

Abstract
Rationale:
Dislocation of the distal radioulnar joint and injury to distal forearm are commonly encountered. However, delayed diagnosis or misdiagnosis has been relatively rare due to improved diagnosis and treatment. Treatment of old dislocation of radioulnar joint is challenging due to development of secondary chronic instability and difficulties in restoration of joint function.
Patient concerns:
This report describes three cases of patients complained about inability to extend their little fingers.
Diagnoses:
Local examination and X-ray revealed chronic ulnar joint dislocation.
Intervention:
Wrist arthroplasty was used to perform ulnar distal articular cleansing and repair of the triangular fibrocartilage complex (TFCC) articular cartilage. The Sauve-Kapandji osteotomy was performed to treat radial joint dislocation and stabilize ulnar joint. Repair of spontaneous fracture of the extensor tendon was also performed. Postoperative gypsum was used for immobilization for 4 weeks.
Outcomes:
The follow-up results are reported. Based on Cooney wrist score, the preoperative scores were poor (55, 50, 60), while the post-operative scores were excellent (90, 85, 90) in all 3 cases.
Lessons:
Early and accurate diagnosis and treatment is important for the recovery of distal radius fracture for patients with dislocation of the ulnar joint. The correct treatment determines the degree of later functional recovery. Early surgical treatment is recommended for patients with unsatisfactory reset. Delayed diagnosis and treatment often lead to chronic and persistent lower ulnar joint subluxation or dislocation, or even osteoarthritis. All patients in this report showed great improvement in wrist function after surgery.
Keywords: old ulnar joint dislocation, Sauve–Kapandji osteotomy, spontaneous tendon rupture, wrist arthroscopy
1. Introduction
Traumatic dislocation of the distal radioulnar joint and injury to distal forearm are commonly encountered.[1] Due to improved diagnostic and therapeutic techniques, delayed diagnosis or misdiagnosis has been relatively rare. Treatment of old dislocation of radioulnar joint is challenging because of secondary chronic instability, difficulties in functional restoration, and unsatisfactory outcomes of conservative treatment.[2] The commonly reported complications include chronic wrist pain, loss of grip, and limited forearm rotation function.[3] However, spontaneous rupture of extensor tendon is rare. In this case series report, we describe 3 patients with chronic ulnar joint dislocation who were treated by Sauve–Kapandji osteotomy assisted by wrist arthroscopy.
2. Methods
The study protocol was reviewed and approved by the institutional ethical committee. Written consent was obtained from all patients.
2.1. Surgical procedure
For all 3 patients, debridement of the articular cavity of the distal radioulnar joint and repair of the triangular fibrocartilage complex (TFCC) articular cartilage were performed with wrist arthroplasty assistance. Patients were placed in the supine position, with the affected upper limb extended outside the booth. Hand surgical finger hinge suspension traction was used. A 2.7 mm tilt 30° arthroscopic operation was used. A 10-gauss needle was inserted into the space between the small extensor tendon and the total extensor tendon as reference for insertion of arthroscope. On arthroscopic examination, synovial hyperplasia, partial congestion, TFCC wear, triangular articular surface, and ulnar styloid cartilage wear were observed. The synovium was cleaned and the articular surface was repaired.
Sauve–Kapandji surgical treatment[4] was used for ulnar joint dislocation, to stabilize ulnar joint. The incision was made over the ulnar curvature. Ulnar small head was separated to protect the dorsal branch of the ulnar nerve. [5, 6] Extensor tendon sheaths were isolated and opened. Ulnar flexor tendon was pulled to the ulnar side, while the extensor tendon was pulled to the radial side. The joint capsule was cut open, displaying the small head of the ulna and the lower end of the radial joint. Bite forceps was used to excise the articular cartilage of the radioulnar joint in the articular surface. About 1.5 cm of ulna was cut at a distance of 3 cm from the distal end of radial joint. The distal ulna was restored to the normal position. The lower radius of the radial joint was fixed with two 3.5 mm hollow screws. Distal end of ulna was wrapped with ulnar brachial tendon and periosteum at the osteotomy site. Broken fingers extensor tendon was cleaned and repaired. Postoperative gypsum fixation was applied for 4 weeks. The wrist mass was examined. Cystic joint fluid was removed.
