

Abstract
Objective:
Lipoprotein(a) [Lp(a)] is a well-described risk factor for atherosclerosis, but Lp(a)-associated risk may vary by race/ethnicity. We aimed to determine whether race/ethnicity modifies Lp(a)-related risk of carotid atherosclerotic plaque outcomes among Black, Caucasian, Chinese, and Hispanic individuals.
Approach and Results:
Carotid plaque presence and score were assessed by ultrasonography at baseline (n=5,155) and following a median 9.4 year period (n=3,380) in Multi-Ethnic Study of Atherosclerosis (MESA) participants. Lp(a) concentrations were measured by immunoassay and examined as a continuous and categorical variable using clinically-based cutoffs, 30 and 50 mg/dL. Lp(a) was related to greater risk of prevalent carotid plaque at baseline in Caucasians alone (all p<0.001): per log unit: (RR: 1.05); Lp(a)≥30 mg/dL: (RR: 1.16); Lp(a)≥50 mg/dL: (RR: 1.20). Lp(a) levels over 50 mg/dL were associated with a higher plaque score at baseline in Caucasians (all p<0.001) and Hispanics (p=0.04). In prospective analyses, Caucasians with Lp(a) ≥50 mg/dL were found to have greater risk of plaque progression (RR: 1.12; p=0.03) and higher plaque scores (all p<0.001) over the 9.4 year follow-up. Race-based differences between Caucasians and Black participants were significant for cross-sectional associations and for carotid plaque score following the 9.4 year study period.
Conclusions:
Race was found to be a modifying variable in Lp(a)-related risk of carotid plaque, and Lp(a) levels may have greater influence on plaque burden in Caucasians than in Black individuals. Borderline results in Hispanics suggest that elevated Lp(a) may increase risk of carotid plaque, but follow-up studies are needed.
Keywords: epidemiology, risk factors, cardiovascular disease, race and ethnicity, lipids and lipoproteins, carotid ultrasound, lipoprotein(a), Lp(a), atherosclerosis, carotid plaque, race, MESA
INTRODUCTION
Cardiovascular risk guidelines from the American College of Cardiology Foundation/American Heart Association and the European Society of Cardiology/European Atherosclerosis Society affirm that circulating levels of Lp(a) are an independent risk factor for atherosclerotic cardiovascular disease (ASCVD) (1, 2). Both recent consensus panels and the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol have recommended Lp(a) assessment for individuals at intermediate to high risk of ASCVD (3, 4) and in children with a family history of familial hypercholesterolemia (5). Despite guideline and panel recommendations as well as the nearly ten thousand Lp(a) studies conducted to date, there remain ongoing controversies regarding Lp(a)-related risk and clinical testing.
Currently, there is no universal clinical cutoff value for Lp(a) that discriminates increased risk of ASCVD development. While clinical laboratories in the United States designate elevated Lp(a) levels at 30 mg/dL, the AHA/ACC and European guidelines recommend a threshold of 50 mg/dL (3, 4). Further complicating this designation, Lp(a) may differentially confer risk of ASCVD outcomes depending on race/ethnicity (6–9). It has been reported that Lp(a) is a significant risk factor for calcific aortic valve disease in Caucasian and Black participants, but not in Hispanics or Chinese Americans (6). Lp(a) has further been shown to be related to greater risk of incident heart failure in Caucasian individuals (7). Finally, Lp(a) has been associated with risk of peripheral artery disease in Hispanics and Caucasians, but not in Black or Chinese Americans (9). While no studies have examined race-based differences in Lp(a) and carotid plaque development, research in largely homogeneous populations and with other subclinical atherosclerosis outcomes have shown inconsistent results so far (10–26).
Given the present gaps in the literature, we aimed to interrogate two clinical Lp(a) cutoff values and examine whether race/ethnicity serves as a modifying variable for Lp(a) and risk of carotid atherosclerotic plaque in Multi-Ethnic Study of Atherosclerosis (MESA) participants. The findings may provide additional justification for inclusion of Lp(a) in clinical guidelines, and any observed race/ethnicity-based differences would inform future recommendations and consensus panels.
MATERIALS AND METHODS
The data that support the findings of this study are available from the corresponding author on reasonable request.
Study population
MESA was begun in order to investigate the prevalence and progression of subclinical CVD in individuals free of known clinical CVD, radiation or chemotherapy-treated cancer, other serious major illnesses, or cognitive impairment in the judgment of the screening interviewer prior to baseline (27). Between 2000 and 2002, 6,814 men and women without CVD, aged 45–84 years, and of Caucasian, Black, Hispanic, or Chinese racial/ethnic backgrounds were enrolled from six communities. Institutional Review Board approval was obtained at all MESA sites, and all participants gave informed consent. Further MESA protocol information is available at www.mesa-nhlbi.org.
Demographic, anthropometric, and clinical measurements
Questionnaires were used to obtain information regarding age, sex, race/ethnicity, education, and lifestyle factors including smoking status, physical activity, and dietary intake. Height and weight were measured by trained staff according to standard procedures, and body mass index (BMI) was calculated as weight (kg)/ height (m2). Resting blood pressure was measured using the Dinamap Monitor PRO 100 (Critikon, Tampa, Florida, USA) automated oscillometric device; three measures were taken; the last two measures were averaged and recorded.
Laboratory measurements
Fasting blood was drawn and collected in EDTA-anticoagulant tubes. Samples were aliquoted and stored at −70°C until analyte measurements were conducted. Fasting total cholesterol and high density lipoprotein cholesterol (HDL-C) concentrations were measured as described previously (28). Lp(a) mass concentration was assessed using a latex-enhanced turbidimetric immunoassay (Denka Seiken, Tokyo, Japan) that controls for the size heterogeneity of apo(a) (8).
