

Abstract
Seventy-eight postinstitutionalized (PI) children adopted at ages 17–36 months were assessed 2, 8, 16, and 24 months postadoption on measures of cortisol and parenting quality, and compared to same-aged children adopted from foster care (FC, n = 45) and nonadopted children (NA, n = 45). In kindergarten (Mage = 6.0 years), teachers, parents, and trained observers completed measures of peer relationships and attention deficit hyperactivity disorder (ADHD) symptoms. PI children had more peer problems and ADHD symptoms according to teachers and observers than NA children with FC children in between, whereas both PI and FC children were at significantly greater risk of hypocortisolism (i.e., blunted cortisol diurnal rhythm and reactivity). Hypocortisolism and ADHD symptoms mediated the association between preadoption adversity and peer difficulties. Higher postadoption parenting quality was protective.
Children whose psychological and social needs are neglected early in life are at risk for maladaptation in various domains of development. In orphanage settings, adversity often takes the form of psychosocial neglect, with multiple staff members providing minimal care in a setting primarily devoid of cognitive or social stimulation (van IJzendoorn et al., 2011). Adoption typically results in a shift to responsive care in an enriched environment and, consequently, rapid recovery of physical growth, resolution of medical problems, and improvements in cognitive development (Ames, 1997; Johnson & Gunnar, 2011). Yet, although likely markedly improved from preadoption functioning, many postinstitutionalized (PI) children display difficulties in social and emotional domains that persist long after adoption (Sonuga-Barke & Kreppner, 2012). It has been suggested that there is a sensitive period in the first 2 years of life for the full development of systems underlying socioemotional competence (e.g., Vanderwert, Marshall, Nelson, Zeanah, & Fox, 2010). Orphanage-reared children provide a unique opportunity to examine the effects of a circumscribed period of psychosocial neglect. However, children adopted from orphanages also share aspects of prenatal and postnatal adversity with internationally adopted children who were placed in foster care (FC). Many studies have shown that even though they tend to be adopted at a younger age than orphanage-reared children, they often share many of the same problems albeit to a lesser degree.
Beginning in early childhood, positive peer interactions and later the establishment of peer friendships become critical developmental tasks (Hartup & Moore, 1990), which predict later psychological and behavioral adjustment (e.g., Reijntjes, Kamphuis, Prinzie, & Telch, 2010). PI youth, especially those who have experienced longer durations of adverse care, are reported to experience more social problems (e.g., Gunnar, van Dulmen, & International Adoption Project Team, 2007; Hawk & McCall, 2011; Pitula et al., 2014) including difficulties forming and maintaining friends (Almas et al., 2015; Hodges & Tizard, 1989). However, very little is known about the peer relationships of PI adoptees in early childhood, particularly using observational instruments rather than parental report. Moreover, our understanding of processes that may predict the development of problematic peer relationships among this at-risk group is limited. Chronic early life stress has been associated with alterations in the diurnal rhythm of cortisol (e.g., Gunnar & Quevedo, 2007; Koss, Hostinar, Donzella, & Gunnar, 2014), and in a recent study by our group, blunted (i.e., decreased) cortisol production was associated with increased attention problems and behavior regulatory problems among internationally adopted children (Koss, Mliner, Donzella, & Gunnar, 2016). The present study was a follow-up in kindergarten of the children previously studied by Koss et al. (2014), with a new focus on peer relationship functioning using a multimethod, multi-informant design. The association between early patterns of cortisol production and later social functioning was examined to further our understanding of biological mechanisms by which early adverse experiences may be transduced into social problems. We also explored whether the expected association of earlier hypothalamic–pituitary–adrenal (HPA) axis functioning with later peer functioning may operate through its effects on problems with attention and behavior regulation. Postadoption parenting quality was considered as a buffer against the negative impact of early deprivation on social functioning.
Peer Relationship Functioning in PI Youth
To date, the majority of research on social functioning in PI youth has focused on older participants, providing evidence for elevated peer problems in middle childhood and adolescence (e.g., Pitula et al., 2014; Raaska et al., 2012). When several age groups have been sampled in the same study, results suggest that social difficulties increase with age within the PI group (Hawk & McCall, 2011), and longitudinal findings have demonstrated increases in peer problems from 6 to 11 years of age (Sonuga-Barke, Schlotz, & Kreppner, 2010). Two distinct possibilities are that the difficulties reported in older PI youth represent a continuation of difficulties from early childhood or that they become evident later in childhood as the social landscape becomes increasingly complex. Yet, our understanding of younger PI children’s peer functioning is limited. Findings specific to younger PI children are mixed, with one research group showing elevated social problems (median age 2.5 years, Fisher, Ames, Chisholm, & Savoie, 1997; modal age 4.5 years, Ames, 1997) and others reporting equal or better peer functioning among previously institutionalized Chinese girls (preschool, Tan & Camras, 2011) and no evidence of more clinically significant disorders of peer functioning among children adopted from Romania (6 years old, Rutter, Kreppner, & O’Connor, 2001). Further research is needed to clarify the social functioning of very young PI children.
Another limitation of the extant literature is a tendency to rely solely on reports by parents or teachers (e.g., Fisher et al., 1997; Groza, 1999; Gunnar et al., 2007; Hawk & McCall, 2011). When more than one informant has been used, different informants’ ratings have often been combined into a single scale for analysis (e.g., Rutter et al., 2001), precluding the possibility of differentiating between different informants’ contributions. Yet, it is quite possible that different informants perceive PI children’s peer relationships differently. Parents have the advantage of seeing their children beyond the classroom setting, such as with friends in the neighborhood. Conversely, whereas parents may be limited in their contact with developmentally typical peers, teachers benefit from the broader perspective of seeing multiple children interact with one another every day. At the same time, teachers may be skewed by their role in maintaining classroom order; in normative populations, teachers often report that children who show noncompliant, inattentive, and disruptive behaviors are more likely to be rejected (Coie, Dodge, & Kupersmidt, 1990). It is also possible that both parents and teachers report on specific peer relationship behaviors based on their more general impression of the child’s social functioning rather than objective observations of specific interactions. Importantly, unbiased, trained observers, such as research staff, are unaware of status and unbiased by previous contacts with the children. As a result, they are well positioned to provide objective information about experiences with and behaviors toward peers (Pepler & Craig, 1998). Still, trained observers are usually reliant on short observations that may not represent the child’s true functioning over longer periods of time. Observers have rarely been utilized as informants in research on PI youths’ peer relationships (for an exception, see Almas et al., 2015). Given that parents, teachers, and observers are expected to contribute unique and additive variance to our understanding of peer relationships, the present study considered information from all three informants.
Biological Underpinnings: Hypocortisolism
The HPA axis and its end product cortisol constitute the primary stress response system and have wide-ranging effects on the body and brain (see Sapolsky, Romero, & Munck, 2000). In humans, the HPA axis produces cortisol. It follows a diurnal rhythm but is elevated in response to real or imagined threat. The typical diurnal rhythm develops over infancy and early childhood and consists of higher levels of cortisol soon after waking followed by a steep drop throughout the day, reaching the lowest levels after falling asleep at night (Gunnar & Quevedo, 2007). In response to stressors, negative feedback mechanisms allow for a relatively rapid return to basal levels. Thus, four measurable components of the HPA axis are (a) morning cortisol values, (b) diurnal slope (i.e., change across the day), (c) baseline cortisol before a stressor, and (d) reactivity slope (i.e., change in response to a stimulus/stressor).
Although rodent studies of early adverse care typically show elevated HPA axis reactivity (e.g., Meaney & Szyf, 2005), in humans, hypocortisolism has often been noted in association with chronic stress (Fries, Hesse, Hellhammer, & Hellhammer, 2005). In the psychosocial stress literature, hypocortisolism is defined as a blunted or absent response to stressors and a low and flat diurnal cortisol pattern (Fries et al., 2005; Gunnar & Vazquez, 2001). Chronic exposure to early life stressors in humans has been found to predict lower basal cortisol, including lower morning levels of cortisol and a flatter diurnal slope (Bernard, Zwerling, & Dozier, 2015; Martin, Kim, Bruce, & Fisher, 2014). In reports using the same sample of PI children as in the present study (Koss et al., 2014, 2016), early institutional care was shown to predict a blunted diurnal rhythm and decreased reactivity to laboratory stressors during the first 2 years after adoption. Notably, in children randomly assigned to care as usual or fostering out of orphanages, hypocortisolism at age 8 years was also reported for those who were adopted after 2 years (McLaughlin et al., 2015). However, in Koss et al. (2014, 2016) analyses, children adopted internationally before 12 months from FC settings also exhibited similar hypocortisolism, thus it is likely that neither institutional care nor late age at adoption are the only factors influencing the establishment of a hypocortisolism HPA axis profile.
Hypocortisolism is associated with a number of behavioral problems (Bernard et al., 2015; Martin et al., 2014). Notably, Koss et al. (2016) found that hypocortisolism mediated the association between psychosocial neglect and attention and externalizing problems. The association between blunted cortisol patterns and mental health outcomes appears to be more common to problems in the externalizing domain, with excessive cortisol production (i.e., hypercortisolism) instead predicting internalizing symptoms, negative emotionality and shyness (Gunnar, Sebanc, Tout, Donzella, & van Dulmen, 2003; Kopala-Sibley et al., 2017). Thus, whether elevated or blunted, atypical patterns of cortisol regulation seem to contribute to increased vulnerability to mental health problems. Importantly, cortisol patterns may constitute a biological mechanism by which early stressful experiences are transduced into elevated risk for psychosocial difficulties.
