigarette users based their answers to questions about their frequency of e-cigarette use. Participants were asked: (1) “Have you ever used an e-cigarette, such as NJOY, Blu, or Smoking Everywhere, even one or two times?” (2) “Have you ever used e-cigarettes fairly regularly?” (3) “Do you now use e-cigarettes?” and (4) “In the past 30 days, have you used an e-cigarette, even one or two times?” Response options to the first three questions were “yes,” “no,” and “don’t know,” and response options for the fourth question were “every day,” “some days,” and “not at all.”
Our first outcome was past 30-day e-cigarette use. Participants who answered “yes” to the first question and “every day” or “some days” to the fourth question were identified as past 30-day e-cigarette users. The second outcome was former experimental e-cigarette use. Participants who answered “yes” to the first question and “no” to the second, third, and fourth questions were categorized as former experimental e-cigarette users.
Combinations of exposure to ever alcohol use and ever marijuana use
Ever use of alcohol and marijuana was considered as exposures for e-cigarette use, and answers to survey questions were used to create combinations of exposure. Ever alcohol use was asked: “Have you ever used alcohol at all including sips of someone’s drink or your own drink?” Ever marijuana use was asked with two questions: “Have you ever used marijuana, hash, THC, grass, pot, or weed?” and “Have you ever smoked part or all of a cigar, cigarillo, or filtered cigar with marijuana in it?” Response options for all questions included “yes” and “no,” and these responses were used to create four combinations of exposure. Participants who answered “yes” to the question about alcohol use and “yes” to either question about marijuana use were categorized as dual ever users of both substances. Participants who answered “yes” to ever use of alcohol and “no” to both questions on ever use of marijuana were categorized as exclusive ever alcohol users, and participants who answered “yes” to either question about ever marijuana use and “no” to ever alcohol use were categorized as exclusive ever marijuana users. Participants who answered “no” to all questions about marijuana and alcohol use were categorized as never users of both substances. These responses were coded in a single variable to represent the four combinations of ever alcohol and ever marijuana use, with never alcohol nor marijuana use serving as the referent.
The second set of combinations of exposure to alcohol and marijuana was created to reflect exposure to the current use of these substances. Time since last alcohol use was asked among participants who reported ever use of alcohol: “How long has it been since you last used alcohol?” Time since last marijuana use was asked to participants who reported ever use of marijuana: “How long has it been since you last used marijuana?” Response options for both questions were “within the past 30 days,” “more than 30 days ago, but within the past year,” and “more than a year ago.” These variables were recorded in binary variables to reflect past 30-day use (yes/no). Participants who answered “within the past 30 days” to the question about alcohol use and “within the past 30 days” to the question about marijuana use were categorized as dual current users of both substances. Participants who answered “within the past 30 days” to the question about alcohol use and one of the other two responses to the question about marijuana were categorized as exclusive current alcohol users. Participants who answered “within the past 30 days” to the question about marijuana use and one of the other two responses to the question about alcohol use were categorized as exclusive current alcohol users. Participants who responded that they did not use neither alcohol nor marijuana in the past 30-days were categorized as non-current users of both substances. All responses were coded into a single variable to represent the four combinations of exposure to current alcohol and marijuana use, with non-current users of both substances serving as the referent.