Imaging
B-mode ultrasonography was conducted at baseline on 5,271 participants (Exam 1 conducted between 2000–2002) and following a median 9.4 years (Exam 5 conducted between 2010–2012) in 3,441 MESA participants, as described by Tattersall et al. (29). Images of the right and left common, bifurcation, and internal carotid arterial segments were obtained and converted into digital records. Images were interpreted by the MESA Carotid Ultrasound Reading Center at the University of Wisconsin. Carotid plaque was defined as focal thickening at least 50% greater than the surrounding intima media or a discrete, focal wall thickening ≥1.5 cm. Kappa values for intra- and inter-reader reproducibility of carotid plaque were respectively 0.83 (95% CI: 0.70–0.96) and 0.89 (95% CI: 0.72–1.00).
Statistical model
Statistical analysis was conducted using Stata (version 15.0, Stata Corp, College Station, TX). Baseline characteristics were presented as means (SD) for continuous variables with normal distributions, medians (interquartile ranges) for continuous variables with skewed distributions, and frequencies (%) for categorical variables. Tukey-Kramer HSD was used to test differences between groups. Lp(a) was examined as a continuous variable (per log unit) and as a categorical variable using two clinical cutoff values (30 and 50 mg/dL). Generalized linear model with log link function was used to estimate the relative risk (RR) per log unit of Lp(a) for the presence of carotid plaque and its progression with 95% confidence intervals (CIs). These outcomes were examined as logistical variables. Carotid plaque score was assessed by the number of carotid plaques (0–12) at both baseline and at the follow-up exam, a median 9.4 years after baseline. Ordered logit regression was used to determine associations of Lp(a) and plaque score. The study sample was stratified by race/ethnicity, and statistical adjustments were made for age, sex, hypertension medication use, lipid lowering medication use, systolic blood pressure, smoking status (never, former, or current), diabetes (as defined by American Diabetes Association criteria), total cholesterol, HDL-C. Individuals with missing covariate data were excluded from analyses. Of the 5,271 participants with baseline ultrasound data, 116 were missing one or more covariates, leaving 5,155 participants for cross-sectional analyses. Of the 3,441 participants with ultrasound measurements at both baseline and at the follow-up exam, 61 were missing one or more covariates, leaving 3,380 participants for prospective analyses. Lp(a)-race interactions were examined by including race/ethnicity as an interaction term in the above regression models. Interactions were deemed significant where p<0.10.
RESULTS
Characteristics of the 5,271 MESA participants of this subcohort are shown in Table 1 and are further stratified by prevalent baseline carotid plaque. Individuals with carotid plaque were more likely to be older, male, Caucasian, former or current smokers, taking hypertension or lipid lowering medication, have diabetes, higher systolic blood pressure, and higher levels of blood lipids including Lp(a) (all p<0.001). The study sample was additionally stratified by race/ethnicity (Supplemental Table I). Across the four races/ethnicities, significant differences were observed in clinical and lifestyle characteristics including Lp(a) and carotid plaque. Black individuals had the highest median Lp(a) levels (p<0.001), while Caucasians showed the highest prevalence of carotid plaque at baseline and following 9.4 years (both p<0.001). Lp(a) distributions of the MESA cohort for each race/ethnicity are presented in Supplemental Figure I (A-D).
Table 1.
Demographic and clinical characteristics of 5,271 MESA participants stratified by the presence or absence of carotid plaque at baseline.
| Factor | All | (−) No plaque | (+)Plaque | p-value |
|---|---|---|---|---|
| N at baseline | 5271 | 2562 | 2709 | |
| Age, years (SD) | 61.8 (10.1) | 58.6 (9.4) | 64.8 (9.8) | <0.001 |
