

Abstract
Introduction
Thyroid cancer (TC) is an important common endocrine malignancy, and its incidence has increased in the past decades. The current TC diagnosis and classification tools are fine-needle aspiration (FNA) and histological examination following thyroidectomy. The metabolite profile alterations of thyroid cells (oncometabolites) can be considered for current TC diagnosis and management protocols.
Methods
This systematic review focuses on metabolite alterations within the plasma, FNA specimens, and tissue of malignant TC contrary to benign, goiter, or healthy TC samples. A systematic search of MEDLINE (PubMed), Scopus, Embase, and Web of Science databases was conducted, and the final 31 studies investigating metabolite biomarkers of TC were included.
Results
A total of 15 targeted studies and 16 untargeted studies revealed several potential metabolite signatures of TC such as glucose, fructose, galactose, mannose, 2-keto-d-gluconic acid and rhamnose, malonic acid and inosine, cholesterol and arachidonic acid, glycosylation (immunoglobulin G [IgG] Fc-glycosylation), outer mitochondrial membrane 20 (TOMM20), monocarboxylate transporter 4 (MCT4), choline, choline derivatives, myo-/scyllo-inositol, lactate, fatty acids, several amino acids, cell membrane phospholipids, estrogen metabolites such as 16 alpha-OH E1/2-OH E1 and catechol estrogens (2-OH E1), and purine and pyrimidine metabolites, which were suggested as the TC oncometabolite.
Conclusion
Citrate was suggested as the first most significant biomarker and lactate as the second one. Further research is needed to confirm these biomarkers as the TC diagnostic oncometabolite.
Keywords: biomarkers, oncometabolites, thyroid cancer, TC, systematic review
Introduction
Thyroid cancer (TC) is the most common endocrine-related tumor in the past decades, and its incidence has been increasing all over the world.1–4 The starting point of TC is the thyroid nodule formation detectable by ultrasonography (US) evaluations.5,6 Thyroid nodules are mostly benign, and the current gold standard discriminative tool between TC and benign thyroid nodules (BTNs) is a cytopathologic analysis of percutaneous fine-needle aspiration (FNA) specimens.7 FNA is a simple test that samples a small amount of tissue from the thyroid with a very thin (or “fine”) needle.8–11 Histopathological report of FNA has a weak point of indeterminate results, negative predictive value, and high cost.12,13 Hence, there is an extreme need to find molecular markers either to support FNA or to take the place of FNA.14–17
Increasing evidence indicates that tumor-associated mutations represent key factors resulting in different profiles of the cancerous cells’ genomics, epigenomics, transcripttomics, proteomics, and metabolomics.18–20,117,118 Metabolomics is an extensive-scale study of small molecules (>1,000 Da), generally popular as metabolites, within cells, biofluids, tissues, or organisms.21–23 The major dissimilarities between cancerous cells and their counterpart noncancerous cells are their metabolites, which are called “oncometabolites”.24 For the first time, it was revealed in 1927 that tumors display a unique metabolic phenotype, and their glucose level is up to 200 times more than that of normal cells.25 Despite ignorance of oncometabolite impact on cancer diagnosis and management by 1970s, oncometabolites were rediscovered in the past decades.26 Oncometabolites are intrinsic metabolites that either start or continue tumor growth and metastasis. The primary oncometabolite was 2-hydroxyglutarate (2HG), which was recognized as a main metabolite with much higher concentrations in gliomas than normal cells.27 Main oncometabolites can be classified into six hallmarks: 1) those involved in glucose and amino acid uptake, 2) use of adaptable modes of nutrient gaining, 3) use of glycolysis/tricarboxylic acid (TCA) cycle and NADPH production, 4) augmented demand for nitrogen, 5) modifications in metabolite-driven gene regulation, and 6) metabolic contacts with the microenvironment. In fact, limited tumors show all six hallmarks together, and each one can be an indicator of tumor and can guide scientists to the exact tumor classifi-cation and higher efficient tumor management policies.28 There are nine oncometabolites in different types of TCs: 2HG, glucose, fumarate, succinate, sarcosine, glutamine, asparagine, choline, and lactate.29 Recently, some studies on the metabolomics analysis of FNA specimens of thyroid nodules have suggested the benefit of oncometabolites approach as the potential application for the cooperative diagnosis tool of TC.30–33 Several metabolic pathways linking it to the TCA, pentose phosphate pathway, and lipid metabolism are candidate biomarkers to discriminate between normal and cancer cells (Figure 1).
Figure 1.

Several metabolic pathways in normal and cancer cells.
Abbreviation: TCA, tricarboxylic acid.
Here, we present the first meticulous summary of the entire available primary research to evaluate the potential of oncometabolites as the discriminative molecular marker between TC and BTNs.
Research design and methods
Search strategy
The study was conducted according to International prospective register of systematic reviews PROSPERO code: CRD42018088928 (http://www.Crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018088928). All related literature searches from four main databases including MED-LINE (PubMed), Scopus, Embase, and Web of Science for relevant articles were retrieved from January 1, 1998, to end of March 2018 with the key words grouping of “metabolomics”, “metabonomics”, “oncometabolites”, “metabolic profiling”, combined with “Thyroid Neoplasm”, “Thyroid Carcinoma”, “Thyroid Adenoma”, “Thyroid Nodules”, and “Thyroid Cancer” (Supplementary materials). To minimize selection bias, two independent investigators (BA and MS) autonomously checked titles, abstracts, and available full-text articles for application. Further articles were recognized by checking the reference lists from the selected studies. Disagreements were fixed by agreement and discussion with a third researcher (KG).
Eligibility criteria
All nominated studies were reviewed by two authors independently and according to their title and abstract were categorized as the included one or excluded one. The inclusion criteria were as follows: 1) participants included thyroid patients with TC; 2) the control population was specified (eg, patients with BTN, goiter patients, or healthy subjects); 3) all metabolomics detection techniques such as HPLC, ultra performance liquid chromatography (ULC), mass spectrometry (MS), tandem mass spectrometry (TMS), and nuclear magnetic resonance (NMR) spectroscopy were selected; and 4) metabolites were examined in plasma, serum, urine, or FNA specimens. Research studies were excluded if they 1) analyzed metabolite profiles in animals (in vivo studies), 2) analyzed metabolite profiles in cell culture (in vitro studies), or 3) did not contain a suitable control group.
Data extraction and analysis
All data on population distinctiveness and indicative oncometabolites were entered in Excel. FK had performed the data completion steps, which was confirmed by another researcher (MP). Due to the inadequate quantity of studies related to TC and metabolomics, and the extensive method ological heterogeneity and the significant dissimilarities in study population characteristics, an assessable meta-analysis of the data was not applicable.
The quality assessment tools
Here, we used Quality Assessment of Diagnostic Accuracy Assessment (QUADAS) and The Newcastle–Ottawa Scale (NOS) assessment tools to assess the methodological quality of the selected research articles. QUADAS and NOS were used to evaluate quality issues particular for “-omics” (QUADOMICS) more than the quality assessment of studies involving in systematic reviews.34,35 Each research article that scored 12/16 or more on the QUADOMICS tool together with 6/8 or more on NOS were considered as “high quality”, while each research article that scored 11/16, 5/8, or less were considered as “low quality”.
Results
Study selection and characteristics
The selection algorithm and results of study selection are presented in Figure 2. A total of 806 articles were retrieved after duplication deletion, including 374 articles from PubMed, 293 from Scopus, 83 from Web of Science, and 56 from Embase. After deleting the review, in vivo/in vitro studies, and book or conference paper with no available full-text articles, the final 31 articles were chosen for further considerations. A total of 15 studies with targeted metabolites (Table 1) and 16 studies with untargeted metabolites methods (Table 2) were selected. Two studies with targeted metabolites were removed because of low quality after quality assessment.
Figure 2.
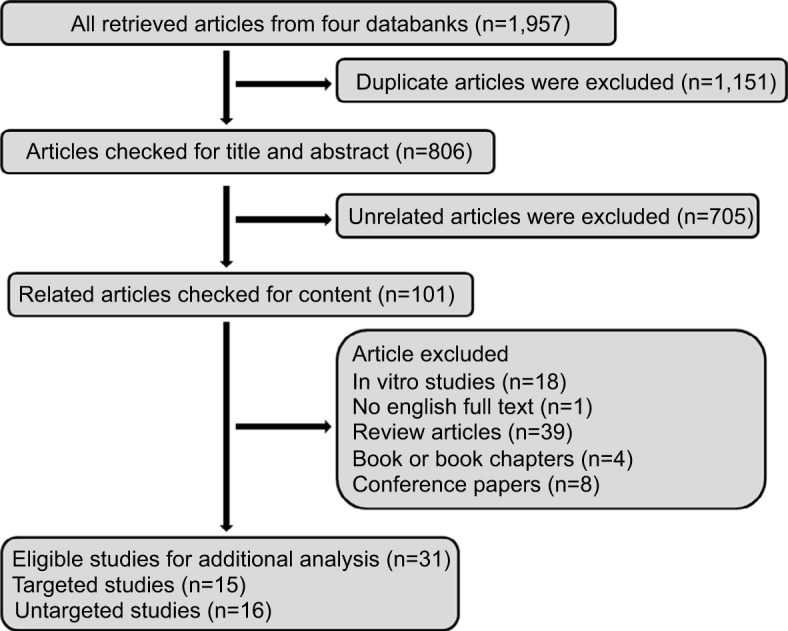
Flow diagram of study selection for the current systematic review.