Covariates
Covariates that were controlled for in analysis include sex, race/ethnicity, education level, household income, and the total number of tobacco products ever used because these covariates have been shown to exhibit a relationship with both e-cigarette use and alcohol and marijuana use.[3,7,8,12,18,19] The 2013-2014 public data for PATH measured participant race and ethnicity with the following categories, which were combined to create a single measure of race/ethnicity: White, Black, Hispanic, and Other. In this manuscript we will refer to participants that responded with “White” race as “Caucasian” and participants that responded with “Black” race as “African American”. Education level was asked to participants: “What is the highest grade or level of school you completed?” With response options: Less than high school, general education development (GED), high school graduate, some college or associates degree, Bachelor’s degree, or advanced degree. GED and high school graduate were collapsed into a single category, and the Bachelor’s Degree and Advanced degree were collapsed together due to the low sample size in these categories. Household income was asked to participants: “Which of the following categories best describes your total household income in the past 12 months?” With response options: <$10,000; $10,000–$24,999; $25,000–$49,999; $50,000–$99,999; and $100,000 or more into a single category. We also collapsed $50,000–$99,999 and the $100,000 or more together due to low sample size. In addition, response options for do not know and refused question were included as viable response options due to high sample sizes in these responses for the survey question about household income. Due to the low sample size for these response options in other variables, these values were set to missing. The total number of tobacco products ever used (other than e-cigarettes) was assessed using a new variable that summed participant responses (no = 0, yes = 1 for a total possible sum of 9) to questions that asked: “Have you ever used (tobacco product), even once or twice?” For nine different tobacco products, which included cigarettes, traditional cigars, cigarillos, filtered cigars, pipe tobacco, hookah, smokeless tobacco, dissolvable tobacco, and snus.[8]
Statistical methods
Final full-sample person-level sampling weights to account for the complex survey design with 100 replicate weights and design variables were used for variance estimation in the analysis of PATH.[4,8] Sampling weights were used to account for oversampling of certain population groups and accounted for non-response.[4,8] Weighted means and standard errors (SE) are provided for continuous variables, and weighted proportions and frequencies are provided for categorical variables. Missing data patterns revealed that 8954 (n = 30,194,335) young adult participants had complete data for the outcomes, exposures, and covariates representing 99% of the original sample of young adults. The total missingness for all study variables was >1%, so only participants with complete data were included in analysis,[20] and analyses were conducted in Stata statistical software version 14.2.[21]
Weighted univariate logistic regression methods were used to evaluate the combinations of exposures, as well as each covariate with each e-cigarette use outcome. Likelihood ratio adjusted Wald tests were used to assess if exposures and covariates should be included in the final adjusted models for both outcomes using the criteria of P < 0.20 for inclusion. Weighted multivariable logistic regression methods were used to generate adjusted odds ratios and 95% confidence intervals are reported exploring the cross-sectional relationship between dual ever use of alcohol and marijuana (as well as each combination of exposure) and dual current use of alcohol and marijuana (as well as each combination of exposure) for each e-cigarette use outcome. Likelihood ratio adjusted Wald tests were conducted after running the final adjusted model to determine if the exposure variable was a significant predictor of the outcome while taking into account the effect of the covariates. F-test statistics with P < 0.05 was considered significant.
Results
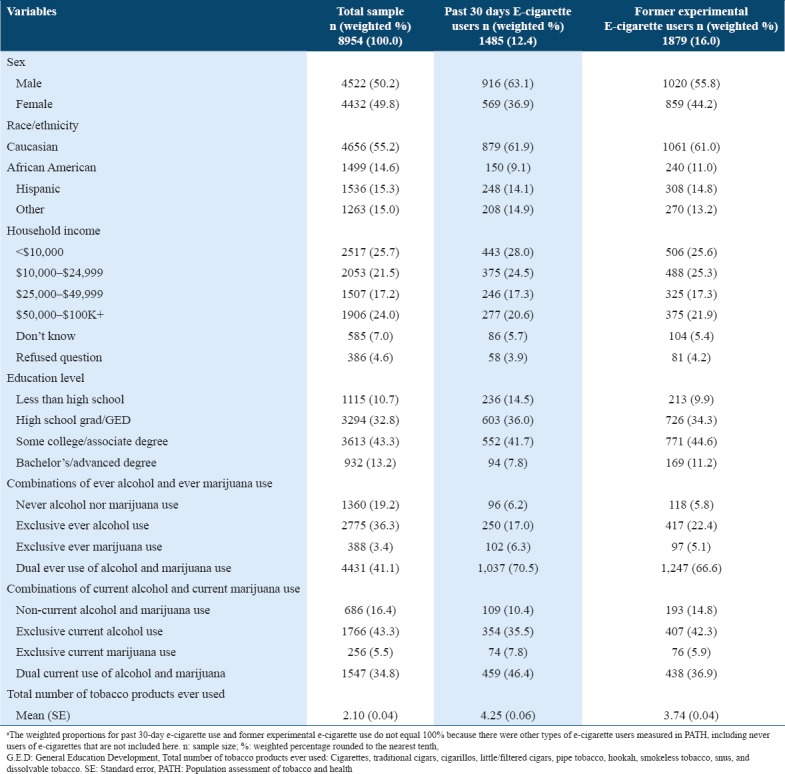
Descriptive statistics for the total PATH Wave 1 nationally representative sample of young adults (n = 8954; N = 30,194,335) and across both of the e-cigarette user types are shown in Table 1. Overall, 49.8% were females, 55.2% were Caucasian, 15.3% were Hispanic, 14.6% were African American and 15.0% were other race, and 56.5% of the young adults had some degree of college education. The prevalence of exclusive ever alcohol use was 36.3% among the total young adult sample, 3.4% were exclusive ever marijuana users, and 41.1% had ever used both substances [Table 1]. The mean number of tobacco products ever used by all young adults was 2.10 (standard error = 0.04). The prevalence of former experimental e-cigarette use was 16.0% (n = 1879; N = 4,816,942) and 12.4% (n = 1485; N = 3,734,432) reported past 30-day e-cigarette use, which is similar to other U.S.A. national estimates.[1] Across the e-cigarette use outcomes, 70.5% of past 30-day e-cigarette users reported ever use of both alcohol and marijuana and 66.6% of former experimental e-cigarette users reported ever use of both alcohol and marijuana. Among past 30-day e-cigarette users, 46.4% reported the dual current use of alcohol and marijuana, while 36.9% of former experimental e-cigarette users reported the dual current use of alcohol and marijuana. Past 30-day e-cigarette users and former experimental e-cigarette users reported ever use of around four tobacco products, on average.
