

Abstract
Heart failure is a clinical condition with complex pathophysiology that involves many different processes. Diagnosis is often difficult in patients presenting for the first time with breathlessness. Many biomarkers have been identified that are elevated in heart failure and their role in assessing prognosis has also been investigated. However, at present the natriuretic peptides appear to be the gold standard biomarker against which the other biomarkers are compared. In this review we will examine the evidence behind the other biomarkers for use in heart failure patients and the current guidelines for their use.
Keywords: Acute heart failure, chronic heart failure, biomarkers, natriuretic peptides, troponin, Nprognosis, diagnosis
The National Institutes of Health Biomarkers Definitions Working Group define a biomarker as “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention”.[1] Biomarkers have become increasingly important in current medical practice as they offer an easy way to either diagnose an illness or to monitor progress. Tijsen et al. have suggested that an ideal biomarker ought to be easy to collect non-invasively, should have a high degree of sensitivity and specificity, should be cheap, easily reproducible and should have a rapid measurement system that assists in prompt clinical management.[2]
For patients presenting with breathlessness, there is a need for a reliable biomarker for the early diagnosis of heart failure. Previous studies have demonstrated a high degree of uncertainty when patients present with breathlessness.[3] Heart failure and chronic obstructive airway disease often coexist in approximately 30% of patients, making diagnosis confusing. The Breathing Not Properly study reported clinical confusion in approximately half of cases presenting to the emergency department with breathlessness.[4] Echocardiography can detect abnormal left ventricular (LV) function, but that may not be the cause of breathlessness because almost 50% of the community-dwelling population with decreased LV function have been shown to be asymptomatic.[5] Hence there is a need for a biomarker that could assist in diagnosis.
Similarly, there is also a need for better monitoring of patients receiving treatment for heart failure. It has been demonstrated that physiological changes often precede clinical deterioration that would lead to a patient attending hospital.[6] Invasive mechanisms such as pacemaker devices with physiological monitoring mechanisms can alert the physician to clinical deterioration.[7] However, these are invasive and not all patients with heart failure have a pacemaker. Non-invasive means such as a biomarker have therefore become useful.
There are many potential biomarkers for heart failure (Figure 1). In this article, we discuss the biomarkers that are available for clinical use in patients with heart failure — both for diagnosis and prognosis — reviewing the evidence and the recommendations of various guidelines. Furthermore, we will highlight some of the emerging biomarkers in this field, along with the evidence for their use.
Figure 1: Different Potential Biomarkers in the Diagnosis and Management of Heart Failure.
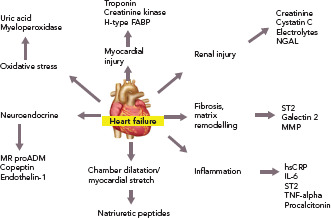
FABP = fatty acid binding protein; hsCRP = high sensitivity C-reactive protein; IL = interleukin; MMP = matrix metalloproteinase; NGAL = neutrophil gelatinase associated lipocalin; ST2 = suppression of tumourigenicity-2; TNF = tumour necrosis factor.
Biomarkers for Diagnosis
The diagnosis of heart failure in a patient presenting with breathlessness for the first time is often difficult, and biomarkers — along with other investigations — can contribute to diagnosis. Traditionally, clinical presentation along with chest X-ray has been used to make a diagnosis of heart failure. However, studies have repeatedly shown a low sensitivity and specificity for making a clinical diagnosis of heart failure. Echocardiography is a useful component of diagnosis, but in the acute setting it may not always be possible to obtain an echocardiogram, particularly out of hours. Additionally, the echocardiogram may be normal in heart failure with preserved ejection fraction (HFpEF).
The natriuretic peptides are the most extensively studied and used biomarkers in heart failure.[8] As a result of myocardial stretch, the B-type natriuretic peptide (BNP) gene is activated and prohormone proBNP1–108 is produced. This is cleaved to the biologically active BNP and the biologically inert but stable NT-proBNP1–76. They down-regulate the sympathetic system, cause diuresis, decrease peripheral resistance and increase smooth muscle relaxation (Figure 2). Atrial natriuretic peptide (ANP) as rapid clearance and is less consistent as a diagnostic marker and hence is not used routinely. However, newer assays have been developed that measure the precursor hormone of ANP, mid-regional proANP (MR-proANP). MR-proANP is more stable, giving more reliable results, and has therefore been identified as a reliable marker. The pharmacokinetics of these molecules is shown in Table 1.[9]
Figure 2: Activation of the B-type Natriuretic Peptide.
