

Abstract
Background:
There is considerable literature about revision anterior cruciate ligament (ACL) reconstruction in athletes vut there is little published evidence about the same in the nonathletes. The injury itself may remain underdiagnosed and untreated in nonsports persons. This study highlights the high incidence of ACL injury in the nonathletic patient cohort, revision rates, and the outcomes of revision ACL reconstruction.
Materials and Methods:
856 nonathletic patients who underwent primary ACL reconstruction were included in this retrospective study. Patients were asked on phone whether they had undergone revision surgery and whether they had symptoms severe enough to seek reintervention. Clinical assessment and preoperative and postoperative International Knee Documentation Committee (IKDC) and Lysholm scoring were used to followup patients who underwent revision intervention.
Results:
Clinically, symptomatic revision rate was 5.9% (51 out of 856 patients), and 33 out of these 856 patients (3.9%) underwent revision ACL reconstruction. The reasons for revision were rupture of the previous graft in 21 and laxity (incompetence) of the graft in 12 patients. The mean preoperative and postoperative IKDC scores were 44.1 and 69.8, respectively, and the improvement was statistically significant (P < 0.001). The IKDC score following revision ACL reconstruction was significantly better in those patients who underwent revision <1 year following the onset of recurrent symptoms (P = 0.015). Meniscal tears were present in 47.6%, and chondral injuries were seen in 33.3% of patients. The tibial tunnel positioning was abnormal in 70% of patients. Femoral tunnel positioning was aberrant in all the patients.
Conclusions:
The revision rate of primary ACL reconstruction of 5.9% in nonathletes and revision ACL reconstruction rate of 3.9% are similar to the reported revision rates of 2.9%–5.8% in athletic patients. Similar to athletes, suboptimal tunnel placement is the major contributor to failure in nonathletes also.
Keywords: Anterior cruciate ligament, anterior cruciate ligament reconstruction, graft failure, revision anterior cruciate ligament reconstruction
Introduction
Anterior cruciate ligament (ACL) injury is one of the most common musculoskeletal injuries with an annual incidence of around 200,000 patients in the United States.1 Intraarticular ACL reconstruction using tendon autograft is the treatment of choice for symptomatic ACL tears with a reported success rate between 75% and 97%.2,3,4 While there is a huge body of literature on ACL injuries, reconstruction and revision operations in athletes published evidence on ACL injuries in nonathletes is conspicuous by its paucity.5 A few centers (including ours) cater to significant numbers of ACL injuries in patients who are not athletes and whose injuries occurred due to reasons other than sports.
Revision ACL reconstruction is an option for patients with symptomatic failures following primary ACL reconstruction. The average revision rate following revision ACL reconstruction in athletes is around 13.7% compared with the average revision rate of 2.9%–5.8% following primary ACL reconstructions.6,7,8,9,10,11,12 All studies6,9,13,14,15,16,17,18,19 except one by Garofolo et al.20 have reported that only around 60%–80% of patients can regain the preinjury sporting ability following revision ACL reconstruction.
The aim of the present study is to study the revision rate of primary ACL reconstruction and the functional outcomes following revision ACL reconstruction in the nonsportsperson population. It provides valuable data for comparison with the published data on revision rates and revision outcomes in the cohorts of athletes. To the best of our knowledge, such data have not been published in the English language literature until now.
Materials and Methods
1318 patients in which arthroscopic primary ACL reconstruction was performed between February 2008 and June 2012 were included in this retrospective study. The approval of the Institutional Ethics Committee was obtained before the commencement of the study. Among these patients, 263 patients were actively involved in sports at various levels and had sustained ACL injury during sports activities. They were excluded from the study since the focus of the study was on the failures of ACL reconstruction in the nonsportsperson population. Forty-two patients with associated posterior cruciate ligament injuries and multi-ligamentous injuries were also excluded. Remaining 1013 patients were not seriously involved in any sports and had sustained ACL injury following two-wheeler accidents (60%), slip and fall indoors during daily activities (20%) and falls outdoors (10%). Most patients with ACL tears following two-wheeler accidents presented with a typical history of deceleration injury. The foot of the injured extremity was planted on the ground to avoid a fall while the vehicle was still moving followed by the driver falling off the vehicle to the side of the injury. ACL injuries due to falls were typically low energy injuries with a significant twisting component.