Table 1.
Thirteen targeted studies related to the cometabolites in TC
| Title of article | First author | Year | Country | Sample size | Type of study | Metabolite measurement techniques | List of targeted metabolites | Significant different metabolites | |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Unbalanced estrogen metabolism in TC36 | Muhammad Zahid | 2013 | USA (Omaha) | n: 40 TC n: 40 HI | Case/control | ULC TMS | Catechol estrogen quinones, estrogen-3,4-quinines, 38 estrogen metabolites (conjugates and DNA adducts) Estrogens (E1 and E2) | Estrogen metabolites |
| 2. | A SSEAT for “Functional” BiomarkerDiscovery37 | Josep Villanueva | 2008 | USA (New York) | n: 48 metastatic TC n: 48 HI | Case/control | MALDI-TOF MS | Fibrinogen α, C3f (complement C3), complement C4 precursor ITIH4, apolipoprotein A-IV Clusterin precursor, C-terminus of β-chain minus Arg-transthyretin precursor | N/A |
| 3. | Human IgG Fc-glycosylation profiling reveals associations with age, sex, female sex hormones, and TC38 | Guoqiang Chen | 2012 | China | n: 138 TC | Case/control | MALDI-FTICR | Seven glycosylation features for IgG | Fc-glycosylation |
| 4. | Multicompartment metabolism in papillary thyroid cancer39 | Joseph M. Curry | 2016 | USA | n: 27 NTC n: 6 FA n: 5 MNG | Case/control | IHC | TOMM20 MCT4 | Multiple tumor compartments with glycolysis in fibroblasts and OXPHOS |
| 5. | Biochemical markers in the follow-up of medullary thyroid cancer40 | Jan Willem B. de Groot | 2006 | The Netherlands | n: 46 MTC | Prospective study | GC | Calcitonin and CEA, plasma tryptophan Plasma platelet serotonin, urine 5-hydroxyindole acetic acid, MIMAA, 3-MT, HVA, VMA, VA, MOPEG, DOPAC | Plasma calcitonin Carcinoembryonic antigen, chromogranin A |
| 6. | Predictive value of sphingosine kinase 1 expression in papillary thyroid carcinoma41 | SUNG-IM DO | 2017 | Korea | n: 110 PTC n: 16 MNG n: 81 NTC | Case/control | IHC | Sphingosine kinase 1 metabolites | Sphingosine kinase 1 |
| 7. | Metabolic changes enhance the cardiovascular risk with differentiated thyroid carcinoma – a case–control study from Manipal Teaching Hospital of Nepal42 | Ankush Mittal | 2012 | Nepal | n: 50 DTC n: 50 HI | Case/control | ELISA CHOD-PAP and GPO-PAP method | fT3, fT4, TSH, total cholesterol Triglycerides, HDL, LDL, VLDL glucose, insulin, fibrinogen CRP | Hypercoagulable state Atherogenic lipid profile |
| 8. | 3, 30-Diindolylmethane modulates estrogen metabolism in patients with TPD: a pilot study43 | Shilpi Rajoria | 2011 | New York, New Jersey | n: 7 TPD | Clinical trial study (a pilot study) | GC-MS | Estrogen metabolites 2-hydroxyestrones (C-2) 16α-hydroxyestrone (C-16) | Antiestrogenic activity that results in more of C-2 product compared with C-16 |
| 10. | Perioperative dynamics and significance of amino acid profiles in patients with cancer45 | Yu Gu | 2015 | China | n: 56 GC n: 28 BC n: 33 TC | Case/control | Amino acid analyzer with spectrophotometrical detection | PFAAs (Asp, Thr, Ser, Glu, Gly, Ala, Cys, Val, Met, Ile, Leu, Tyr, Phe, Lys, His, Arg, Pro, NH3, NEAAs, EAAs, BCAAs, GAAs, TAAs) | PFAA |
| 11. | Estrogens in female TC: alteration of urinary profiles in preoperative cases and postoperative cases46 | Seon Hwa Lee | 2003 | South Korea | n: 18 premenopausal PTC women (preoperative and postoperative patients in luteal phase) | Case/control | Highly sensitive GC-MS | Estrogen metabolites 16alpha-OH E1/2-OH E1 Catechol estrogens (2-OH E1) | 2-hydroxylation in estrogen metabolism |
| 12. | Increased expression of phosphatidylcholine (16:0/18:1) and (16:0/18:2) in thyroid papillary cancer47 | Seiji Ishikawa | 2012 | Japan | n: 7 TC cases | Case series | HE-stained, tandem mass (MS/MS) analysis, imaging mass spectrometry analysis | Phosphatidylcholine (16:0/18:1), phosphatidylcholine (16:0/18:2), sphingomyelin (d18:0/16:1) | Phosphatidylcholine Sphingomyelin |
| 13. | Application of metabolomics in prediction of lymph node metastasis in papillary thyroid carcinoma48 | Ji Won Seo | 2018 | Korea | n: 52 metastatic PTC | Case series | H-NMR spectroscopy | Isoleucine, leucine, valine, lactate, threonine, alanine, uracil, lysine, glutamate, methionine, aspartate, choline, phosphocholine, glycerophosphocholine, taurine, myo-inositol, glycine, phosphoethanolamine, inosine, thyrosine, hypoxanthine, formate, succinate, uridine | Lactate |
Abbreviations: 3-MT, 3-methoxytyramine; aMT6, melibiose 6-sulfatoxymelatonin; BC, breast cancer; CEA, carcinoembryonic antigen; C3f, complement C3f; DOPAC, 3,4-Dihydroxyphenylacetic acid; DTC, differentiated thyroid carcinoma; FPA, fibrinogen α; fT3, free triiodothyronine; fT4, free thyroxine; GC, gastric cancer; GC-MS, gas chromatography–mass spectrometry; GC-TOF-MS, gas chromatography–time-of-flight mass spectrometry; GLA, alpha-galactosidase; HDL, high-density lipoprotein; HI, healthy individual; HVA, homovanillic acid; IHC, immunohistochemistry; ITIH4, inter-α-trypsin inhibitor heavy chain H4; LDL, low-density lipoprotein; MALDI-FTICR, matrix-assisted laser desorption ionization–Fourier transform ion cyclotron resonance; MALDI-TOF MS, matrix assisted laser desorption ionization–time of flight mass spectrometry; MCT4, monocarboxylate transporter 4; MIMAA, N’-methylimidazole acetic acid; MNG, multinodular goiter; MOPEG: 3-methoxy-4-hydroxyphenylglycol; MTC, medullary thyroid cancer; N/A, not applicable; NAT, normal adjacent tissue; NTC, noncancerous thyroid tissue; OA, oxaloacetate; OXPHOS, Mitochondrial oxidative phosphorylation; PFAA, plasma-free amino acid; PHE, phenylalanine; PTC, papillary thyroid carcinoma; PUFA, polyunsaturated fatty acid; SSEAT, Sequence-specific Exopeptidase Activity Test; TC, thyroid cancer; TMS, tandem mass spectrometry; TOMM20, translocase of outer mitochondrial membrane 20; TSH, thyroid-stimulating hormone; TPD, thyroid proliferative disease; ULC, ultra performance liquid chromatography; VA, valine; VLDL, very-low-density lipoprotein.
Table 2.
