

Jaipur Foot was hailed by the Times magazine as among the greatest inventions of the 20th century. Technically, it is a modification of the Solid Ankle, Cushioned Heel (SACH) Foot, and hence not a unique or novel product. The dictionary defines an invention as a NEW device, method, or process developed from studies and experimentation, but as per the Wikipedia, it may be an improvement upon a product for creating a new result.
The SACH Foot was developed by J. Foort and C.W. Radcliffe of the Prosthetic Devices Research Project, Institute of Engineering Research, University of California (Berkeley), who designed the first prototypes of the present version of the SACH Foot, in 1957.1
The SACH Foot development was facilitated by the earlier work done by the UC-Berkeley project on fundamental studies of human locomotion. Initial evaluations of the UC-Berkeley SACH Foot yielded extremely favorable amputee reactions, particularly to the shock absorption of the heel and the “smooth transition of weight from heel to toe during the stance phase.” In the spring of 1957, production models were found to be acceptable to the testing agency resulting in a May 24, 1957, approval by the Committee on Prosthetics Research and Development.1
The SACH Foot gained near-universal acceptance in the European and North American countries but failed to gain favor in the Southeast Asia and the South American and African countries. The reasons were varied. It necessitated the use of a shoe, and hence all the countries with a barefoot culture rejected it. Most of these countries were farming nations with the people working in the fields filled with water, conditions not conducive to or compatible with the use of the SACH Foot. Most of the rural folk in all these nations worked or walked on uneven terrain, which did not exactly wear well with the SACH Foot, and it interfered with their floor-sitting culture. All researches and developments in these countries were aimed at doing away with these “deficiencies.”
To do away with the shoe, the SACH Foot was given a cloak of a rubber foot. This made the foot exceptionally heavy, and there was still the issue of not being able to squat. It was these problems that Dr. P K Sethi was trying to grapple with. The wooden keel in the SACH Foot prevented any simulation of either the ankle movements or the subtarsal movements of inversion and eversion, incapacitating the ability of the amputee to squat or sit cross-legged.
Replacing the wooden keel by a block of rubber imparted some unique properties to the footpiece. A semblance of ankle dorsiflexion became possible at the wooden block and replaced rubber block interface, thereby enabling the amputee to squat. In addition, a rotational torque could be elicited between the new rubber block and the metatarsal block of rubber which simulated supination and pronation of the foot, which now facilitated cross-legged sitting involving inversion of the foot [Figure 1].
Figure 1.
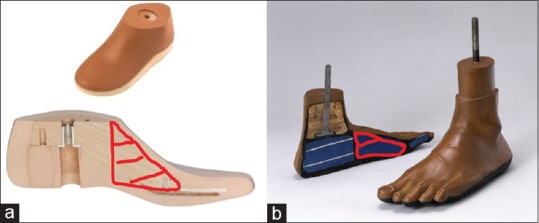
(a) The Solid Ankle, Cushioned Heel Foot and cross-section showing the solid wooden ankle and the keel marked in red-striped area. (b) The Jaipur Foot and cross-section showing the solid wooden ankle but the keel replaced by the red-striped rubber block
More than this, the greater problem was the wooden shank to which the SACH Foot was attached. The shank was being made of wood, hollowed and shaped like the stump. Wood was hard to come by, and this not only took time to craft but was heavy and costly. The West was switching to polymers such as “Plastazote.” Plastazote was easily heat molded (85°C–140°C) and would adhere to most materials, but this was very costly and only imported at the time.
Dr. Sethi happened to visit the local School of Art and Craft and was impressed by the work of Master Ram Chanderji who was teaching the students to make various decoration pieces out of aluminum. He was so adept at his art that Dr. Sethi asked him if he could fabricate a human lower limb. Masterji promptly shaped out a lower limb out of a welded aluminum tube that was so absolutely lifelike that it even showed the vein markings. Dr. Sethi arranged to have this master craftsman transferred to the Rehabilitation Research Centre (RRC) and initiated him into making the shanks of the below-knee prosthesis with a patellar tendon-bearing (PTB) top [Figure 2].