Table 1.
Participant characteristics for the 2013-2014 PATH young adults (ages 18-24) by e-cigarette user type
The results of univariate analyses revealed that the combinations of exposure to ever alcohol and ever marijuana use were significantly associated with each outcome. Unadjusted associations for exposures and covariates are presented in Table 2. Sex, race/ethnicity, household income, education level, and total number of tobacco products ever used all met the requirements for inclusion in the multivariable models for both outcomes. Adjusted associations for exposures and covariates are presented in Table 3. While some of the demographic factors and the number of tobacco products ever used exhibited significant associations with e-cigarette use outcomes, the strongest associations were with the combinations of exposure to alcohol and marijuana use.
Table 2.
Unadjusted multiple logistic regression models of alcohol use and marijuana use on e-cigarette use outcomes in the PATH 2013–2014 sample of young adults (ages 18–24)
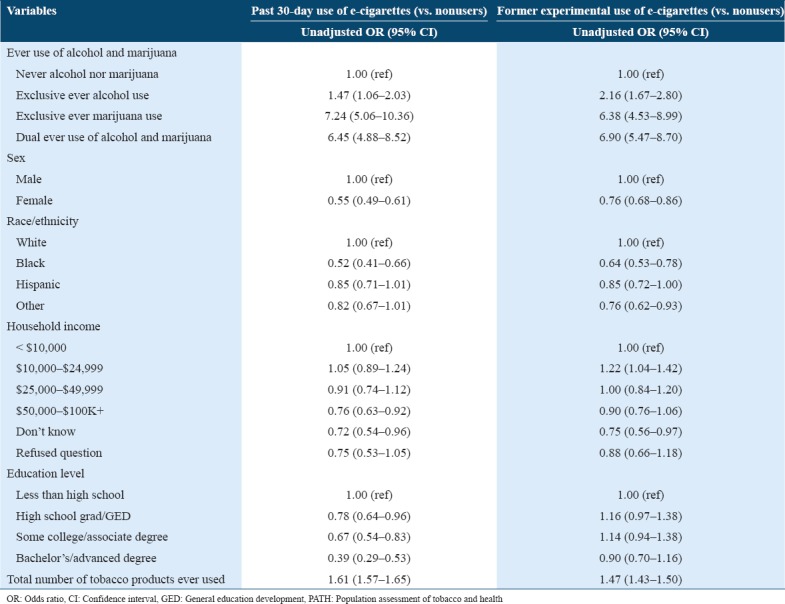
Table 3.