However, the role of cortisol in explaining associations between early psychosocial neglect and later peer relationships has not been examined, and the direct link between hypocortisolism and social functioning has received minimal attention (however, see Gunnar et al., 2003). Understanding the direct associations between cortisol dysregulation and peer relationships could shed light not only on the function of the HPA axis more generally, but also on potential pathways to target in interventions seeking to improve physiological and behavioral regulation in children who have experienced adversity. We hypothesized that a history of early institutional care would predispose children to heightened peer problems through the biological mechanism of blunted cortisol activity.
Attention Deficit Hyperactivity Disorder Symptoms
The association of cortisol with peer difficulties may operate via hypocortisolism’s association with attention deficit hyperactivity disorder (ADHD) symptoms, which include deficits in inhibitory control and symptoms of inattention, hyperactivity, and impulsivity. ADHD has been associated in a bidirectional manner with peer problems beginning in early childhood (Stenseng, Belsky, Skalicka, & Wichstrøm, 2015). Because elevated ADHD symptoms are one of the most reliable findings in this literature and were previously reported as predicted by hypocortisolism in this sample (Koss et al., 2014), we examined whether the association of earlier hypocortisolism with later peer problems might be explained through associations with ADHD symptoms. We hypothesized that ADHD symptoms would mediate the relationship between hypocortisolism and peer problems in kindergarten.
Parenting Quality
The quality of parenting that PI children receive in their adoptive homes may help them recover from the negative institutional effects on biological and social systems. Previous research in normative samples has shown that high-quality parenting, characterized by positive regard, emotional support, and effective limit setting, plays an important role in predicting children’s social adjustment (e.g., Landry, Smith, & Swank, 2006). In addition, there is evidence that parenting quality moderates the association between risk due to fearful temperament (Shin & Kim, 2008) or peer behavior (e.g., aggression, Karreman, de Haas, van Tuijl, van Aken, & Deković, 2010) and social maladjustment. Adoptive parents may play an especially important role in reversing some of the negative consequences of preadoptive adverse care experiences. Indeed, there is some evidence that the quality of adoptive parenting for internationally adopted children is associated with better cognitive and social development (Ames, 1997; Stams, Juffer, & van IJzendoorn, 2002). Aiming to improve the physiological and behavioral regulatory capacities of children exposed to early adverse caregiving, several research teams have implemented parenting interventions with the parents of maltreated and PI children, with an emphasis on increasing parental responsiveness, sensitivity, and nurturance (see Dozier, Zeanah, Wallin, & Shauffer, 2012 for a review). So far, results suggest successful outcomes in cognitive, behavioral, social, and physiological domains (Almas et al., 2015; Dozier et al., 2006). Thus, the present study explored parenting quality as a potential moderator of the link between preadoptive care and social outcomes.
The Present Study
In order to examine how similar or different PI children were from children reared from birth in the United States, PI adoptees were compared with children who were raised in their families of origin (nonadopted [NA]), which were demographically similar to the families of adopted PI children. Moreover, in studies of children adopted from orphanages it is also important to have an adoption comparison group. Notably, in the English and Romanian Adoption Study, Rutter et al. (2007) chose a domestic (i.e., United Kingdom) adoption group, most of whom were adopted at birth, as the comparison for children adopted from Romania. Equating for age at adoption, Groza and Ryan (2002) chose domestically adopted children with special needs as a comparison for Romanian adopted children. Likewise, van den Dries, Juffer, van IJzendoorn, and Bakermans-Kranenburg (2010) were able to compare a group of girls adopted into the Netherlands from FC in China with a group adopted from Chinese orphanages. Our adoption comparison group, consisting of children adopted into the United States from FC overseas, was broadly representative of the countries and ages at adoption typical for families in the United States who adopt internationally from FC. Because countries using FC for wards of the state tend to release children for adoption earlier than those using institutional care, FC children were younger at adoption than PI children. Both NA and FC children were roughly comparable to PI children on age at testing and family socioeconomic status.
In kindergarten, PI youth were hypothesized to experience more problems with peer functioning than both NA and FC children. FC children had less preadoption adversity and were adopted earlier, so we expected them to fall between NA and PI children. Moreover, it was expected that this relation would be attenuated among children who experienced higher quality parenting. Hypocortisolism and ADHD symptoms were hypothesized to statistically mediate the association between early deprivation and social outcomes (see Figure 1 for a conceptual model of this multiple mediation analysis). If supported, this would suggest that chronic stress and its impacts on stress-mediating and behavior regulatory systems may contribute to or provide a useful index of the mechanisms through which stressful early experiences “get under the skin” to influence later social development.
Figure 1.
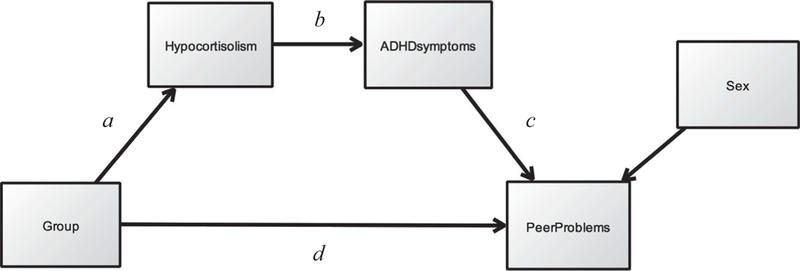
Conceptual model for multiple mediation analysis. ADHD = attention deficit hyperactivity disorder.
Method
Participants
Participants were 168 children taking part in a longitudinal study investigating the transition to family care following international adoption. Only the children who were not homeschooled (95%; homeschooled n = 4 PI, 2 FC, 3 NA) were considered for the kindergarten follow-up. The PI group (60% female) comprised children adopted from an institution (orphanage) between the ages of 17.3 and 36.1 months. Most (63.2%) had spent 80% or more of their preadoption lives in institutional care (range = 14%–100%; two missing). Almost all (98.7%) had not spent any time in FC. Thirty-two percent of PI children were of Southeast Asian or Pacific Islander origin; 29.5% were from Africa; 25.6% from Russia, Europe, India, or Nepal; and 12.8% from Latin America or the Caribbean. Most adoptive households (76.0%) reported an annual income > $75,000 (three missing). FC children (35% female) were adopted between 6.7 and 2.7 months, and had spent no more than 4 months in a hospital or other institutional setting (median = .76 months). Most participants (82.2%) had spent more than 80% of their preadoption lives in FC. SE Asian origin was reported for 73.3% and Latin American origin for 26.7%. Most adoptive parents (86.4%) reported an annual income > $75,000 (one missing). The NA comparison group (NA; 47% female) consisted of children born and raised in their biological families in the Midwest. Their parents were of roughly the same income as those who adopted internationally (i.e., 77.3% with household annual income > $75,000, missing = 1). Additional demographic information is shown in Table 1.
Table 1.
Participant Demographic Information
| Variable | PI | FC | NA |
|---|---|---|---|
| Sample size, n (% female) | 78 (60) | 45 (35) | 45 (47) |
| Race (%) | |||
| Asian | 42.3 | 73.3 | 4.4 |
| African/Black | 33.3 | — | — |
| Caucasian | 12.8 | — | 86.7 |
| Latin American/Native American | 5.1 | 22.2 | — |
| Mixed race | 2.6 | — | 8.9 |
| Other/unknown | 3.8 | 4.4 | — |
| Ethnicity—Hispanic/Latino (%) | 7.7 | 26.7 | 4.5 |
| Age at adoption (months), M (SD) | 24.7 (5.2) | 9.7 (1.4) | — |
| Time in institution (months), M (SD) | 18.3 (7.8) | 0.8 (0.9) | — |
| % Preadoptive life in institution, M (SD) | 76.9 (28.1) | 8.9 (10.6) | — |
| Age at Session 1 (months), M (SD) | 26.0 (4.7) | 32.8 (4.8) | 27.6 (5.8) |
| Age in kindergarten (years), M (SD) | 5.9 (0.3) | 6.0 (0.3) | 6.0 (0.3) |
Note. PI = postinstitutionalized; FC = foster care; NA = nonadopted.
Children originally contacted for the longitudinal study were excluded based on prenatal alcohol exposure (9 PI, 2 FC) or if they had a diagnosis of autism spectrum disorder (1 NA), or a congenital, cognitive, or endocrine disorder (2 PI, 1 FC). Two NA children who experienced significant early life stress (i.e., parental maltreatment, medical trauma) were also excluded. Ns reported above were after exclusion.
Procedures
Because they were to be seen within a month or so of arrival in this country, PI children were recruited from an adoption medical clinic where families often made their appointments before traveling to get their children and through the major adoption agencies in our Midwestern state that also facilitated contact with families prior to adoption. Of those contacted for this longitudinal study, 70% agreed to participate. FC children, who were not tested immediately after adoption, were recruited through the International Adoption Project Registry maintained by our research group. Letters are mailed every several months to all families who have recently adopted internationally through the major agencies. Interested parents join the registry and provide information about the child’s age at adoption and type of preadoption living situation. Approximately 50% of those contacted for the registry join the registry. Of those contacted for the longitudinal study, 80% of FC parents agreed to participate. NA children were recruited from a participant pool maintained by our department through letters sent to all families of live births in the metropolitan area and through website and other advertising. A very small percentage of those sent letters join the registry. However, of those on the registry who were contacted for the longitudinal study, 100% agreed to participate.