| Sex, n (% female) | 2789 (53.0) | 1427 (55.8) | 1362 (49.7) | <0.001 |
| Race/ethnicity, n (%) | <0.001 | |||
| White | 2028 (38.5) | 873 (34.1) | 1155 (42.7) | |
| Chinese | 630 (12.0) | 388 (15.2) | 242 (8.9) | |
| Black | 1441 (27.4) | 687 (26.8) | 754 (27.8) | |
| Hispanic | 1168 (22.2) | 611 (23.9) | 557 (20.6) | |
| Smoking, n (%) | <0.001 | |||
| Never | 2645 (50.4) | 1440 (56.4) | 1205 (44.6) | |
| Former | 1924(36.6) | 828 (32.4) | 1096 (40.6) | |
| Current | 683 (13.0) | 284 (11.1) | 399 (14.8) | |
| SBP (mm Hg), mean (SD) | 126.4 (21.5) | 122.1 (19.7) | 130.6 (22.3) | <0.001 |
| Hypertension medication, n (%) | 1953 (37.1) | 751 (29.3) | 1202 (44.4) | <0.001 |
| Lipid lowering medication, n (%) | 843 (16.0) | 276 (10.8) | 567 (21.0) | <0.001 |
| Diabetes, n (%) | 645 (12.2) | 214 (8.4) | 431 (16.0) | <0.001 |
| Total cholesterol (mg/dL), mean (SD) | 194.1 (35.6) | 191.9 (34.0) | 196.1 (37.0) | <0.001 |
| HDL-C (mg/dL), mean (SD) | 50.8 (14.9) | 50.9 (14.5) | 50.7 (15.2) | NS |
| Lp(a) (mg/dL), median (IQR) | 17.1 (7.4, 40) | 15.7 (7, 35) | 18.4 (7.8, 44.3) | <0.001 |
Individuals with missing covariate data were excluded. Definitions: MESA= Multi-Ethnic Study of Atherosclerosis; SBP=systolic blood pressure; HDL-C=high density lipoprotein-cholesterol; Lp(a)=lipoprotein(a)
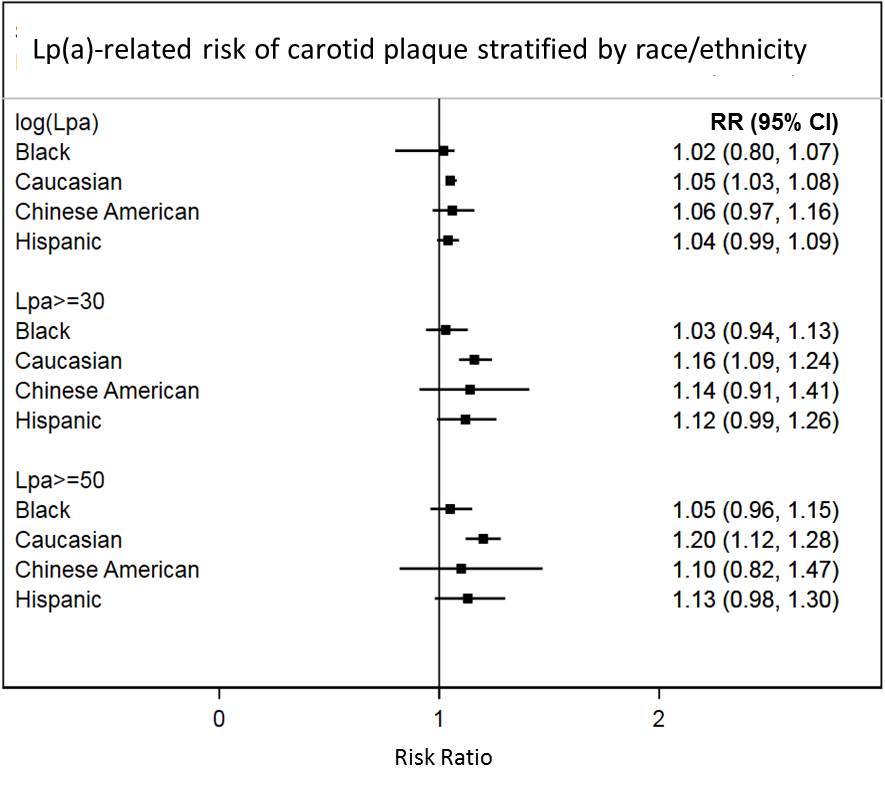
Cross-sectional relations of Lp(a) and baseline carotid plaque are shown in Table 2. Greater Lp(a) levels were related to significantly greater risk of plaque in Caucasians, irrespective of whether Lp(a) was examined as a continuous or categorical variable (all p<0.001). Both clinical cutoff values discriminated risk of plaque in Caucasians. Including race/ethnicity as an interaction term showed significant differences in relations of Lp(a) and prevalent carotid plaque between Caucasian and Black participants: Lp(a)≥30 mg/dL (p for interaction=0.02), and Lp(a)≥50 mg/dL (p for interaction=0.01).
Table 2.
Lp(a)-related risk of carotid plaque at baseline* was assessed in 5,155 Multi-Ethnic Study of Atherosclerosis participants stratified by race/ethnicity.
| Black N=1393 |
Caucasian N=1986 |
Chinese American N=620 |
Hispanic N=1156 |
|
|---|---|---|---|---|
| per Lp(a) log unit | 1.02 (0.80 − 1.07) | 1.05 (1.03 − 1.08) <0.001 |
1.06 (0.97 − 1.16) | 1.04 (0.99 − 1.09) 0.10 |
| Lp(a)≥ 30 mg/dL | 1.03 (0.94 − 1.13) | 1.16 (1.09 − 1.24)† <0.001 |
1.14 (0.91 − 1.41) | 1.12 (0.99 − 1.26) 0.07 |
| Lp(a)≥ 50 mg/dL | 1.05 (0.96 − 1.15) | 1.20 (1.12 − 1.28)† <0.001 |
1.10 (0.82 − 1.47) | 1.13 (0.98 − 1.30) 0.11 |
Risk ratios and 95% confidence intervals are shown, p-values where significant or approaching significance. Covariate adjustments were made for age, sex, systolic blood pressure, hypertension and lipid lowering medication use, total cholesterol, HDL-C, diabetes, and smoking status. Race-interactions were tested between racial/ethnic groups. Individuals with missing covariate data were excluded. Definitions: Lp(a)=lipoprotein(a); diabetes=treated and untreated cases; HDL-C=high density lipoprotein-cholesterol; smoking status=current, former, never
Carotid plaque is modeled as a logistical variable (0 or 1); absent or present at baseline
Significantly different than Black participants (p for interaction<0.10)
Cross-sectional associations of Lp(a) and baseline carotid plaque score as determined by total plaque number are shown in Table 3. Greater Lp(a) levels were related to significantly greater plaque score in Caucasians, irrespective of whether Lp(a) was examined as a continuous or categorical variable (all p<0.001). A significant relationship was also found in Hispanics with Lp(a) ≥50 mg/dL (p=0.04). Including race/ethnicity as an interaction term showed differences in relations of Lp(a) and carotid plaque score between Caucasian and Black participants: per log unit of Lp(a) (p for interaction=0.10), Lp(a)≥30 mg/dL (p for interaction=0.007), and Lp(a)≥50 mg/dL (p for interaction=0.001).
Table 3.