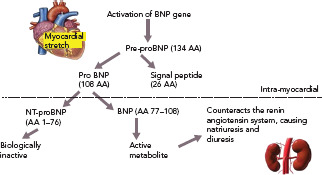
AA = amino acid; BNP = B-type natriuretic peptide; NT-proBNP = N-terminal-proBNP.
Table 1: Pharmacokinetics of the Natriuretic Peptides.
| Natriuretic Peptide | Production | Half-life | Clearance |
|---|---|---|---|
| B-type natriuretic peptide (BNP) | Produced from pre-proBNP, which is released from myocytes under stress. | 20 min | Endocytosis, renal filtration or passive excretion |
| N-terminal-proBNP | Produced from proBNP, formed mainly in the left ventricle. | 60–90 min | Renal excretion |
| Atrial natriuretic peptide | Produced by muscle cells in the atrial wall as a result of stretch. | 1 min | Renal clearance of its metabolites |
The Breathing Not Properly Study was one of the first major trials studying the role of natriuretic peptides in the emergency department for the diagnosis of heart failure.[10]Here the authors measured BNP levels in 1,586 patients presenting to the emergency department with acute breathlessness. Patients with clinically diagnosed heart failure had higher BNP levels compared with those without heart failure (mean 675 ± 450 pg/ml versus 110 ± 225 pg/ml; p=0.001). Increasing severity of heart failure, as measured by New York Heart Association (NYHA) functional class, correlated directly with increasing concentrations of BNP (p<0.001). BNP was the best single predictor of a final diagnosis of heart failure compared with all individual history, physical examination, chest x-ray and laboratory findings. A cut-off BNP value of 100 pg/ml had a sensitivity of 90% and a specificity of 76%. In addition, BNP was more accurate (83%) than either the National Health and Nutrition Examination Survey criteria (67%) or the Framingham criteria (73%), two established criteria for heart failure diagnosis. Importantly, the best method of diagnosis of heart failure was seen when BNP and clinical findings were combined.
The use of NT-proBNP in the diagnosis of acutely decompensated heart failure was first demonstrated in the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) study.[11] Here, NT-proBNP had a high sensitivity for the diagnosis of heart failure, again supplementing clinical judgment as BNP did in the Breathing Not Properly study. Subsequently, the International Collaborative Of NT-proBNP (ICON) study examined optimal applications of NT-proBNP in 1256 acutely dyspnoeic patients.[12] Patients with acutely decompensated heart failure had considerably higher NT-proBNP concentrations compared with those without heart failure (4,639 pg/ml versus 108 pg/ml; p<0.001) and symptom severity correlated with NT-proBNP concentrations (p=0.008). As natriuretic peptide concentrations rise with increasing age, the ICON investigators found the best approach for use of NT-proBNP in heart failure diagnosis was through use of age-stratified cut-off points; this approach improved the positive predictive value of the assay considerably.
The utility of MR-proANP in the diagnosis of heart failure was demonstrated in the Biomarkers In Acute Heart Failure (BACH) study.[13] In the diagnosis of acute heart failure in those presenting to the emergency department with dyspnoea, a MR-proANP level greater than the predefined cut point of 120 pmol/l was found to be non-inferior to BNP at the 100 pg/ml cut point. Combining MR-proANP and BNP increased diagnostic accuracy from 73.6% with BNP alone to 76.6%. It was also found that in cases where BNP and NT-proBNP could be less informative (obesity, old age, renal dysfunction or ‘grey zone’ values), MR-proANP added value when used in combination with each biomarker. Thus it has been suggested that the addition of MR-proANP with other natriuretic peptides adds to diagnostic accuracy.
