

Abstract
Cerebral palsy (CP), a heterogeneous disorder of movement and posture, is one of the most important causes of disability affecting children. With a wide variability in the clinical presentation and a paucity of reliable diagnostic tests, decision-making in CP is fraught with difficulties and challenges. The plethora of musculoskeletal manifestations includes poor muscle function, spasticity, rigidity, muscle weakness, poor selective motor control, soft-tissue and joint contractures, torsional malalignments, and lever arm dysfunctions. Children with CP are at a high risk of further worsening and progression of these musculoskeletal abnormalities with the natural course of the disease. A comprehensive assessment that includes a combination of detailed medical history, functional assessment, clinical examination, analysis of gait, and radiological assessment is required to provide a favorable treatment outcome in these children. A close surveillance is essential so as to identify risk factors for the development and progression of musculoskeletal problems so that early interventions can be carried out to circumvent them. This review article is to highlight the importance of clinical examination in the assessment of children with CP.
Keywords: Cerebral palsy, clinical examination, gait analysis
Introduction
Cerebral palsy (CP) is defined as a qualitative motor disorder of movement and posture appearing before the age of 3 years, due to non-progressive damage of the brain, occurring before growth of the nervous system is complete.1 The effect of the nonprogressive damage may however contribute to a misunderstanding of the secondary musculoskeletal pathology, which is not static but is most definitely progressive.2 The presentation of patients with CP is highly variable, ranging from those with mild neurological deficit to those with severe involvement. The diagnostic matrix to be followed in case of CP includes a detailed history, gait analysis, physical examination of lower limbs, examination of upper extremities and spine, and additional tests for appropriate clinical evaluation. The above diagnostic matrix is an important pillar for decision-making in CP [Figure 1].
Figure 1.
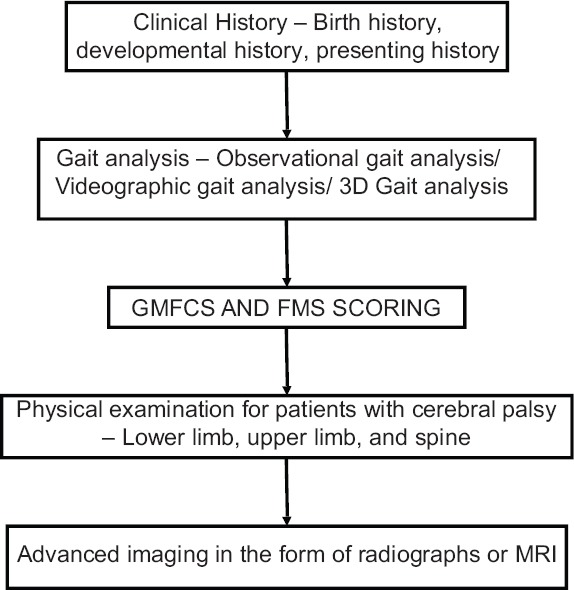
Diagnostic flowchart in cerebral palsy
Search criteria
The authors identified the relevant articles using a protocol based on searching Cochrane Database of Systematic Reviews (1993–2017; www.cochrane.org); Google Scholar; MEDLINE (1956–2016); and PubMed. Searches were also supplemented by hand searching. Interventions and keywords for investigation were identified using (1) contributing authors’ knowledge of the field; (2) internationally recognized CP websites such as the American Academy of Cerebral Palsy and Developmental Medicine (www.aacpdm.org); and (3) the top twenty hits in Google using the search terms “cerebral palsy” and “Clinical Examination” as an indicator of popular subject matter. The full search strategy is available from the authors on request.
History
The most important aspect in the initial clinical evaluation of a child with CP is the medical and surgical history of the child. The history includes information regarding the birth, developmental milestones, other associated medical problems, surgical history, ongoing medications, and physiotherapy treatment.
The birth history includes important details about antenatal problems, perinatal history including whether child was preterm, full term, or post-term, and whether there were other associated factors leading to hypoxic injury to the brain such as prolonged labor, meconium aspiration. etc. Treatment of a child in the neonatal Intensive Care Unit after delivery is an important pointer in history. An immature or preterm infant with periventricular leukomalacia typically presents with spastic diplegia, whereas a child with periventricular hemorrhage is more likely to present with hemiplegia.3 A full-term child with watershed ischemia may present with quadriparesis and that with focal ischemia may present with hemiparesis.
History of developmental milestones is important, as it signifies the stages of physical development as the child becomes more mature. The current functional activity level of the child provides a good insight for treatment, future prognosis, capacity, and goal setting. The earlier the child attains standing balance, the better is the outcome with respect to hip deformities. It is also important to acquire previous history of associated medical illness, physiotherapy records, and previous surgical records to accurately assess present deformities and compensations. Present functional ability at home, school, and in community as well as other functional skills such as walking, running, and stair climbing also affect treatment plans and outcome analysis.
Clinical Examination
Physical examination, especially in children with CP, has limitations and benefits. The information collected during physical examination is based on static responses, whereas functional activities, such as walking, are dynamic. The independence of gait analysis and physical examination measures supports the notion that each provides information that is important in the delineation of problems of children with CP.4 The method of assessment, the skill of the examiner, and the participation of the child can all affect the usefulness of the examination.