Out of 1013 patients in the nonsportsperson category, 856 patients were available for telephonic followup, and 157 were lost to followup. Mean followup was 5.2 years (range 8.3–4.4 years). Failure was defined as “a knee that demonstrates recurrent pathologic laxity that was present before surgery, or a stable knee that has a range of motion from 10 to 120° of flexion that is stiff and painful even with activities of daily living.”21 A total of 51 out of 856 patients (5.9%) had a symptomatic failure. Thirty-three of the 856 (3.9%) had undergone revision ACL reconstruction [Table 1]. Eighteen patients with symptomatic failure had refused to undergo reoperation.
Table 1.
Patient profile in revision anterior cruciate ligament reconstruction
| Variable | Number of patients |
|---|---|
| Etiology | |
| Re tear | 21 |
| Laxity | 12 |
| Primary intervention | |
| BPTB graft | 19 |
| Hamstring | 14 |
| Tibial tunnel position | |
| Too anterior | 16 |
| Normal | 10 |
| Too posterior | 7 |
| Femur tunnel position | |
| Too anterior | 10 |
| Too anterior and vertical | 19 |
| Too vertical | 4 |
| Time interval between index operation and symptoms | |
| 1 year or less | 19 |
| >1 year | 14 |
| Duration of symptoms prior to reoperation | |
| 1 year or less | 20 |
| >1 year | 13 |
BPTB=Bone -Patellar tendon - Bone
The reasons for revision were rupture of the previous graft in 21 and laxity (incompetence) of the graft in 12 patients. In patients with rupture of the graft, second episode of fall from two-wheeler or slip and fall was the reason for injury to the ACL graft. At the time of primary intervention, patellar bone-tendon-bone (B-T-B) graft had been used in 19 patients, and four-strand hamstring graft had been used in 14 patients. The new lesions were confirmed using magnetic resonance imaging (MRI) scan and laxity was evaluated on KT-1000 arthrometer. The duration of time between the onset of recurrent symptoms and reoperation varied from 1 month to 72 months (mean 20.9 standard deviation [SD] 24.5). The patients were divided into two groups – those who were operated within 1 year of the onset of recurrent symptoms and those who were operated after 1 year from the onset of recurrent symptoms.
All the revisions were performed in one sitting, and no patient had staged revision in our series. Patients with earlier hamstring grafts underwent revision using patellar B-T-B grafts and vice versa. The femoral and tibial tunnel positions that were used at the time of primary operation were assessed using the Bernard and Hertel grid.21 A true lateral image of the knee is obtained using the image intensifier with the knee in 90° of flexion and the medial and lateral femoral condyles overlapping as closely as possible. The Bernard-Hertel grid is drawn as follows – The Blumensaat's line is drawn first as a tangent to the roof of the intercondylar notch. It represents the maximum sagittal diameter of the lateral femoral condyle. Two lines are drawn perpendicular to the Blumensaat's line, at the anterior and posterior borders of the lateral femoral condyle. A third line is drawn parallel to the Blumensaat's line along the inferior border of the condyle. Measurements are made along the Blumensaat's line and along the perpendicular line at the posterior border of the lateral femoral condyle which represents the maximum height of the intercondylar notch. It has been shown that the center of the femoral attachment of the ACL is located at a point which is located at the 27% mark along Blumensaat's line and 34% mark of the height of the intercondylar notch (with the zero% mark at the posterior end of the Blumensaat's line.
In patients with faulty placement of earlier femoral tunnels, new tunnels were drilled in the desired position using the anteromedial portal technique [Figures 1 and 2]. No significant problems were experienced during repositioning the tibial tunnels. In 8 patients, the entry point of the old femoral tunnel was too close to the entry hole of the new tunnel, leaving a narrow bridge of bone between the tunnels. This led to the poor purchase of the interference screw inserted via the inside-out technique. In such patients, outside-in interference screw insertion was used to improve the screw purchase. The minimum diameter of the graft (both BPTB and hamstring grafts) used to fill the tunnels was 10 mm. Postoperative rehabilitation included an active range of motion exercises from the 1st postoperative day and gradually increasing partial weight bearing with elbow crutches for 3 weeks. The hinged knee brace was applied during ambulation for 3 weeks. Routine daily activities were permitted after 4 weeks and physically demanding activities such as running were allowed after 12 weeks and sporting activities were allowed after 9 months.