The list of 16 untargeted studies related to the cometabolites in TC
| Title of article | First author | Year | Country | Sample size | Type of study | Metabolite measurement techniques | Significant different metabolites | |
|---|---|---|---|---|---|---|---|---|
| 1. | Development of data independent acquisition workflows for metabolomic analysis on a quadrupole-orbitrap platform49 | Juntuo Zhou | 2017 | China | n: 30 TC n: 27 HI | Case/control | LC-DIA-MS | Carnitine Trimethylamine N-oxide Some amino acids |
| 2. | Analysis on the metabolite composition of serum samples from patients with papillary thyroid carcinoma using NMR50 | Wen-Xin Zhao | 2015 | China | n: 20 PTC n: 20 BTN n: 20 HI | Case/control | NOEPR-CPMG NMR | A list of metabolites involves glucose metabolism, lipids, amino acids, and nucleic acid |
| 3. | Detection of metastatic breast and TC in lymph nodes by desorption electrospray ionization mass spectrometry imaging51 | Jialing Zhang | 2017 | USA | n: 18 NLN n: 8 LNMP n: 16 LNMBC | Case/control | DESI-MS | Ceramides Glycerophosphoinositol |
| 4. | Serum metabolic profiling and features of papillary thyroid carcinoma and nodular goiter52 | Zhenzhen Yao | 2011 | China | n: 30 PTC n: 80 MNG n: 30 HI | Case/control | Liquid chromatography-LTQ Orbitrap MS | 3-Hydroxybutyric acid |
| 5. | Distinct metabolomic profiles of papillary thyroid carcinoma and benign thyroid adenoma53 | Yanan Xu | 2015 | China | n: 57 PTC n: 48 BTA | Case/control | GC-TOFMS UPLC–Q-TOF-MS | Purine and pyrimidine metabolites Taurine Hypotaurine |
| 6. | Serum and urine 1H NMR-based metabolomics in the diagnosis of selected thyroid diseases54 | Wojciech Wojtowicz | 2017 | Poland | n: 20 NN n: 13 FA n: 17 TC n: 17 HI | Case/control | NMR | Amino acids: alanine, creatine, glutamine, tyrosine, valine Carboxylic acids: acetate, citrate, formate, lactate Monosaccharides: glucose Alcohols: glycerol Imidazolinones: creatinine |
| 7. | Metabolic alteration of urinary steroids in premenopausal and postmenopausal women and men with papillary thyroid carcinoma55 | Man Ho Choi | 2011 | Korea | n: 21 premenopausal female n: 19 postmenopausal female n: 16 male PTC | Case/control | GC-MS | Androgens Androstenedione Androstenediol 16α-hydroxy DHEA Corticoid |
| 9. | Metabolomics approach to thyroid nodules: a high-resolution magic-angle spinning NMR-based study31 | Paolo Miccoli | 2012 | Italy, France, Brazil | n: 28 PTC n: 40 FA n: 4 BN | Case/control | HRMAS HRMAS-NMR | Lactate Taurine Phosphocholine Myo-inositol Scyllo-inositol |
| 10. | Metabolomic analysis of percutaneous fine-needle aspiration specimens of thyroid nodules: potential application for thepreoperative diagnosis of TC57 | Inseon Ryoo | 2016 | Korea | n: 35 PTC n: 69 BN | Case/control | NMR | Lactate Glycine Citrate Glutamine Glutamate Choline O-phosphocholine |
| 11. | A distinct serum metabolic signature of distant metastatic papillary thyroid carcinoma58 | Chen-Tian Shen | 2017 | China | n: 37 distant metastatic PTC n: 40 ablation group | Case/control | GC-TOF-MS | Phthalimide, cyclohexanamine, aminooxyacetic acid, 3-hydroxypyruvate, carbamate, canavanine, creatine, asparagine, uridine, 4-deoxypyridoxine, 2-hydroxypyridine, γ-aminobutyric acid, myo-inositol, pyroglutamic acid, stearic acid, palmitic acid, fructose, heptadecanoic acid, phenyl acetate, glycerol-3-phosphate, lactose, arachidic acid, uric acid, valine, palmitoleic acid, γ-linoleic acid, parabanic acid, picolinic acid, oxalic acid, uracil, d-altrose |
| 12. | Toward the reliable diagnosis of indeterminate thyroid lesions: a HRMAS NMR-based metabolomics case of study59 | Liborio Torregrossa | 2012 | Italy, France, Brazil | n: 72 PTC | Case series | HRMAS | ↑ PHE, taurine, and lactate ↓ Choline and choline derivatives ↓ myo- and scyllo-inositol |
| 13. | Exhaled breath volatile biomarker analysis for TC60 | Lei Guo | 2015 | China | n: 39 PTC n: 25 MNG | Case/control | GC/MS | Sulfurous acid, cyclohexylmethyl hexyl ester, isolongifolene-5-ol, 3,5-Decadien-7-yne, 6-t-butyl-2,2,9,9-tetramethyl, cyclohexanone, 4-hydroxybutyric acid, phenol, 2,2-dimethyldecane, ethylhexanol, ethylene glycol mono vinyl ester, cyclopropane, 1-bromo-1-(3-methyl-1-pentenylidene)–2,2,3,3-tetramethyl, (3-Methyl-oxiran-2-yl)-methanol, cyclopentane, 1,1,3-trimethyl-3-(2-methyl-2-propenyl), trans-2-dodecen-1-ol |
| 14. | Association of PBDEs and hydroxylated metabolites (OH-PBDEs) serum levels with thyroid function in TC patients61 | Sisi Lui | 2017 | China | n: 33 PTC | Case series | Chemiluminescence enzyme immunoassay | Diphenylethers (PBDEs) Hydroxylated metabolites (OH-PBDEs) |
| 15. | Noninvasive diagnosis of papillary thyroid microcarcinoma: a NMR-based metabolomics approach62 | Jinghui Lu | 2016 | China, Italy | n: 35 PTC | Case series | HRMAS H-NMR | Lysine Glutamate Tyrosine Catecholamines (dopamine, norepinephrine, and epinephrine) |
| 16. | Follicular adenomas exhibit a unique metabolic profile. 1H NMR studies of thyroid lesions63 | StanisławDeja | 2013 | Poland | n: 45 TC n: 19 HI | Cohort | H-NMR | Isoleucine, valine, alanine, NACs, methionine, citrate, creatine, choline, GPC, scyllo-inositol, taurine, glycine, myo-inositol, lactate, histidine, tyrosine, phenylalanine |
Abbreviations: BN, benign nodule; BTA, benign thyroid adenoma; BTN, benign thyroid nodule; DESI-MS, desorption electrospray ionization mass spectrometry; DHEA, dehydroepiandrosterone; FA, follicular adenoma; GC-TOF-MS, gas chromatography–time-of-flight mass spectrometry; GC-MS, gas chromatography–mass spectrometry; HI, healthy individual; HRMAS, high-resolution magic angle spinning; LC-DIA-MS, liquid chromatography–data independent-mass spectrometry; LNMBC, lymph node with metastatic breast cancer; LNMP, lymph node with metastatic NAC, N-acetyl-cysteine; PHE, phenylalanine; PTC; MNG, multinodular goiter; NAT, normal adjacent tissue; NOEPR, nuclear over Hauser effect spectroscopy with P re-saturation; CPMG, Carr-Pure-Me boom-Gill sequence; NLN, normal lymph node; NMR, nuclear magnetic resonance; NN, non-neoplastic nodule; OH-PBDE, hydroxylated polybrominated diphenylether; PBDE, polybrominated diphenylether; PTC, papillary thyroid carcinoma; TC, thyroid cancer; UPCL-Q-TOF-MS, The ultra-high performance liquid chromatography-quadrupole time-of-flight mass spectrometry.
The sample size of the study population was different from one case report that discussed 138 TC cases. Five studies were conducted in USA, 12 in China, five in Korea, two in Poland, two in Italy, one in Japan, one in Nepal, and one in the Nether-lands. Both case/control and case report/series were included in the studies. In most case/control studies, the metabolites were compared between TC as the case group with healthy individuals and BTN or goiter patients as the controls. Exceptionally in two studies, the case/control was based on menopause TC and non-menopause TC. One study in Nepal evaluated the oncometabolites in differentiated thyroid carcinoma (DTC) with an increasing risk of cardiovascular disease. The oncometabolites included amino acids such as isoleucine, leucine, valine, lactate, threonine, alanine, uracil, lysine, glutamate, methionine, aspartate, choline, phosphocholine, glycerophosphocholine, taurine, myo-inositol, glycine, phosphoethanolamine, inosine, thyrosine, hypoxanthine, formate, succinate, and uridine; carboxylic acids such as acetate, citrate, fumarate, and lactate; monosaccharides such as glucose and glycosylation; estrogen metabolites such as 16 alpha-OH E1/2-OH E1 and catechol estrogens (2-OH E1); lipids such as total cholesterol, triglycerides, HDL, LDL, and VLDL; fibrinogen; calcitonin; and carcinoembryonic antigen (CEA). The unique phospholipids of bilayer membrane (phosphatidylcholine, phosphatidylcholine, and sphingomyelin) in addition to thyroid hormones, free triiodothyronine (fT3), free thyroxine (fT4), and thyroid-stimulating hormone (TSH) were also included in the list of metabolites. Some studies used the oncometabolites for TC diagnosis and some for follow-up and management of TC patients.
Amongst all selected studies in this systematic review, two studies were considered metabolite profile of premenopausal women. A targeted study conducted in Manipal Teaching Hospital of Nepal suggested that the hypercoagulable state atherogenic lipid profile is the different metabolite correlated with an increasing risk of cardiovascular disease in DTC patients. Other studies considered the different metabolite profiles as the discriminative tool of thyroid malignancy.