Adjusted multiple logistic regression models of alcohol use and marijuana use on e-cigarette use outcomes in the PATH 2013–2014 sample of young adults (ages 18–24)
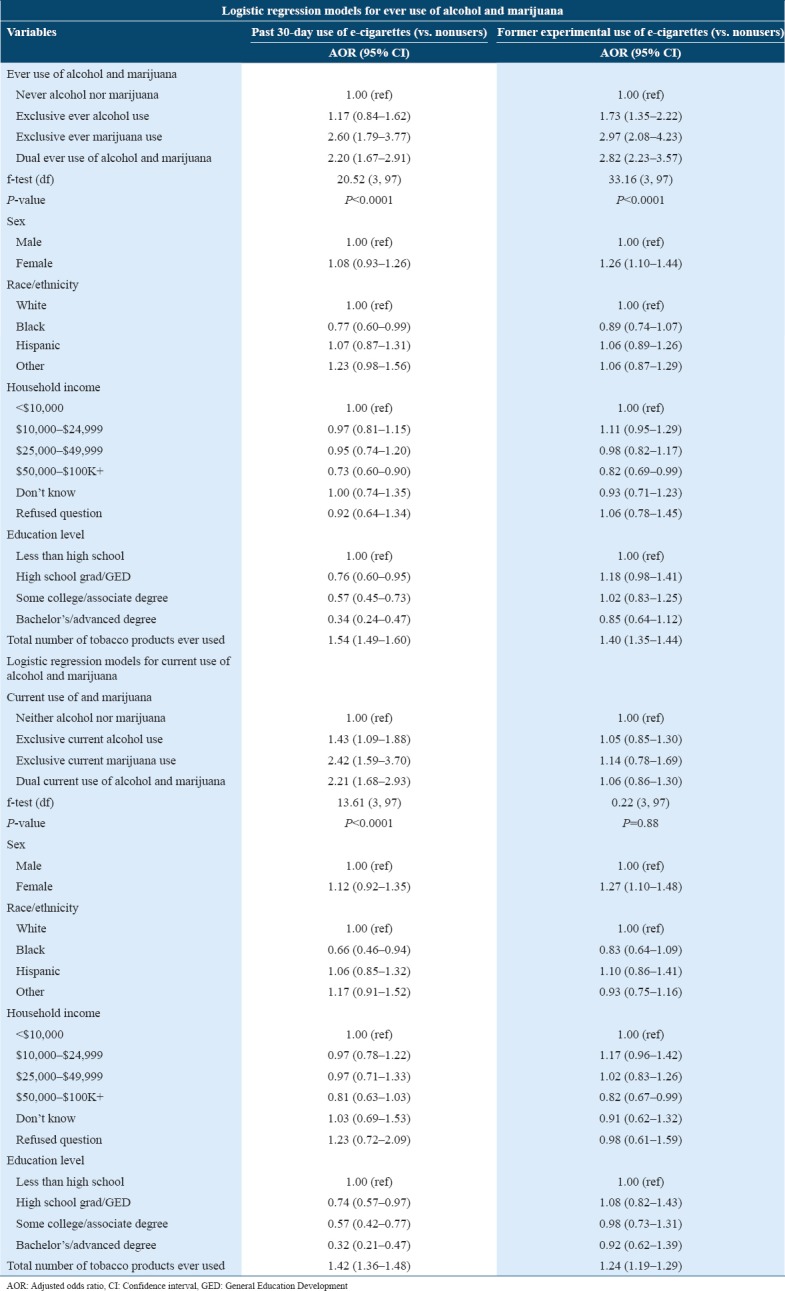
After adjusting for covariates, dual ever use of alcohol and marijuana remained associated with past 30-day e-cigarette use (AOR = 2.20; 95% confidence interval [CI] = 1.67–2.91). In addition, the odds of past 30-day e-cigarette use were 2.60 (95% CI = 1.79–3.77) times higher in exclusive ever marijuana users compared to participants who had never used alcohol or marijuana. However, exclusive ever alcohol use was not significantly associated with past 30-day e-cigarette use (AOR = 1.17; 95% CI = 0.84–1.62). It should be noted that the odds of past 30-day e-cigarette use among exclusive ever marijuana users were higher than the odds ratio for e-cigarette use among young adult dual ever alcohol and marijuana users, as well as young adults who were exclusive ever alcohol users. In addition, while other tobacco use was hypothesized to have a strong relationship with e-cigarette use, the odds of past 30-day e-cigarette use among young adults who had ever used other tobacco products were 1.54 (95% CI = 1.49-1.60), which shows that exclusive ever marijuana use and dual ever use of alcohol and marijuana were more strongly associated with past 30-day e-cigarette use.