It should be remembered that there are many other causes of raised natriuretic peptides besides heart failure.[14] These include cardiac causes such as acute coronary syndrome, myocarditis, cardioversion etc., along with non-cardiac causes such as age, anaemia and renal failure. Conversely, obesity has been shown to decrease natriuretic peptide levels.[14]
Kim and Januzzi have suggested cut-off points for different scenarios.[14] For BNP, they have suggested a ‘grey zone’ approach. A value of <100 pg/ml would exclude heart failure and >400 pg/ml would confirm heart failure. For those in the ‘grey zone’ of 100–400 pg/ml, further tests would be required. For NT proBNP, an age-stratified approach is suggested. Values <450 pg/ml would be used as a cut-off for patients aged <50 years, <900 pg/ml for those aged 50–75 years and <1,800 pg/ml for those aged >75 years. In patients with renal dysfunction, (glomerular filtration rate <60 ml/min/1.73 m2), a BNP cut-off value of 200 pg/ml or NT-proBNP of <1,200 pg/ml should be used. Similarly, different cut-off values for BNP have been suggested based on BMI. A cut-off of 170 pg/ml is recommended for BMI <25 kg/m2, 110 pg/ml for BMI 25–35 kg/m2 and 54 pg/ml for BMI >35 kg/m2. No correction is required for NT-proBNP based on BMI. All these values have a high sensitivity and specificity.
Among the other non-natriuretic-peptide biomarkers, the troponins are often elevated in patients with heart failure.[15] However they only represent myocardial injury and are therefore not specific for making a diagnosis of heart failure. They could also be increased in any condition that puts increased stress on the heart muscle. They may also be useful in diagnosing concomitant acute coronary syndromes in the presence of heart failure.[16]
Similarly, biomarkers, such as soluble suppression of tumourigenicity-2 (ST2), galectin-3 and pro-adrenomedullin, are also increased in patients with heart failure.[17] However, they are not useful for the diagnosis of heart failure as they are not specific for these patients and are increased in other conditions as well.[18] Their characteristics are summarised in Table 2 and are discussed in detail in the prognosis section.
Table 2: Characteristics of Other Biomarkers for Heart Failure.
| Biomarker | Physiological Actions | Conditions Where it is Increased | Cardiac Actions | Role in Heart Failure Management |
|---|---|---|---|---|
| Galectin-3[69] | Mediator of tumour growth and metastasis | Increasing age, diabetic nephropathy, fibrotic conditions of liver and lung, chronic pancreatitis | Promotes cardiac fibroblast proliferation, collagen deposition and ventricular dysfunction | Diagnostic capability = no Prognostic capability = yes |
| Neutrophil gelatinase associated lipocalin (NGAL)[70] | Produced by neutrophils and endothelial cells as an acute phase protein | Earliest marker of nephrotoxic or ischaemic renal injury | Action on the heart unknown, but levels increase in acute heart failure even in the presence of normal renal function | Diagnostic capability = yes Prognostic capability = yes |
| mid-regional pro-adrenomedullin (MR-ProADM)[71] | First found in pheochromocytoma cells. They have vasodilatory effects and increase nitric oxide synthesis | Increases myocardial contractility via a cyclic AMP-independent mechanism. Also causes vasodilatation and increases cardiac index | Diagnostic capability = no Prognostic capability = yes |
The American and European guidelines on the management of heart failure both give measuring natriuretic peptides for the diagnosis of heart failure a class 1A recommendation.[19,20] The European guidelines recommended that the upper limit of normal in a non-acute setting is 35 pg/ml for BNP and 125 pg/ml for NT-proBNP. In the acute setting, the cut-off values are higher at 100 pg/ml for BNP and 300 pg/ml for NT-proBNP. At these cut-off values the negative predictive values are similar and high at 0.94–0.98 in both the acute and non-acute settings but the positive predictive values are low. Therefore it has been suggested that the use of the natriuretic peptides are mainly for ruling out a diagnosis of heart failure rather than establishing it, when there is clinical uncertainty. However, at higher natriuretic peptide values, the positive predictive value is high. The American guidelines do not specify any cut-off values. Both sets of guidelines mention that other biomarkers are elevated in acute or stable heart failure, but they do not recommend their routine use for the diagnosis of heart failure.