Figure 2.
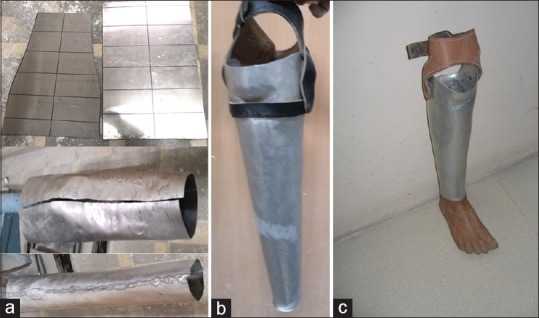
(a) Aluminum sheet cut as the shank piece, bent and shaped over an anvil like the calf with a patellar tendon-bearing top (b) the aluminum shank with patellar tendon-bearing top and thigh corset (c) the aluminum prosthesis with Jaipur Foot
His crafted PTB top prosthesis shanks were so near “total contact sockets” to those fabricated using negative plaster casts and plaster molds. In a later modification to the aluminum socket, the P K Sethi Memorial Rehabilitation Research center at the Santokba Durlabhji Hospital, under the stewardship of Dr. Anil Jain, and in co-operation with the International Committee of Red Cross, added an ethylene vinyl acetate liner in 1995 which gave the socket air-cushioning effect akin to that of a suction socket, allowing the thigh strap to be dispensed with [Figure 3].2
Figure 3.
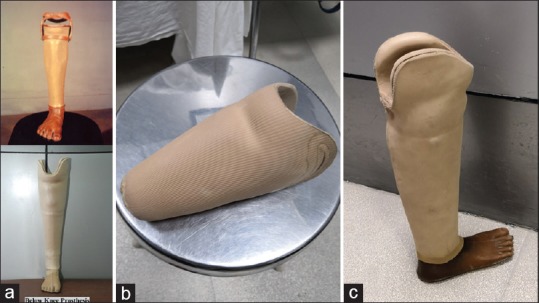
(a) The finished aluminum prosthesis with thigh corset and with the ethylene vinyl acetate liner without the corset, (b) the ethylene vinyl acetate liner, (c) the aluminum prosthesis with the Jaipur Foot and the ethylene vinyl acetate liner insert
The Jaipur Foot was attached by a bolt screwed into a wooden block “gutka” fitted into the distal end of the shank. The placement of the “gutka” determined the varus–valgus alignment and the dorsiflexion–plantar flexion of the foot, with a few blows producing the correct balancing and alignment comparable to the normal limb. This soon graduated into the aluminum quadrilateral top socket of the above-knee prosthesis with a PTB top socket below the knee component. Dr. Sethi enjoined upon Master Ram Chander to start training the other workers in the workshop and pretty soon, there was a reasonable workforce of workers, even amputee patients who wished to train.
This was giving vision to Dr. Sethi's ambition and the dream of demystifying knowledge and simplifying technology so that it reached and was understood by the masses and rural folk. Perhaps, the principal, rather sole involvement, in this endeavor was that of Master Ram Chanderji. It would have been natural for him to crave recognition for this development of the aluminum shank with PTB top for which he deserved full credit, but it is in deference to him that he did not.
The natural corollary to this was the setting up of camps in rural areas. Dr. Sethi's idea at these camps was to fit the local amputees with the aluminum prosthesis with the Jaipur Foot, but more than that impart training to the local artisans by allowing the team of Master Ram Chanderji and other workers to demonstrate and teach the fabrication of the aluminum shank with PTB top from aluminum sheets and welded tubes on just an anvil and using a hammer. The idea was that in the event of any pressure points developing, the amputee did not have to run back to Jaipur and the RRC, but could have his/her problem resolved by the local blacksmith by a few blows from the hammer.3
Somewhere down the line, the number of amputees fitted at these camps overtook the concept of imparting training to the local artisans, and it all boiled down to a game of numbers.