Gait analysis
Gait analysis is commonly ignored in the examination of children with CP and is sometimes performed last in the examination sequence. However, gait analysis is most important as it indicates relative functional deviations rather than static physical examination. The first and most important part in the examination of a child with CP is observing the gait when the child walks into the consultation room. Gait analysis can be done with different techniques such as observational gait analysis, videographic gait analysis, and instrumented 3D gait analysis.5,6,7 Observational gait analysis is performed by observing the gait cycle in both sagittal and coronal planes and observing joint angles at different stages of gait cycle at different levels. Videographic gait analysis is performed by observing gait in slow-motion video and analyzing the movements of different joints in both coronal and sagittal planes. The most comprehensive gait analysis is performed by instrumented 3D gait analysis with the use of reflective markers in a gait laboratory. However, 3D gait analysis requires a setup with a lot of infrastructure expenditure, and often sufficient findings can be obtained by observation and slow-motion videographic gait analysis on a day-to-day basis.
Gait patterns in cerebral palsy
Depending on the involvement of spasticity or contracture of different muscles, there are different patterns of gait observed in children with CP. Gait pattern variations related to topographical type of CP are best seen in contrast between unilateral spastic CP and bilateral spastic CP.8
In spastic hemiplegia, there is more involvement distally and therefore true equinus is the basis of common patterns. Winters et al. described four gait patterns in spastic hemiplegics based on sagittal kinematics.9
Type 1 hemiplegia gait – Drop foot type
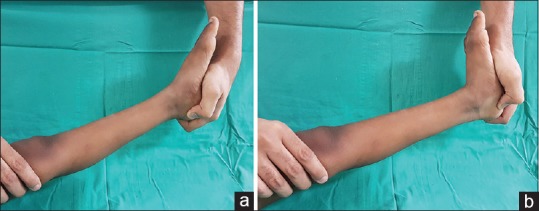
Type 2 hemiplegia gait – True equinus with or without recurvatum knee [Figure 2a and b]
Type 3 hemiplegia gait – Stiff knee gait
Type 4 hemiplegia gait – In sagittal plane, the ankle is in equinus, knee in flexion, hip in flexion and anterior pelvic tilt is present. In coronal plane, there is hip adduction and internal rotation.
Figure 2.

Type II hemiplegic gait. (a): Anteroposterior view showing right-sided hemiplegia with ankle equinus in stance. (b): Lateral view showing right-sided hemiplegia with ankle equinus in stance
Gait patterns in spastic diplegia
In spastic diplegia, there is more proximal involvement and therefore apparent equinus and crouch gait are seen commonly.10 There are four common patterns of gait in spastic diplegia as described by Rodda et al.11
Type 1 – True equinus
Type 3 – Apparent equinus
Figure 3.

Type II diplegic gait. (a): Anteroposterior view showing jump gait with bilateral hip and knee flexion and ankle equinus. (b): Lateral view showing jump gait with bilateral hip and knee flexion and ankle equinus
Figure 4.

Type IV diplegic gait. (a): Anteroposterior view showing crouch gait with bilateral hip and knee flexion and ankle dorsiflexion. (b): Lateral view showing crouch gait with bilateral hip and knee flexion and ankle dorsiflexion
Physical Assessment
A standard, detailed physical examination is crucial in assessing children with movement disorders, especially CP. The four primary reasons for the need to classify CP include (1) to provide a detailed description that can delineate the nature of the problem and its severity, (2) to provide predictions of both current and future service needs for an individual, (3) to provide comparison so that groups of patients with CP at one institution can be compared with those at another, and (4) to evaluate change so that one individual with CP can be evaluated at various times and change can be documented.12
In CP, the Gross Motor Function Classification System, developed by Palisano et al.,13 has been in use for over two decades. It is a five-level clinical classification system that describes the gross motor function of people with CP on the basis of self-initiated movement abilities. The purpose of this system is to classify the child's present gross motor function in a systematic and reliable manner and serves as a useful matrix for identification of where a child is at a specific point in time in relation to its age and gross motor function. Distinctions between levels are based on functional abilities; the need for walkers, crutches, wheelchairs, or canes/walking sticks; and to a much lesser extent, the actual quality of movement. The various levels that are described include:
Level I – The child can walk indoors and outdoors and climb stairs without using hands for support and can perform usual activities such as running and jumping but has decreased speed, balance, and coordination
Level II – The child can climb stairs with a railing but has difficulty with uneven surfaces, inclines, or in crowds and has minimal ability to run or jump
Level III – The child walks with assistive mobility devices indoors and outdoors on level surfaces, able to climb stairs using a railing, and may propel a manual wheelchair but needs assistance for long distances or uneven surfaces
Level IV – Here, the walking ability is severely limited even with assistive devices such as wheelchairs most of the time and may propel own power wheelchair, standing transfers, with or without assistance
Level V – The child has physical impairments that restrict voluntary control of movements, has very poor head, neck, and trunk control, has impairment in all areas of motor function, and cannot sit or stand independently, even with adaptive equipment.
The physical examination itself can be categorized into the following:
Functional mobility assessment
Over the years, various simple categorical scales have been developed for the assessment of functional ability and functional mobility of children with CP. These scales were designed to be responsive to change and can be used to document the serial attainment of mobility and functional abilities, the deterioration or improvement in these skills after intervention, or other changes consequent on growth and development. The Functional Mobility Scale (FMS) had been described by Graham et al.14 to classify the extent of mobility in children, taking into account the range of assistive devices a child might use for mobility. The scale is useful in documenting change over time following interventions such as orthopedic surgery or selective dorsal rhizotomy and was found to be highly sensitive to detect changes after operative intervention.15
The FMS rates walking ability at three specific distances such as 5, 50, and 500 m and is further graded from 1 to 6 depending on the level of mobility. The scoring represents the child's mobility in the home, at school, and in the community setting. The walking ability of the child is rated at each of the three distances according to the need for assistive devices such as crutches, walkers, or wheelchairs.