Figure 1.
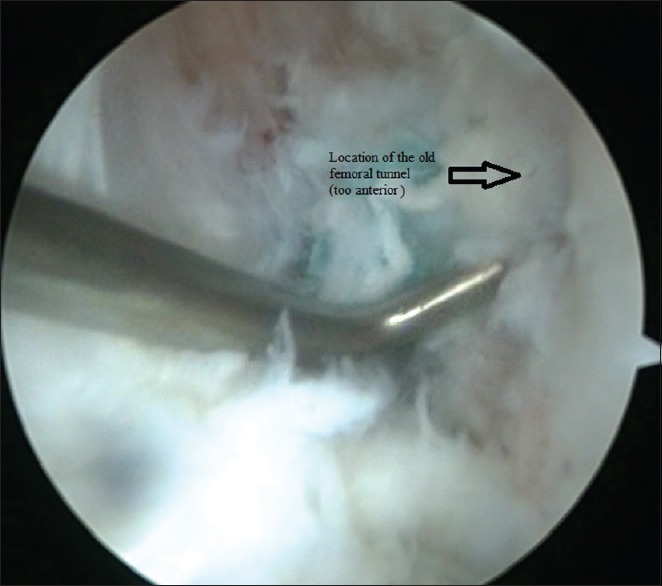
Aberrant femoral tunnel placement during primary anterior cruciate ligament reconstruction (tunnel has been placed too anteriorly)
Figure 2.
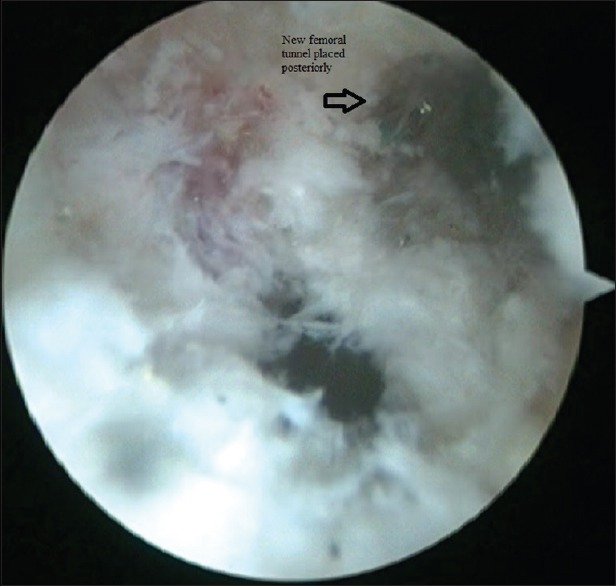
Tunnel has been revised to the optimal position (moved posteriorly) during revision anterior cruciate ligament reconstuction
Tunnel widening was measured on MRI using the techniques described earlier by Clatworthy et al.22 and Weber et al.23 Tunnel widening was defined as increase in the diameter by 50% over the initial diameter.22 Tunnel widening was seen in 6 patients with tibial tunnels that were acceptably placed during the index operation. No differences were found between B-T-B and hamstring grafts regarding tunnel widening. When B-T-B graft was used, tunnel widening was managed using grafts with thicker bone plugs with or without interference screws of larger diameter than those used in the earlier operation. When hamstring grafts were used for the revision procedure, 6-strand grafts were used to increase the bulk of the graft. No allografts or synthetic grafts were used in any of the patients. Additional autologous bone grafting was not performed in any of our patients to fill the mouth of the tunnels facing the intraarticular surface. Notchplasty was performed in 3 patients in whom the notch was too narrow. Arthroscopic partial meniscectomy was performed in 20 patients with meniscal tears.
Outcomes were assessed using the International Knee Documentation Committee (IKDC)24 and the Lysholm25 scores. Scores were obtained preoperatively and 6 months and annually during followup. Data analysis was performed with the help of computer using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA, version 19.0). Student's t-test was used to test the significance of difference between quantitative variables. Yate's and Fisher's Chi-square tests were used for qualitative variables. A P < 0.05 was considered to denote significant relationship.