These aluminum socket prostheses were so comfortable and durable that some patients, like an interior designer from Delhi, have been using them for more than 10 years.2 They are not willing to part with them or change them for the costlier modern-day plastic materials even though they can afford to. According to the patients, these plastic material appliances do not allow the stump to breathe, are not alterable should some discomfort points appear and cannot be rectified locally. Hence, rural and semi-urban folk do not opt even for the molded total contact socket fabricated out of polyethylene pipes used for irrigation and sewage. They may yield high-volume appliances and may be good for producing numbers, but also have a very high rejection rate.2
The high rejection rate was reported by an International Society of Prosthetics and Orthotics (ISPO) team visiting projects in developing countries to study the use of “appropriate technology,” as defined by an ISPO committee. Projects in India, Uganda, and Honduras were studied. The ISPO committee reported poor craftsmanship in 56% owing to any or combination of poor fit, misalignment, socket-wall inadequacy, and limb-length discrepancy in the high-density polyethylene (HDPE)–Jaipur Foot system. The HDPE pipe socket and shank were fabricated after heating the pipe to 200°C. The fleeting time interval before the HDPE pipe cooled and hardened did not allow the proper shaping of the “shank” for the varus–valgus and rotational alignment, as well as the consequent socket wall inadequacy and probable poor fit. The technical quality of the Jaipur Foot was considered acceptable, even better than the results reported by the ISPO of SACH Foot designs.4
Apparently, the cost of the HDPE pipe versus the aluminum sheet, the ease and lesser time of fabrication of the HDPE shank once the plaster mold was taken, and possibly some other factors eased out the aluminum socket from the mass production and fitment of these artificial limbs, and the aluminum socket lost out to the HDPE socket, notwithstanding all its advantages. Dr. Sethi's ambitious vision of simplifying and disseminating technology just about bit the dust, much against the need and necessity of the times. It is unfortunate that what should have been a laud to a revolutionary concept of demystifying science and technology and taking it to the rural masses, turned into a controversy centered around whose concept it was to replace the wooden keel of the SACH foot by a rubber metatarsal block [Figure 4], to give some measure of dorsiflexion needed for squatting, and a wee bit of torsion to enable the inversion for sitting cross-legged. So stands the prevalent status of the Jaipur foot and the “Jaipur Prosthesis”.
Figure 4.
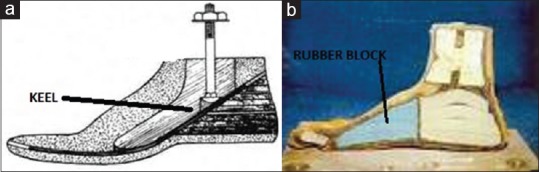
(a) Cut section diagrammatic representation of Solid Ankle, Cushioned Heel Foot (b) Cut section diagrammatic representation of Jaipur Foot
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Staros A. Chief VA prosthetics center: The SACH (solid-ankle cushion-heel) Foot. Orthop Prosthet Appliance J. 1957:23–31. [Google Scholar]
- 2.Anil J, Sethi PK. Jaipur: Personal Communication; 2018. Memorial Rehabilitation Research Center, Santokba Durlabhji Hospital. [Google Scholar]
- 3.Sethi PK. The Knud Jansen lecture. Technological choices in prosthetics and orthotics for developing countries. Prosthet Orthot Int. 1989;13:117–24. doi: 10.3109/03093648909079418. [DOI] [PubMed] [Google Scholar]
- 4.Jensen JS, Heim S. Preliminary experiences with modified SACH feet manufactured and used in a tropical developing world setting. Prosthet Orthot Int. 1999;23:245–8. doi: 10.3109/03093649909071641. [DOI] [PubMed] [Google Scholar]