After adjusting for covariates, the odds of past 30-day e-cigarette use were 2.21 (95% CI = 1.68–1.93) times higher in dual current users of alcohol and marijuana compared to young adults who had not used alcohol or marijuana in the past 30 days. In addition, the odds of past 30-day e-cigarette use were significantly higher in participants who were exclusive current alcohol users (AOR = 1.43; 95% CI = 1.09–1.88), and exclusive current marijuana users exhibited the highest odds of past 30-day e-cigarette use (AOR = 2.42; 95% CI = 1.59–3.70). While other tobacco product use was significantly associated with past 30-day e-cigarette use (AOR = 1.42; 95% CI = 1.09–1.88), both exclusive current marijuana use and dual current use of alcohol and marijuana were more strongly associated with past 30-day e-cigarette use.
After adjusting for covariates, the odds of former experimental e-cigarette use were 2.82 (95% CI= 2.23–3.57) times higher in dual ever users of alcohol and marijuana compared to never users of alcohol or marijuana. In addition, the odds of former experimental e-cigarette use were significantly higher in participants who were exclusive ever alcohol users (AOR = 1.73; 95% CI = 1.35–2.22), as well as participants who were exclusive ever marijuana users, compared to those who had never used alcohol or marijuana (AOR= 2.97; 95% CI = 2.08–4.23). It should also be noted that while other tobacco product use was significantly associated with former experimental e-cigarette use (AOR = 1.37; 95% CI = 1.35–1.44), all categories of ever alcohol and ever marijuana use were more strongly associated with this type of e-cigarette use.
After adjusting for covariates, none of the combinations of exposure to current alcohol and/or marijuana use were significantly associated with former experimental e-cigarette use (F-test = 0.22, df = 3, 97 P = 0.88), or there may not have been enough sample size across the categories of exposure to detect a difference. However, other tobacco product use remained significantly associated with former experimental e-cigarette use in the adjusted model (AOR = 1.24; 95% CI = 1.19–1.29).
Discussion
This study adds to the literature by identifying patterns between risky substance use behaviors and an emerging class of tobacco products. Specifically, we found that dual ever alcohol and marijuana use increased the odds of past 30-day and former experimental e-cigarette use and that dual current alcohol and marijuana use significantly increased the odds of past 30-day e-cigarette use. Our findings extend previous research by finding that dual use of both alcohol and marijuana significantly increased the odds of past 30-day e-cigarette use and former experimental e-cigarette use, rather than looking at the contribution of each type of substance use separately. These findings are consistent with a study of college students which found that marijuana use significantly increased odds of past 30-day e-cigarette use (AOR = 2.37; CI = 1.69–3.31).[7] In addition, our overall findings are similar to research by Cohn et al. and colleagues, who found that alcohol use every day/some days (AOR = 9.03, 95% CI: 2.18–37.36) and marijuana use every day/some days (AOR = 3.30; 95% CI: 1.56–6.43) were each significantly associated with e-cigarette use.[11] However, it should be noted that the pattern of results in this study is different from the study by Cohn et al. and colleagues: Exclusive ever and exclusive current marijuana use were the exposures that had the highest odds ratios for e-cigarette use, while alcohol users exhibited the highest odds of e-cigarette use in their study. It should also be noted that both current and ever exclusive alcohol use exhibited the lowest odds ratios across the e-cigarette outcomes. The findings that exclusive ever alcohol use was not significantly associated with past 30-day e-cigarette use, as well as that exclusive current alcohol use was not associated with former experimental e-cigarette use, are similar to a previous research study which also found no associations between ever alcohol use and past 30-day alcohol use with past 30-day e-cigarette use.[7] Alcohol use is a highly prevalent behavior, and it is possible that e-cigarette users do not differ from non-users of e-cigarettes in terms of alcohol use in this nationally representative study sample.
Despite being the exposure group with the smallest sample size, both ever and current exclusive marijuana users had the highest odds of past 30-day e-cigarette use, and ever exclusive marijuana users had highest odds of former experimental e-cigarette use. This was contrary to our original hypothesis that dual users of alcohol and marijuana would exhibit the highest odds of e-cigarette use. It is possible that this association can be explained by the fact that e-cigarette devices can be filled with marijuana oils instead of nicotine solution. Users report that this emerging mode of marijuana administration is better tasting, more efficient, and cost-effective, and users report a perceived reduction in respiratory harm.[22] Previous research has shown that among states without medical marijuana laws 53.8% of marijuana users reported ever use of an e-cigarette device to vape marijuana, while 68.6% of marijuana users living in states with medical marijuana laws reported ever use of an e-cigarette device to vape marijuana.[23] This indicates that research on e-cigarette devices being used to vape marijuana is an important trend to watch, as more states are legalizing marijuana for medical and recreational use. The mode of marijuana administration is not available in PATH wave 1, and therefore, was not assessed in this study, and future researchers should consider whether e-cigarette users are using their e-cigarette devices to also vape marijuana when examining this association. Our findings indicate that exclusive marijuana users may be a group that is particularly vulnerable to e-cigarette use, and intervention campaigns should target marijuana users directly.