Biomarkers for Prognosis
The natriuretic peptides again are the most extensively investigated biomarker for assessing prognosis of patients with heart failure — both in the acute setting as well as for patients with chronic heart failure seen in the office setting. It has been shown that at baseline, the higher the BNP, the worse the prognosis, with patients having almost a five-fold greater mortality between the highest and lowest tertiles.[21]
In patients admitted with heart failure, the risk of readmission and death is high if the discharge BNP is not lower than the admission value.[22] Many of the large heart failure studies have also examined the role of biomarkers in prognosis. In the Valsartan Heart Failure Trial (Val-HEFT), patients with the greatest fall in BNP with treatment had the best prognosis.[3] Similarly, in the Organized Program To Initiate Lifesaving Treatment In Hospitalized Patients With Heart Failure (OPTIMIZE-HF) study, discharge BNP was shown to affect prognosis.[24] A meta analysis by Doust et al. found that for every 100 pg/ml increase in BNP there was a 35% increase in the risk of death.[25]
In the Framingham study, it was shown that even in asymptomatic patients without overt heart failure, every standard deviation of the log BNP value was associated with a 27% increase in the risk of death, 28% increase in first cardiovascular event, 77% increase in the risk of heart failure, 66% increase in AF and a 53% increase in stroke/transient ischaemic attack.[26] However there was no relation with coronary artery events. Similar results were also obtained from community-dwelling populations in the Omsted county study.[27]
In a comparison of NT-proBNP and MR-proANP using a sample of 525 chronic heart failure patients of all NYHA classes, MR-proANP was found to be positively correlated with NYHA class, and — after correction for NT-proBNP, age, ejection fraction, NYHA class, creatinine, and BMI — MR-proANP was found to be a predictor of poor survival.[28] In the PRIDE study, elevated MR-proANP was independently prognostic and reclassified mortality risk at 1 year (HR 2.00; p<0.001) and at 4 years (HR 3.12; p=0.001).[29] MR-proANP was also associated with death up to 4 years, both alone and with other biomarkers. In chronic heart failure, the Gruppo Italiano Perlo Stuio Della Sopravvivenza Nell’insufficienza Cardiaca Heart Failure (GISSI-HF) study,[30] showed that the prognostic accuracy for MR-proANP for mortality was best with an area under the curve (AUC) of 0.74 (95% CI [0.71–0.77]) with an optimal cut-off point of 278 pmol/l, followed by NT-proBNP with an AUC of 0.73 (95% CI [0.70–0.76]) and an optimal cut-off of 1,181 pg/mol. Changes in MR-proANP over 3 months also appeared to be predictive of future mortality.
Among the other non-natriuretic-peptide biomarkers, high baseline troponin corresponded to a worse prognosis with an OR of 2.5 for death within a year.[31] Serial measurements of high sensitivity troponins (hsTn) during a hospitalisation for acute heart failure can risk stratify patients for 90-day mortality and readmission.[15] It has been shown that patients whose discharge troponin value rose compared with the admission value had the greatest risk.[32] Another study showed that an elevated hsTn as well as a >20% increase in the value was associated with increased mortality.[33] The prognostic value is enhanced when combined with natriuretic peptides.[34] Here the troponins are likely to reflect the level of myocardial strain and stress secondary to the heart failure rather than a coexisting acute coronary syndrome.
Adrenomedullin (ADM) is a 52-amino acid peptide thought to be upregulated as a result of increased volume overload and is mediated by vasoactive hormones. However, because of its rapid clearance from the circulation and short half-life (22 minutes), using ADM as a routine biomarker is impractical. MR-proADM, the mid-regional segment of ADM’s precursor pre-proADM, is released in equimolar concentrations as ADM and thus is an effective substitute, and because of its inactivity and longer half-life, MR-proADM is a better surrogate marker. The BACH trial[13] ADM appeared to predict 90-day mortality or rehospitalisation due to cardiovascular causes better than BNP/proBNP. Similar results were also reported by Klip et al.[35] ADM was also found to be predictive of mortality in a cohort of community-dwelling patients.[36]
Other biomarkers, including ST2, have been shown to be associated with adverse outcomes in heart failure and predict mortality risk in these patients. It is also known as interleukin-1 receptor-like 1, and is a member of the interleukin-1 receptor family.[37] In the PRIDE study[17] ST2 values >0.20 ng/ml had an increased risk of death at 1 year. It was better than other biomarkers in both acute and chronic heart failure in predicting prognosis and works synergistically with the natriuretic peptides to enhance mortality prediction in acute and chronic heart failure. Similarly, in the Val-HEFT study, change in ST2 values over time was significantly and independently associated with mortality.[38] It has also been shown to be predictive of mortality and cardiovascular events in non-ischaemic dilated cardiomyopathy.[39] Some of the important trials highlighting the usefulness of ST2 are summarised in Table 3
Table 3: Studies Involving the Biomarker ST2.