The rating is from 1 to 6 which is described as follows:
1 – The child mostly uses a wheelchair but may stand for transfers and does some stepping supported by a caretaker or with the help of a walker; 2 – The child uses a walker or frame to ambulate; 3 – The child independently walks but with the help of crutches; 4 – The child walks independently but with the help of sticks (one or two); 5 – The child walks independently only on leveled surfaces; 6 – The child walks independently on all surfaces; C – The child crawls for mobility at home (5 m); N – Not applicable (e.g., the child does not complete 500 m).
Children with CP, despite having a similar diagnosis, vary in their abilities and level of functioning within and across different environmental contexts such as home, school, or a community setting.16 Capacity (what a child can do in standardized, controlled environment) may or may not be the same as performance (what a child actually does in his/her daily environment). The FMS is a performance measure and it is important to rate what the child actually does at the time of assessment and not what they can do or used to be able to do. The FMS has been found to be a reliable tool that can be used by clinicians to assess mobility in children with CP.17
Muscle tone assessment
Tone can be defined as resistance to passive stretch at the relaxed state of muscle activity. It is difficult and cumbersome to assess the tone in CP children, as this can be influenced by apprehension and excitement in the child and the position in which the child is assessed. Hypertonia in a CP child can be due to spasticity, dystonia, rigidity, or a combination of the above features. First, the muscle contracture at rest is assessed by manual palpation of the muscle in testing. Second, the limb is moved slowly through its passive range and later at various speeds or velocity and catch or the resistance to passive motion is assessed. The spasticity assessment is commonly done using the Modified Ashworth scale18,19,20 and the Tardieu scale.21
Modified Ashworth scale
The Modified Ashworth scale, which is used to grade the amount of spasticity, is one of the commonly performed tests as it does not need any equipment and can be performed quickly, easily, and in a day-care clinic. The test is performed manually to determine the resistance of muscle to passive stretching. This was initially described as a measure of spasticity but depends on the speed at which the test is performed. In the original article, it was suggested that the movement of the limb segments should be performed through the full range of movement enough to be a test of spasticity during walking [Table 1].
Table 1.
Modified Ashworth scale
| Grading | Description |
|---|---|
| 0 | No increase in muscle tone |
| 1 | Slight increase in muscle tone, manifested by a catch and release or by minimal resistance at the end of the ROM |
| 1+ | Slight increase in muscle tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM |
| 2 | More marked increase in muscle tone through most of the ROM, but affected part(s) can be easily moved |
| 3 | Considerable increase in muscle tone, passive movement difficult |
| 4 | Affected part(s) are rigid in flexion or extension |
ROM=Range of motion
Due to the potential shortcomings of this test regarding reliability and chances of error in measurements, assessments of spasticity using this scale should be interpreted with caution.19,20
Tardieu scale
This is a scale for measuring spasticity that takes into account the resistance to passive movement at both slow and fast speeds. As this test is simple and relatively easy to perform and recorded as an angle measure, it can be easily correlated with gait analysis, if required. The various parameters include the following:
V1 – Velocity to stretch as slow as possible
V2 – Velocity to stretch with the speed of limb segment falling with gravity
V3 – Velocity to stretch as fast as possible (> natural drop)
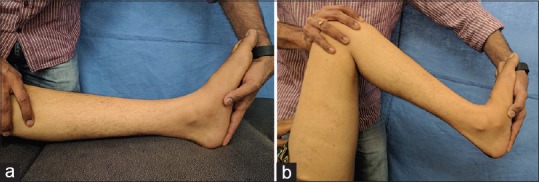
R1 – Angle of catch seen at velocity V2 or V3 [Figure 5a]
R2 – Full range of motion (ROM) achieved when muscle is at rest and tested at V1 velocity [Figure 5b].
Figure 5.
Tardieu scale. (a): Clinical photograph showing Tardieu score at the ankle (R1). (b): Clinical photograph showing Tardieu score at the ankle (R2)
A large difference between R1 and R2 in outer and middle ROM indicates a larger dynamic component and a small difference between R1 and R2 in middle and inner ROM indicates a predominant fixed contracture.
The Tardieu scale has an excellent intra- and inter-rater reliability when assessed at the elbow and ankle joints of children with CP, with no difference noted between visual and goniometric measurements.22 Training is associated with a highly significant improvement in reliability.
Although we use these scales routinely during the assessment of the CP children, they have some disadvantages because they are not standardized, stimulus is not well controlled, and they lack reliability and validity for all the muscle groups. They offer only qualitative and subjective information in measuring spasticity.23
Analysis of range of motion and joint contractures
Assessing the muscle length and joint contractures is an integral part of the physical examination.24 The muscle length is indirectly measured by assessing the ROM of the joint through which the muscle acts. These have to be undertaken with appropriate precautions and standardization, as abnormally false results and errors commonly arise due to faulty technique of examination. Reliability studies suggest that the standard error of measurement of passive joint range is of the order of 5°.25 Although it is difficult to differentiate static and dynamic deformities in nonanesthetized child, a comprehensive static examination gives a good insight on the type of contracture and in planning the management of the same.26
Hip joint
Hip deformity is one of the common presenting abnormalities in CP. Although the hips per se are normal at birth, late displacements occur due to abnormal balance, loss of selective motor control, and tone abnormalities. Thus, hip screening is an essential part of examination of a CP child,27 especially in non-walkers and late walkers. The components of hip examination include the following:
Thomas’ hip flexion test [Figure 6] is commonly used for measuring hip flexion contracture.28 The test is performed with the patient in supine position and the uninvolved limb is adequately flexed to eliminate exaggerated lumbar lordosis. The angle formed between the horizontal axis of the thigh and horizontal line parallel to the floor measures the hip flexion contracture. The reliability and repeatability of the test was reported by Kilgour and McWhirk et al.29,30
Staheli described a prone extension test [Figure 7] to assess hip flexion contracture, especially for children with CP and in bilateral hip pathologies.31 It is performed with the patient prone on the edge of the couch, one hand of the examiner to stabilize the pelvis and the other extends the thigh while observing the lumbar lordosis. The point at which the pelvis rises indicates the end point and the angle between the long axis of thigh and the horizontal line measures the flexion contracture.