2.2. Treatment after surgery
Wound dressing was changed every alternate day and stitches were removed 2 weeks after surgery. Gypsum was removed and functional exercises were introduced 4 weeks after surgery.
2.3. Follow-up assessment
Cooney wrist score[5] was used to evaluate the wrist function with respect to pain, function, range of motion, flexion/extension activity, grip strength, and rotation. Accordingly, excellent score was 90 to 100, good 80 to 89, 65 to 79, poor < 65 points.
3. Results
A total of 3 patients are included in this report. Follow-up was performed at 18, 12, and 6 months for all patients. The preoperative Cooney wrist score scores were poor, while the postoperative scores were excellent in all 3 patients.
3.1. Case 1
A 71-year-old woman was hospitalized because of the inability to extend the left little finger. The patient had sustained trauma to left wrist 20 years ago, which was left untreated. One month before hospitalization, she developed sudden pain on the ulnar side of wrist accompanied by local lumps and inability to extend the left little finger. On local examination, there was tenderness on ulnar side of the left wrist joint and a 2 × 2 cm cystic mass was observed on the dorsal aspect of the left wrist. Movements at the left wrist joint and forearm rotation were limited; dorsiflexion of the left little finger metacarpophalangeal joint was obstructed. X-ray showed distal ulnar distal fracture and lower ulnar joint dislocation. Diagnosis revealed old lower ulnar joint dislocation, ulnar impact syndrome, and left small extensor tendon spontaneous rupture. The preoperative Cooney wrist score was 55 (poor), while the postoperative score was 90 (excellent). Detailed scores are listed in Table 1. Images of this case are shown in Fig. 1.
Table 1.
Summary of case 1.
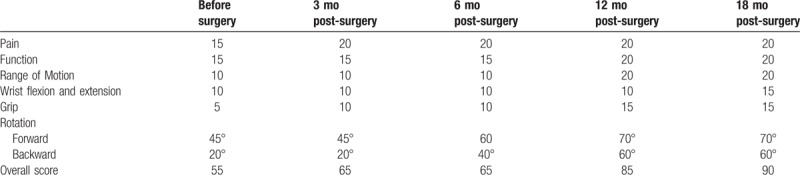
Figure 1.
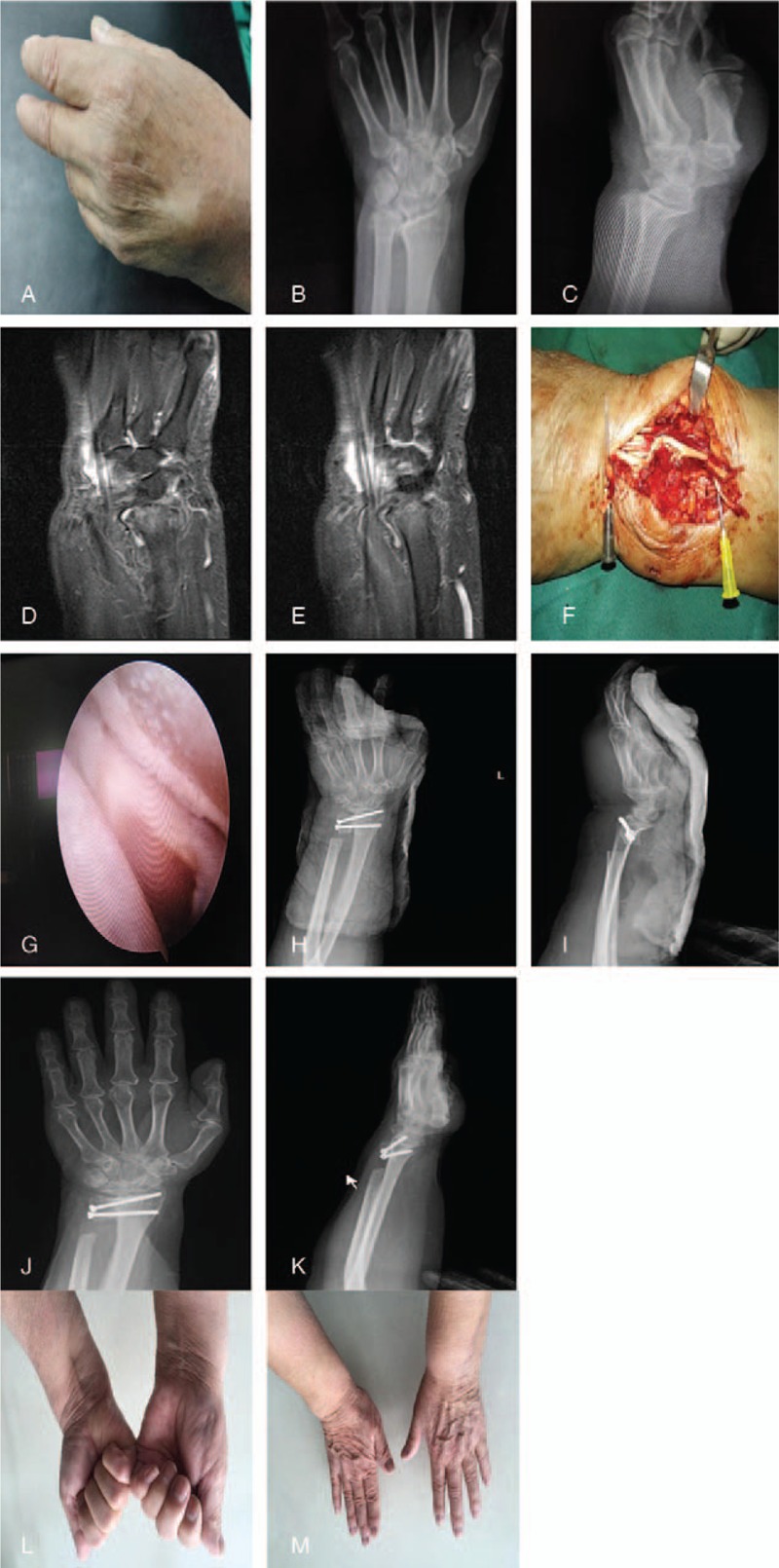