Results
The mean age of the patients was 29.9 years (range 20–38 years). The mean interval of time between initial operation and revision was 5.3 years (range 4–9 years). The right knee was involved in 65% of patients and the left knee in 35% of patients. The ratio between sports-related and nonsports-related ACL injury in our series was 1:3.9.
Overall rate of symptomatic failure of primary ACL reconstruction was 5.9% and revision ACL reconstruction rate was 3.9% and there were no patients in our series who presented with failed reconstruction following the revision and no re-revisions were performed till date. In the revision cohort, the tibial tunnel positioning was abnormal in 23 out of 33 of patients. The tibial tunnel was too anterior in 16 and too posterior in 7 patients. Femoral tunnel positioning was aberrant in all the 33 patients. In 10 patients, the femoral tunnel was too anterior; in 4 patients, it was too vertical and in the remaining 19 patients, it was too anterior as well as too vertical [Table 1]. Meniscal tears were present in 20 out of 33 patients-bucket handle type of medial meniscal tears in 11 patients, lateral meniscal tears in 6 patients and combined medial and lateral meniscal tears in 3 patients [Table 2]. Chondral injuries were seen in 11 patients. In 7 patients, chondral injury was in the patella and femoral condyles were involved in fourpatients. Two patients showed early changes of osteoarthritis on plain radiographs.
Table 2.
Associated injuries noted at the time of revision anterior cruciate ligament reconstruction
| Associated injury | Number of patients |
|---|---|
| Medial meniscal tears | 11 |
| Lateral meniscal tears | 6 |
| Combined medial and lateral meniscal tears | 3 |
| Chondral injury (patella) | 7 |
| Chondral injury (femoral condyles) | 4 |
The mean preoperative IKDC score was 44.1 (range 16.1–73.6, SD 15.5). The mean postoperative IKDC score was 69.8 (range 38.2–87.3, SD 12.5). The change in IKDC score was statistically significant (P < 0.001). Preoperative Lysholm scores were categorized as poor in 14 patients, fair in 16 patients, and good in 3 patients. Postoperative Lysholm scores were categorized as fair in 14 patients, good in 14 patients, and excellent in 5 patients. The change in scores was statistically significant (P < 0.001).
There was no significant difference in the IKDC scores between patients who had B-T-B and hamstring grafts at the time of primary ACL reconstruction. In addition, there was no significant difference in the scores between patients who underwent revision for re-tear of the graft and those who were revised for excessive laxity of the graft. The only significant difference noted was between patients who were symptomatic for more than 1 year and <1 year following primary ACL reconstruction [Table 3]. The IKDC score following revision ACL reconstruction was significantly better in those patients who underwent revision <1 year following the onset of recurrent symptoms (P = 0.015).
Table 3.
Association between International knee Documentation Committee Scores and other variables following revision anterior cruciate ligament reconstruction
| Variable | Preoperative IKDC score | Postoperative IKDC score | Significance | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| Time interval between onset of symptoms and revision | |||||
| 1 year or less | 40.9 | 14.8 | 65.6 | 13.1 | P=0.0151 (S) |
| >1 year | 50.3 | 15.7 | 77.7 | 5.9 | |
| Cause of failure of ACL reconstruction | |||||
| Rupture of graft | 46.4 | 15.3 | 69.7 | 13.9 | P=0.3737 (NS) |
| Laxity of graft | 40.5 | 15.9 | 69.8 | 10.5 | |
| Type of graft used at index operation | |||||
| B-T-B graft | 43.5 | 14.5 | 68.2 | 13.4 | P=0.7256 (NS) |
| Hamstring graft | 44.9 | 17.5 | 72.0 | 11.3 | |
IKDC=International knee Documentation Committee, ACL=Anterior cruciate ligament, SD=Standard deviation, S=Significant, NS=Not significant
Discussion
The revision rate of around 4% in nonathletes in our study is similar to the revision rates of 2.9%–5.8% in athletes as reported in the earlier studies.6,7,8,9,10,11,12 Errors of femoral tunnel placement were the most common iatrogenic error in our series of nonathletes. Thus, tunnel placement errors are as likely to predispose to failure in nonathletes as in athletes.4 None of the patients in our series has undergone re-revision for failed revision of ACL reconstruction till now. This is much better than the reported average revision rate of 13.7% in athletes undergoing revision ACL reconstructions.11 Correct placement of tunnels during revision surgery, the absence of the risk of reinjury due to contact sports and lifestyle modification by patients to minimize the risk of reinjury are possible explanations for the longevity of the revised grafts in the nonathlete cohorts.