There are several additional explanations that can account for the significant findings in this study. First, previous research has shown that reasons for e-cigarette use include curiosity and experimentation,[24] and experimentation with e-cigarettes is associated with sensation seeking,[11] which is a trait typically associated with alcohol and marijuana users.[25] Second, research has established that individuals who use psychoactive substances have increased odds of using more than one substance, and our findings suggest e-cigarette use is a component of poly-substance use and poly-tobacco use.[26] In this study, past 30-day e-cigarette users had tried the highest number of tobacco products (m = 4.25), indicating a willingness to experiment with different tobacco products, which could lead to the current use of tobacco products that have well-known adverse health effects such as cigarettes. Third, research has indicated that young adults who use with alcohol and marijuana are more likely than non-users to prescribe to the view that alcohol, marijuana, and tobacco products are not harmful.[27,28] Finally, the observed associations between ever and current use of alcohol and marijuana with e-cigarette use are in alignment with the emerging adulthood hypothesis, which states that emerging adulthood (ages 18–25) is the developmental period characterized by the highest amount of substance use compared to other age groups, as well as the initiation of tobacco products.[29]
Strengths and limitations
There are substantial gaps in the literature in regard to how alcohol and marijuana use contributes to e-cigarette use among a national sample of U.S.A. young adults. This study helped to fill in that gap by examining the associations of alcohol and marijuana use contemporaneously, in a nationally representative sample. By considering participants’ dual use of alcohol and marijuana, we were able to identify how these associations vary compared to the exclusive use of each substance. Finally, most of the other research on e-cigarette use analyzed past 30-day use or ever use, while the current study includes former experimental e-cigarette users. Importantly, former experimental users constituted a significant proportion of the total study sample (16.0%) and featured strong associations with dual ever use of alcohol and marijuana, as well as exclusive use of each substance, so researchers in the future should examine this group thoroughly to determine if this subgroup represents a particular type of experimental substance user. Individuals who use psychoactive substances are at risk for using a variety of substances that can result in adverse health outcomes (i.e., respiratory and cardiovascular damage from nicotine, liver damage and cardiovascular disease from alcohol, attention, and learning and memory deficits from marijuana), and future interventions should be designed that comprehensively target poly-substance users instead of targeting the use of these substances separately.
This study also included some limitations. First, it was secondary data analysis, so it was limited to the self-reported data that were collected by the initial researchers. Second, we used a cross-sectional design, so causality and directionality cannot be determined. Future researchers should consider the longitudinal nature of the associations presented in this study. In addition, using e-cigarette devices to vape marijuana were not measured in PATH wave 1, and future researchers should examine if this behavior is a confounder in the association between marijuana use and e-cigarette use. Finally, previous research has shown that sensation seeking, and impulsivity may be confounders in tobacco use behaviors, but their contributions in associations were not addressed here because they were not included in the PATH wave one public data.
Conclusion
Given that associations between dual use of alcohol and marijuana with e-cigarette use outcomes remained significant after controlling for covariates, we show that ever and current users of alcohol and marijuana exhibit increased odds of e-cigarette use, which have been shown to usually contain nicotine and other potentially toxic chemical constituents that have not been fully assessed for safety when inhaled.[30] The consistent findings across both ever and current use of alcohol and marijuana provide strong evidence that these behaviors are associated with e-cigarette use. More research is needed to determine if these three behaviors cooccur, and to assess longitudinal patterns in young adults. Public health prevention programs should target young adults who are at risk of using all three substances to comprehensively address young adult substance use, rather than programs that target the use of these substances separately, as well as intervening before individuals become binge drinkers or heavy marijuana users. Marijuana users, in particular, may represent an important subgroup to target with intervention campaigns since this group exhibited the highest odds of e-cigarette use, above and beyond the dual use of marijuana and alcohol. Strategies that could address these substance use behaviors include raising the minimum age of tobacco sales, mass-reach health communication interventions using social media and other platforms used by young adults[31] and event-based strategies (i.e., intervention campaigns conducted in bars, clubs, and music concerts)[32] to dissuade use among young adults in the places where substance use is likely to occur. In conclusion, the associations between both ever and current use of alcohol and marijuana with e-cigarette use across different e-cigarette users reveal that these types of substance users are important subpopulations to target in public health interventions aimed at reducing the public health burden accounted for by e-cigarettes.[17]
Acknowledgments
We would like to thank the original researchers of the PATH for their hard work and for making their data publicly available, as well as the participants of the study.