Discussion
Cancer studies highlighted the fact that cancer cells are common in biological capabilities such as constant proliferative signaling, growth suppressor’s avoidance, resistance to cell death, replicative immortality, high angiogenesis, reprogrammed energy metabolism, immune-mediated destruction, invasion, and metastasis.11,64,65,119 Metabolic reprogramming orchestrates cancer cell properties, so “cancer metabolism” became an important research topic for cancer management. The first study on cancer metabolism in 1924 suggested that the cancer phenotype for glucose metabolism is unique one and with higher ability of glucose uptake and lactate production is typical in several tumors.66 These pathways are named as “aerobic glycolysis” or the “Warburg effect”, which has the effect on the extracellular fluid around tumor tissue and change it to acidic pH.67–69 Glucose is the critical source of carbon that helps in the maintenance of cancer cell anabolism, TCA anaplerosis, aerobic glycolysis, hexokinase II activation, and modified signal transduction.70,71 Glucose was the most frequent metabolite elevated in most cancers26,72,73 and has been used as the oncometabolite of TCs in both targeted42,44 and untargeted studies.50,54,56 Analysis of the serum metabolic alterations among PTC, benign thyroid tumor, and healthy controls suggested that glucose metabolism cannot be the only important metabolite because metabolism of lipids, amino acids, and nucleic acids is important as well.50 Moreover, it was shown that the mRNA quantity of metabolic enzyme-coding genes resulting in different glucose, fructose, galactose, mannose, 2-keto-d-gluconic acid and rhamnose, malonic acid and inosine, cholesterol and arachidonic acid significantly increased in PTC.56 These studies were confirmed by detecting 31 different metabolites related to amino acid, lipid, glucose, vitamin metabolism, and diet/gut microbiota interaction.74
Metabolome analysis of amino acid profile is under consideration for biomarkers of thyroid malignancy. The plasma-free amino acid (PFAA) profiles of breast cancer, gastric cancer, and TC patients and investigation of their diagnostic potential were shown in the study by Gu et al.75 Carnitine, trimethylamine N-oxide (TMAO), proline, glutamine, and asparagine were known as the most significant metabolites of 392 metabolites in TC.49 In serum specimens of papillary TC patients, the amount of metabolites like valine, leucine, isoleucine, lactic acid, alanine, glutamic acid, lysine, glycine, whereas the lipids, choline, tyrosine decreased.76 Similarly alanine, creatine, glutamine, tyrosine, and valine in both serum and urine of TC patients were diagnosed by H NMR-based method.77
Glycosylation is one of the most frequent posttranslational modification reactions, and almost half of all proteins in eukaryotes are glycosylated.11,78 Some findings revealed the potential of IgG glycosylation as a biomarker for inflammation, metabolic health, and cancers.79,80 In TC, it was suggested that human IgG Fc-glycosylation profiling could be linked with age, sex, female sex hormones, and TC risk.38 IgG glycosylation in addition to glycans, glycome and glycoproteome are important in controlling thyroid cancer development and progression.81,82 The translocase of outer mitochondrial membrane 20 (TOMM20), a marker of oxidative phosphorylation, and monocarboxylate transporter 4 (MCT4), a marker of glycolysis, are candidate metabolites for aggressive behavior of TC.39
High levels of lactate and choline and low levels of citrate, glutamine, and glutamate in malignant thyroid nodules were reported by Ryoo et al33 and suggested them as the discriminative biomarker for determining the preoperative metabolomic profiles of thyroid nodules. Lactate is often augmented in several malignancies including head and neck cancers.30,31,83,84 High lactate level is the sign of glycolytic pathway increasing in response to hypoxia or ischemia in tumor tissues.85–87 Lactogenesis, an important step for the production of lactate, is started and triggered by gene mutations (the Warburg effect), so deregulated lactate metabolism and signaling are the critical elements in carcinogenesis.88 Lactate was established as an important factor in terms of cancer cell mobility and immune suppressor molecule that promote the tumor evasion as well.89,90 Lactate was found to be the most promising metabolite for discrimination of lymph node metastasis from nonmetastatic TC.48 Two studies confirmed that reduced levels of fatty acids and elevated levels of several amino acids (phenylalanine, tyrosine, lactate, serine, cystine, lysine, glutamine/glutamate, taurine, leucine, alanine, isoleucine, and valine) in papillary thyroid micro-carcinoma (PTMC) and rise of phenylalanine, taurine, and lactate and a reduction of choline and choline derivatives, myo- and scyllo-inositol in the malignant tumors vs to the benign ones.59,62
Phospholipids are esters of glycerol, fatty acids, phosphoric acid, and other alcohols. Nearly, all frequent phospholipids are phosphatidylcholine, phosphatidylethanolamine, phosphatidylinositol, and phosphatidylserine. Evidence showed that phosphatidylcholine, the major phospholipid element of eukaryotic membranes, like choline metabolites resulting from its metabolism, has an important role in cancer proliferation and survival.91 In thyroid malignancies, the increased multiplication and proliferation of cancer cells are linked to the increased choline contents even in FNA specimen.47,57,92 Choline was in the list of discriminative oncometabolites of TC with lymph node metastasis from non-metastatic one.48 These findings are contradictory with a study in which the content of lipids, choline, and tyrosine decreased in malignant TC compared to that in the benign one.31,50
Another metabolite that increased as the result of glycolysis in TC is glycine. It could be one of the essential metabolites in tumorigenesis and mitochondrial synthesis, and consumption of glycine was suggested as a discriminative metabolites triggering the cancer cell growth and development.33 Glycine dehydrogenase enzyme (GLDC), which cleavages glycine and mediates folate cycle charging, is highly expressed in tumor-promoting cells.93–95
Oncometabolomic analysis revealed that citrate uptake largely affected cancer cell metabolism through citrate-dependent metabolic pathways, and the extracellular citrate is provided to cancer cells through a plasma membrane-specific variant of the mitochondrial citrate transporter (pmCiC).96 In the study by Ryoo et al,57 it was suggested that citrate was the most powerful discriminator oncometabolite for diagnosis of TC. Previous studies also indicated that ATP citrate lyase, essential for cell proliferation, is upregulated in some human malignancies such as lung, colorectal, and ovarian cancers.97,98 The inhibition of ATP citrate lyase can block the proliferation of multiple tumor cell lines.99
The role of isocitrate dehydrogenase (IDH) mutations and d-2-HG accumulation in malignancy has increased recently.100 2-HG has been considered as oncometabolites and epigenetic modifiers in different malignancies such as gliomas,101–103 myelogenous leukemia,104 and renal cancer.105 Non-synonymous variants of IDH1 gene have been detected in thyroid carcinomas, and in PTC, the increased levels of 2-HG were reported.106–109 However, it has not been considered as an oncometabolite in TCs.
There are three main forms of estrogen in the human body: estradiol, estrone, and estriol. These forms of estrogen together with estrogen receptor and other estrogen metabolites (16 alpha-OH E1/2-OH E1 and catechol estrogens [2-OH E1]) are more commonly associated with cancer risk.110,111 For checking the possible outcome of estrogens in premenopausal female TC, the concentrations of 14 estrogens were assessed in the urine of patients with PTC preoperatively and postoperatively, and it was confirmed that low mean value of 16α-OH E1/2-OH E1 was observed in preoperative patients, and it was considerably dissimilar to the ratio of postoperative TC cases. The increase of 2-hydroxylation in estrogen metabolism may have a noteworthy relationship with the risk of TC formation in females.46 Moreover, it was shown that higher exposure to estrogens can increase the risk for TC, and 38 urinary estrogen metabolites were checked by Zahid et al, they suggested the unbalanced estrogen metabolism and formation of estrogen-DNA adducts as the role player in the initiation of TC.36 Supporting information indicated to anti-estrogenic dietary supplement function of 3,3′-diindolylmethane (DIM) to help reduce the risk of developing thyroid proliferative disease (TPD).43
In addition, the synthesis of purines and pyrimidine is upregulated in cancer cells, and the catalyzing enzymes of this pathway including thymidylate synthase and inosine synthetase 2 are subjected to Myc-induced upregulation.112,113 Glutamine is a nitrogen source for multiple steps of both purine and pyrimidine synthesis.114 Glutamine is a critical nutrient indispensable for cancer cell growth and is the new therapeutic target in cancers.115,116 In preoperative percutaneous FNA specimens of TC, it was shown that glutamine and glutamate are presented with lower relative concentrations.50,57 These results were generally in agreement with a previous finding obtained using surgical specimens.59 Pathway analysis indicated the “alanine, aspartate and glutamate metabolism” and “inositol phosphate metabolism” as the most relevant pathways in thyroid carcinogenesis.74 However, gastric cancer cells was promoted by cysteine, but inhibited by alanine and glutamic acid because alanine and glutamic acid induced apoptosis of gastric cancer cells.45 Follicular adenomas exhibit a unique metabolic profile with several oncometabolite profiles including glutamine.63
Conclusion
Because of the complexity of thyroid carcinogenesis, a wide range of oncometabolites is suggested as TC diagnostic markers. Potential biomarkers common to all thyroid lesions were mainly fatty acids, amino acids, cell membrane phospholipids, estrogen metabolites (16 alpha-OH E1/2-OH E1 and catechol estrogens(2-OH E1), purine and pyrimidine metabolites, citrate, glucose, mannose, pyruvate, and 3-hydroxybutyrate glycosylation (IgG Fc-glycosylation), TOMM20, MCT4, choline, choline derivatives, myo-/scyllo-inositol, and lactate. Among all metabolites, citrate was suggested as the first most significant oncometabolite and lactate as the second one in thyroid malignancies.