Case 1: A 71-year-old woman hospitalized due to left little finger extension obstruction for more than 1 month. Diagnosis: old ulnar joint dislocation, ulnar impact syndrome, and spontaneous rupture of the left small extensor tendon. Distal ulnar articular cleft and TFCC articular cartilage repair was performed assisted by wrist arthroscopy. Sauve–Kapandji osteotomy was performed to treat ulnar joint dislocation, stabilize the ulnar joint; spontaneous fracture of the extensor tendon was repaired. (A–E) General view, X-ray, and MRI images of wrist before surgery; (F) intraoperative view of the broken tendon; (G) wrist arthroscopy revealed intra-articular synovial hyperplasia; (H, I): front and lateral X-ray of wrist immediately after the surgery; (J, K) front and lateral X-ray of wrist 6 months after surgery; (L, M) patient's wrist and finger activity, 6 months after surgery.
3.2. Case 2
A 79-year-old woman was hospitalized because of inability to extend the right little finger since 1 year. She complained of inability to extend the right little finger and pain in the right wrist ulnar distal end since 1 year; however, she did not seek any medical treatment. Local examination revealed a cystic mass of about 3 × 6 cm on the dorsal aspect of the right wrist and tenderness on the ulnar side of the right wrist joint; other findings included fixation of ulnar distal elasticity, laxity of distal radioulnar joint, limited forearm rotation, and little finger metacarpophalangeal joint activity. X-ray showed dislocation of the distal radioulnar joint and osteophyte formation, and distal to dorsal ulnar shift. Diagnosis revealed old distal ulnar joint dislocation with osteoarthritis and spontaneous rupture of right ring finger extensor tendon. The preoperative Cooney wrist score was 50 (poor), while the postoperative score was 85 (excellent). Detailed scores are listed in Table 2. Images of this patient are shown in Fig. 2.
Table 2.