| Study | Number of Patients | Patient Group | Findings |
|---|---|---|---|
| PRIDE[17] | 593 | Patients admitted to the ER with breathlessness | Inferior to NPs for the diagnosis of heart failure, but higher ST2 values associated with worse NYHA class and symptoms. Values also correlate with risk of death at 1 year |
| Rehman et al.[72] | 346 | Acute heart failure | Patients with higher values were more likely to die in one year, with a two fold increased risk of mortality compared with those with normal values. When ST2 values were low, NPs did not predict mortality |
| Boisot et al.[73] | 150 | Acute decompensated heart failure | Values decrease with treatment and patients with a rapid decrease had better outcomes. Percentage change with treatment was predictive of 90-day mortality |
| MERLIN-TIMI 36[74] | 4426 | NSTE-ACS | Weak correlation with NPs and troponins but strongly predictive of the risk of heart failure after NSTE-ACS |
| TIME-CHF[57] | 458 (HFrEF) 112 (HFpEF) |
Acute heart failure | ST2 levels significantly higher in HFpEF than in HFrEF patients. Similar effect on predicting prognosis in both groups |
HFpEF = heart failure with preserved ejection fraction; HFrEF = heart failure with reduced ejection fraction; MERLIN-TIMI = Metabolic Efficiency With Ranolazine For Less Ischemia In Non-ST Elevation Acute Coronary Syndromes - Thrombolysis In Myocardial Infarction; NP = natriuretic peptide; NSTE-ACS = non ST segment elevation acute coronary syndrome; NYHA = New York Heart Association; PRIDE = ProBNP Investigation Of Dyspnea In The Emergency Department; ST2 = soluble suppression of tumourigenicity-2; TIME-CHF = Trial of Intensified Versus Standard Medical Therapy In Elderly Patients With Congestive Heart Failure.
Galectin-3 is secreted by activated macrophages and causes cardiac fibrosis by proliferation of cardiac fibroblasts.[40] It also regulates inflammation, immunity and cancer, and can act as a surrogate marker of cardiac remodelling and the fibrosis that is seen in heart failure. It has not been shown to be useful in diagnosis, but has strong prognostic value. In the Pravastatin Or Atorvastatin Evaluation And Infection Therapy — Thrombolysis In MI 22 (PROVE-IT-TIMI 22) study,[41] higher galectin-3 levels correlated with the development of heart failure. Similarly, in the Coordinating Study Evaluating Outcomes Of Advising And Counselling In Heart Failure (COACH) trial,higher levels increased the risk of death or rehospitalisation over 18 months.[42] Its value also correlated with inflammatory markers such as C-reactive protein, vascular endothelial growth factor and interleukin-6. It has also been shown to predict mortality in non-ischaemic dilated cardiomyopathy.[39,43]
Numerous studies however have shown that when more than one biomarker is studied, they predict prognosis much better than the individual markers alone. For example, Gaggin et al. demonstrated that a model that contains clinical data, NT-proBNP, hsTn1 and ST2 along with endothelin-1, had a very good predictive value.[44] This is understandable because each of these markers studies the impact of heart failure on various different pathophysiological processes that comprise heart failure.
The American heart failure guidelines recommend the use of natriuretic peptides and troponins for risk stratification and for determining prognosis in both acute and ambulatory patients with heart failure.[19] The European guidelines mention the role of biomarkers in determining prognosis, but do not issue any specific recommendations.[20]
Biomarkers as a Guide For Therapy
Studies have consistently shown that patients whose BNP or NT-proBNP values show greater reductions tend to have better prognosis.[23] It would therefore appear logical that we could use BNP values to guide therapy with frequent monitoring of the values to assess whether patients need more intense heart failure treatment.[45] However, results have been conflicting and not entirely as expected.
Early studies were promising. In the Systolic Heart Failure Treatment Supported By BNP (STARS-BNP) trial,Jourdain et al. randomised 220 patients with NYHA functional class II and III to either routine medical therapy or to a natriuretic-peptide-guided therapy where the aim was to reduce BNP to <100 pg/ml.[46] At 15 months, there were far fewer clinical end points (heart-failure-related death or hospitalisation) in the BNP-guided group (24% versus 52%; p<0.001). However those in the BNP-guided arm had significantly higher physician visits and drug changes although only around a third of patients reached the target BNP value of <100 pg/ml. Similarly the Pro-BNP Outpatient Tailored CHF Therapy (PROTECT) trial by Januzzi et al. with 151 subjects also showed a benefit for patients who had NT-proBNP-guided therapy for heart failure.[47]
Despite the initial positive trials, later larger trials were not so convincing. The NT-proBNP—Assisted Treatment To Lessen Serial Cardiac Readmissions and Death (BATTLESCARRED) trial randomised 364 patients with heart failure to either natriuretic-peptide-guided therapy, clinical-guided therapy or usual care.[48] They found that intensive heart failure management that was guided by NT-proBNP monitoring was associated with improved mortality compared with usual care. However, when compared to clinical guided therapy, natriuretic-peptide-guided therapy improved long term mortality only in patients aged <75 years.