For the present analyses, all children participated in four laboratory sessions and a kindergarten assessment. The first laboratory session (i.e., Session 1) occurred approximately 2 months after adoption for PI children (M = 1.7, SD = 0.7, range = 0.33–3.25), and Sessions 2–4 took place approximately 8, 16, and 24 months after adoption. Children in the comparison groups were roughly matched in age to the PI children at the first assessment and then were tested at equivalent intervals. Overall, children were aged 18.6–37.4 months (M = 28.6, SD = 5.9) at the first session. Note that 21 of the PI participants in the present sample were recruited after the targeted time of the first laboratory session and so are missing data from that time point. During the kindergarten assessment, children (Mage = 6.0 years, SD = 0.3) were visited in their kindergarten classrooms between October and June, and parents and teachers received questionnaire packets in the mail or completed questionnaires online. Data collection for the present analyses began on August 14, 2008 and concluded on March 6, 2015.
Measures
Peer Functioning
Peer Relations Observation Inventory–Revised.
Behaviors were scored live with a modification of the National Institute of Child Health and Human Development Observational Rating Scales of Caregiving Environment (Gunnar, Kryzer, van Ryzin, & Phillips, 2010). Originally designed for preschool use, the measure needed only slight modification for use in the kindergarten classroom (note, the variables included in the present study were not impacted by these modifications). This instrument examines the frequency of specific kinds of behavior displayed by or directed toward the target child during 6 blocks of 20 observational intervals (30 s per interval), during structured classroom instruction (60%–100% of observed intervals) and unstructured free play or recess time (0%–40% of observed intervals). Observers, blind to group status, coded (a) the child’s mean level of positive or neutral social integration (on a 1–3 scale, where 1 = alone, 2 = low integration in a social interaction, and 3 = high integration during each interval), (b) the proportion of intervals where the child directed negative social actions to another child or group of children (e.g., relational, physical, or verbal aggression), and (c) the proportion of intervals where the child received negative social actions from a single child or group. Coders were initially trained to reliability on the Peer Relations Observation Inventory–Revised (PROI–R) against the third author in the university’s laboratory preschool. Periodic reliability checks (n = 47) of coding pairs were conducted in the laboratory preschool. All variables showed good to excellent interrater agreement (intra-class correlation coefficient = .66–.92, median = .81). Given the possibility that behaviors may vary over structured and unstructured times, the proportion of structured intervals was used as a covariate in analyses.
Observer rating scales.
After completing the PROI–R, observers rated participants’ social behaviors on a 5-point Likert scale (never/not true to frequently/very true) using an adapted version of the Peers and Social Skills Questionnaire (OSLC, 1982– 2007, e.g., Kerr, Capaldi, Pears, & Owen, 2009). Subscales used in the present analyses assess (a) social status/acceptance, (b) social skills, (c) victimization, and (d) aggression. These subscales demonstrated acceptable internal consistency in the present sample (Cronbach’s α = .60–.85). Of the full sample of 168 children, 147 were assessed in kindergarten (missing: 13 due to parent decline, 7 were not yet in kindergarten, and 1 due to early attrition from the study). Of these, eight are missing observer data due to the school being too far to permit a visit and two because the school declined to participate.
Teacher and parent Health and Behavior Questionnaire.
Parents and kindergarten teachers com pleted the MacArthur Health and Behavior Questionnaire (HBQ; Essex et al., 2002), version 1.0 for children aged 4–8 years. Subscales were used assessing (a) peer acceptance/rejection, (b) overt victimization, (c) prosocial behavior, (d) social withdrawal, (e) overt aggression, and (f) relational aggression. Items were rated on a 4-point Likert scale (not at all like to very much like) for subscales a–b and on a 3-point scale (rarely applies to certainly applies or never or not true to often or very true) for subscales c–f. In the present sample, parent subscales showed acceptable internal consistency (Cronbach’s α = .65–.89). Most teacher subscales demonstrated acceptable internal consistency (Cronbach’s α = .76–.92), aside from victimization (Cronbach’s α = .51), so this variable was excluded from further analysis. Two schools declined to participate, and one teacher and two parents failed to return questionnaires, resulting in HBQ data from 145 teachers and 146 parents.
Composite formation.
To reduce the number of peer variables included in analyses, a data-driven approach to creating composite variables was used. Exploratory factor analysis (EFA) was conducted in SPSSArmonk, NY, USA. using the principal factors method and oblique rotation. Initially, the number of factors was not specified. The first iteration of the EFA was applied to the 18 peer relationship variables (excluding teacher-reported victimization). This analysis returned five factors with eigenvalues larger than 1; however, the fifth factor had an eigenvalue of 1.05 and was only defined by one variable so the EFA was repeated requesting no more than four factors. Four factors were obtained (determinant > 0.00001; Kaiser–Meyer–Olkin = 0.69; Bartlett’s test of sphericity p < .0001). The first factor was defined by observer ratings of social status, social skills, peer victimization, and aggression, and the proportion of intervals during which the participant received and directed negative interactions with peers (i.e., observer factor). The second factor was defined by parent ratings of overt aggression, peer victimization, peer acceptance, relational aggression, and prosocial behavior (i.e., parent factor). The third factor was defined by teacher ratings of overt aggression, prosocial behavior, relational aggression, and peer acceptance (i.e., teacher factor). Finally, a fourth factor emerged that was defined not by the rater but by the subset of items assessing social integration/withdrawal; this factor comprised teacher ratings of social withdrawal, parent ratings of social withdrawal, and observer-coded social integration (i.e., social withdrawal factor). Rather than using the factor scores generated by the EFA, which had high levels of missingness due to listwise deletion, four scales were constructed using the variables that loaded most highly on each component. Variables with negative factor loadings were reverse scored, then variables were standardized and averaged to create the four composites; the calculated composites were all highly correlated with their respective factor scores (all rs > .9). These composites showed acceptable internal consistency (Cronbach’s α = .65–.88). All were log transformed to correct positive skew, resulting in acceptable skewness and kurtosis (i.e., −1 to 1).
Cortisol
Refer to Koss et al. (2014, 2016) for a full description of salivary cortisol data collection and preparation. Briefly, a hypocortisolism factor was derived from children’s diurnal and laboratory cortisol collected at Sessions 1–4. Parents were instructed to collect saliva samples at morning, midday, and bedtime on 3 days the child was with the parent and not in day care or preschool. In addition, three saliva samples were collected throughout the laboratory session at each of the four assessments, reflecting children’s reactivity to the demands of the laboratory session as a whole (including brief separations, exposure to novel and arousing stimuli, interactions with strangers). Factor scores for children’s diurnal cortisol (intercept, morning cortisol and slope, diurnal change) were extracted from the between-level portion of the multilevel structural equation linear growth model (one estimate of the person-level intercept and one estimate of the person-level slope). Similar procedures were conducted for laboratory cortisol, resulting in one estimate of the person-level intercept (e.g., arrival) and person-level slope (e.g., laboratory reactivity). All multilevel structural equation model (MSEM) analyses for obtaining estimates controlled for children’s time since waking and medication use.
Each of these estimates was entered into a principle component analysis with varimax rotation to obtain a hypocortisolism index; this resulted in a factor reflecting lower morning cortisol, flatter diurnal slope, and a more blunted laboratory response. Higher scores on this factor reflect more hypocortisolism. The factor structure was not invariant across groups (PI, FC, NA), but the factor correlated highly (r = .996) with a mean score composed conceptually based on the criteria for hypocortisolism: low morning cortisol (i.e., morning cortisol reverse scored), flatter diurnal slope, and low laboratory reactivity (laboratory reactivity reverse scored). All results remained the same using the mean score and the factor score (data are available upon request). To remain consistent with previous publications using this sample, the present analyses use the factor scores. Thirty-four children were missing a hypocortisolism score because they had no diurnal data available (8 PI, 1 FC, 4 NA) or because they were late recruits (21 PI).
ADHD Symptoms
Teacher’s responses to the HBQ subscale assessing ADHD symptoms (Cronbach’s α = .85) were used, consistent with previous research highlighting the predictive validity of teacher reports (Power et al., 1998).
Prekindergarten Parenting Quality
An observational method for evaluating parenting quality was derived from Sroufe and colleagues (e.g., Roisman, Padrón, Sroufe, & Egeland, 2002). During each of four laboratory sessions across the ages of 18–60 months, parent and child participated in a 10-min free play interaction and a 10-min structured play/problem-solving interaction, each followed by a request to initiate clean up. Trained coders rated parents’ behaviors to yield two scores for each participant: supportive presence (i.e., extent to which the parent acted as a secure base, such as helping the child feel comfortable with the task, and extent of the parent’s involvement, including his or her attentiveness to the child and the task) and structure and limit setting (i.e., how adequately the parent attempted to establish his/her expectations for the child’s behavior). These scores (rated 1–7) were combined to yield an overall parenting quality variable, with higher scores = better quality. Initially, coders were trained by the third author (who was trained by A. Sroufe) to 80% agreement within one scale point using 10 videotapes. Reliability was maintained by having a pair of coders rate 20% of the cases and verifying agreement between informants (ICC supportive presence = .79, structure and limit setting = .81). A weighted mean of the four sessions’ scores was used (Cronbach’s α = .79, missing = 3 due to absence of any coded data). This mean was weighted toward later sessions to reflect the expectation that assessments closer to kindergarten would have a stronger association with kindergarten behavior.