Supplementary Materials
Acknowledgments
The authors thank the Endocrinology and Metabolism Research Center, Endocrinology and Metabolism Clinical Sciences Institute, Tehran University of Medical Sciences.
Abbreviations
- BC
breast cancer
- BN
benign nodule
- BTA
benign thyroid adenoma
- BTN
benign thyroid nodules
- CEA
carcinoembryogenic antigen
- CPMG
Carr-Pure-Me boom-Gill sequence
- DESI-MS
desorption electrospray ionization mass spectrometry
- DTC
differentiated thyroid carcinoma
- FA
follicular adenoma
- FTC
follicular thyroid cancer
- GC
gastric cancer
- GC-TOF-MS
gas chromatography time-of-flight mass spectrometry
- HI
healthy individual
- HRMAS
high-resolution magic angle spinning
- LC-DIA-MS
liquid chromatography–data independent-mass spectrometry
- LNMBC
lymph node with metastatic breast cancer
- LNMP
lymph node with metastatic PTC
- MNG
multinodular goiters
- MTC
medullary thyroid cancer
- NAT
normal adjacent tissue
- NLN
normal lymph node
- NMR
nuclear magnetic resonance
- NN
non-neoplastic nodule
- NOEPR
nuclear over Hauser effect spectroscopy with P resaturation
- NTC
noncancerous thyroid tissue
- PTC
papillary thyroid carcinoma
- TCP
thyroid cancer patients
- TMS
tandem mass spectrometry
- TPD
thyroid proliferative disease
- ULC
ultra performance liquid chromatography
- UPLC–QTOFMS
ultra-performance liquid chromatography–quadruple time-of-flight mass spectrometry
- UTC
undifferentiated thyroid carcinoma
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Enewold L, Zhu K, Ron E, et al. Rising thyroid cancer incidence in the United States by demographic and tumor characteristics, 1980–2005. Cancer Epidemiology Biomarkers & Prevention. 2009;18(3):784–791. doi: 10.1158/1055-9965.EPI-08-0960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vergamini LB, Frazier AL, Abrantes FL, Ribeiro KB, Rodriguez-Galindo C. Increase in the incidence of differentiated thyroid carcinoma in children, adolescents, and young adults: a population-based study. J Pediatr. 2014;164(6):1481–1485. doi: 10.1016/j.jpeds.2014.01.059. [DOI] [PubMed] [Google Scholar]
- 3.Larijani B, Shirzad M, Mohagheghi MA, et al. Epidemiologic analysis of the Tehran cancer institute data system registry (TCIDSR) Asian Pac J Cancer Prev. 2004;5(1):36–39. [PubMed] [Google Scholar]
- 4.Haghpanah V, Soliemanpour B, Heshmat R, et al. Endocrine cancer in Iran: based on cancer registry system. Indian J Cancer. 2006;43(2):80. doi: 10.4103/0019-509x.25889. [DOI] [PubMed] [Google Scholar]
- 5.Moon WJ, Baek JH, Jung SL, et al. Ultrasonography and the ultrasound-based management of thyroid nodules: consensus statement and recommendations. Korean J Radiol. 2011;12(1):1–14. doi: 10.3348/kjr.2011.12.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Larijani B, Mohagheghi MA, Bastanhagh MH, et al. Primary thyroid malignancies in Tehran, Iran. Med Princ Pract. 2005;14(6):396–400. doi: 10.1159/000088112. [DOI] [PubMed] [Google Scholar]
- 7.Cooper DS, Doherty GM, Haugen BR. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214. doi: 10.1089/thy.2009.0110. [DOI] [PubMed] [Google Scholar]
- 8.Cibas ES, Ali SZ. NCI Thyroid FNA State of the Science Conference. The Bethesda system for reporting thyroid cytopathology. Am J Clin Pathol. 2009;132(5):658–665. doi: 10.1309/AJCPPHLWMI3JV4LA. [DOI] [PubMed] [Google Scholar]
- 9.Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur J Endocrinol. 2006;154(6):787–803. doi: 10.1530/eje.1.02158. [DOI] [PubMed] [Google Scholar]
- 10.Haghpanah V, Shooshtarizadeh P, Heshmat R, Larijani B, Tavangar SM. Immunohistochemical analysis of survivin expression in thyroid follicular adenoma and carcinoma. Appl Immunohistochem Mol Morphol. 2006;14(4):422–425. doi: 10.1097/01.pai.0000213100.88074.b8. [DOI] [PubMed] [Google Scholar]
- 11.Sanii S, Saffar H, Tabriz HM, Qorbani M, Haghpanah V, Tavangar SM. Expression of matrix metalloproteinase-2, but not caspase-3, facilitates distinction between benign and malignant thyroid follicular neoplasms. Asian Pac J Cancer Prev. 2012;13(5):2175–2178. doi: 10.7314/apjcp.2012.13.5.2175. [DOI] [PubMed] [Google Scholar]
- 12.Proietti A, Borrelli N, Giannini R, et al. Molecular characterization of 54 cases of false-negative fine-needle aspiration among 1347 papillary thyroid carcinomas. Cancer Cytopathol. 2014;122(10):751–759. doi: 10.1002/cncy.21454. [DOI] [PubMed] [Google Scholar]
- 13.Haddadi-Nezhad S, Larijani B, Tavangar SM, Nouraei SM. Comparison of fine-needle-nonaspiration with fine-needle-aspiration technique in the cytologic studies of thyroid nodules. Endocr Pathol. 2003;14(4):369–374. doi: 10.1385/ep:14:4:369. [DOI] [PubMed] [Google Scholar]
- 14.Khatami F, Larijani B, Tavangar SM. Circulating Tumor BRAF Mutation and Personalized Thyroid Cancer Treatment. Asian Pac J Cancer Prev. 2017;18(2):293. doi: 10.22034/APJCP.2017.18.2.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Khatami F, Tavangar SM. Liquid biopsy in thyroid cancer: new insight. Int J Hematol Oncol Stem Cell Res. 2018;12(3):234–247. [PMC free article] [PubMed] [Google Scholar]
- 16.Tavangar SM, Monajemzadeh M, Larijani B, Haghpanah V. Immunohistochemical study of oestrogen receptors in 351 human thyroid glands. Singapore Med J. 2007;48(8):744–747. [PubMed] [Google Scholar]
- 17.Mohammadi-Asl J, Larijani B, Khorgami Z, et al. Qualitative and quantitative promoter hypermethylation patterns of the P16, TSHR, RASSF1A and RARβ2 genes in papillary thyroid carcinoma. Med Oncol. 2011;28(4):1123–1128. doi: 10.1007/s12032-010-9587-z. [DOI] [PubMed] [Google Scholar]
- 18.Kildegaard HF, Baycin-Hizal D, Lewis NE, Betenbaugh MJ. The emerging CHO systems biology era: harnessing the “omics revolution for biotechnology. Curr Opin Biotechnol. 2013;24(6):1102–1107. doi: 10.1016/j.copbio.2013.02.007. [DOI] [PubMed] [Google Scholar]
- 19.Sarmadi S, Izadi-Mood N, Sotoudeh K, Tavangar SM, Expression AP. Altered PTEN expression; a diagnostic marker for differentiating normal, hyperplastic and neoplastic endometrium. Diagn Pathol. 2009;4(1):41. doi: 10.1186/1746-1596-4-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gilany K, Minai-Tehrani A, Amini M, Agharezaee N, Arjmand B. The challenge of human spermatozoa proteome: a systematic review. J Reprod Infertil. 2017;18(3):267. [PMC free article] [PubMed] [Google Scholar]
- 21.Johnson CH, Ivanisevic J, Siuzdak G. Metabolomics: beyond biomarkers and towards mechanisms. Nat Rev Mol Cell Biol. 2016;17(7):451–459. doi: 10.1038/nrm.2016.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gilany K, Jafarzadeh N, Mani-Varnosfaderani A, et al. Metabolic fingerprinting of seminal plasma from non-obstructive Azoospermia patients: positive versus negative sperm retrieval. J Reprod Infertil. 2018;19(2):109–114. [PMC free article] [PubMed] [Google Scholar]
- 23.Agharezaee N, Marzbani R, Rezadoost H, Koukhaloo SZ, Arjmand B, Gilany K. Metabolomics: a bird’s eye view of infertile men. Tehran University Medical Journal. 2018;75(12):860–868. [Google Scholar]
- 24.Collins RRJ, Patel K, Putnam WC, Kapur P, Rakheja D. Oncometabolites: a new paradigm for oncology, metabolism, and the clinical laboratory. Clin Chem. 2017;63(12):1812–1820. doi: 10.1373/clinchem.2016.267666. [DOI] [PubMed] [Google Scholar]