Figure 6.

Clinical photograph showing measurement of hip flexion deformity by the Thomas test
Figure 7.

Clinical photograph showing Staheli prone extension test
On comparing the above tests, the Thomas’ test showed the best results in normal population whereas the Staheli's test was shown to have accurate results in children with CP.32
The next part of assessment is to measure the amount of adductor contracture. With the patient in supine position, passive abduction of the hip is performed with the knee in extension and with the knee in 90° flexion (Phelp's Test) [Figure 8a and b]. If abduction improves on knee flexion, the primary pathology lies in the medial hamstring muscles and gracilis. If both the measurements are the same, the prime pathology is in the adductor muscles.
Figure 8.
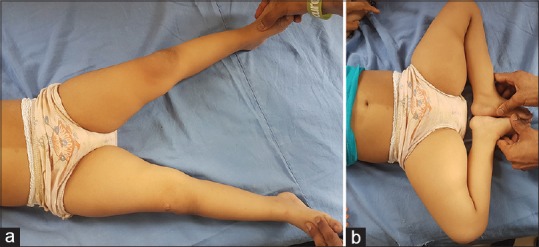
Phelp's test. (a): Clinical photograph showing passive hip abduction with knees in extension. (b): Clinical photograph showing improved hip abduction with knee flexion
It has been proposed that, with a significant hip flexion contracture in combination with combined hip abduction of <80°, there is an increased risk of hip subluxation and chronic hip pain in the near future.33
Knee joint
The commonly presenting deformity in knee is that of flexion contracture, which is more pronounced in a nonambulatory child. The first step in assessment is to differentiate true joint contracture from contracture due to muscle spasticity or tightness.
Joint contracture – With the hip in extension and ankle in gravity-assisted plantar flexion, the residual knee flexion measures true joint contracture [Figure 9]
Muscle (hamstrings) contracture – Also called popliteal angle test, it is performed with the hip joint in 90° of flexion in supine position, the residual knee flexion shows the amount of muscle tightness or contracture. In a unilateral popliteal angle [Figure 10a], the tested leg is kept in 90-90 position of knee and hip with the other limb extended, the knee of the tested limb is extended until resistance and further loss of knee extension is measured. In a bilateral popliteal angle test [Figure 10b], both the limbs are kept in 90-90 position of hip and knee joints, and the popliteal angle is measured one by one with the other limb in identical position. Hamstring shift measures the difference between unilateral and bilateral popliteal angles and gives a direct measure of hip flexion contracture or anterior pelvic tilt.34,35 The bilateral popliteal angle test is more reliable for assessing the hamstring tightness than its unilateral counterpart, as the latter test gives false high values if there is an associated psoas muscle contracture.
Figure 9.

Clinical photograph showing knee flexion deformity
Figure 10.
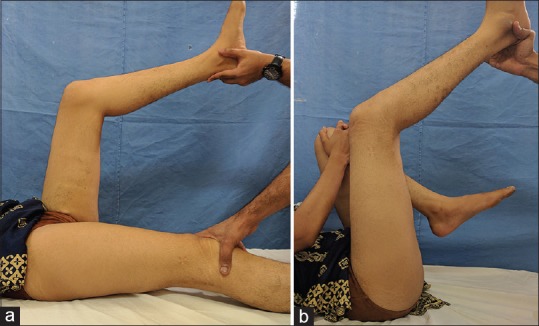
Popliteal angle test for hamstring contracture. (a): Clinical photograph showing unilateral popliteal angle. (b): Clinical photograph showing bilateral popliteal angle. Difference between the two measurements is the “hamstring shift”
In ambulatory children, a crouch gait develops as a part of the natural course of the disease, especially in diplegic children, in which there is a failure of plantar flexion–knee extension couple.36 While contemplating crouch correction, other abnormalities such as lever arm dysfunction due to torsional malalignments, planovalgus feet, and muscle imbalance have to be kept in mind to provide overall improvement in the outcome.37
Assessment of rectus femoris spasticity using Duncan-Ely's/Prone Rectus test [Figure 11] is essential, as this in conjunction with hamstring contracture can result in a stiff knee gait pattern, which necessitates a different approach to management.
Figure 11.

Clinical photograph showing prone rectus test. Note the pelvic rise on knee flexion indicating spasticity of the rectus femoris
Ankle and foot
The most common deformities seen in CP include equino-varus and plano-valgus. Assessment of equinus (gastro-soleus spasticity/contracture) is done by passive dorsiflexion of ankle with knee in extension and then with knee joint in 90° flexion (Silverskiold test) [Figure 12a and b]. A difference of 20°–30° shows a spastic gastrocnemius component.