Results
Data Analytic Plan
Group differences (PI, FC, NA) in peer problems were assessed using four separate linear regressions with each peer composite (observer-rated, parentrated, and teacher-rated peer problems, social withdrawal) as the outcome variable. Child sex, age at kindergarten, and the proportion of structured versus unstructured time in the kindergarten classroom were initially used as covariates (note, age at adoption was not included as a covariate because of the difficulty with using a continuous measure of age at adoption given that all NA children would have 0s here, and age at adoption and FC vs. PI status is confounded; however, correlational results showed that age at adoption was not significantly associated with teacher-reported peer problems within the PI [r = − .04, p = .76] or FC groups [r = −.16, p = .33]). Two dummy-coded group variables with PI as the reference group were entered to assess the effect of group. Next, to assess whether parenting quality moderated the association between group and each of the peer composites, parenting quality (centered) and the interaction of parenting quality with group were added to each of the four regression models in a stepwise manner. Group differences in hypocortisolism were assessed via a separate linear regression analysis, with child sex and child age at Session 1 as initial covariates. Next, a path analysis was conducted to assess the mediating roles of hypocortisolism and ADHD symptoms in the association between group and peer problems (see Figure 1 for a conceptual model). A product-of-coefficients approach using bootstrapped standard errors was used, as recommended by Preacher and Hayes (2008), to test the pathway delineated by paths a, b, and c in Figure 1. Missing data were handled using full-information maximum likelihood using the “lavaan” package in R (Rosseel, 2012), although results remained the same when using multiple imputation (note, multiple imputation procedures and results available upon request). In all analyses, covariates that were not significant in initial models were omitted from final models for parsimony.
Descriptive Statistics
Descriptive statistics for variables of interest are shown in Table 2, and intercorrelations are shown in Table 3. All peer problems variables were relatively highly correlated except for social withdrawal, which was not significantly correlated with any of the other factors.
Table 2.
Descriptive Statistics of the Variables of Interest by Group
| PI M (SD) |
FC M (SD) |
NA M (SD) |
Grand M (SD) |
|
|---|---|---|---|---|
| 1. Peer problems—observer | 0.21 (0.18) | 0.18 (0.19) | 0.12 (0.10) | 0.17 (0.17) |
| 2. Peer problems—parent | 0.28 (0.15) | 0.29 (0.13) | 0.25 (0.12) | 0.28 (0.14) |
| 3. Peer problems—teacher | 0.27 (0.17) | 0.23 (0.15) | 0.17 (0.12) | 0.23 (0.16) |
| 4. Peer problems—social withdrawal | 0.30 (0.16) | 0.31 (0.13) | 0.30 (0.14) | 0.30 (0.15) |
| 5. ADHD symptoms | 0.54 (0.45) | 0.46 (0.44) | 0.24 (0.37) | 0.43 (0.44) |
| 6. Hypocortisolism | 0.57 (0.64) | 0.51 (0.65) | −1.05 (0.68) | 0.02 (1.00) |
| 7. Parenting quality | 5.60 (0.67) | 5.70 (0.75) | 5.69 (0.70) | 5.66 (0.69) |
Note. PI = postinstitutionalized; FC = foster care; NA = nonadopted; ADHD = attention deficit hyperactivity disorder.
Table 3.
Correlations Among Variables of Interest
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Peer problems—observer | 1 | |||||
| 2. Peer problems—parent | .30*** | 1 | ||||
| 3. Peer problems—teacher | .32*** | .33*** | 1 | |||
| 4. Peer problems—social withdrawal | .08 | .10 | .11 | 1 | ||
| 5. ADHD symptoms | .19* | .29*** | .66*** | −.03 | 1 | |
| 6. Hypocortisolism | .12 | .13 | .25** | .03 | .26** | 1 |
| 7. Parenting quality | −.06 | −.07 | −.28*** | −.07 | −.24** | −.06 |
Note. Values calculated using pairwise complete observations. ADHD = attention deficit hyperactivity disorder.
p < .05.
p < .01.
p < .001.
Covariates
There was a significant effect of child sex on teacher-rated peer problems, b = .06, t(143) = 2.42, p < .05, with boys having more problems than girls. Thus, sex was included as a covariate in final analyses predicting peer problems. Remaining covariates (i.e., age at kindergarten, proportion of structured to unstructured time) were not significant in predicting peer problems or hypocortisolism and so were not included in further analyses.
Group Predicting Peer Problems
Controlling for sex, group significantly predicted observer- and teacher-rated peer problems (see Table 4, Step 1). According to observers, PI children had significantly more peer problems than did NA children, with FC children in the middle and not significantly different than either group. According to teachers, PI children had significantly more peer problems than both NA and FC children. Due to the absence of group differences in parent-rated peer problems and social withdrawal, these peer composites were not investigated further and are thus not included in Table 4. Figure 2 shows peer problem ratings by group for all four composites.
Table 4.
Hierarchical Linear Regression Examining the Main Effect of Group and the Moderating Effect of Parenting Quality on Peer Problems
| Dependent variable |
||||||
|---|---|---|---|---|---|---|
| Observer-rated peer problems |
Teacher-rated peer problems |
|||||
| b (SE) | t Value | ΔR2 | b (SE) | t Value | ΔR2 | |
| 1. Sex | .05 (.03) | 1.83* | .08* | .08 (.03) | 3.03** | .13*** |
| Group—FC | −.04 (.04) | −1.19 | −.07 (.03) | −2.26* | ||
| Group—NA | −.10 (.03) | −2.96** | −.11 (.03) | −3.70*** | ||
| 2. Parenting | −.00 (.01) | −0.21 | .00 | −.03 (.02) | −2.80** | .05** |
| 3. FC × Parenting | .08 (.03) | 2.45* | .05* | .04 (.03) | 1.26 | .01 |
| NA × Parenting | .00 (.03) | −0.07 | .03 (.03) | 0.89 | ||
Note. For the factored group variable, PI is always used as the reference group. PI = postinstitutionalized; FC = foster care; NA = nonadopted.
p < .05.
p < .01.
p < .001.
Figure 2.
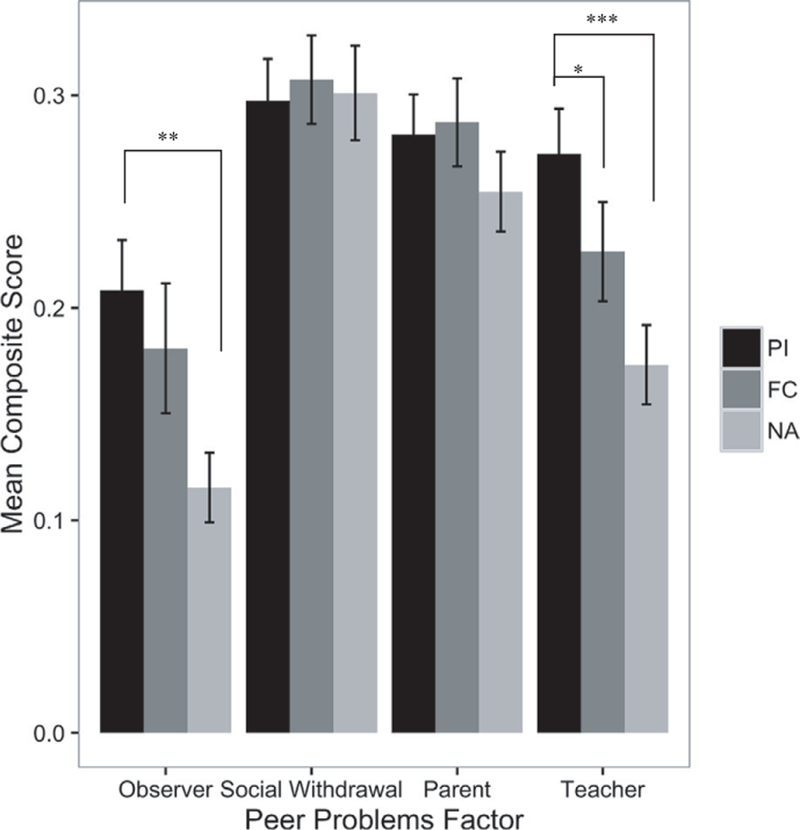
Group differences in peer problems. Raw, nonimputed values used, with bars indicating standard error of the mean. PI = postinstitutionalized; FC = foster care; NA = nonadopted.
*p < .05. **p < .01. ***p < .001.