- 25.Warburg O, Wind F, Negelein E. The metabolism of tumors in the body. J Gen Physiol. 1927;8(6):519–530. doi: 10.1085/jgp.8.6.519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Zhou Z, Ibekwe E, Chornenkyy Y. Metabolic alterations in cancer cells and the emerging role of Oncometabolites as drivers of neoplastic change. Antioxidants. 2018;7(1):16. doi: 10.3390/antiox7010016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ward PS, Patel J, Wise DR, et al. The Common Feature of Cancer-Associated IDH1 and IDH2 Mutations is a Neomorphic Enzyme Activity Converting α-ketoglutarate to the Oncometabolite 2-Hydroxyglutarate. Cancer Cell. 2010;17(3):225–234. doi: 10.1016/j.ccr.2010.01.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pavlova NN, Thompson CB. The emerging hallmarks of cancer metabolism. Cell Metab. 2016;23(1):27–47. doi: 10.1016/j.cmet.2015.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wishart DS, Mandal R, Stanislaus A, Ramirez-Gaona M. Cancer metabolomics and the human metabolome database. Metabolites. 2016;6(1):10. doi: 10.3390/metabo6010010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Gupta N, Kakar AK, Chowdhury V, Gulati P, Shankar LR, Vindal A. Magnetic resonance spectroscopy as a diagnostic modality for carcinoma thyroid. Eur J Radiol. 2007;64(3):414–418. doi: 10.1016/j.ejrad.2007.03.006. [DOI] [PubMed] [Google Scholar]
- 31.Miccoli P, Torregrossa L, Shintu L, et al. Metabolomics approach to thyroid nodules: a high-resolution magic-angle spinning nuclear magnetic resonance-based study. Surgery. 2012;152(6):1118–1124. doi: 10.1016/j.surg.2012.08.037. [DOI] [PubMed] [Google Scholar]
- 32.Tian Y, Nie X, Xu S, et al. Integrative metabonomics as potential method for diagnosis of thyroid malignancy. Sci Rep. 2015;5:14869. doi: 10.1038/srep14869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ryoo I, Kwon H, Kim SC, et al. Metabolomic analysis of percutaneous fine-needle aspiration specimens of thyroid nodules: Potential application for the preoperative diagnosis of thyroid cancer. Sci Rep. 2016;6(1):30075. doi: 10.1038/srep30075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bae JM. A suggestion for quality assessment in systematic reviews of observational studies in nutritional epidemiology. Epidemiol Health. 2016;38:e2016014. doi: 10.4178/epih.e2016014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lumbreras B, Porta M, Márquez S, Pollán M, Parker LA, Hernández-Aguado I. QUADOMICS: an adaptation of the Quality Assessment of Diagnostic Accuracy Assessment (QUADAS) for the evaluation of the methodological quality of studies on the diagnostic accuracy of “-omics”-based technologies. Clin Biochem. 2008;41(16–17):1316–1325. doi: 10.1016/j.clinbiochem.2008.06.018. [DOI] [PubMed] [Google Scholar]
- 36.Zahid M, Goldner W, Beseler CL, Rogan EG, Cavalieri EL. Unbalanced estrogen metabolism in thyroid cancer. Int J Cancer. 2013;133(11):n/a–9. doi: 10.1002/ijc.28275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Villanueva J, Nazarian A, Lawlor K, Yi SS, Robbins RJ, Tempst P. A sequence-specific exopeptidase activity test (SSEAT) for “functional” biomarker discovery. Mol Cell Proteomics. 2008;7(3):509–518. doi: 10.1074/mcp.M700397-MCP200. [DOI] [PubMed] [Google Scholar]
- 38.Chen G, Wang Y, Qiu L, et al. Human IgG Fc-glycosylation profiling reveals associations with age, sex, female sex hormones and thyroid cancer. J Proteomics. 2012;75(10):2824–2834. doi: 10.1016/j.jprot.2012.02.001. [DOI] [PubMed] [Google Scholar]
- 39.Curry JM, Tassone P, Cotzia P, et al. Multicompartment metabolism in papillary thyroid cancer. Laryngoscope. 2016;126(10):2410–2418. doi: 10.1002/lary.25799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.de Groot JW, Kema IP, Breukelman H, et al. Biochemical markers in the follow-up of medullary thyroid cancer. Thyroid. 2006;16(11):1163–1170. doi: 10.1089/thy.2006.16.1163. [DOI] [PubMed] [Google Scholar]
- 41.Do SI, Kim HS, Kim K, et al. Predictive value of sphingosine kinase 1 expression in papillary thyroid carcinoma. Anticancer Res. 2017;37(10):5399–5405. doi: 10.21873/anticanres.11967. [DOI] [PubMed] [Google Scholar]
- 42.Mittal A, Poudel B, Pandeya DR, Gupta SP, Sathian B, Yadav SK. Metabolic changes enhance the cardiovascular risk with differentiated thyroid carcinoma – a case control study from Manipal Teaching Hospital of Nepal. Asian Pac J Cancer Prev. 2012;13(5):2335–2338. doi: 10.7314/apjcp.2012.13.5.2335. [DOI] [PubMed] [Google Scholar]
- 43.Rajoria S, Suriano R, Parmar PS, et al. 3,3′-diindolylmethane modulates estrogen metabolism in patients with thyroid proliferative disease: a pilot study. Thyroid. 2011;21(3):299–304. doi: 10.1089/thy.2010.0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Shang X, Zhong X, Tian X. Metabolomics of papillary thyroid carcinoma tissues: potential biomarkers for diagnosis and promising targets for therapy. Tumour Biol. 2016;37(8):11163–11175. doi: 10.1007/s13277-016-4996-z. [DOI] [PubMed] [Google Scholar]
- 45.Gu Y, Chen T, Fu S, et al. Perioperative dynamics and significance of amino acid profiles in patients with cancer. J Transl Med. 2015;13(1):35. doi: 10.1186/s12967-015-0408-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lee SH, Kim KM, Jung BH, Chung WY, Park CS, Chung BC. Estrogens in female thyroid cancer: alteration of urinary profiles in pre- and post-operative cases. Cancer Lett. 2003;189(1):27–32. doi: 10.1016/s0304-3835(02)00514-1. [DOI] [PubMed] [Google Scholar]
- 47.Ishikawa S, Tateya I, Hayasaka T, et al. Increased expression of phosphatidylcholine (16:0/18:1) and (16:0/18:2) in thyroid papillary cancer. PLoS One. 2012;7(11):e48873. doi: 10.1371/journal.pone.0048873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Seo JW, Han K, Lee J, et al. Application of metabolomics in prediction of lymph node metastasis in papillary thyroid carcinoma. PLoS One. 2018;13(3):e0193883. doi: 10.1371/journal.pone.0193883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Zhou J, Li Y, Chen X, Zhong L, Yin Y. Development of data-independent acquisition workflows for metabolomic analysis on a quadrupoleorbitrap platform. Talanta. 2017;164:128–136. doi: 10.1016/j.talanta.2016.11.048. [DOI] [PubMed] [Google Scholar]
- 50.Zhao WX, Wang B, Zhang LY, Yan SY, Yang YH. Analysis on the metabolite composition of serum samples from patients with papillary thyroid carcinoma using nuclear magnetic resonance. Int J Clin Exp Med. 2015;8(10):18013. [PMC free article] [PubMed] [Google Scholar]
- 51.Zhang J, Feider CL, Nagi C, et al. Detection of metastatic breast and thyroid cancer in lymph nodes by desorption electrospray ionization mass spectrometry imaging. J Am Soc Mass Spectrom. 2017;28(6):1166–1174. doi: 10.1007/s13361-016-1570-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Yao Z, Yin P, Su D, et al. Serum metabolic profiling and features of papillary thyroid carcinoma and nodular goiter. Mol Biosyst. 2011;7(9):2608–2614. doi: 10.1039/c1mb05029j. [DOI] [PubMed] [Google Scholar]
- 53.Xu Y, Zheng X, Qiu Y, Jia W, Wang J, Yin S. Distinct metabolomic profiles of papillary thyroid carcinoma and benign thyroid adenoma. J Proteome Res. 2015;14(8):3315–3321. doi: 10.1021/acs.jproteome.5b00351. [DOI] [PubMed] [Google Scholar]
- 54.Wojtowicz W, Zabek A, Deja S, et al. Serum and urine 1H NMR-based metabolomics in the diagnosis of selected thyroid diseases. Sci Rep. 2017;7(1):9108. doi: 10.1038/s41598-017-09203-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Choi MH, Moon JY, Cho SH, Chung BC, Lee EJ. Metabolic alteration of urinary steroids in pre- and post-menopausal women, and men with papillary thyroid carcinoma. BMC Cancer. 2011;11(1):342. doi: 10.1186/1471-2407-11-342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Chen M, Shen M, Li Y, et al. GC-MS-based metabolomic analysis of human papillary thyroid carcinoma tissue. Int J Mol Med. 2015;36(6):1607–1614. doi: 10.3892/ijmm.2015.2368. [DOI] [PubMed] [Google Scholar]