Associations of Lp(a) and baseline plaque score in 5,155 Multi-Ethnic Study of Atherosclerosis participants stratified by race/ethnicity.
| Black N=1393 |
Caucasian N=1986 |
Chinese American N=620 |
Hispanic N=1156 |
|
|---|---|---|---|---|
| per Lp(a) log unit | 0.06 (−0.05 − 0.17) | 0.15 (0.09 − 0.22)† <0.001 |
0.13 (−0.03 − 0.29) | 0.07 (−0.02 − 0.17) |
| Lp(a)≥ 30 mg/dL | 0.11 (−0.10 − 0.32) | 0.47 (0.28 − 0.66)† <0.001 |
0.17 (−0.25 − 0.59) | 0.22 (−0.05 − 0.49) |
| Lp(a)≥ 50 mg/dL | 0.07 (−0.14 − 0.29) | 0.55 (0.34 − 0.76)† <0.001 |
0.25 (−0.31 − 0.81) | 0.33 (0.01 − 0.66) 0.04 |
Regression coefficients and 95% confidence intervals are shown, p-values where significant. Covariate adjustments were made for age, sex, systolic blood pressure, hypertension and lipid lowering medication use, total cholesterol, HDL-C, diabetes, and smoking status. Race-interactions were tested among racial/ethnic groups. Individuals with missing covariate data were excluded. Definitions: Lp(a)=lipoprotein(a); diabetes=treated and untreated cases; HDL-C=high density lipoprotein-cholesterol; smoking status=current, former, never
Modeled as an ordinal variable with plaque score values between 0 to 12
Significantly different than Black participants (p for interaction<0.10)
Prospective associations between Lp(a) and risk of carotid plaque progression over the mean 9.4-year study period are shown in Table 4. Lp(a)-related risk of plaque progression was only found in Caucasians with Lp(a) levels ≥50 mg/dL. There were no race significant interactions.
Table 4.
Lp(a)-related risk of carotid plaque progression* over a median 9.4 year period in 3,380 Multi-Ethnic Study of Atherosclerosis participants stratified by race/ethnicity†.
| Black N=885 |
Caucasian N=1326 |
Chinese American N=435 |
Hispanic N=734 |
|
|---|---|---|---|---|
| per Lp(a) log unit | 1.04 (0.98 − 1.10) | 1.02 (0.99 − 1.05) | 1.01 (0.94 − 1.09) | 0.99 (0.95 − 1.03) |
| Lp(a)≥ 30 mg/dL | 1.02 (0.91 − 1.15) | 1.06 (0.97 − 1.17) | 0.93 (0.76 − 1.12) | 1.02 (0.90 − 1.15) |
| Lp(a)≥ 50 mg/dL | 1.05 (0.93 − 1.18) | 1.12 (1.01 − 1.24) 0.03 |
0.97 (0.77 − 1.21) | 1.09 (0.95 − 1.25) |
Risk ratios and 95% confidence intervals are shown, p-values where significant. Covariate adjustments were made for age, sex, systolic blood pressure, hypertension and lipid lowering medication use, total cholesterol, HDL-C, diabetes, and smoking status. Race-interactions were tested between racial/ethnic groups. Definitions: Lp(a)=lipoprotein(a); diabetes=treated and untreated cases; HDL-C=high density lipoprotein-cholesterol; smoking status=current, former, never
Carotid plaque progression was modeled as a logistical variable (0 or 1); progression was considered to have occurred when a new plaque developed after baseline
No significant race-interactions were observed
Prospective associations of Lp(a) and plaque score following a median period of 9.4 years are shown in Table 5. Greater Lp(a) levels were related to a significantly greater plaque score in Caucasians, irrespective of whether Lp(a) was examined as a continuous or categorical variable (all p≤0.001). No associations were detected in other race/ethnicities. Including race/ethnicity as an interaction term revealed significant differences in the relations of Lp(a) and carotid plaque number between Caucasian and Black participants: Lp(a)≥30 mg/dL (p for interaction=0.05), and Lp(a)≥50 mg/dL (p for interaction=0.01). A race interaction between Caucasians and Chinese American participants was also observed for the Lp(a)≥30 mg/dL cutoff (p for interaction=0.04).
Table 5.
Prospective associations between Lp(a) levels and carotid plaque score* following a median period of 9.4 years in 3,380 Multi-Ethnic Study of Atherosclerosis participants stratified by race/ethnicity.
| Black N=885 |
Caucasian N=1326 |
Chinese American N=435 |
Hispanic N=734 |
|
|---|---|---|---|---|
| per Lp(a) log unit | 0.05 (−0.8 − 0.18) | 0.12 (0.05 − 0.20) 0.001 |
0.04 (−0.12 − 0.20) | 0.07 (−0.04 − 0.17) |
| Lp(a)≥ 30 mg/dL | 0.04 (−0.21 − 0.29) | 0.38 (0.16 − 0.61)† 0.001 |
−0.21 (−0.64 − 0.22)** | 0.20 (−0.10 − 0.51) |
| Lp(a)≥ 50 mg/dL | 0.06 (−0.20 − 0.32) | 0.51 (0.25 − 0.77)† <0.001 |
−0.04 (−0.59 − 0.50) | 0.35 (−0.03 − 0.73) |
Regression coefficients and 95% confidence intervals are shown, p-values where significant or approaching significance. Covariate adjustments were made for age, sex, systolic blood pressure, hypertension and lipid lowering medication use, total cholesterol, HDL-C, diabetes, and smoking status. Race-interactions were tested among racial/ethnic groups
Modeled as an ordinal variable with plaque score values from 0 to 12
Significantly different than Black participants (p for interaction<0.10)
Significantly different than Caucasian participants (p for interaction<0.10)
Definitions: Lp(a)=lipoprotein(a); diabetes=treated and untreated cases; HDL-C=high density lipoprotein-cholesterol; smoking status=current, former, never
DISCUSSION
In a multi-ethnic cohort, Lp(a) was found to be significantly related to all carotid plaque outcomes in Caucasians. Significant race interactions were observed between Black and Caucasian individuals for all outcomes except plaque progression. The absence of a race interaction with plaque progression was likely due to a combination of factors including the selection bias for healthier individuals in the follow-up sample and that the ordinal plaque score variable has a power advantage over the logistical plaque progression outcome—facilitating the identification of an interaction when examining the former.