Parenting Moderation of Group to Peer Problems
Parenting quality was significantly directly related to teacher-reported peer problems but did not have a significant indirect effect (see Table 4, Steps 2 and 3). Conversely, parenting quality was not significantly related to observer-reported peer problems, but the interaction of group (PI vs. FC) and parenting quality was significant. To probe this interaction, simple slopes were calculated following procedures outlined by Aiken and West (1991) to test whether PI versus FC status was associated with observer-rated peer problems at high and low (±1 SD from the mean) levels of parenting quality. Simple slope analysis indicated that PI versus FC status was associated with more peer problems when paired with lower (b = −.05, t = −2.22, p < .05) but not higher parenting quality (b = −.04, t = −1.80, p = .07). Visual inspection of Figure 3 suggests that PI children with low parenting quality had the most peer problems. In contrast, parenting quality appears to have little impact on NA children’s peer relationship functioning.
Figure 3.
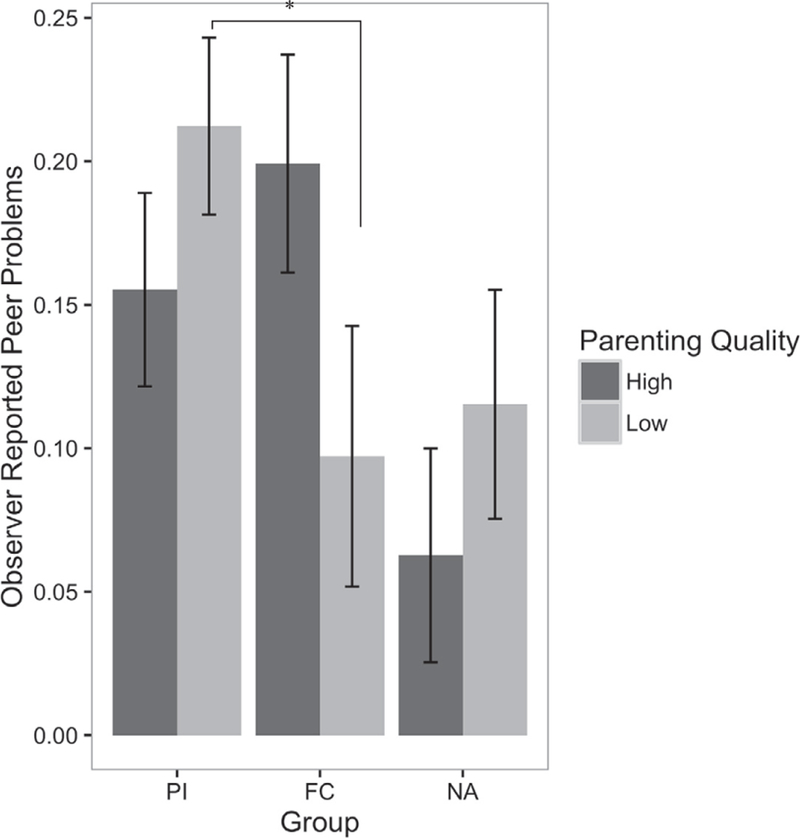
Observer-reported peer problems by group with high- (+1 SD) versus low-quality (−1 SD) parenting and standard error bars. PI = postinstitutionalized; FC = foster care; NA = nonadopted.
*p < .05.
Cortisol and ADHD Mediation of Group to Peer Problems
First, as a reflection of our earlier report (Koss et al., 2016), even in this subsample of children who attended kindergarten, group significantly predicted hypocortisolism (R2 = .57, p < .001). PI children had more blunted patterns of cortisol than NA children, b = −1.62, t(134) = −11.93, p < .001. Group membership alone accounted for 56% of the variance in hypocortisolism levels. ADHD symptoms were also significantly different by group. PI children displayed more teacher-reported ADHD symptoms compared to NA children, b = −.30, t (142) = −3.51, p < .001. FC children were in the middle and not significantly different than PI children for both hypocortisolism and ADHD symptoms.
Hypocortisolism was significantly associated with higher teacher-reported peer problems, b = .04, t(116) = 2.75, p < .01, but not with those reported by trained observers or parents, b = .02, t(109) = 1.23, p = .22; b = .02, t(114) = 1.44, p = .15, respectively. ADHD symptoms predicted observer-, parent-, and teacher-reported peer problems, b = .07, t(135) = 2.24, p < .05; b = .09, t(141) = 3.58, p < .001; b = .23, t(143) = 10.44, p < .001, respectively, such that more ADHD symptoms were associated with more peer problems, regardless of informant. Because teacher-reported problems were the only ones associated with both hypocortisolism and ADHD symptoms, this variable was the only one examined as a possible outcome of multiple mediation.
The path analysis was modeled as shown in Figure 4. All paths in the proposed multiple mediation were significant for PI children compared to NA children but, consistent with the results above, FC children were not significantly different from PI children. The final model explains 42.6% of the variance in teacher-reported peer problems. The indirect effect, modeled by the product of the coefficients for paths a, b, and c with bootstrapped standard errors, was significant (b = −.05, z = −3.00, p < .01), suggesting significant mediation by both hypocortisolism and ADHD symptoms. Additionally, path d was no longer significant, which suggests complete mediation by these variables.
Figure 4.
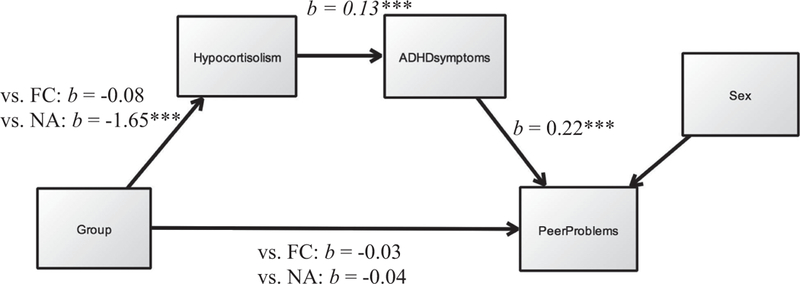
Final results of path analysis. Postinstitutionalized children are the reference group. ADHD = attention deficit hyperactivity disorder; FC = foster care; NA = nonadopted.
***p < .001.
Discussion
The present study used a multimethod, multi-informant approach to investigate peer relationship functioning among internationally adopted kindergarten-aged PI children compared with children adopted internationally from FC and children born and raised in the United States. As hypothesized, PI children, who were all adopted after the age of 17 months, had more peer difficulties than never-institutionalized NA children. Because NA children came from homes similar in income and parental education to PI children’s adoptive homes, findings are consistent with the argument that PI children’s experiences prior to adoption may be responsible for differences between the two groups. These results are also consistent with previous studies that demonstrate poorer social functioning among young PI children compared with family-reared controls and within-country adoptees (Ames, 1997; Fisher et al., 1997; Sonuga-Barke et al., 2010). The present findings provide evidence that the peer difficulties previously documented in older PI children, adolescents, and adults (e.g., Hodges & Tizard, 1989; Pitula et al., 2014; Sonuga-Barke et al., 2010) are also characteristic of young PI children’s early social functioning.
In the present study, the group differences described above were not noted using parent report. Previous studies using parent report have noted that parents rated PI children as exhibiting more social problems than NA and earlier adopted youth (e.g., Fisher et al., 1997; Gunnar et al., 2007; Pitula et al., 2014). However, in the majority of those studies, PI children were older than those in the present study. It is also the case that in previous studies, parent-reported behavioral and emotional problems tended to be greater among older than younger children (e.g., Gunnar et al., 2007). Thus, it may be that deficits in peer competence for PI children become more obvious to parents with age either because of the increasing competence of PI children’s peers or because of the increasing opportunities to obtain feedback from teachers about peer issues their children are having at school.
On the social withdrawal dimension, PI children did not differ from FC or NA children. This is somewhat surprising given previous findings that 2- to 3-year-old Romanian orphanage adoptees scored higher than Canadian-born children on the social withdrawal scale of the Child Behavior Checklist (Fisher et al., 1997). However, in a study of early adolescent youth, a history of institutional care was not associated with social withdrawal (Pitula et al., 2014). It may be that socially withdrawn behaviors are present when PI children first enter the adoptive home and subside as children acclimate to their adoptive environments and habituate to new peers. In fact, Fisher et al. (1997) hypothesized that the adopted PI children in their study were wary of other children behaving unlike the PI children’s orphanage peers, who tended to be oriented to adults and were rather passive, restrained and quiet with peers.
Hypocortisolism was investigated as a potential biological correlate of peer problems that might suggest a mechanism for the transduction of early institutional care into poor peer functioning. As expected, and consistent with previous research in the larger sample from which the children in this study were drawn (Koss et al., 2014, 2016), PI and FC children were at significantly greater risk of hypocortisolism compared with NA children. In turn, we found that hypocortisolism in the years immediately following adoption predicted elevated peer difficulties according to kindergarten teachers. Few studies have addressed the direct link between cortisol regulation and social functioning, and so the present study lends support to the importance of examining these peer outcomes, particularly in PI children, who have consistently been shown to have dysregulated cortisol patterns. Studies of typically developing children that have measured cortisol concurrently with behavior have generally shown that among preschool- and kindergarten-aged children, poor peer functioning is associated with elevations in cortisol rather than blunting (Gunnar et al., 2003, 2010), although during periods when social groups are just forming, elevated cortisol levels are the mode and do not predict poor peer outcomes (Gunnar, Tout, de Haan, Pierce, & Stansbury, 1997). Studies that have examined cortisol activity following periods of victimization have tended to find blunted HPA axis activity (Ouellet-Morin et al., 2011), consistent with the expectation that chronic stress will downregulate the pituitary–adrenal axis (Fries et al., 2005).