The Trial of Intensified versus Standard Medical Therapy In Elderly Patients With Congestive Heart Failure (TIME-CHF) randomised trial on the other hand did not find any benefit either in terms of quality of life or cardiovascular outcomes with intensive management guided by NT-proBNP.[49] Similarly, the Can Pro-Brain-Natriuretic Peptide Guided Therapy Of Chronic Heart Failure Improve Heart Failure Morbidity And Mortality? (PRIMA) study also failed to show any benefit with natriuretic-peptide-guided therapy.[50]
Troughton et al. performed an individual patient data meta-analysis of the various trials that studied the effect of natriuretic peptide monitoring during heart failure therapy.[51] They identified 11 eligible studies, of which eight had individual patient data (n=2,000). Pooling the data, they found that there was a survival benefit in the group that had natriuretic peptide monitoring. However, when classified according to age, this benefit was seen only in those aged <75 years and not in those >75 years of age. The authors explain that perhaps in the elderly, due to intolerance, optimal drug dosages would not have been achieved and hence explain why monitoring natriuretic peptide values did not improve mortality. The superior mortality benefit in the younger group could conversely be explained by the fact that these patients tolerated the higher dosages of the drugs and were able to achieve maximal dosages of guideline-directed medical therapeutic agents. The meta-analysis also noted significant benefit in terms of hospital readmission rates in those where treatment was guided by natriuretic peptide monitoring.
Similarly, a recent Cochrane review of the subject concluded that there was low-quality evidence to suggest that natriuretic peptide-guided therapy could lead to a reduction in heart failure admissions, but there was uncertainty regarding the effect of natriuretic-peptide-guided therapy on mortality and all cause admission and quality of life.[52]
Other biomarkers such as ST2 have also been shown to change with therapy.[53] The use of beta-blockers and mineralocorticoid receptor blockers have been shown to reduce elevated ST2 levels. However, data are lacking in large trials studying specifically the utility of other markers besides the natriuretic peptides in guiding therapy.
The American guidelines give a Class IIa (level of evidence B) recommendation for the use of BNP or NT-pro BNP to achieve optimal dosing for guideline-directed medical therapy in select euvolaemic patients (in the outpatient setting) who are followed up in a well-structured heart failure management programme.[19] However, they suggest that using serial natriuretic peptide monitoring during therapy does not help in reducing hospitalisation or mortality in either the ambulatory outpatient setting or in the acute decompensated setting.
The European guidelines do not advocate the use of natriuretic peptides in monitoring the progress of patients being treated for heart failure, stating there is insufficient data to recommend it.[20]
Heart Failure with Preserved Ejection Fraction
Most of the studies of biomarkers in heart failure are confined to patients with heart failure with reduced ejection fraction (HFrEF). This could be due to the fact that HFpEF has been defined as a separate and distinct entity much more recently compared with the traditional HFrEF subgroup, and also because HFpEF is generally more difficult to diagnose clinically. Studies have shown that the natriuretic peptides are moderately increased in HFpEF and that values fall to normal during symptom-free periods.[54,55] Although the sensitivity of these biomarkers is slightly lower for patients with HFpEF compared with HFrEF, it still has a high diagnostic accuracy.