In the nonsportsperson category of patients, there is nil or very low expectation regarding sporting activities and the need for revision ACL reconstruction is related to the symptoms of instability and/or pain that interfere with activities of daily living. Athletes with traumatic re-rupture of the ligament have been said to have better outcomes than patients with gradual failure due to laxity.26 In our study, we found no significant difference (statistical or clinical) between acute traumatic graft failures and gradual failures due to laxity of the graft in nonathletes undergoing revision ACL reconstruction. There was no significant difference in outcomes between revisions using B-T-B and hamstring grafts in our series. This is similar to the experience of other authors in earlier reports.26,27,28,29
While elite athletes are likely to undergo earlier revisions to facilitate earlier return to sports, nonathletes are often likely to delay the revision. In the present series, patients who remained symptomatic for more than 1 year following the failure of the graft had inferior outcome scores (IKDC) than those who presented early following failure of the graft. Our experience is different from that of Johnson et al. who found no significant correlation between the outcome scores and the time interval between failure and revision.26
In the athletic population, delay in revision has been associated with increased incidence of secondary injuries to the menisci, articular cartilage, other ligaments in the knee and coronal plane malalignment of the lower limb.5,30,31,32,33 Joseph et al. reported the significantly higher incidence of meniscal and cartilage injuries in both athletic and nonathletic patient groups when the primary ACL was delayed by more than 1 year.5 There was a high incidence of meniscal (60.6%) and chondral (33.3%) injuries in our patients presenting for revisions. Thus, the ACL-injured knees in nonathletes seem to be as susceptible to secondary injury to menisci and cartilage as the ACL-deficient knees in athletes.
The main limitation of this study is that 15.5% of patients were lost to followup and their outcomes could not be ascertained. However, the cohort in which the desired outcomes could be ascertained was large enough to provide useful information on the outcomes. This study draws attention to the need for high index of suspicion regarding ACL injuries even in nonathletic injuries to the knee, the incidence of revision ACL reconstruction and the medium-term favorable outcomes of the revision surgery in this group of patients. The study draws attention to the fact that revision rates of primary ACL reconstruction in nonathletes are not less than the revision rates in athletes. Errors in tunnel placement during ACL reconstruction are as likely to cause failure in the low-demand nonathlete patients as in the high-demand athletes.
Conclusions
The revision rate following ACL reconstruction in nonathletes in the present study is similar to the rates reported earlier in athletes. Accurate tunnel placement is as important in these patients as in the sportspersons. In our study, delay in revision was associated with lower functional outcome scores and a high incidence of meniscal and chondral injuries. Earlier revision is advisable even in the nonathlete patient groups. Until now, there are no re-revisions of the ACL reconstructions in our patients.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Gianotti SM, Marshall SW, Hume PA, Bunt L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: A national population-based study. J Sci Med Sport. 2009;12:622–7. doi: 10.1016/j.jsams.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 2.Biau DJ, Tournoux C, Katsahian S, Schranz PJ, Nizard RS. Bone-patellar tendon-bone autografts versus hamstring autografts for reconstruction of anterior cruciate ligament: Meta-analysis. BMJ. 2006;332:995–1001. doi: 10.1136/bmj.38784.384109.2F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Spindler KP, Kuhn JE, Freedman KB, Matthews CE, Dittus RS, Harrell FE., Jr Anterior cruciate ligament reconstruction autograft choice: Bone-tendon-bone versus hamstring: Does it really matter? A systematic review. Am J Sports Med. 2004;32:1986–95. doi: 10.1177/0363546504271211. [DOI] [PubMed] [Google Scholar]