Null findings were largely observed in the other races/ethnicities, though associations of Lp(a) with prevalent plaque outcomes were statistically borderline in Hispanics. For Hispanic participants, it must be acknowledged that ‘Hispanic’ does not represent a homogeneous race, and genetic/ancestral overlaps with European, African, and Native American populations have been reported (30). Indeed, it has been estimated that Hispanic Americans may share >65% ancestry with European Americans (30). This large degree of overlap may translate to similarities in Lp(a) pathogenicity, which contributed to the borderline results observed here. By contrast, despite the approximate 3-fold higher median Lp(a) levels in Black individuals, no relations between Lp(a) and carotid plaque outcomes were found in this group or in Chinese Americans. While this is the first multi-ethnic cohort study to interrogate Lp(a) and carotid atherosclerotic plaque, other studies have examined Lp(a) and carotid plaque as well as other measures of subclinical coronary atherosclerosis.
Previous studies
To date, few large cohort studies have examined Lp(a) and carotid atherosclerosis, but positive associations have been reported in smaller samples. In studies of patient populations (11, 12), a subanalysis of 152 AIM-HIGH clinical trial subjects (13), and subcohort studies (10, 14), Lp(a) has been shown to increase risk of carotid atherosclerosis outcomes including stenosis, occlusion, and/or plaque burden. Most relevant to the present findings, a cross-sectional analysis in the biracial Atherosclerosis Risk in Communities (ARIC) cohort showed that Lp(a) was related to greater carotid wall thickness in both Black and Caucasian individuals in an age-adjusted model (31). While no race interactions were identified in the ARIC study, methodological differences may have contributed to the inconsistency with the present findings. Among these, the carotid wall thickness outcome used in ARIC is a composite value of extracranial common carotid artery, internal carotid artery, and carotid bifurcation intima media thicknesses and is less precise than the carotid plaque variable used here. In addition, Lp(a) assessment in the ARIC study may have been another source of imprecision as it pre-dated an important methodological advancement in measuring Lp(a). It is now recognized that either controlling for apo(a) isoform size heterogeneity or using an apo(a) isoform size-insensitive assay is crucial for obtaining accurate Lp(a) values. Taken together, differences in the outcome and exposure variables may have contributed to the null race interaction in ARIC and their identification here.
In contrast to studies of carotid atherosclerosis, those of Lp(a) and risk of coronary atherosclerosis as assessed by coronary artery calcification (CAC) have offered equivocal findings. Lp(a) has been shown to be unrelated to CAC in a number of cohort studies (16, 17) including MESA (6) and the Dallas Heart Study (15), but also in smaller studies of Black individuals (18) and postmenopausal women (24). While the above null findings are counter to Lp(a) increasing risk of coronary atherosclerosis in the general population, there is evidence that Lp(a) is related to CAC in subgroups with underlying ASCVD risk factors. Specifically, Lp(a)-related risk of CAC has been reported in European patients with chest pain (23), healthy black individuals with a family history of early-onset CAD (25), European individuals with a family history of ASCVD (26), hypercholesterolemia patients (21, 22), females with diabetes (17) and male smokers (19). Collectively, these studies provide nuanced evidence that Lp(a) is related to coronary atherosclerosis, but appear to dispute the established causal role of Lp(a) in coronary events such as myocardial infarction. And yet, as proposed by Nordestgaard and Langsted (2016), Lp(a) likely promotes coronary events by contributing to thrombosis and stenosis and not early atherogenesis (32), which is supported by the above study findings. Indeed, it must be acknowledged that our results in the carotid vascular bed may be more consistent with a role for Lp(a) promoting stenosis than inducing early atherogenesis. As this remains a controversial area in Lp(a) research, further studies are warranted.
Implications and further research
The race-based differences in Lp(a) and risk of carotid plaque affirm previous observations that Lp(a) may be more pathogenic in Caucasians and potentially Hispanic individuals compared to Black or Chinese Americans for certain CV-related outcomes (6, 7, 9), though not all (8). Given recent advances in Lp(a) lowering therapies such as PCSK9 inhibitors and antisense oligonucleotides, it is possible that these pharmacotherapies may be more efficacious in Caucasians and Hispanics in reducing a broader range of CV outcomes than in other populations.
A biological/biochemical explanation for the observed race-based differences remains uncertain but there are a number of possibilities. Previous research has demonstrated that the KIV type II domain of the Lp(a) component, apo(a), differs by race/ethnicity and influences circulating levels of Lp(a) (33–35), but our results suggest that properties of Lp(a) other than circulating concentrations may contribute to its atherogenecity. Indeed, a number of heterogeneous regions of apo(a) have been identified (36). Of these, the KIV10 domain influences lysine residue binding (37), has been shown to affect vascular cell permeability in tissue culture (38), and defects in KIV10 were found to lower apo(a)/Lp(a) vascular accumulation and reduce atherogenecity in experimental murine models (39, 40). Genetic heterogeneity in KIV10 may therefore be expected to have implications for risk of atherogenesis or stenosis. In addition to KIV10 domain variations, race-based differences in Lp(a) oxidation would also lead to differences in atherogenic burden. However, the one prospective cohort study to examine this phenomenon showed that oxidized Lp(a) levels are greater in Black individuals compared to Caucasians (41), which would refute such a mechanism—though confirmation studies are warranted. Finally, it is well-documented that Lp(a) localizes to atherosclerotic plaques (42–46); however, there remains a paucity of data across different races/ethnicities, and analyzing carotid plaque composition in other races would be appropriate. Taken together, additional research of Lp(a) particle biochemistry and its localization to atherosclerotic plaques may provide insights in to putative race-based differences in Lp(a) pathogenecity observed here.