Markers of inflammation such as ST2 have been shown to be increased in HFpEF patients and correlated well with pro-inflammatory comorbidities.[56] In a study of 458 patients with HFrEF and 112 patients with HFpEF, ST2, high sensitivity C-reactive protein and cystatin C levels have been shown to be higher in HFpEF than HFrEF, while NT-ProBNP and troponin values were higher in HFrEF.[57] However, although they predicted prognosis to a similar level in both types, Manzano-Fernandez et al. showed that ST2 values were lower in HfpEF than HFrEF, while maintaining their prognostic predictability.[58]
Similarly, markers of myocardial fibrosis like galectin-3 have been shown to be elevated in HFpEF. In the COACH study, higher levels of galectin-3 were associated with higher rates of rehospitalisation and death in HFpEF but not HFrEF patients.[42] Despite this, studies have failed to show any correlation between levels of galectin-3 and measures of cardiac structure and function including left ventricular geometry.[59]
The role of biomarkers in the diagnosis of HFpEF has recently been reviewed by Michalska-Kasiczak et al.[60] They conclude that one single biomarker may not be sufficient for the correct diagnosis of HFpEF as it is a very heterogeneous group of patients. They suggest that a panel of biomarkers including mRNAs may be required.
Because of the paucity of data, neither the American nor the European guidelines differentiate between the two subgroups with regards to the biomarkers.[19,20]
Newer Biomarkers and Future Prospects
Many new biomarkers that have been studied in heart failure. However most of these have limited data and often fall short when compared to the NPs. These biomarkers target different aspects of the pathogenesis of heart failure, such as myocardial injury, inflammatory response, renal injury and volume status. Some of the novel ones, for example ST2, galectin 3 and pro-ADM, have been discussed earlier.
Neutrophil gelatinase-associated lipocalin is expressed by neutrophils and epithelial cells.[61] It is a marker of renal injury. The values are also high in heart failure, even when the reductions in renal function or minimal. Studies such as Optimal Trial In Myocardial Infarction With The Angiotensin II Antagonist Losartan (OPTIMAAL)and NGAL Evaluation Along With B-type Natriuretic Peptide (BNP) In Acutely Decompensated Heart Failure (GALLANT) have demonstrated a role for this marker in the diagnosis and prognostic prediction in patients with heart failure.[62,63]
Another exciting prospect is the role of circulating microRNA (miRNA) in heart failure. It has been shown that these are differentially expressed in the failing heart.[64] Different miRNAs, such as miR423-5p, miR320a and miR22, have been shown to be increased in patients with heart failure.[65] A recent meta-analysis of the role of miRNAs in the management of heart failure suggested that miR423-5p offered the best potential as a biomarker.[66] However, large-scale trials are required to validate their utility.
Many other molecules, such as procalcitonin, matrix metalloproteinases, interleukins and tumour necrosis factor alpha, have been studied in heart failure. However none of them are specific and have variable findings. It is most likely that future heart failure biomarker studies would involve a panel of markers, including natriuretic peptides, ST2 and hsTn1, which study the different pathophysiological processes that are involved in heart failure. The use of genetic testing including miRNA could become more widespread.
Metabolomic profiling (study of the byproducts of metabolism) and transcriptomics (the study of complete sets of RNA transcripts produced by the genome) are another two areas that are undergoing extensive research in the field of heart failure. Initial studies have been promising but more research is required to see if these become standard of care for patients with heart failure in the future.[67,68]
Conclusion
The use of biomarkers in the management of patients with heart failure has increased tremendously over the past few years. Currently the natriuretic peptides are the most commonly used biomarker and help in the diagnosis and prognostication of patients with heart failure. Their role in the monitoring of treatment is still debatable, although it seems reasonable that patients have their natriuretic peptide values checked at discharge.
There are many new biomarkers currently under investigation. The results are promising and they evaluate different aspects of the heart failure spectrum. At present they appear to have a synergistic role along with the natriuretic peptides — both in terms of diagnosis and determination of prognosis. However, on their own, none of them are specific for heart failure and none are recommended for routine clinical use at present. Further research is required to see which of the newer agents can be used as a reliable biomarker for the diagnosis and monitoring of patients with heart failure.