References
- 1.In:Services USDoHaH, editor. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2016. E-cigarette Use Among Youth and Young Adults. A Report of the Surgeon General. [Google Scholar]
- 2.Hedden SL, Kennet J, Lipari R, Medley G, Tice P. Behavioral Trends in the United States:Results from the 2014 National Survey on Drug Use and Health. 2015 [Google Scholar]
- 3.Richardson A, Williams V, Rath J, Villanti AC, Vallone D. The next generation of users:Prevalence and longitudinal patterns of tobacco use among US young adults. Am J Public Health. 2014;104:1429–36. doi: 10.2105/AJPH.2013.301802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hyland A, Ambrose BK, Conway KP, Borek N, Lambert E, Carusi C, et al. Design and methods of the population assessment of tobacco and health (PATH) study. Tob Control. 2017;26:371–8. doi: 10.1136/tobaccocontrol-2016-052934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Prevention CfDCa. National Adult Tobacco Survey 2013-2014 (unpublished data) 2013-2014 [Google Scholar]
- 6.Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. 2000;55:469–80. [PubMed] [Google Scholar]
- 7.Saddleson ML, Kozlowski LT, Giovino GA, Hawk LW, Murphy JM, MacLean MG, et al. Risky behaviors, e-cigarette use and susceptibility of use among college students. Drug Alcohol Depend. 2015;149:25–30. doi: 10.1016/j.drugalcdep.2015.01.001. [DOI] [PubMed] [Google Scholar]
- 8.Bluestein M. Exploring Associations Between the use of Psychoactive Substances and e-Cigarettes in a Nationally Representative Sample of Young Adults. Texas Medical Center Dissertations (via ProQuest):The University of Texas Health Science Center at Houston, School of Public Health in Austin (UTHealth) 2017 [Google Scholar]
- 9.Bachman J, O'Malley P, Johnston L, Schulenberg J. Smoking, Drinking, and Drug Use in Young Adulthood. New York: Psychology Press; 1997. [Google Scholar]
- 10.In:Services USDoHaH, editor. A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2016. US Department of Health and Human Services. E-cigarette Use Among Youth and Young Adults. [Google Scholar]
- 11.Cohn A, Villanti A, Richardson A, Rath JM, Williams V, Stanton C, et al. The association between alcohol, marijuana use, and new and emerging tobacco products in a young adult population. Addict Behav. 2015;48:79–88. doi: 10.1016/j.addbeh.2015.02.005. [DOI] [PubMed] [Google Scholar]
- 12.Richardson A, Rath J, Ganz O, Xiao H, Vallone D. Primary and dual users of little cigars/cigarillos and large cigars:Demographic and tobacco use profiles. Nicotine Tob Res. 2013;15:1729–36. doi: 10.1093/ntr/ntt053. [DOI] [PubMed] [Google Scholar]
- 13.Moss HB, Chen CM, Yi HY. Early adolescent patterns of alcohol, cigarettes, and marijuana polysubstance use and young adult substance use outcomes in a nationally representative sample. Drug Alcohol Depend. 2014;136:51–62. doi: 10.1016/j.drugalcdep.2013.12.011. [DOI] [PubMed] [Google Scholar]
- 14.Bernat DH, Klein EG, Forster JL. Smoking initiation during young adulthood:A longitudinal study of a population-based cohort. J Adolesc Health. 2012;51:497–502. doi: 10.1016/j.jadohealth.2012.02.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Loukas A, Marti CN, Cooper M, Pasch KE, Perry CL. Exclusive e-cigarette use predicts cigarette initiation among college students. Addict Behav. 2018;76:343–7. doi: 10.1016/j.addbeh.2017.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hecht SS, Carmella SG, Kotandeniya D, Pillsbury ME, Chen M, Ransom BW, et al. Evaluation of toxicant and carcinogen metabolites in the urine of e-cigarette users versus cigarette smokers. Nicotine Tob Res. 2015;17:704–9. doi: 10.1093/ntr/ntu218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Preventing Tobacco use Among Youth and Young Adults:A Report of the Surgeon General. Rockville: US Department of Health and Human Services CfDCaP, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2012. [Google Scholar]