To our knowledge, this is the first study to assess HPA axis functioning several years prior to the assessment of peer functioning. The measures of cortisol obtained in the present study were collected early in development, when children were between 1.5 and 5 years of age. Whether or not the children were in out-of-home care (e.g., day care) at this time and thus in the presence of peers was unrelated to cortisol functioning as measured at home and in the laboratory. So although our findings indicated that hypocortisolism was related to international adoption and, in the PI group, to low levels of social interaction with caregivers in the institution (Koss et al., 2014), it is unlikely that poor peer relationships and victimization by peers were producing the hypocortisolism we observed. Thus, in the present study, hypocortisolism a year or more before the assessment of peer functioning predicted lower peer competence.
As expected, problems with attention and hyperactivity/impulsivity were concurrently associated with elevated peer difficulties according to observers, parents, and teachers. This is consistent with research showing that children with inhibitory control difficulties are more likely to have problems with peers, possibly because they are less likely to inhibit impulses, more likely to invade peers’ personal space, and more likely to behave in inattentive and dysregulated manners (e.g., Schwartz, 2000). These types of disinhibited peer behaviors are known to be aversive to peers and are likely to result in victimization and rejection (Hanish et al., 2004). In addition to ADHD, problems with peers may also arise via deficits in social awareness/cognition, prosocial behavior, and propensity to trust, which have been shown to increase with longer durations of institutional care in previous research (Pitula, Wenner, Gunnar, & Thomas, 2016; Wismer Fries & Pollak, 2004).
To further explain the association between early institutional care and peer relationships, ADHD symptoms mediated the association between hypocortisolism and peer problems. Previous research has shown that low cortisol activity predicts attention and externalizing problems (Koss et al., 2016), and other studies have shown associations between ADHD symptoms and peer problems (Stenseng et al., 2015). However, ours is the first to examine relationships among all three of these variables within the same study. The relation between peer functioning and the activity of stress-mediating and behavior regulatory systems is likely to be complex and may involve operant conditioning mechanisms. Previous studies of children reared in deprived, institutional settings have noted hypoarousal of both the HPA and the sympathetic adrenomedullary systems (McLaughlin et al., 2015), and it has been argued that hypoarousal of these systems impairs the individual’s ability to react to regulatory cues of punishment (van Honk, Schutter, Hermans, & Putman, 2003). Insensitivity to punishment cues is argued to lead individuals to engage in behaviors that are antisocial and likely to impair relationships with others (van Goozen, Fairchild, Snoek, & Harold, 2007). To better elucidate the mechanisms underlying peer problems in children with early adverse histories, it will be important to clarify the neurobiology and physiology involved in children’s responses to reinforcement in peer interaction. Studies have also found context-dependent associations between autonomic reactivity to stressful peer experiences and aggression and victimization (e.g., physical vs. relational aggression and victimization, Pitula, Murray-Close, Banny, & Crick, 2015). To understand the mechanisms relating the activity of stress-responsive systems to peer relationship functioning, it may be important to extend beyond the assessment of a single system to examine how multiple systems respond in real time to peer interaction experiences.
In the present study, a history of early institutional deprivation predicted more peer problems but only in the context of relatively lower parenting quality. Thus, supportive postadoption parenting may reduce the detrimental effects of early inconsistent caregiving on later social functioning. These findings lend credence to efforts by several research groups to promote parental responsiveness, sensitivity, and nurturance among parents of maltreated and PI children (Dozier et al., 2012) and are consistent with recent findings showing better social competence (i.e., decreased social reticence with an unfamiliar peer) among PI children who received a supportive FC intervention compared with those who remained in the institution (Almas et al., 2015). Although it is possible that a bidirectional relationship exists between children’s parenting quality and our outcome variables (e.g., children with initial hypocortisolism and regulation problems may be more challenging to parent), a recent study by our group (Lawler, Koss, & Gunnar, 2017) provides evidence for a unidirectional, predictive effect of early parenting on later child regulation in this population.
Note that the moderation effect by parenting only emerged for observer ratings of peer problems. Teachers reported better peer functioning for children whose parents were scored as exhibiting higher parenting quality several years earlier regardless of whether the children were adopted or not. This may reflect the longer time period that teachers had to observe children relative to the few hours of our classroom observations. It may also reflect biases that some teachers may hold based on their knowledge of the adopted children’s backgrounds, which may have made it difficult to detect the moderation effect noted in the more objective observational measures. Nonetheless, this moderation finding should be interpreted with caution as it was not present across informants. In addition, we should note that parents participating in our study were generally supportive and effective, consistent with previous reports indicating that the quality of parenting provided by adoptive parents is typically high (e.g., Brodzinsky & Pinderhughes, 2002). Thus, to the extent that the moderation finding can be replicated, it suggests that many adoptive parents may benefit from additional support and intervention to “supercharge” their parenting abilities in order to promote optimal peer outcomes.
Across the majority of indices of behavioral functioning, FC children’s performance placed them somewhere between NA and PI children; the only significant difference between PI and FC children emerged on the teacher composite of peer functioning. FC children are also expected to have experienced disruptions in care prior to adoption: In the present study, PI and FC children had experienced a similar number of different care settings prior to adoption. Findings suggest that the social impairments experienced by internationally adopted children are not solely the result of institutional neglect but may also be related to experiences common to children adopted internationally from both FC and institutional care, which may include poor prenatal care, early disruption with placement out of the biological home, changes in placements, and/or the experience of adoption into another country. At the same time, the fact that FC children were adopted earlier on average than PI children and did not significantly differ from NA children on most measures of functioning may indicate the dramatic plasticity and recovery that is particularly characteristic of children adopted during the first year of life (van der Voort et al., 2014). Nevertheless, group sizes were relatively small in the present study, and the results likely would have looked different had we used FC children adopted as late as the PI children. When we have done so in previous studies, we have found both FC and PI children to exhibit more problems than NA children (Tarullo, Garvin, & Gunnar, 2011).
Limitations
Although the present study was bolstered by several strengths, most notably its reliance on multiple informants and its prospective longitudinal design, there are several limitations worth noting. The first limitation concerns the use of duration of institutional or foster care as a proxy for measures of caregiving prior to adoption. Children’s experiences are likely to differ within the same type of setting depending on qualities of the institution, country of origin, or family setting in which they are placed. Although we have measures of care quality for this sample, they are based on what the parents observed, which was often founded on only a few minutes of observation. Due to inherent differences between children adopted from FC and from institutional care, and because we wanted our samples to be representative of the larger population from which they were drawn, PI and FC groups in the present study were not matched on age at adoption or country of origin. Similarly, it is possible that children exhibiting more problem behaviors may take longer to be adopted. However, in previous research (e.g. Nelson et al., 2007), when children have been randomized to institutional care as usual or a FC treatment intervention, age at placement has been determined only by when the study began. Given that these children still showed improvements following FC placement, we can be more confident that duration of care is impacting problem behavior rather than the reverse.
Notably, we did not control for racial or ethnic background in our hypocortisolism analyses because we had previously shown that cortisol did not differ by race or ethnicity for this sample (Koss et al., 2014, 2016). There are also several potential limitations concerning the measurement of peer functioning. For example, our assessment of peer functioning did not include measures of friendship, such as the number of reciprocal friendships or friendship quality, content, and closeness, which may be distinct from evaluations of how well one gets along in one’s peer group (Hartup, 1996). In previous studies of PI adolescents, there have been reports of shallow relationships and difficulties forming and maintaining close friendships (Hodges & Tizard, 1989), suggesting that this is an area worth investigating in more depth.
Conclusions and Future Directions
Limitations notwithstanding, the current study provides further evidence that early experiences with inconsistent caregiving may place children at risk for social maladjustment. These findings highlight the important role of supportive and responsive caregiving in future socioemotional competence, as well as the influence of biological and behavioral dysregulation. Given some evidence that peer problems increase as PI children age (Sonuga-Barke et al., 2010), further research is needed to more fully describe the developmental course of social adjustment and related difficulties in children who have been exposed to psychosocially depriving caregiving. The present study provides an important first step by documenting the emergence of a broad range of social deficits as early as kindergarten and the contributions of patterns of cortisol and behavior and attention regulation to these difficulties.
Consistent with transactional models of risk (e.g., Cicchetti & Valentino, 2006), it is likely that early peer difficulties contribute to later peer problems via dynamic and reciprocal interactions across multiple systems (e.g., academic functioning, self-esteem, stress, and associated alterations in physiological systems). For instance, children who are rejected by peers are more limited in their opportunities to learn critical social skills, such as cooperative problem solving and effective conflict management, which leads to more peer rejection, associations with unskilled/unpopular peers, socialization of deviant social skills, and so on (Hartup & Moore, 1990). Moreover, there is some evidence to suggest that the combination of blunted cortisol responses and peer problems, particularly victimization, places children at elevated risk for the development of emotional symptoms such as depression (Von Klitzing et al., 2012). Emerging evidence also suggests that some genotypes are more susceptible to the negative impacts of early adverse care, particularly with regard to attention problems (Stevens et al., 2009). For these reasons, it is important to intervene as early as possible by addressing processes that are known to increase risk for early peer difficulties. By targeting key mechanisms early in life, such as by improving self-regulation and addressing biological stress regulation mechanisms, it may be possible to redirect developmental pathways away from pervasive maladaptation, thereby reducing the need for costlier interventions and, ultimately, decreasing the burden of mental illness on children, families, and their communities.