Strengths and limitations
The present analysis represents the first cohort study showing a modifying influence of race/ethnicity on Lp(a) and risk of carotid atherosclerotic plaque. The study was well-powered in terms of sample sizes and numbers of carotid plaque cases in both cross-sectional and prospective analyses. While the study design does not permit the determination of causality, the mean 9.4-year study period allowed for the assessment of temporality of associations. In terms of limitations, Lp(a) is likely related to ASCVD risk depending upon the vascular bed or event outcome similar to other lipid and non-lipid risk factors (47, 48). Therefore, race-based differences in Lp(a) and risk of carotid plaque should therefore not be generalized to other vascular beds or event outcomes. It must also be recognized that there was a selection bias for healthier individuals in the prospective analyses since these participants completed a follow-up visit a median 9.4 years after baseline. The sample showed a lower rate of incident CVD, which may have contributed to the weaker findings for the plaque progression outcome. Finally, statistical adjustments were made for typical ASCVD risk factors, but the possibility of confounding cannot be excluded.
Conclusions
Race was found to be a modifying variable in Lp(a)-related risk of carotid atherosclerotic plaque, and Lp(a) levels may have greater influence on plaque burden in Caucasians than in Black individuals. Borderline results in Hispanics suggest that elevated Lp(a) may increase risk of carotid plaque, but follow-up studies are needed. Collectively, these results have implications for the role of Lp(a) in influencing ASCVD risk across different races, and additional studies are warranted to continue exploring differences in the molecular biochemistry and pathogenecity of Lp(a) particles among races/ethnicities.
Supplementary Material
{kind=link}
Highlights.
In Multi-Ethnic Study of Atherosclerosis cohort participants, Lp(a) was related to greater risk of carotid plaque and its progression in Caucasians
In Hispanics participants, Lp(a)-associated risk of carotid plaque was statistically borderline and equivocal
Significant race interactions were observed whereby Lp(a)-associated risk of plaque outcomes was significantly different in Caucasians than from Black individuals
ACKNOWLEDGEMENTS
The authors thank the other investigators, the staff, and the participants of the MESA study for their valuable contributions. A full list of participating MESA investigators and institutions can be found at http://www.mesa-nhlbi.org. The authors also thank Denka Seiken (Tokyo, Japan) for providing Lp(a) assay reagents at no cost.
SOURCES OF FUNDING
This research was supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 from the National Heart, Lung, and Blood Institute, and by grants UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 from NCATS.
NONSTANDARD ABBREVIATIONS AND ACRONYMS
- Lp(a)
Lipoprotein(a)
- MESA
Multi-Ethnic Study of Atherosclerosis
- ASCVD
Atherosclerotic cardiovascular disease
- ARIC
Atherosclerosis Risk in Communities
- CAC
Coronary artery calcification
Footnotes
DISCLOSURES
Dr. Karger reports grants and non-financial support from Siemens Healthcare Diagnostics, outside of the submitted work.
References
- 1).Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, Hoes AW, Jennings CS, Landmesser U, Pedersen TR, Reiner Z, Riccardi G, Taskinen MR, Tokgozoglu L, Verschuren WMM, Vlachopoulos C, Wood DA, Zamorano JL, Cooney MT. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J 2016;37:2999–3058. [DOI] [PubMed] [Google Scholar]
- 2).Greenland P, Alpert JS, Beller GA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2010;56:e50–103. [DOI] [PubMed] [Google Scholar]
- 3).Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J 2010;31:2844–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4).Grundy SM, Stone NJ, Bailey AL, et al. 2018. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018 pii: S0735–1097(18)39034-X.
- 5).Wiegman A, Gidding SS, Watts GF, et al. Familial hypercholesterolaemia in children and adolescents: gaining decades of life by optimizing detection and treatment. Eur Heart J 2015;36:2425–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6).Cao J, Steffen BT, Budoff M, Post WS, Thanassoulis G, Kestenbaum B, McConnell JP, Warnick R, Guan W, Tsai MY. Lipoprotein(a) Levels Are Associated With Subclinical Calcific Aortic Valve Disease in White and Black Individuals: The Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 2016;36:1003–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7).Steffen BT, Duprez D, Bertoni AG, Guan W, Tsai MY. Lipoprotein(a)-related risk of incident heart failure is evident in Caucasians but not in other racial/ethnic groups: The Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 2018;38:2498–2504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8).Guan W, Cao J, Steffen BT, Post WS, Stein JH, Tattersall MC, Kaufman JD, McConnell JP, Hoefner DM, Warnick R, Tsai MY. Race is a key variable in assigning lipoprotein(a) cutoff values for coronary heart disease risk assessment: the Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 2015;35:996–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9).Forbang NI, Criqui MH, Allison MA, Ix JH, Steffen BT, Cushman M, Tsai MY. Sex and ethnic differences in the associations between lipoprotein(a) and peripheral arterial disease in the Multi-Ethnic Study of Atherosclerosis. J Vasc Surg 2016;63:453–8. [DOI] [PubMed] [Google Scholar]