Summary of case 2.
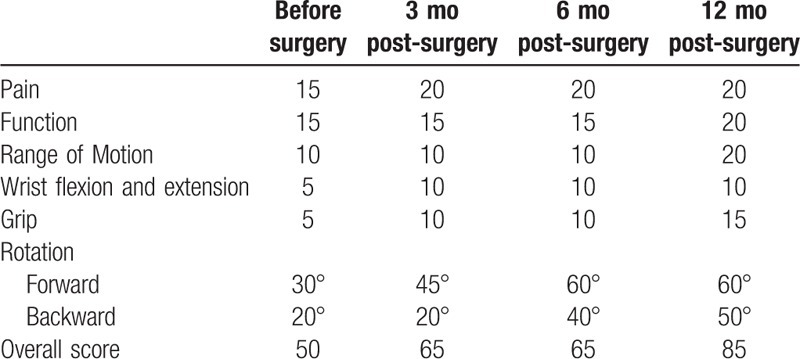
Figure 2.

Case 2: A 79-year-old woman hospitalized due to inability to extend the right little finger since 1 year. Diagnosis: old distal ulnar joint dislocation with osteoarthritis and spontaneous rupture of right ring finger extensor tendon. Distal ulnar articular cleft and TFCC articular cartilage repair was performed assisted by wrist arthroscopy. Sauve–Kapandji osteotomy was performed to treat ulnar joint dislocation, stabilize the ulnar joint; spontaneous fracture of the extensor tendon was repaired. (A–E) General view, X-ray, CT, and MRI images of wrist before surgery; (F) intraoperative view of the broken tendon; (G) wrist arthroscopy revealed intra-articular synovial hyperplasia; (H) general view of patient's hand immediately after the surgery; (I, J) front and lateral X-ray of wrist immediately after the surgery; (K, L) patient's wrist and finger activity, 6 months after surgery.
3.3. Case 3
A 54-year-old man was hospitalized because of right hand injury and inability to extend the right little finger. The patient injured his right hand with heavy weight about 6 months ago. Swelling of the affected area and restricted movements of right hand were observed. The patient was treated at a local hospital. X-ray did not show any obvious fracture. Nine days before hospitalization, the patient developed restricted extension of right little finger. Local examination revealed impaired dorsiflexion at the right auscium metacarpophalangeal joint, tenderness over the right ulnar styloid process, distal radioulnar joint relaxation, and limited rotation at the wrist joint. X-ray showed lower right ulnar joint dislocation. Diagnosis revealed old distal ulnar joint dislocation with spontaneous rupture of right little finger extensor tendon. The preoperative Cooney wrist score was 60 (poor), while the postoperative score was 90 (excellent). Detailed scores are listed in Table 3. Images of this patient are shown in Fig. 3.
Table 3.
Summary of case 3.
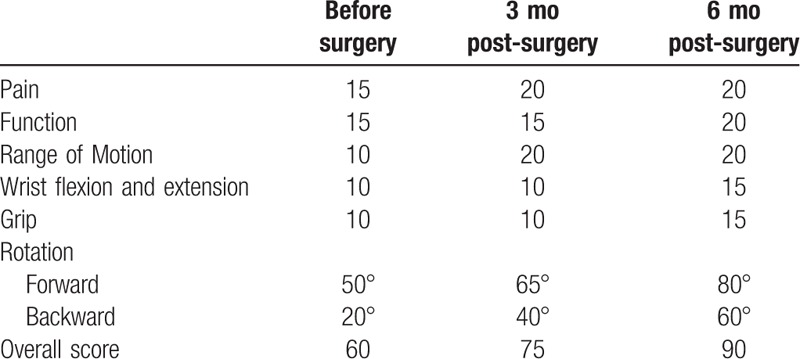
Figure 3.