Acknowledgments
This research was supported in part by P50MH078105. Preparation of this manuscript was facilitated by a doctoral fellowship to Clio E. Pitula from the Social Sciences and Humanities Research Council of Canada.
Contributor Information
Clio E. Pitula, University of Colorado, School of Medicine
Megan R. Gunnar, University of Minnesota
References
- Aiken LS, & West SG (1991). Multiple regression: Testing and interpreting interactions Newbury Park, CA: Sage. [Google Scholar]
- Almas AN, Degnan KA, Walker OL, Radulescu A, Nelson CA, Zeanah CH, & Fox NA (2015). The effects of early institutionalization and foster care intervention on children’s social behaviors at the age of eight. Social Development, 24, 225–239. 10.1111/sode.12089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ames E (1997). The development of Romanian orphanage children adopted to Canada (Final Report to the National Welfare Grants Program: Human Resources Development Canada) Burnaby, BC: Simon Fraser University. [Google Scholar]
- Bernard K, Zwerling J, & Dozier M (2015). Effects of early adversity on young children’s diurnal cortisol rhythms and externalizing behavior. Developmental Psychobiology, 57, 935–947. 10.1002/dev.21324 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brodzinsky D, & Pinderhughes E (2002). Parenting and child development in adoptive families. In Bornstein MH (Ed.), Handbook of parenting (Vol. 1, pp. 279–313). Mahwah, NJ: Erlbaum. [Google Scholar]
- Cicchetti D, & Valentino K (2006). Ecological-transactional perspective on child maltreatment: Failure of the average expectable environment and its influence on child development. In Cicchetti D & Cohen DJ (Eds.), Development and psychopathology (Vol. 3, 2nd ed., pp. 129–201). New York, NY: Wiley. [Google Scholar]
- Coie JD, Dodge KA, & Kupersmidt JB (1990). Peer group behavior and social status. In Asher SR & Coie JD (Eds.), Peer rejection in childhood (pp. 17–59). New York, NY: Cambridge University Press. [Google Scholar]
- Dozier M, Peloso E, Lindhiem O, Gordon MK, Manni M, Sepulveda S, … Levine S (2006). Developing evidence based interventions for foster children: An example of a randomized clinical trial with infants and toddlers. Journal of Social Issues, 62, 767–785. 10.1111/j.1540-4560.2006.00486.x [DOI] [Google Scholar]
- Dozier M, Zeanah CH, Wallin AR, & Shauffer C (2012). Institutional care for young children: Review of literature and policy implications. Social Issues and Policy Review, 6, 1–25. 10.1111/j.1751-2409.2011.01033.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Essex MJ, Boyce TW, Heim Goldstein L, Armstrong JM, Kraemer HC, Kupfer DJ, … MacArthur Assessment Battery Working Group. (2002). The confluence of mental, physical, social, and academic difficulties in middle childhood. II: Developing the MacArthur Health and Behavior Questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 41, 588–603. 10.1097/00004583-200205000-00017 [DOI] [PubMed] [Google Scholar]
- Fisher L, Ames EW, Chisholm K, & Savoie L (1997). Problems reported by parents of Romanian orphans adopted to British Columbia. International Journal of Behavioral Development, 20, 67–82. 10.1080/016502597385441 [DOI] [Google Scholar]
- Fries E, Hesse J, Hellhammer J, & Hellhammer D (2005). A new view on hypocortisolism. Psychoneuoendocrinology, 30, 1010–1016. 10.1016/j.psyneuen.2005.04.006 [DOI] [PubMed] [Google Scholar]
- Groza V (1999). Institutionalization, behavior, and international adoption. Journal of Immigrant Health, 1, 133–143. 10.1023/A:1022060902280 [DOI] [PubMed] [Google Scholar]
- Groza V, & Ryan SD (2002). Pre-adoption stress and its association with child behavior in domestic special needs and international adoptions. Psychoneuroendocrinology, 27, 181–197. 10.1016/S0306-4530(01)00044-0 [DOI] [PubMed] [Google Scholar]
- Gunnar MR, Kryzer E, van Ryzin M, & Phillips D (2010). The rise in cortisol in family day care: Associations with aspects of care quality, child behavior, and child sex. Child Development, 81, 851–869. 10.1111/j.1467-8624.2010.01438.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gunnar M, & Quevedo K (2007). The neurobiology of stress and development. Annual Review of Psychology, 58, 145–173. 10.1146/annurev.psych.58.110405.085605 [DOI] [PubMed] [Google Scholar]
- Gunnar MR, Sebanc AM, Tout K, Donzella B, & van Dulmen MM (2003). Peer rejection, temperament, and cortisol activity in preschoolers. Developmental Psychobiology, 43, 346–358. 10.1002/dev.10144 [DOI] [PubMed] [Google Scholar]
- Gunnar MR, Tout K, de Haan M, Pierce S, & Stansbury K (1997). Temperament, social competence, and adrenocortical activity in preschoolers. Developmental Psychobiology, 31, 65–85. [DOI] [PubMed] [Google Scholar]
- Gunnar MR, van Dulmen MH; International Adoption Project Team. (2007). Behavior problems in postinstitutionalized internationally adopted children. Development and Psychopathology, 19, 129–148. 10.1017/s0954579407070071 [DOI] [PubMed] [Google Scholar]
- Gunnar MR, & Vasquez DM (2001). Low cortisol and a flattening of expected daytime rhythm: Potential indices of risk in human development. Development and Psychopathology, 13, 515–538. [DOI] [PubMed] [Google Scholar]
- Hanish LD, Eisenberg N, Fabes RA, Spinrad TL, Ryan P, & Schmidt S (2004). The expression and regulation of negative emotions: Risk factors for young children’s peer victimization. Developmental Psychobiology, 16, 335–353. https://doi.org/10.10170S0954579404044542 [DOI] [PubMed] [Google Scholar]
- Hartup WW (1996). The company they keep: Friendships and their developmental significance. Child Development, 67, 1–13. 10.1111/j.1467-8624.1996.tb01714.x [DOI] [PubMed] [Google Scholar]
- Hartup WW, & Moore SG (1990). Early peer relations: Developmental significance and prognostic implications. Early Childhood Research Quarterly, 5, 1–17. 10.1016/0885-2006(90)90002-I [DOI] [Google Scholar]
- Hawk B, & McCall R (2011). Specific extreme behaviors of postinstitutionalized Russian adoptees. Developmental Psychology, 47, 732–738. 10.1037/a0021108 [DOI] [PubMed] [Google Scholar]
- Hodges J, & Tizard B (1989). Social and family relationships of ex-institutional adolescents. Journal of Child Psychology and Psychiatry, 30, 77–97. 10.1111/j.1469-7610.1989.tb00770.x [DOI] [PubMed] [Google Scholar]
- Johnson DE, & Gunnar MR (2011). IV. Growth failure in institutionalized children. Monographs of the Society for Research in Child Development, 76, 92–126. 10.1111/j.1540-5834.2011.00629.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karreman A, de Haas S, van Tuijl C, van Aken MG, & Deković M (2010). Relations among temperament, parenting and problem behavior in young children. Infant Behavior & Development, 33, 39–49. 10.1016/j.infbeh.2009.10.008 [DOI] [PubMed] [Google Scholar]
- Kerr DCR, Capaldi DM, Pears KC, & Owen LD (2009). A prospective three generational study of fathers’ constructive parenting: Influences from family of origin, adolescent adjustment, and offspring temperament. Developmental Psychology, 45, 1257–1275. 10.1037/a0015863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kopala-Sibley DC, Dougherty LR, Dyson MW, Lap-took RS, Olino TM, Bufferd SJ, & Klein DN (2017). Early childhood cortisol reactivity moderates the effects of parent–child relationship quality on the development of children’s temperament in early childhood. Developmental Science, 20, 10.1111/desc.12378 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koss KJ, Hostinar CE, Donzella B, & Gunnar MR (2014). Social deprivation and the HPA axis in early development. Psychoneuroendocrinology, 50, 1–13. 10.1016/j.psyneuen.2014.07.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koss KJ, Mliner SB, Donzella B, & Gunnar MR (2016). Early adversity, hypocortisolism, and behavior problems at school entry: A study of internationally adopted children. Psychoneuroendocrinology, 66, 31–38. 10.1016/j.psyneuen.2015.12.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Landry SH, Smith KE, & Swank PR (2006). Responsive parenting: Establishing early foundations for social, communication, and independent problem-solving skills. Developmental Psychology, 42, 627–642. 10.1037/0012-1649.42.4.627 [DOI] [PubMed] [Google Scholar]