- 57.Ryoo I, Kwon H, Kim SC, et al. Metabolomic analysis of percutaneous fine-needle aspiration specimens of thyroid nodules: potential application for the preoperative diagnosis of thyroid cancer. Sci Rep. 2016;6(1):30075. doi: 10.1038/srep30075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Shen CT, Zhang Y, Liu YM, et al. A distinct serum metabolic signature of distant metastatic papillary thyroid carcinoma. Clin Endocrinol. 2017;87(6):844–852. doi: 10.1111/cen.13437. [DOI] [PubMed] [Google Scholar]
- 59.Torregrossa L, Shintu L, Nambiath Chandran J, et al. Toward the reliable diagnosis of indeterminate thyroid lesions: a HRMAS NMR-based metabolomics case of study. J Proteome Res. 2012;11(6):3317–3325. doi: 10.1021/pr300105e. [DOI] [PubMed] [Google Scholar]
- 60.Guo L, Wang C, Chi C, et al. Exhaled breath volatile biomarker analysis for thyroid cancer. Transl Res. 2015;166(2):188–195. doi: 10.1016/j.trsl.2015.01.005. [DOI] [PubMed] [Google Scholar]
- 61.Liu S, Zhao G, Li J, et al. Association of polybrominated diphenylethers (PBDEs) and hydroxylated metabolites (OH-PBDEs) serum levels with thyroid function in thyroid cancer patients. Environ Res. 2017;159:1–8. doi: 10.1016/j.envres.2017.07.042. [DOI] [PubMed] [Google Scholar]
- 62.Lu J, Hu S, Miccoli P, et al. Non-invasive diagnosis of papillary thyroid microcarcinoma: a NMR-based metabolomics approach. Oncotarget. 2016;7(49):81768. doi: 10.18632/oncotarget.13178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Deja S, Dawiskiba T, Balcerzak W, et al. Follicular adenomas exhibit a unique metabolic profile. 1H NMR studies of thyroid lesions. PLoS One. 2013;8(12):e84637. doi: 10.1371/journal.pone.0084637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100(1):57–70. doi: 10.1016/s0092-8674(00)81683-9. [DOI] [PubMed] [Google Scholar]
- 65.Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi: 10.1016/j.cell.2011.02.013. [DOI] [PubMed] [Google Scholar]
- 66.Warburg O. Über den Stoffwechsel der Carcinomzelle. Naturwissenschaften. 1924;12(50):1131–1137. [Google Scholar]
- 67.Warburg O. On the origin of cancer cells. Science. 1956;123(3191):309–314. doi: 10.1126/science.123.3191.309. [DOI] [PubMed] [Google Scholar]
- 68.Volk T, Jähde E, Fortmeyer HP, Glüsenkamp KH, Rajewsky MF. pH in human tumour xenografts: effect of intravenous administration of glucose. Br J Cancer. 1993;68(3):492–500. doi: 10.1038/bjc.1993.375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Delli Castelli D, Ferrauto G, Cutrin JC, Terreno E, Aime S. In vivo maps of extracellular pH in murine melanoma by CEST-MRI. Magn Reson Med. 2014;71(1):326–332. doi: 10.1002/mrm.24664. [DOI] [PubMed] [Google Scholar]
- 70.Fadaka A, Ajiboye B, Ojo O, Adewale O, Olayide I, Emuowhochere R. Biology of glucose metabolization in cancer cells. J Oncol Sci. 2017;3(2):45–51. [Google Scholar]
- 71.Hamanaka RB, Chandel NS. Targeting glucose metabolism for cancer therapy. J Exp Med. 2012;209(2):211–215. doi: 10.1084/jem.20120162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lee AS. Glucose-regulated proteins in cancer: molecular mechanisms and therapeutic potential. Nat Rev Cancer. 2014;14(4):263–276. doi: 10.1038/nrc3701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Wolf A, Agnihotri S, Micallef J, et al. Hexokinase 2 is a key mediator of aerobic glycolysis and promotes tumor growth in human glioblastoma multiforme. J Exp Med. 2011;208(2):313–326. doi: 10.1084/jem.20101470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Shen C-T, Zhang Y, Liu Y-M, et al. A distinct serum metabolic signature of distant metastatic papillary thyroid carcinoma. Clin Endocrinol. 2017;87(6):844–852. doi: 10.1111/cen.13437. [DOI] [PubMed] [Google Scholar]
- 75.Gu Y, Chen T, Fu S, et al. Perioperative dynamics and significance of amino acid profiles in patients with cancer. J Transl Med. 2015;13(1):35. doi: 10.1186/s12967-015-0408-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Zhao WX, Wang B, Zhang LY, Yan SY, Yang YH. Analysis on the metabolite composition of serum samples from patients with papillary thyroid carcinoma using nuclear magnetic resonance. Int J Clin Exp Med. 2015;8(10):18013–18022. [PMC free article] [PubMed] [Google Scholar]
- 77.Wojtowicz W, Zabek A, Deja S, et al. Serum and urine 1H NMR-based metabolomics in the diagnosis of selected thyroid diseases. Sci Rep. 2017;7(1):9108. doi: 10.1038/s41598-017-09203-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Miyoshi E, Ito Y, Miyoshi Y. Involvement of aberrant glycosylation in thyroid cancer. J Oncol. 2010;2010(2):1–7. doi: 10.1155/2010/816595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Plomp R, Ruhaak LR, Uh HW, et al. Subclass-specific IgG glycosylation is associated with markers of inflammation and metabolic health. Sci Rep. 2017;7(1):12325. doi: 10.1038/s41598-017-12495-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Zhang D, Chen B, Wang Y, et al. Disease-specific IgG Fc N-glycosylation as personalized biomarkers to differentiate gastric cancer from benign gastric diseases. Sci Rep. 2016;6(1):25957. doi: 10.1038/srep25957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Pinho SS, Reis CA. Glycosylation in cancer: mechanisms and clinical implications. Nat Rev Cancer. 2015;15(9):540–555. doi: 10.1038/nrc3982. [DOI] [PubMed] [Google Scholar]
- 82.Ząbczyńska M, Kozłowska K, Pocheć E. Glycosylation in the thyroid gland: vital aspects of glycoprotein function in thyrocyte physiology and thyroid disorders. Int J Mol Sci. 2018;19(9):2792. doi: 10.3390/ijms19092792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Brizel DM, Schroeder T, Scher RL, et al. Elevated tumor lactate concentrations predict for an increased risk of metastases in head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2001;51(2):349–353. doi: 10.1016/s0360-3016(01)01630-3. [DOI] [PubMed] [Google Scholar]
- 84.Walenta S, Schroeder T, Mueller-Klieser W. Lactate in solid malignant tumors: potential basis of a metabolic classification in clinical oncology. Curr Med Chem. 2004;11(16):2195–2204. doi: 10.2174/0929867043364711. [DOI] [PubMed] [Google Scholar]
- 85.Koppenol WH, Bounds PL, Dang CV. Otto Warburg’s contributions to current concepts of cancer metabolism. Nat Rev Cancer. 2011;11(5):325–337. doi: 10.1038/nrc3038. [DOI] [PubMed] [Google Scholar]
- 86.Rogatzki MJ, Ferguson BS, Goodwin ML, Gladden LB. Lactate is always the end product of glycolysis. Front Neurosci. 2015;9(408):22. doi: 10.3389/fnins.2015.00022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Michiels C. Physiological and pathological responses to hypoxia. Am J Pathol. 2004;164(6):1875–1882. doi: 10.1016/S0002-9440(10)63747-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.San-Millán I, Brooks GA. Reexamining cancer metabolism: lactate production for carcinogenesis could be the purpose and explanation of the Warburg Effect. Carcinogenesis. 2017;38(2):119–133. doi: 10.1093/carcin/bgw127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Romero-Garcia S, Moreno-Altamirano MM, Prado-Garcia H, Sánchez-García FJ. Lactate contribution to the tumor microenvironment: mechanisms, effects on immune cells and therapeutic relevance. Front Immunol. 2016;7(Pt 2):52. doi: 10.3389/fimmu.2016.00052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Jiang B. Aerobic glycolysis and high level of lactate in cancer metabolism and microenvironment. Genes Dis. 2017;4(1):25–27. doi: 10.1016/j.gendis.2017.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ridgway ND. The role of phosphatidylcholine and choline metabolites to cell proliferation and survival. Crit Rev Biochem Mol Biol. 2013;48(1):20–38. doi: 10.3109/10409238.2012.735643. [DOI] [PubMed] [Google Scholar]