Case 3: A 54-year-old man hospitalized due to right hand injury and inability to extend the right little finger. Diagnosis: old distal ulnar joint dislocation with spontaneous rupture of right little finger extensor tendon. Distal ulnar articular cleft and TFCC articular cartilage repair was performed assisted by wrist arthroscopy. Sauve–Kapandji osteotomy was performed to treat ulnar joint dislocation, stabilize the ulnar joint; spontaneous fracture of the extensor tendon was repaired. (A–E) General view, X-ray, CT, and MRI images of wrist before surgery; (F) intraoperative view of the broken tendon; (G) wrist arthroscopy revealed intra-articular synovial hyperplasia; (H, I) front and lateral X-ray of wrist immediately after the surgery; (J, K) patient's wrist and finger activity, 6 months after surgery.
4. Discussion
The ulnar radial joint is a trochlear joint, which facilitates forearm pronation. The soft tissue of forearm interosseous membrane, the lower ulnar joint capsule, the articular disc, the TFCC, the lower radial ligament, and the ulnar wrist extensor, all play an important role in maintaining the stability of the ulnar joint.[6] Studies have shown that posterior rotation generates tension in the dorsal lateral ulnar ligament, which shifts ulna to the dorsal side, while pronation generates tension in the radial ligament of the palm side, which shifts ulnar to the palmar side.[2,7] Injury of dorsal joint capsule leads to anteroposterior instability of the ulnar joint, and injury of the palmar side of the joint capsule leads to radial ulnar joint dorsal instability at posterior rotation.[8] Most cases of lower radioulnar joint dislocation have dorsal dislocation, which is due to wrist joint pronation caused by violent impact. Mild cases tend to have only ligament injury, which causes a simple dislocation. Severe cases usually have distal ulnar fractures.[8,9] Fractures of distal radius tend to increase the load on distal ulna, causing ulnar joint mismatch, which results in instability of the distal radioulnar joint (also referred to as the secondary ulnar impact syndrome). Such patients often experience chronic wrist pain, loss of grip, and limited forearm rotation. Two patients in this report showed dorsal shift of the ulna after dislocation; thus, the extensor tendon experienced repeated long-term wear, leading to spontaneous fracture of the tendon and severe ulnar impact syndrome.
Previously, old ulnar joint dislocation was commonly treated with small ulnar resection; however, biomechanical studies have shown that small ulnar resection might lead to wrist instability.[10,11] Radial extension has also been used for the treatment of old radioulnar joint dislocation. Although integrity of the ulna and the inferior radioulnar joint is retained with this method, it is difficult to extend the radius to achieve the desired length, which results in recurrent ulnar dislocation. Soft tissue repair and reconstruction is another approach to treat dislocation of the distal radioulnar joint, such as by rotation of the anterior muscle flap shift; however, the surgery may cause muscular avulsion, and result in decreased muscle tension and recurrence of lower ulnar dislocation.[12] With Sauvé–Kapandji surgery, the ulnar head and radial incision were fused to ensure the integrity of the lower radial joint and radial wrist joint structure, thus avoiding ulnar instability at the wrist. Through the formation of pseudo-joint, rotation function of forearm is better recovered. The normal wrist axial load, function of the wrist tendon, and the normal shape of the wrist are also maintained.[13] This treatment reduces ulnar joint instability caused by impact of ulnar and cartilage injury. Most common complication after Sauvé–Kapandji surgery is the instability of the proximal ulna. Ross et al[11] have reported 33% incidence rate of proximal ulnar instability after Sauvé–Kapandji surgery. Stabilization of the ulna after Sauvé–Kapandji surgery is still a challenge for the treatment of ulnar joint dislocation.
For patients with dislocation of the ulnar joint, early and accurate diagnosis and treatment plays a vital role in the recovery of distal radius of fracture. For patients with distal radius fractures, the correct treatment determines the degree of later functional recovery. For patients with unsatisfactory reset, early surgical treatment is recommended. Delayed diagnosis and treatment often lead to chronic and persistent lower ulnar joint subluxation, dislocation, or even osteoarthritis. For patients with chronic arthritis, arthroplasty can be used to relieve pain.[14,15]
To conclude, all 3 patients described in this report showed great improvement in wrist function after surgery; however, more experience is required to confirm the clinical efficacy of this surgical procedure.
Author contributions
Conceptualization: Hui Qian, Zongbao Liu.
Formal analysis: Guozhao Chen.