- Lawler JM, Koss KJ, & Gunnar MR (2017). Bidirectional effects of parenting and child behavior in internationally adopting families. Journal of Family Psychology, 31, 563–573. 10.1037/fam0000309 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin CG, Kim HK, Bruce J, & Fisher PA (2014). Child diurnal cortisol rhythms, Parenting quality, and externalizing behaviors in preadolescence. Psychoneuroendocrinology, 40, 170–180. 10.1016/j.psyneuen.2013.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Sheridan MA, Tibu F, Fox NA, Zeanah CH, & Nelson CA (2015). Causal effects of the early caregiving environment on development of stress response systems in children. Proceedings of the National Academy of Sciences of the United States of America, 112, 5637–5642. 10.1073/pnas.1423363112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meaney MJ, & Szyf M (2005). Environmental programming of stress responses through DNA methylation: Life at the interface between a dynamic environment and a fixed genome. Dialogues in Clinical Neuroscience, 7, 103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nelson CA, Zeanah CH, Fox NA, Marshall PJ, Smyke AT, & Guthrie D (2007). Cognitive recovery in socially deprived young children: The Bucharest Early Intervention Project. Science, 318, 1937–1940. 10.1126/science.1143921 [DOI] [PubMed] [Google Scholar]
- Ouellet-Morin I, Odgers CL, Danese A, Bowes L, Shakoor S, Papadopoulos AS, & Arseneault L (2011). Blunted cortisol responses to stress signal social and behavioral problems among maltreated/bullied 12-year-old children. Biological Psychiatry, 70, 1016–1023. 10.1016/j.biopsych.2011.06.017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pepler DJ, & Craig WM (1998). Assessing children’s peer relationships. Child Psychology & Psychiatry Review, 3, 176–182. [Google Scholar]
- Pitula CE, Murray-Close D, Banny AM, & Crick NR (2015). Prospective associations between peer aggression and victimization: The moderating roles of physiological stress reactivity and gender. Social Development, 24, 621–639. 10.1111/sode.12110 [DOI] [Google Scholar]
- Pitula CE, Thomas KM, Armstrong JM, Essex MJ, Crick NR, & Gunnar MR (2014). Peer victimization and internalizing symptoms among post-institutionalized, internationally adopted youth. Journal of Abnormal Child Psychology, 42, 1069–1076. 10.1007/s10802-014-9855-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pitula CE, Wenner JA, Gunnar MR, & Thomas KM (2016). To trust or not to trust: Social decision-making in post-institutionalized, internationally adopted youth. Developmental Science, 20, e12375 10.1111/desc.12375 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Power TJ, Doherty BJ, Panichelli-Mindel SM, Karustis JL, Eiraldi RB, Anastopoulos AD, & DuPaul GJ (1998). The predictive validity of parent and teacher reports of ADHD symptoms. Journal of Psychopathology and Behavioral Assessment, 20, 57–81. [Google Scholar]
- Preacher KJ, & Hayes AF (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891. 10.3758/BRM.40.3.879 [DOI] [PubMed] [Google Scholar]
- Raaska H, Lapinleimu H, Sinkkonen J, Salmivalli C, Matomäki J, Mäkipää S, & Elovainio M (2012). Experiences of school bullying among internationally adopted children: Results from the Finnish Adoption (FINADO) Study. Child Psychiatry and Human Development, 43, 592–611. 10.1007/s10578-012-0286-1 [DOI] [PubMed] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, & Telch MJ (2010). Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse & Neglect, 34, 244–252. 10.1016/j.chiabu.2009.07.009 [DOI] [PubMed] [Google Scholar]
- Roisman GL, Padrón E, Sroufe LA, & Egeland B (2002). Earned-secure attachment status in retrospect and prospect. Child Development, 73, 1204–1219. 10.1111/1467-8624.00467 [DOI] [PubMed] [Google Scholar]
- Rosseel Y (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48, 1–36. 10.18637/jss.v048.i02 [DOI] [Google Scholar]
- Rutter M, Beckett C, Castle J, Colvert E, Kreppner J, Mehta M, & Sonuga-Barke E (2007). Effects of profound early institutional deprivation: An overview of findings from a UK longitudinal study of Romanian adoptees. European Journal of Developmental Psychology, 4, 332–350. 10.1080/17405620701401846 [DOI] [Google Scholar]
- Rutter ML, Kreppner JM, & O’Connor TG (2001). Specificity and heterogeneity in children’s responses to profound institutional privation. British Journal of Psychiatry, 179, 97–103. 10.1192/bjp.179.2.97 [DOI] [PubMed] [Google Scholar]
- Sapolsky RM, Romero LM, & Munck AU (2000). How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocrine Reviews, 21, 55–89. 10.1210/edrv.21.1.0389 [DOI] [PubMed] [Google Scholar]
- Schwartz D (2000). Subtypes of victims and aggressors in children’s peer groups. Journal of Abnormal Child Psychology, 28, 181–192. 10.1023/A:1005174831561 [DOI] [PubMed] [Google Scholar]
- Shin Y, & Kim HY (2008). Peer victimization in Korean preschool children: The effects of child characteristics, parenting behaviours and teacher-child relationships. School Psychology International, 29, 590–605. 10.1177/0143034308099203 [DOI] [Google Scholar]
- Sonuga-Barke EJ, & Kreppner J (2012). The development and care of institutionally reared children. Child Development Perspectives, 6, 174–180. 10.1111/j.1750-8606.2011.00231.x [DOI] [Google Scholar]
- Sonuga-Barke EJ, Schlotz W, & Kreppner J (2010). Differentiating developmental trajectories for conduct, emotion, and peer problems following early deprivation. Monographs of the Society for Research in Child Development, 75, 102–124. 10.1111/j.1540-5834.2010.00552.x [DOI] [PubMed] [Google Scholar]
- Stams GJM, Juffer F, & van IJzendoorn MH (2002). Maternal sensitivity, infant attachment, and temperament in early childhood predict adjustment in middle childhood: The case of adopted children and their biologically unrelated parents. Developmental Psychology, 38, 806–821. 10.1037/0012-1649.38.5.806 [DOI] [PubMed] [Google Scholar]
- Stenseng F, Belsky J, Skalicka V, & Wichstrøm L (2015). Peer rejection and attention deficit hyperactivity disorder symptoms: Reciprocal relations through ages 4, 6, and 8. Child Development, 87, 365–373. 10.1111/cdev.12471 [DOI] [PubMed] [Google Scholar]
- Stevens SE, Kumsta R, Kreppner JM, Brookes KJ, Rutter M, & Sonuga-Barke EJ (2009). Dopamine transporter gene polymorphism moderates the effects of severe deprivation on ADHD symptoms: Developmental continuities in gene–environment interplay. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 150, 753–761. 10.1002/ajmg.b.31010 [DOI] [PubMed] [Google Scholar]
- Tan TX, & Camras LA (2011). Social skills of adopted Chinese girls at home and in school: Parent and teacher ratings. Children and Youth Services Review, 33, 1813–1821. 10.1016/j.childyouth.2011.05.006 [DOI] [Google Scholar]
- Tarullo AR, Garvin MC, & Gunnar MR (2011). Atypical EEG power correlates with indiscriminately friendly behavior in internationally adopted children. Developmental Psychology, 47, 417–431. 10.1037/a0021363 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van den Dries L, Juffer F, van IJzendoorn MH, & Bakermans-Kranenburg MJ (2010). Infants’ physical and cognitive development after international adoption from foster care or institutions in China. Journal of Developmental & Behavioral Pediatrics, 31, 144–150. 10.1097/DBP.0b013e3181cdaa3a [DOI] [PubMed] [Google Scholar]
- van der Voort A, Linting M, Juffer F, Schoenmaker C, Bakermans-Kranenburg MJ, & van IJzendoorn MH (2014). More than two decades after adoption: Associations between infant attachment, early maternal sensitivity and the diurnal cortisol curve of adopted young adults. Children and Youth Services Review, 46, 186–194. 10.1016/j.childyouth.2014.08.022 [DOI] [Google Scholar]
- van Goozen SH, Fairchild G, Snoek H, & Harold GT (2007). The evidence for a neurobiological model of childhood antisocial behavior. Psychological Bulletin, 133, 149–182. 10.1037/0033-2909.133.1.149 [DOI] [PubMed] [Google Scholar]
- van Honk J, Schutter DJ, Hermans EJ, & Putman P (2003). Low cortisol levels and the balance between punishment sensitivity and reward dependency. NeuroReport, 14, 1993–1996. 10.1097/01.wnr.0000091690.72892.ec [DOI] [PubMed] [Google Scholar]
- van IJzendoorn MH, Palacios J, Sonuga-Barke EJ, Gunnar MR, Vorria P, McCall RB, … Juffer F (2011). I. Children in institutional care: Delayed development and resilience. Monographs of the Society for Research in Child Development, 76, 8–30. 10.1111/j.1540-5834.2011.00626.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanderwert RE, Marshall PJ, Nelson CA, Zeanah CH, & Fox NA (2010). Timing of intervention affects brain electrical activity in children exposed to severe psychosocial neglect. PLoS ONE, 5, e11415 10.1371/journal.pone.0011415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Von Klitzing K, Perren S, Klein AM, Stadelmann S, White LO, Groeben M, … Hatzinger M (2012). The interaction of social risk factors and HPA axis dysregulation in predicting emotional symptoms of five-and six-year-old children. Journal of Psychiatric Research, 46, 290–297. 10.1016/j.jpsychires.2011.12.004 [DOI] [PubMed] [Google Scholar]
- Wismer Fries AB, & Pollak SD (2004). Emotion understanding in postinstitutionalized Eastern European children. Developmental Psychobiology, 16, 355–369. 10.1017/S0954579404044554 [DOI] [PMC free article] [PubMed] [Google Scholar]