Figure 12.
Silverskiold test. (a): Clinical photograph showing degree of ankle equinus with knee in extension. (b): Clinical photograph showing correction of ankle equinus with knee flexion indicating predominantly gastrocnemius contracture
Muscle strength analysis and selective motor control
Assessment of muscle strength and selective motor control is an integral part of the examination protocol of children with CP. As muscle strength is directly proportional to motor function, strength evaluation is necessary for providing optimal functional outcomes. Muscle strength analysis is also required to assess the appropriateness for surgical interventions.
The Medical Research Council (MRC) grading for muscle strength assessment has been in use for decades.38 The main disadvantage of this grading system is that it neither considers the ROM for which a movement can be performed nor defines the strength of resistance against which a movement can be performed. The MRC grading system consists of six grades (scale of 0–5) in relation to the maximum range expected for that muscle [Table 2].
Table 2.
Medical Research Council grading of muscle power
| Grade | Description |
|---|---|
| 0 | Complete paralysis |
| 1 | Flicker of contraction present |
| 2 | Movement possible if gravity eliminated |
| 3 | Movement against gravity but not against resistance |
| 4 | Movement possible against resistance but less than normal power |
| 5 | Normal power |
In children with CP, who have poor comprehension and in whom isolated muscle testing is cumbersome, manual muscle testing using Kendall scale is used.39 It is a 10-point scale which provides a simpler way to assess muscle strength or muscle imbalance [Table 3]. However, it relies heavily on the examiner's judgment and experience, the amount of force generated, and the accuracy of patient positioning. It is subjective and prone to have a significant examiner bias. Studies have shown that clinically small but significant differences in strength may not be detected by this method. However, under strict evaluation protocols, this method was still found to be useful.40 For children who are under the age of 5, and who cannot follow complex directions for maximal force production, the manual muscle testing method, as well as any other method of strength assessment, is still a vague screening tool. In recent studies, use of a handheld dynamometer has been shown to provide more reliable results in assessing muscle strength, especially the isometric strength.41
Table 3.
Kendall Scale
| Grade | Description |
|---|---|
| 10 | Holds test position against strong pressure |
| 9 | Holds test position against moderate-to-strong pressure |
| 8 | Holds test position against moderate pressure |
| 7 | Holds test position against slight-to-moderate pressure |
| 6 | Holds test position against slight pressure |
| 5 | Holds test position (no pressure) |
| 4 | Gradual release from test position |
| 3 | Holds against resistance through full ROM with gravity eliminated or <100% ROM with against gravity |
| 2 | Moves through full ROM with gravity eliminated |
| 1 | Moves through <100% ROM with gravity eliminated |
| T | Visible or palpable muscle contraction |
| 0 | No muscle contraction possible |
ROM=Range of motion
Selective motor control
In children with CP, the reduced ability to control and isolate movements provides great hindrance in muscle strength assessment. The typical scale for muscle group selectivity is given as follows:
Grade 0 – No ability/only patterned movement observed
Grade 1 – Partial ability/partially isolated movements
Grade 2 – Complete ability/completely isolated movements.
To assess the overactivity of tibialis anterior muscle (varus/supination), confusion test is used. Here, due to loss of selective motor control, resistance to hip flexion causes the overactive tibialis anterior muscle to act and there is dorsiflexion at the ankle and forefoot supination.
Recently, a newer assessment scheme has been put forth, the Selective Control Assessment of Lower Extremities, which gives a comprehensive scheme for the motor function assessment.42
Torsional profile and concept of lever arm dysfunction
“Lever arm dysfunction” is a term originally coined by Gage in 199143 to describe the particular orthopedic deformities that arise in an ambulatory child with CP. Lever arm dysfunction describes a general class of bone modeling, remodeling, and or traumatic deformities that include hip subluxation, torsional deformities of long bones, and/or foot deformities. Since muscles and ground reaction forces (GRFs) must act on skeletal levers to produce locomotion, abnormalities of these lever arm systems greatly interfere with the child's ability to walk.
In CP, the muscles and the GRFs are neither appropriate nor adequate because of contractures, poor selective motor control, and abnormality of the bony lever arms due to bony malalignments. Among the malalignments, excessive femoral anteversion (FAV) and tibial torsion are the two commonly described conditions in literature.44 Excessive FAV and coxavalga can produce intoeing gait and hip instability.45
The Craig's test/Trochanteric prominence test [Figure 13] has been used for the assessment of FAV. With the patient in prone position and knee at 90° flexion, the angle between the vertical line and long axis of the leg at the greatest prominence of the greater trochanter palpated laterally measures the amount of FAV. In recent studies, it has been found that trochanteric prominence test in combination with hip internal rotation X-rays is a better predictor of FAV and neck-shaft angle as compared with computed tomography.46
Figure 13.

Clinical photograph showing Craig test to measure femoral anteversion
Tibial torsion malalignment can be assessed clinically by the following:
Thigh foot angle [Figure 14] – With the patient in prone position, knee in 90° flexion, and neutral ankle and hind foot position, the angle between the thigh axis and foot axis (axis between the 2nd and 3rd metatarsals) gives tibial torsional measurement
Bi-malleolar axis method – With the knee in full extension, the leg is rotated to align the femur bi-condylar axis horizontally. The angle between the horizontal and bimalleolar axis measures the tibial torsion47
Second toe test – With the patient in prone position, the leg is rotated so that the 2nd toe points vertically down. Now with the thigh held and knee flexed, the angle between the vertical line and the leg axis gives the measure of tibial torsion.