Funding acquisition: Guozhao Chen.
Supervision: Guozhao Chen, Zongbao Liu.
Validation: Guozhao Chen.
Writing – original draft: Hui Qian, Guozhao Chen, Zongbao Liu.
Writing – review & editing: Hui Qian, Zongbao Liu.
Footnotes
Abbreviations: MRI = magnetic resonance imaging, TFCC = triangular fibrocartilage complex.
The study was self-funded.
The authors report no conflicts of interest.
References
- [1].George AV, Lawton JN. Management of complications of forearm fractures. Hand Clin 2015;31:217–33. [DOI] [PubMed] [Google Scholar]
- [2].Thomas BP, Sreekanth R. Distal radioulnar joint injuries. Indian J Orthop 2012;46:493–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Pritsch T, Moran SL. The management of congenital and acquired problems of the distal radioulnar joint in children. Hand Clin 2010;26:579–91. [DOI] [PubMed] [Google Scholar]
- [4].Fujita S, Masada K, Takeuchi E, et al. Modified Sauve-Kapandji procedure for disorders of the distal radioulnar joint in patients with rheumatoid arthritis. Surgical technique. J Bone Joint Surg Am 2006;88(suppl 1):24–8. [DOI] [PubMed] [Google Scholar]
- [5].Willis AA, Berger RA, Cooney WP3rd. Arthroplasty of the distal radioulnar joint using a new ulnar head endoprosthesis: preliminary report. J Hand Surg Am 2007;32:177–89. [DOI] [PubMed] [Google Scholar]
- [6].Mizuseki T, Ikuta Y. The dorsal carpal ligaments: their anatomy and function. J Hand Surg Br 1989;14:91–8. [DOI] [PubMed] [Google Scholar]
- [7].Ehman EC, Hayes ML, Berger RA, et al. Subluxation of the distal radioulnar joint as a predictor of foveal triangular fibrocartilage complex tears. J Hand Surg Am 2011;36:1780–4. [DOI] [PubMed] [Google Scholar]
- [8].Tse WL, Lau SW, Wong WY, et al. Arthroscopic reconstruction of triangular fibrocartilage complex (TFCC) with tendon graft for chronic DRUJ instability. Injury 2013;44:386–90. [DOI] [PubMed] [Google Scholar]
- [9].Stoffelen D, Fortems Y, De Smet L, et al. Dislocation of the distal radioulnar joint associated with a transstyloid radiocarpal fracture dislocation. A case report and review of the literature. Acta Orthop Belg 1996;62:52–5. [PubMed] [Google Scholar]
- [10].Coulet B, Boretto JG, Allieu Y, et al. Pronating osteotomy of the radius for forearm supination contracture in high-level tetraplegic patients: technique and results. J Bone Joint Surg Br 2010;92:828–34. [DOI] [PubMed] [Google Scholar]
- [11].Ross M, Thomas J, Couzens G, et al. Salvage of the unstable Sauve-Kapandji procedure: a new technique. Tech Hand Up Extrem Surg 2007;11:87–92. [DOI] [PubMed] [Google Scholar]
- [12].Swigart CR, Badon MA, Bruegel VL, et al. Assessment of pronator quadratus repair integrity following volar plate fixation for distal radius fractures: a prospective clinical cohort study. J Hand Surg Am 2012;37:1868–73. [DOI] [PubMed] [Google Scholar]
- [13].Coughlin TA, Cresswell T. Revision of failed Sauve-Kapandji procedure for Madelung's deformity with an unusual anatomical variant. J Hand Surg Eur Vol 2011;36:158–9. [DOI] [PubMed] [Google Scholar]
- [14].Crosby CA, Reitz JL, Mester EA, et al. Rehabilitation following thumb CMC, radiocarpal, and DRUJ arthroplasty. Hand Clin 2013;29:123–42. [DOI] [PubMed] [Google Scholar]
- [15].Degreef I, De Smet L. The Scheker distal radioulnar joint arthroplasty to unravel a virtually unsolvable problem. Acta Orthop Belg 2013;79:141–5. [PubMed] [Google Scholar]