- 4.Wilde J, Bedi A, Altchek DW. Revision anterior cruciate ligament reconstruction. Sports Health. 2014;6:504–18. doi: 10.1177/1941738113500910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Joseph C, Pathak SS, Aravinda M, Rajan D. Is ACL reconstruction only for athletes? A study of the incidence of meniscal and cartilage injuries in an ACL-deficient athlete and non-athlete population: An Indian experience. Int Orthop. 2008;32:57–61. doi: 10.1007/s00264-006-0273-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Battaglia MJ, 2nd, Cordasco FA, Hannafin JA, Rodeo SA, O’Brien SJ, Altchek DW, et al. Results of revision anterior cruciate ligament surgery. Am J Sports Med. 2007;35:2057–66. doi: 10.1177/0363546507307391. [DOI] [PubMed] [Google Scholar]
- 7.Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;7:189–98. doi: 10.5435/00124635-199905000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Gifstad T, Drogset JO, Viset A, Grøntvedt T, Hortemo GS. Inferior results after revision ACL reconstructions: A comparison with primary ACL reconstructions. Knee Surg Sports Traumatol Arthrosc. 2013;21:2011–8. doi: 10.1007/s00167-012-2336-4. [DOI] [PubMed] [Google Scholar]
- 9.Noyes FR, Barber-Westin SD. Revision anterior cruciate surgery with use of bone-patellar tendon-bone autogenous grafts. J Bone Joint Surg Am. 2001;83-A:1131–43. doi: 10.2106/00004623-200108000-00001. [DOI] [PubMed] [Google Scholar]
- 10.O’Neill DB. Revision arthroscopically assisted anterior cruciate ligament reconstruction with previously unharvested ipsilateral autografts. Am J Sports Med. 2004;32:1833–41. doi: 10.1177/0363546504264585. [DOI] [PubMed] [Google Scholar]
- 11.Wright RW, Gill CS, Chen L, Brophy RH, Matava MJ, Smith MV, et al. Outcome of revision anterior cruciate ligament reconstruction: A systematic review. J Bone Joint Surg Am. 2012;94:531–6. doi: 10.2106/JBJS.K.00733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wright RW, Magnussen RA, Dunn WR, Spindler KP. Ipsilateral graft and contralateral ACL rupture at five years or more following ACL reconstruction: A systematic review. J Bone Joint Surg Am. 2011;93:1159–65. doi: 10.2106/JBJS.J.00898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Grossman MG, ElAttrache NS, Shields CL, Glousman RE. Revision anterior cruciate ligament reconstruction: Three- to nine-year followup. Arthroscopy. 2005;21:418–23. doi: 10.1016/j.arthro.2004.12.009. [DOI] [PubMed] [Google Scholar]
- 14.Salmon LJ, Pinczewski LA, Russell VJ, Refshauge K. Revision anterior cruciate ligament reconstruction with hamstring tendon autograft: 5- to 9-year followup. Am J Sports Med. 2006;34:1604–14. doi: 10.1177/0363546506288015. [DOI] [PubMed] [Google Scholar]
- 15.Anand BS, Feller JA, Richmond AK, Webster KE. Return-to-sport outcomes after revision anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2016;44:580–4. doi: 10.1177/0363546515618381. [DOI] [PubMed] [Google Scholar]
- 16.Andriolo L, Filardo G, Kon E, Ricci M, Della Villa F, Della Villa S, et al. Revision anterior cruciate ligament reconstruction: Clinical outcome and evidence for return to sport. Knee Surg Sports Traumatol Arthrosc. 2015;23:2825–45. doi: 10.1007/s00167-015-3702-9. [DOI] [PubMed] [Google Scholar]
- 17.Grassi A, Zaffagnini S, Marcheggiani Muccioli GM, Neri MP, Della Villa S, Marcacci M. After revision anterior cruciate ligament reconstruction, who returns to sport? A systematic review and meta-analysis. Br J Sports Med. 2015;49:1295–304. doi: 10.1136/bjsports-2014-094089. [DOI] [PubMed] [Google Scholar]