Figure 14.

Clinical photograph showing Thigh Foot Angle test to measure tibial torsion
Standing balance and equilibrium
To conclude the physical examination, assessment of posture, trunk balance, and position of the pelvis and lower extremities in standing position (static) and during walking (dynamic) in both planes gives overall information regarding motor control and compensatory mechanisms. Children with CP tend to have delayed and reduced posterior equilibrium responses. A comprehensive analysis of equilibrium in all planes should be done before planning for any modality of treatment.
Upper-limb Examination
The upper extremity examination includes an assessment of tone, ROM of joints, strength of muscles, and assessment of upper-limb functions. Assessment of tone is by the Ashworth scale similar to that for lower extremity muscles. ROM is assessed at each of the joints at shoulder, elbow, forearm, wrist, and hand.
Assessment of upper-limb function
The Manual Ability Classification System describes how children with CP use their hands to manipulate relevant and appropriate objects for activity of daily living, classifying them into five levels48 [Table 4]. Other assessment scales for upper-limb evaluation are Assisting Hand Assessment score, Quality of Upper Extremity Skills Test (QUEST), Melbourne Assessment of Unilateral Upper limb Function, and Shriners Hospital Upper Extremity Evaluation.
Table 4.
Manual Ability Classification System scoring system
| Level of ability | Description |
|---|---|
| Level I | Handles objects easily and successfully. Atmost, limitations in the ease of performing manual tasks requiring speed and accuracy |
| Level II | Handles most objects but with somewhat reduced quality and/or speed of achievement. May avoid some tasks or use alternative ways of performance |
| Level III | Handles objects with difficulty; needs help to prepare and/or modify activities |
| Level IV | Handles a limited selection of easily managed objects in adapted situations. Requires continuous support |
| Level V | Does not handle objects and has severely limited ability to perform even simple actions. Requires total assistance |
Spine Examination
Spine deformities are a common presentation in CP. They present in varied patterns – scoliosis, kyphosis, lordosis, pelvic obliquity, and a combination of these. Scoliosis is the most common spinal deformity in patients with CP.49 The incidence of scoliosis increases with increasing severity of the disease. The classic curve pattern is a long C-shaped curve that is often kyphoscoliotic or lordoscoliotic. The curve progression is gradual; however, it can become rapid with onset of puberty, deteriorating neurological function, or spending prolonged time in wheelchair. Scoliosis developing at a younger age (<15 years of age) has a higher risk for progression, and progression can be seen even after skeletal maturity in severely affected children.50 Nonoperative management of spinal deformity can be achieved by sitting modifications and bracing. However, nonoperative management does not halt the progression of deformity. Surgical management depends on factors such as patient's age, functional capabilities, curve pattern, and other comorbidities.
Conclusions
A detailed bi-annual examination of all children with CP is essential. The frequency of examinations should be more if the child is nonambulant, has deterioration on subsequent examination, or undergoes any surgical management. Although strict guidelines have not been established for a streamlined physical assessment of children with CP, a comprehensive clinical examination using the described diagnostic matrix should be undertaken by every clinician before contemplating the management of these children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.MacKeith RC, Polani PE. Cerebral palsy. Lancet. 1958;1:61. [Google Scholar]
- 2.Boyd RN, Graham HK. Botulinum toxin A in the management of children with cerebral palsy-indications and outcome. Eur J Neurol. 1997;4:15–22. [Google Scholar]
- 3.Volpe JJ. Neurology of the Newborn. 5th ed. Philadelphia: Elsevier; 2008. [Google Scholar]
- 4.Desloovere K, Molenaers G, Feys H, Huenaerts C, Callewaert B, Van de Walle P, et al. Do dynamic and static clinical measurements correlate with gait analysis parameters in children with cerebral palsy? Gait Posture. 2006;24:302–13. doi: 10.1016/j.gaitpost.2005.10.008. [DOI] [PubMed] [Google Scholar]
- 5.Stuberg WA, Colerick VL, Blanke DJ, Bruce W. Comparison of a clinical gait analysis method using videography and temporal-distance measures with 16-mm cinematography. Phys Ther. 1988;68:1221–5. [PubMed] [Google Scholar]
- 6.Chambers HG, Sutherland DH. A practical guide to gait analysis. J Am Acad Orthop Surg. 2002;10:222–31. doi: 10.5435/00124635-200205000-00009. [DOI] [PubMed] [Google Scholar]