- 10).Cambillau M, Simon A, Amar J, Giral P, Atger V, Segond P, Levenson J, Merli I, Megnien JL, Plainfosse MC, et al. Serum Lp(a) as a discriminant marker of early atherosclerotic plaque at three extracoronary sites in hypercholesterolemic men. The PCVMETRA Group. Arterioscler Thromb 1992;12:1346–52. [DOI] [PubMed] [Google Scholar]
- 11).Klein JH, Hegele RA, Hackam DG, Koschinsky ML, Huff MW, Spence JD. Lipoprotein(a) is associated differentially with carotid stenosis, occlusion, and total plaque area. Arterioscler Thromb Vasc Biol 2008:1851–6. [DOI] [PubMed]
- 12).Iwamoto T, Feng Y, Shinozaki K, Koyama S, Oyama T, Takasaki M. Clinical significance of lipoprotein(a) in carotid plaque types and ischemic stroke in the elderly. Geriatrics & Gerontology International 2003; 3: 93–100. [Google Scholar]
- 13).Hippe DS, Phan BAP, Sun J, Isquith DA, O’Brien KD, Crouse JR, Anderson T, Huston J, Marcovina SM, Hatsukami TS, Yuan C, Zhao XQ. Lp(a) (Lipoprotein(a)) Levels Predict Progression of Carotid Atherosclerosis in Subjects With Atherosclerotic Cardiovascular Disease on Intensive Lipid Therapy: An Analysis of the AIM-HIGH (Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides: Impact on Global Health Outcomes) Carotid Magnetic Resonance Imaging Substudy-Brief Report. Arterioscler Thromb Vasc Biol 2018;38:673–678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14).Willeit J, Kiechl S, Santer P, Oberhollenzer F, Egger G, Jarosch E, Mair A. Lipoprotein(a) and asymptomatic carotid artery disease. Evidence of a prominent role in the evolution of advanced carotid plaques: the Bruneck Study. Stroke 1995;26:1582–7. [DOI] [PubMed] [Google Scholar]
- 15).Guerra R, Yu Z, Marcovina S, Peshock R, Cohen JC, Hobbs HH. Lipoprotein(a) and apolipoprotein(a) isoforms: no association with coronary artery calcification in the Dallas Heart Study. Circulation 2005;111:1471–9. [DOI] [PubMed] [Google Scholar]
- 16).Kullo IJ, Bailey KR, Bielak LF, Sheedy PF 2nd, Klee GG, Kardia SL, Peyser PA, Boerwinkle E, Turner ST. Lack of association between lipoprotein(a) and coronary artery calcification in the Genetic Epidemiology Network of Arteriopathy (GENOA) study. Mayo Clin Proc 2004;79:1258–63. [DOI] [PubMed] [Google Scholar]
- 17).Qasim AN, Martin SS, Mehta NN, Wolfe ML, Park J, Schwartz S, Schutta M, Iqbal N, Reilly MP. Lipoprotein(a) is strongly associated with coronary artery calcification in type-2 diabetic women. Int J Cardiol 2011;150:17–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18).Moliterno DJ, Jokinen EV, Miserez AR, Lange RA, Willard JE, Boerwinkle E, Hillis LD, Hobbs HH. No association between plasma lipoprotein(a) concentrations and the presence or absence of coronary atherosclerosis in African-Americans. Arterioscler Thromb Vasc Biol 1995;15:850–5. [DOI] [PubMed] [Google Scholar]
- 19).Cassidy AE, Bielak LF, Kullo IJ, Klee GG, Turner ST, Sheedy PF 2nd, Peyser PA. Sex-specific association of lipoprotein(a) with presence and quantity of coronary artery calcification in an asymptomatic population. Med Sci Monit 2004;10:CR493–503. [PubMed]
- 20).Jiang Y, Guo K, Chen M, Bao J, Shen C, Li Y. Serum lipoprotein(a) positively correlates with coronary artery calcification in low-risk chinese han patients: a study from a single center. PLoS One 2013;8:e71673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21).Sun D, Zhou BY, Zhao X, Li S, Zhu CG, Guo YL, Gao Y, Wu NQ, Liu G, Dong Q, Li JJ. Lipoprotein(a) level associates with coronary artery disease rather than carotid lesions in patients with familial hypercholesterolemia. J Clin Lab Anal 2018;32:e22442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22).Alonso R, Mata P, Muñiz O, Fuentes-Jimenez F, Díaz JL, Zambón D, Tomás M, Martin C, Moyon T, Croyal M, Thedrez A, Lambert G. PCSK9 and lipoprotein (a) levels are two predictors of coronary artery calcification in asymptomatic patients with familial hypercholesterolemia. Atherosclerosis 2016;254:249–253. [DOI] [PubMed] [Google Scholar]
- 23).Greif M, Arnoldt T, von Ziegler F, Ruemmler J, Becker C, Wakili R, D’Anastasi M, Schenzle J, Leber AW, Becker A. Lipoprotein (a) is independently correlated with coronary artery calcification. Eur J Intern Med 2013;24:75–9. [DOI] [PubMed] [Google Scholar]
- 24).Nishino M, Malloy MJ, Naya-Vigne J, Russell J, Kane JP, Redberg RF. Lack of association of lipoprotein(a) levels with coronary calcium deposits in asymptomatic postmenopausal women. J Am Coll Cardiol 2000;35:314–20. [DOI] [PubMed] [Google Scholar]
- 25).Kral BG, Kalyani RR, Yanek LR, Vaidya D, Fishman EK, Becker DM, Becker LC. Relation of Plasma Lipoprotein(a) to Subclinical Coronary Plaque Volumes, Three-Vessel and Left Main Coronary Disease, and Severe Coronary Stenoses in Apparently Healthy African-Americans With a Family History of Early-Onset Coronary Artery Disease. Am J Cardiol 2016;118:656–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26).Verweij SL, de Ronde MWJ, Verbeek R, Boekholdt SM, Planken RN, Stroes ESG, Pinto-Sietsma SJ. Elevated lipoprotein(a) levels are associated with coronary artery calcium scores in asymptomatic individuals with a family history of premature atherosclerotic cardiovascular disease. J Clin Lipidol 2018;12:597–603.e1. [DOI] [PubMed] [Google Scholar]
- 27).Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: Objectives and design. Am J Epidemiol 2002;156:871–881. [DOI] [PubMed] [Google Scholar]