- 18.Shelbourne KD, Benner RW, Gray T. Return to sports and subsequent injury rates after revision anterior cruciate ligament reconstruction with patellar tendon autograft. Am J Sports Med. 2014;42:1395–400. doi: 10.1177/0363546514524921. [DOI] [PubMed] [Google Scholar]
- 19.Johnson DL, Fu FH. Anterior cruciate ligament reconstruction: Why do failures occur? Instr Course Lect. 1995;44:391–406. [PubMed] [Google Scholar]
- 20.Garofalo R, Djahangiri A, Siegrist O. Revision anterior cruciate ligament reconstruction with quadriceps tendon-patellar bone autograft. Arthroscopy. 2006;22:205–14. doi: 10.1016/j.arthro.2005.08.045. [DOI] [PubMed] [Google Scholar]
- 21.Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997;10:14–21. [PubMed] [Google Scholar]
- 22.Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: A prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7:138–45. doi: 10.1007/s001670050138. [DOI] [PubMed] [Google Scholar]
- 23.Weber AE, Delos D, Oltean HN, Vadasdi K, Cavanaugh J, Potter HG, et al. Tibial and femoral tunnel changes after ACL reconstruction: A Prospective 2-year longitudinal MRI study. Am J Sports Med. 2015;43:1147–56. doi: 10.1177/0363546515570461. [DOI] [PubMed] [Google Scholar]
- 24.IKDC (International knee Documentation Committee) [Last visited on 2018 Jul 01]. Available from: http://www.orthopaedicscore.com/scorepages/international_knee_documentation_comitee.html .
- 25.Briggs KK, Lysholm J, Tegner Y, Rodkey WG, Kocher MS, Steadman JR. The reliability, validity, and responsiveness of the Lysholm score and Tegner activity scale for anterior cruciate ligament injuries of the knee: 25 years later. Am J Sports Med. 2009;37:890–7. doi: 10.1177/0363546508330143. [DOI] [PubMed] [Google Scholar]
- 26.Johnson WR, Makani A, Wall AJ, Hosseini A, Hampilos P, Li G, et al. Patient outcomes and predictors of success after revision anterior cruciate ligament reconstruction. Orthop J Sports Med. 2015;3:2325967115611660. doi: 10.1177/2325967115611660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ahn JH, Lee YS, Ha HC. Comparison of revision surgery with primary anterior cruciate ligament reconstruction and outcome of revision surgery between different graft materials. Am J Sports Med. 2008;36:1889–95. doi: 10.1177/0363546508317124. [DOI] [PubMed] [Google Scholar]
- 28.Kamath GV, Redfern JC, Greis PE, Burks RT. Revision anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39:199–217. doi: 10.1177/0363546510370929. [DOI] [PubMed] [Google Scholar]
- 29.Mahmoud SS, Odak S, Coogan S, McNicholas MJ. A prospective study to assess the outcomes of revision anterior cruciate ligament reconstruction. Int Orthop. 2014;38:1489–94. doi: 10.1007/s00264-014-2324-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Brambilla L, Pulici L, Carimati G, Quaglia A, Prospero E, Bait C, et al. Prevalence of associated lesions in anterior cruciate ligament reconstruction: Correlation with surgical timing and with patient age, sex, and body mass index. Am J Sports Med. 2015;43:2966–73. doi: 10.1177/0363546515608483. [DOI] [PubMed] [Google Scholar]
- 31.Griffith TB, Allen BJ, Levy BA, Stuart MJ, Dahm DL. Outcomes of repeat revision anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41:1296–301. doi: 10.1177/0363546513482568. [DOI] [PubMed] [Google Scholar]
- 32.Gupta R, Masih GD, Chander G, Bachhal V. Delay in surgery predisposes to meniscal and chondral injuries in anterior cruciate ligament deficient knees. Indian J Orthop. 2016;50:492–8. doi: 10.4103/0019-5413.189606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Michalitsis S, Vlychou M, Malizos KN, Thriskos P, Hantes ME. Meniscal and articular cartilage lesions in the anterior cruciate ligament-deficient knee: Correlation between time from injury and knee scores. Knee Surg Sports Traumatol Arthrosc. 2015;23:232–9. doi: 10.1007/s00167-013-2497-9. [DOI] [PubMed] [Google Scholar]