- 7.Krebs DE, Edelstein JE, Fishman S. Reliability of observational kinematic gait analysis. Phys Ther. 1985;65:1027–33. doi: 10.1093/ptj/65.7.1027. [DOI] [PubMed] [Google Scholar]
- 8.Rodda J, Graham HK. Classification of gait patterns in spastic hemiplegia and spastic diplegia: A basis for a management algorithm. Eur J Neurol. 2001;8(Suppl 5):98–108. doi: 10.1046/j.1468-1331.2001.00042.x. [DOI] [PubMed] [Google Scholar]
- 9.Winters TF, Jr, Gage JR, Hicks R. Gait patterns in spastic hemiplegia in children and young adults. J Bone Joint Surg Am. 1987;69:437–41. [PubMed] [Google Scholar]
- 10.Sutherland DH, Davids JR. Common gait abnormalities of the knee in cerebral palsy. Clin Orthop Relat Res. 1993;288:139–47. [PubMed] [Google Scholar]
- 11.Rodda JM, Graham HK, Carson L, Galea MP, Wolfe R. Sagittal gait patterns in spastic diplegia. J Bone Joint Surg Br. 2004;86:251–8. doi: 10.1302/0301-620x.86b2.13878. [DOI] [PubMed] [Google Scholar]
- 12.Bax M, Goldstein M, Rosenbaum P, Leviton A, Paneth N, Dan B, et al. Proposed definition and classification of cerebral palsy, April 2005. Dev Med Child Neurol. 2005;47:571–6. doi: 10.1017/s001216220500112x. [DOI] [PubMed] [Google Scholar]
- 13.Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39:214–23. doi: 10.1111/j.1469-8749.1997.tb07414.x. [DOI] [PubMed] [Google Scholar]
- 14.Graham HK, Harvey A, Rodda J, Nattrass GR, Pirpiris M. The functional mobility scale (FMS) J Pediatr Orthop. 2004;24:514–20. doi: 10.1097/00004694-200409000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Rosenbaum P, Stewart D. The World Health Organization international classification of functioning, disability, and health: A model to guide clinical thinking, practice and research in the field of cerebral palsy. Semin Pediatr Neurol. 2004;11:5–10. doi: 10.1016/j.spen.2004.01.002. [DOI] [PubMed] [Google Scholar]
- 16.Diwan S, Diwan J, Bansal AB, Patel PR. Changes in capacity and performance in mobility across different environmental settings in children with cerebral palsy: An exploratory study. J Clin Diagn Res. 2015;9:YC01–3. doi: 10.7860/JCDR/2015/11639.6399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Harvey AR, Morris ME, Graham HK, Wolfe R, Baker R. Reliability of the functional mobility scale for children with cerebral palsy. Phys Occup Ther Pediatr. 2010;30:139–49. doi: 10.3109/01942630903454930. [DOI] [PubMed] [Google Scholar]
- 18.Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67:206–7. doi: 10.1093/ptj/67.2.206. [DOI] [PubMed] [Google Scholar]
- 19.Gregson JM, Leathley M, Moore AP, Sharma AK, Smith TL, Watkins CL, et al. Reliability of the tone assessment scale and the modified Ashworth scale as clinical tools for assessing poststroke spasticity. Arch Phys Med Rehabil. 1999;80:1013–6. doi: 10.1016/s0003-9993(99)90053-9. [DOI] [PubMed] [Google Scholar]
- 20.Clopton N, Dutton J, Featherston T, Grigsby A, Mobley J, Melvin J, et al. Interrater and intrarater reliability of the modified Ashworth scale in children with hypertonia. Pediatr Phys Ther. 2005;17:268–74. doi: 10.1097/01.pep.0000186509.41238.1a. [DOI] [PubMed] [Google Scholar]
- 21.Haugh AB, Pandyan AD, Johnson GR. A systematic review of the Tardieu scale for the measurement of spasticity. Disabil Rehabil. 2006;28:899–907. doi: 10.1080/09638280500404305. [DOI] [PubMed] [Google Scholar]
- 22.Yam WK, Leung MS. Interrater reliability of modified Ashworth scale and modified Tardieu scale in children with spastic cerebral palsy. J Child Neurol. 2006;21:1031–5. doi: 10.1177/7010.2006.00222. [DOI] [PubMed] [Google Scholar]
- 23.Damiano DL, Quinlivan JM, Owen BF, Payne P, Nelson KC, Abel MF, et al. What does the Ashworth scale really measure and are instrumented measures more valid and precise? Dev Med Child Neurol. 2002;44:112–8. doi: 10.1017/s0012162201001761. [DOI] [PubMed] [Google Scholar]
- 24.Cusick BD, editor. Progressive Casting & Splinting. Tucson (AZ): Therapy Skill Builders; 1990. [Google Scholar]
- 25.McDowell BC, Hewitt V, Nurse A, Weston T, Baker R. The variability of goniometric measurements in ambulatory children with spastic cerebral palsy. Gait Posture. 2000;12:114–21. doi: 10.1016/s0966-6362(00)00068-0. [DOI] [PubMed] [Google Scholar]
- 26.Thomason P, Rodda J, Willoughby K, Graham HK. Orthopaedic assessment in cerebral palsy and clinical practice. In: Dan B, Mayston M, Paneth N, Rosenbloom L, editors. Cerebral Palsy: Science and Clinical Practice. London: Mac Keith Press; 2014. [Google Scholar]
- 27.Dobson F, Boyd RN, Parrott J, Nattrass GR, Graham HK. Hip surveillance in children with cerebral palsy. Impact on the surgical management of spastic hip disease. J Bone Joint Surg Br. 2002;84:720–6. doi: 10.1302/0301-620x.84b5.12398. [DOI] [PubMed] [Google Scholar]
- 28.Thomas HO. Liverpool: Dobb; 1876. Diseases of Hip, Knee, and Ankle Joints, with their Deformities, Treated by New and Efficient Method. [DOI] [PubMed] [Google Scholar]