- 28).Tsai MY, Johnson C, Kao WH, Sharrett AR, Arends VL, Kronmal R, Jenny NS, Jacobs DR, Arnett D, O’Leary D, Post W. Cholesteryl ester transfer protein genetic polymorphisms, hdl cholesterol, and subclinical cardiovascular disease in the multi-ethnic study of atherosclerosis. Atherosclerosis 2008;200:359–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29).Tattersall MC, Gassett A, Korcarz CE, Gepner AD, Kaufman JD, Liu KJ, Astor BC, Sheppard L, Kronmal RA, Stein JH. Predictors of carotid thickness and plaque progression during a decade: the Multi-Ethnic Study of Atherosclerosis. Stroke 2014;45:3257–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30).Bryc K, Durand EY, Macpherson JM, Reich D, Mountain JL. The genetic ancestry of African Americans, Latinos, and European Americans across the United States. Am J Hum Genet 2015;96:37–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31).Schreiner PJ, Heiss G, Tyroler HA, Morrisett JD, Davis CE, Smith R. Race and gender differences in the association of Lp(a) with carotid artery wall thickness. The Atherosclerosis Risk in Communities (ARIC) Study. Arterioscler Thromb Vasc Biol 1996;16:471–8. [DOI] [PubMed] [Google Scholar]
- 32).Nordestgaard BG, Langsted A. Lipoprotein (a) as a cause of cardiovascular disease: insights from epidemiology, genetics, and biology. J Lipid Res 2016;57:1953–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33).Mack S, Coassin S, Rueedi R, et al. A genome-wide association meta-analysis on lipoprotein (a) concentrations adjusted for apolipoprotein (a) isoforms. J Lipid Res 2017;58:1834–1844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34).Marcovina SM, Albers JJ, Wijsman E, Zhang Z, Chapman NH, Kennedy H. Differences in Lp[a] concentrations and apo[a] polymorphs between black and white Americans. J Lipid Res 1996;37:2569–85. [PubMed] [Google Scholar]
- 35).Thanassoulis G, Campbell CY, Owens DS, et al. Genetic associations with valvular calcification and aortic stenosis. N Engl J Med 2013;368:503–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36).Scanu AM. Lp(a) lipoprotein--coping with heterogeneity. N Engl J Med 2003;349:2089–90. [DOI] [PubMed] [Google Scholar]
- 37).Armstrong VW, Harrach B, Robeneck H, et al. Heterogeneity of human lipoprotein Lp(a): cytochemical and Biochemical studies on the interaction of two Lp(a) species with the LDL receptor. J Lipid Res 1990;31:429–441. [PubMed] [Google Scholar]
- 38).Cho T, Jung Y, Koschinsky ML. Apolipoprotein(a), through its strong lysine-binding site in KIV(10’), mediates increased endothelial cell contraction and permeability via a Rho/Rho kinase/MYPT1-dependent pathway. J Biol Chem 2008;283:30503–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39).Hughes SD, Lou XJ, Ighani S, Verstuyft J, Grainger DJ, Lawn RM, Rubin EM. Lipoprotein(a) vascular accumulation in mice. In vivo analysis of the role of lysine binding sites using recombinant adenovirus. J Clin Invest 1997;100:1493–500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40).Boonmark NW, Lou XJ, Yang ZJ, Schwartz K, Zhang JL, Rubin EM, Lawn RM. Modification of apolipoprotein(a) lysine binding site reduces atherosclerosis in transgenic mice. J Clin Invest 1997;100:558–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41).Tsimikas S, Clopton P, Brilakis ES, Marcovina SM, Khera A, Miller ER, de Lemos JA, Witztum JL. Relationship of oxidized phospholipids on apolipoprotein B-100 particles to race/ethnicity, apolipoprotein(a) isoform size, and cardiovascular risk factors: results from the Dallas Heart Study. Circulation 2009;119:1711–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42).Rath M, Niendorf A, Reblin T, Dietel M, Krebber HJ, Beisiegel U. Detection and quantification of lipoprotein(a) in the arterial wall of 107 coronary bypass patients. Arteriosclerosis 1989;9:579–92. [DOI] [PubMed] [Google Scholar]
- 43).Niendorf A, Rath M, Wolf K, Peters S, Arps H, Beisiegel U, Dietel M. Morphological detection and quantification of lipoprotein(a) deposition in atheromatous lesions of human aorta and coronary arteries. Virchows Arch A Pathol Anat Histopathol 1990;417:105–11. [DOI] [PubMed] [Google Scholar]
- 44).Jürgens G, Chen Q, Esterbauer H, Mair S, Ledinski G, Dinges HP. Immunostaining of human autopsy aortas with antibodies to modified apolipoprotein B and apoprotein(a). Arterioscler Thromb 1993;13:1689–99. [DOI] [PubMed] [Google Scholar]
- 45).Pepin JM, O’Neil JA, Hoff HF. Quantification of apo[a] and apoB in human atherosclerotic lesions. J Lipid Res 1991;32:317–27. [PubMed] [Google Scholar]
- 46).Reblin T, Meyer N, Labeur C, Henne-Bruns D, Beisiegel U. Extraction of lipoprotein(a), apo B, and apo E from fresh human arterial wall and atherosclerotic plaques. Atherosclerosis 1995;113:179–88. [DOI] [PubMed] [Google Scholar]
- 47).Stoekenbroek RM, Boekholdt SM, Luben R, Hovingh GK, Zwinderman AH, Wareham NJ, Khaw KT, Peters RJ. Heterogeneous impact of classic atherosclerotic risk factors on different arterial territories: the EPIC-Norfolk prospective population study. Eur Heart J 2016;37:880–9. [DOI] [PubMed] [Google Scholar]
- 48).Tunstall-Pedoe H, Peters SAE, Woodward M, Struthers AD, Belch JJF. Twenty-Year Predictors of Peripheral Arterial Disease Compared With Coronary Heart Disease in the Scottish Heart Health Extended Cohort (SHHEC). J Am Heart Assoc 2017;6(9). pii: e005967. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.