- 18.Carroll Chapman SL, Wu LT. E-cigarette prevalence and correlates of use among adolescents versus adults:A review and comparison. J Psychiatr Res. 2014;54:43–54. doi: 10.1016/j.jpsychires.2014.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Temple JR, Shorey RC, Lu Y, Torres E, Stuart GL, Le VD, et al. E-cigarette use of young adults motivations and associations with combustible cigarette alcohol, Marijuana, and other illicit drugs. Am J Addict. 2017;26:343–8. doi: 10.1111/ajad.12530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Perez AT. In: Conduct of Stroke-Related Clinical trials. 6th ed. Mohr JP, Wolf PA, Moskowitz MA, Mayberg MR, Von Kummer R, editors. New York: Churchill Livingstone; 2015. [Google Scholar]
- 21.StataCorp. Stata Statistical Software:Release 14. College Station, TX: StataCorp LP; 2015. [Google Scholar]
- 22.Budney AJ, Sargent JD, Lee DC. Vaping cannabis (marijuana):Parallel concerns to e-cigs? Addiction. 2015;110:1699–704. doi: 10.1111/add.13036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Borodovsky JT, Crosier BS, Lee DC, Sargent JD, Budney AJ. Smoking, vaping, eating:Is legalization impacting the way people use cannabis? Int J Drug Policy. 2016;36:141–7. doi: 10.1016/j.drugpo.2016.02.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Pepper JK, Ribisl KM, Emery SL, Brewer NT. Reasons for starting and stopping electronic cigarette use. Int J Environ Res Public Health. 2014;11:10345–61. doi: 10.3390/ijerph111010345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Verdejo-García A, Lawrence AJ, Clark L. Impulsivity as a vulnerability marker for substance-use disorders:Review of findings from high-risk research, problem gamblers and genetic association studies. Neurosci Biobehav Rev. 2008;32:777–810. doi: 10.1016/j.neubiorev.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 26.Olthuis JV, Darredeau C, Barrett SP. Substance use initiation:The role of simultaneous polysubstance use. Drug Alcohol Rev. 2013;32:67–71. doi: 10.1111/j.1465-3362.2012.00470.x. [DOI] [PubMed] [Google Scholar]
- 27.Agaku I, Omaduvie U, Vardavas C, Filippidis F. Cannabis use is associated with reduced harm perception towards illicit drugs and experimentation with new psychoactive substances among European adolescents and young adults. Eur Respir J. 2015;46(suppl 59):46–54. [Google Scholar]
- 28.Pedersen W, Fjaer EG, Gray P, Soest Tv. Perceptions of harms associated with tobacco, alcohol, and cannabis among students from the UK and Norway. Contemp Drug Probl. 2016;43:47–61. [Google Scholar]
- 29.Thompson AB, Mowery PD, Tebes JK, McKee SA. Time trends in smoking onset by sex and race/ethnicity among adolescents and young adults:Findings from the 2006-2013 national survey on drug use and health. Nicotine Tobacco Res. 2018;20:312–20. doi: 10.1093/ntr/ntx010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stratton K, Kwan LY, Eaton DL, editors. Public Health Consequences of E-Cigarettes. Washington, DC: The National Academies Press; 2018. National Academies of Sciences E, Medicine; p. 680. [PubMed] [Google Scholar]
- 31.Robinson MN, Tansil KA, Elder RW, Soler RE, Labre MP, Mercer SL, et al. Mass media health communication campaigns combined with health-related product distribution:A community guide systematic review. Am J Prev Med. 2014;47:360–71. doi: 10.1016/j.amepre.2014.05.034. [DOI] [PubMed] [Google Scholar]
- 32.Leibel K, Lee JG, Goldstein AO, Ranney LM. Barring intervention? Lesbian and gay bars as an underutilized venue for tobacco interventions. Nicotine Tob Res. 2011;13:507–11. doi: 10.1093/ntr/ntr065. [DOI] [PubMed] [Google Scholar]