- 29.Kilgour G, McNair P, Stott NS. Intrarater reliability of lower limb sagittal range-of-motion measures in children with spastic diplegia. Dev Med Child Neurol. 2003;45:391–9. doi: 10.1017/s0012162203000744. [DOI] [PubMed] [Google Scholar]
- 30.McWhirk LB, Glanzman AM. Within-session inter-rater realiability of goniometric measures in patients with spastic cerebral palsy. Pediatr Phys Ther. 2006;18:262–5. doi: 10.1097/01.pep.0000234960.88761.97. [DOI] [PubMed] [Google Scholar]
- 31.Staheli LT. The prone hip extension test: A method of measuring hip flexion deformity. Clin Orthop Relat Res. 1977;123:12–5. [PubMed] [Google Scholar]
- 32.Lee KM, Chung CY, Kwon DG, Han HS, Choi IH, Park MS, et al. Reliability of physical examination in the measurement of hip flexion contracture and correlation with gait parameters in cerebral palsy. J Bone Joint Surg Am. 2011;93:150–8. doi: 10.2106/JBJS.J.00252. [DOI] [PubMed] [Google Scholar]
- 33.Valencia FG. Management of hip deformities in cerebral palsy. Orthop Clin North Am. 2010;41:549–59. doi: 10.1016/j.ocl.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 34.Gage JR, Schwartz MH, Koop SE, Novacheck TF. London: Mac Keith Press; 2009. The Identification and Treatment of Gait Problems in Cerebral Palsy. [Google Scholar]
- 35.Hoffinger SA, Rab GT, Abou-Ghaida H. Hamstrings in cerebral palsy crouch gait. J Pediatr Orthop. 1993;13:722–6. doi: 10.1097/01241398-199311000-00006. [DOI] [PubMed] [Google Scholar]
- 36.Gage JR. Surgical treatment of knee dysfunction in cerebral palsy. Clin Orthop Relat Res. 1990;253:45–54. [PubMed] [Google Scholar]
- 37.Rodda JM, Graham HK, Nattrass GR, Galea MP, Baker R, Wolfe R, et al. Correction of severe crouch gait in patients with spastic diplegia with use of multilevel orthopaedic surgery. J Bone Joint Surg Am. 2006;88:2653–64. doi: 10.2106/JBJS.E.00993. [DOI] [PubMed] [Google Scholar]
- 38.Paternostro-Sluga T, Grim-Stieger M, Posch M, Schuhfried O, Vacariu G, Mittermaier C, et al. Reliability and validity of the medical research council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J Rehabil Med. 2008;40:665–71. doi: 10.2340/16501977-0235. [DOI] [PubMed] [Google Scholar]
- 39.Kendall HO, Kendall FP, Wadsworth GE, editors. 2nd ed. London: Williams and Wilkins; 1971. Muscle Testing and Function. [Google Scholar]
- 40.Wadsworth CT, Krishnan R, Sear M, Harrold J, Nielsen DH. Intrarater reliability of manual muscle testing and hand-held dynametric muscle testing. Phys Ther. 1987;67:1342–7. doi: 10.1093/ptj/67.9.1342. [DOI] [PubMed] [Google Scholar]
- 41.Berry ET, Giuliani CA, Damiano DL. Intrasession and intersession reliability of handheld dynamometry in children with cerebral palsy. Pediatr Phys Ther. 2004;16:191–8. doi: 10.1097/01.PEP.0000145932.21460.61. [DOI] [PubMed] [Google Scholar]
- 42.Fowler EG, Staudt LA, Greenberg MB, Oppenheim WL. Selective control assessment of the lower extremity (SCALE): Development, validation, and interrater reliability of a clinical tool for patients with cerebral palsy. Dev Med Child Neurol. 2009;51:607–14. doi: 10.1111/j.1469-8749.2008.03186.x. [DOI] [PubMed] [Google Scholar]
- 43.Gage JR. London: Mac Keith Press; 1991. Gait Analysis in Cerebral Palsy. [Google Scholar]
- 44.Laplaza FJ, Root L, Tassanawipas A, Glasser DB. Femoral torsion and neck-shaft angles in cerebral palsy. J Pediatr Orthop. 1993;13:192–9. [PubMed] [Google Scholar]
- 45.Bobroff ED, Chambers HG, Sartoris DJ, Wyatt MP, Sutherland DH. Femoral anteversion and neck-shaft angle in children with cerebral palsy. Clin Orthop Relat Res. 1999;364:194–204. doi: 10.1097/00003086-199907000-00025. [DOI] [PubMed] [Google Scholar]
- 46.Chung CY, Lee KM, Park MS, Lee SH, Choi IH, Cho TJ, et al. Validity and reliability of measuring femoral anteversion and neck-shaft angle in patients with cerebral palsy. J Bone Joint Surg Am. 2010;92:1195–205. doi: 10.2106/JBJS.I.00688. [DOI] [PubMed] [Google Scholar]
- 47.Schwartz MH, Rozumalski A. A new method for estimating joint parameters from motion data. J Biomech. 2005;38:107–16. doi: 10.1016/j.jbiomech.2004.03.009. [DOI] [PubMed] [Google Scholar]
- 48.Eliasson AC, Krumlinde-Sundholm L, Rösblad B, Beckung E, Arner M, Ohrvall AM, et al. The manual ability classification system (MACS) for children with cerebral palsy: Scale development and evidence of validity and reliability. Dev Med Child Neurol. 2006;48:549–54. doi: 10.1017/S0012162206001162. [DOI] [PubMed] [Google Scholar]
- 49.Koop SE. Scoliosis in cerebral palsy. Dev Med Child Neurol. 2009;51(Suppl 4):92–8. doi: 10.1111/j.1469-8749.2009.03461.x. [DOI] [PubMed] [Google Scholar]
- 50.Saito N, Ebara S, Ohotsuka K, Kumeta H, Takaoka K. Natural history of scoliosis in spastic cerebral palsy. Lancet. 1998;351:1687–92. doi: 10.1016/S0140-6736(98)01302-6. [DOI] [PubMed] [Google Scholar]