- 92.Li Y, Chen M, Liu C, et al. Metabolic changes associated with papillary thyroid carcinoma: a nuclear magnetic resonance-based metabolomics study. Int J Mol Med. 2018;41(5):3006–3014. doi: 10.3892/ijmm.2018.3494. [DOI] [PubMed] [Google Scholar]
- 93.Kwon H, Oh S, Jin X, An YJ, Park S. Cancer metabolomics in basic science perspective. Arch Pharm Res. 2015;38(3):372–380. doi: 10.1007/s12272-015-0552-4. [DOI] [PubMed] [Google Scholar]
- 94.Jain M, Nilsson R, Sharma S, et al. Metabolite profiling identifies a key role for glycine in rapid cancer cell proliferation. Science. 2012;336(6084):1040–1044. doi: 10.1126/science.1218595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Zhang WC, Shyh-Chang N, Yang H, et al. Glycine decarboxylase activity drives non-small cell lung cancer tumor-initiating cells and tumorigenesis. Cell. 2012;148(1–2):259–272. doi: 10.1016/j.cell.2011.11.050. [DOI] [PubMed] [Google Scholar]
- 96.Mycielska ME, Dettmer K, Rümmele P, et al. Extracellular citrate affects critical elements of cancer cell metabolism and supports cancer development In Vivo. Cancer Res. 2018;78(10):2513–2523. doi: 10.1158/0008-5472.CAN-17-2959. [DOI] [PubMed] [Google Scholar]
- 97.Hatzivassiliou G, Zhao F, Bauer DE, et al. ATP citrate lyase inhibition can suppress tumor cell growth. Cancer Cell. 2005;8(4):311–321. doi: 10.1016/j.ccr.2005.09.008. [DOI] [PubMed] [Google Scholar]
- 98.Zaidi N, Swinnen JV, Smans K. ATP-citrate lyase: a key player in cancer metabolism. Cancer Res. 2012;72(15):3709–3714. doi: 10.1158/0008-5472.CAN-11-4112. [DOI] [PubMed] [Google Scholar]
- 99.Ren JG, Seth P, Ye H, et al. Citrate suppresses tumor growth in multiple models through inhibition of glycolysis, the tricarboxylic acid cycle and the IGF-1R pathway. Sci Rep. 2017;7(1):4537. doi: 10.1038/s41598-017-04626-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Dang L, Yen K, Attar EC. IDH mutations in cancer and progress toward development of targeted therapeutics. Ann Oncol. 2016;27(4):599–608. doi: 10.1093/annonc/mdw013. [DOI] [PubMed] [Google Scholar]
- 101.Ye D, Guan KL, Xiong Y. Metabolism, activity, and targeting of D- and L-2-hydroxyglutarates. Trends Cancer. 2018;4(2):151–165. doi: 10.1016/j.trecan.2017.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Ward PS, Cross JR, Lu C, et al. Identification of additional IDH mutations associated with oncometabolite R(-)-2-hydroxyglutarate production. Oncogene. 2012;31(19):2491–2498. doi: 10.1038/onc.2011.416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Choi C, Ganji SK, Deberardinis RJ, et al. 2-hydroxyglutarate detection by magnetic resonance spectroscopy in IDH-mutated patients with gliomas. Nat Med. 2012;18(4):624–629. doi: 10.1038/nm.2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Gross S, Cairns RA, Minden MD, et al. Cancer-associated metabolite 2-hydroxyglutarate accumulates in acute myelogenous leukemia with isocitrate dehydrogenase 1 and 2 mutations. J Exp Med. 2010;207(2):339–344. doi: 10.1084/jem.20092506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Shim EH, Livi CB, Rakheja D, et al. L-2-Hydroxyglutarate: an epi-genetic modifier and putative oncometabolite in renal cancer. Cancer Discov. 2014;4(11):1290–1298. doi: 10.1158/2159-8290.CD-13-0696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Rakheja D, Boriack RL, Mitui M, Khokhar S, Holt SA, Kapur P. Papillary thyroid carcinoma shows elevated levels of 2-hydroxyglutarate. Tumour Biol. 2011;32(2):325–333. doi: 10.1007/s13277-010-0125-6. [DOI] [PubMed] [Google Scholar]
- 107.Hemerly JP, Bastos AU, Cerutti JM. Identification of several novel non-p.R132 IDH1 variants in thyroid carcinomas. Eur J Endocrinol. 2010;163(5):747–755. doi: 10.1530/EJE-10-0473. [DOI] [PubMed] [Google Scholar]
- 108.Ward PS, Lu C, Cross JR, et al. The potential for isocitrate dehydrogenase mutations to produce 2-hydroxyglutarate depends on allele specificity and subcellular compartmentalization. J Biol Chem. 2013;288(6):jbc. M112:3804–3815. doi: 10.1074/jbc.M112.435495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Alimoghaddam K, Shariftabrizi A, Tavangar SM, et al. Anti-leukemic and anti-angiogenesis efficacy of arsenic trioxide in new cases of acute promyelocytic leukemia. Leuk Lymphoma. 2006;47(1):81–88. doi: 10.1080/10428190500300373. [DOI] [PubMed] [Google Scholar]
- 110.Miller VM. Estrogen metabolomics: a physiologist’s perspective. Hypertension. 2010;56(5):816–818. doi: 10.1161/HYPERTENSIONAHA.110.154385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Alakwaa FM, Chaudhary K, Garmire LX. Deep learning accurately predicts estrogen receptor status in breast cancer metabolomics data. J Proteome Res. 2018;17(1):337–347. doi: 10.1021/acs.jproteome.7b00595. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Tong X, Zhao F, Thompson CB. The molecular determinants of de novo nucleotide biosynthesis in cancer cells. Curr Opin Genet Dev. 2009;19(1):32–37. doi: 10.1016/j.gde.2009.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Mannava S, Grachtchouk V, Wheeler LJ, et al. Direct role of nucleotide metabolism in C-MYC-dependent proliferation of melanoma cells. Cell Cycle. 2008;7(15):2392–2400. doi: 10.4161/cc.6390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Cory JG, Cory AH. Critical roles of glutamine as nitrogen donors in purine and pyrimidine nucleotide synthesis: asparaginase treatment in childhood acute lymphoblastic leukemia. In Vivo. 2006;20(5):587–589. [PubMed] [Google Scholar]
- 115.Cantor JR, Sabatini DM. Cancer cell metabolism: one hallmark, many faces. Cancer Discov. 2012;2(10):881–898. doi: 10.1158/2159-8290.CD-12-0345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Wise DR, Thompson CB. Glutamine addiction: a new therapeutic target in cancer. Trends Biochem Sci. 2010;35(8):427–433. doi: 10.1016/j.tibs.2010.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Khatami F, Larijani B, Heshmat R, Keshtkar A, Mohammadamoli M, Teimoori-Toolabi L, Nasiri S, Tavangar SM. Meta-analysis of promoter methylation in eight tumor-suppressor genes and its association with the risk of thyroid cancer. Plos One. 2017;12(9):e0184892. doi: 10.1371/journal.pone.0184892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Natanzi MM, Pasalar P, Kamalinejad M, Dehpour AR, Tavangar SM, Sharifi R, Ghanadian N, Rahimi-Balaei M, Gerayesh-Nejad S. Effect of aqueous extract of Elaeagnus angustifolia fruit on experimental cutaneous wound healing in rats. Acta Medica Iranica. 2012;50(9):589–596. [PubMed] [Google Scholar]
- 119.Omidfar K, Moinfar Z, Sohi AN, Tavangar SM, Haghpanah V, Heshmat R, Kashanian S, Larijani B. Expression of EGFRvIII in thyroid carcinoma: immunohistochemical study by camel antibodies. Immunological Investigations. 2009 Jan 1;38(2):165–80. doi: 10.1080/08820130902735998. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.