References
- 1.Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clin Pharmacol Ther. 2001;69:89–95. doi: 10.1067/mcp.2001.113989. [DOI] [PubMed] [Google Scholar]
- 2.Tijsen AJ, Pinto YM, Creemers EE. Circulating microRNAs as diagnostic biomarkers for cardiovascular diseases. Am J Physiol Heart Circ Physiol. 2012;303:H1085–H95. doi: 10.1152/ajpheart.00191.2012. [DOI] [PubMed] [Google Scholar]
- 3.Fonseca C. Diagnosis of heart failure in primary care. Heart Fail Rev. 2006;11:95–107. doi: 10.1007/s10741-006-9481-0. [DOI] [PubMed] [Google Scholar]
- 4.McCullough PA, Nowak RM, McCord J et al. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: analysis from Breathing Not Properly (BNP) Multinational Study. Circulation. 2002;106:416–22. doi: 10.1161/01.CIR.0000025242.79963.4C. [DOI] [PubMed] [Google Scholar]
- 5.McDonagh TA, Morrison CE, Lawrence A et al. Symptomatic and asymptomatic left-ventricular systolic dysfunction in an urban population. Lancet. 1997;350:829–33. doi: 10.1016/S0140-6736(97)03033-X. [DOI] [PubMed] [Google Scholar]
- 6.Zhang J, Goode KM, Cuddihy PE, Cleland JG. Predicting hospitalization due to worsening heart failure using daily weight measurement: analysis of the Trans-European Network-Home-Care Management System (TEN-HMS) study. Eur J Heart Fail. 2009;11:420–7. doi: 10.1093/eurjhf/hfp033. [DOI] [PubMed] [Google Scholar]
- 7.Yu CM, Wang L, Chau E, Chan RH, Kong SL, Tang MO et al. Intrathoracic impedance monitoring in patients with heart failure: correlation with fluid status and feasibility of early warning preceding hospitalization. Circulation. 2005;112:841–8. doi: 10.1161/CIRCULATIONAHA.104.492207. [DOI] [PubMed] [Google Scholar]
- 8.Lin DC, Diamandis EP, Januzzi JL, Jr. et al. Natriuretic peptides in heart failure. Clin Chem. 2014;60:1040–6. doi: 10.1373/clinchem.2014.223057. [DOI] [PubMed] [Google Scholar]
- 9.Curry FR. Atrial natriuretic peptide: an essential physiological regulator of transvascular fluid, protein transport, and plasma volume. J Clin Invest. 2005;115:1458–61. doi: 10.1172/JCI25417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347:161–7. doi: 10.1056/NEJMoa020233. [DOI] [PubMed] [Google Scholar]
- 11.Januzzi JL, Jr., Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol. 2005;95:948–54. doi: 10.1016/j.amjcard.2004.12.032. [DOI] [PubMed] [Google Scholar]
- 12.Januzzi JL, van Kimmenade R, Lainchbury J et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256 patients: the International Collaborative of NT-proBNP Study. Eur Heart J. 2006;27:330–7. doi: 10.1093/eurheartj/ehi631. [DOI] [PubMed] [Google Scholar]
- 13.Maisel A, Mueller C, Nowak R et al. Mid-region pro-hormone markers for diagnosis and prognosis in acute dyspnea: results from the BACH (Biomarkers in Acute Heart Failure) trial. J Am Coll Cardiol. 2010;55:2062–76. doi: 10.1016/j.jacc.2010.02.025. [DOI] [PubMed] [Google Scholar]
- 14.Kim HN, Januzzi JL., Jr Natriuretic peptide testing in heart failure. Circulation. 2011;123:2015–9. doi: 10.1161/CIRCULATIONAHA.110.979500. [DOI] [PubMed] [Google Scholar]
- 15.Xue Y, Clopton P, Peacock WF, Maisel AS. Serial changes in high-sensitive troponin I predict outcome in patients with decompensated heart failure. Eur J Heart Fail. 2011;13:37–42. doi: 10.1093/eurjhf/hfq210. [DOI] [PubMed] [Google Scholar]
- 16.Daubert MA, Jeremias A. The utility of troponin measurement to detect myocardial infarction: review of the current findings. Vasc Health Risk Manag. 2010;6:691–9. doi: 10.2147/VHRM.S5306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Januzzi JL, Jr., Peacock WF, Maisel AS et al. Measurement of the interleukin family member ST2 in patients with acute dyspnea: results from the PRIDE (Pro-Brain Natriuretic Peptide Investigation of Dyspnea in the Emergency Department) study. J Am Coll Cardiol. 2007;50:607–13. doi: 10.1016/j.jacc.2007.05.014. [DOI] [PubMed] [Google Scholar]
- 18.Schmitz J, Owyang A, Oldham E, Song Y, Murphy E, McClanahan TK et al. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity. 2005;23:479–90. doi: 10.1016/j.immuni.2005.09.015. [DOI] [PubMed] [Google Scholar]
- 19.Yancy CW, Jessup M, Bozkurt B et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–e239. doi: 10.1016/j.jacc.2013.05.019. [DOI] [PubMed] [Google Scholar]
- 20.Ponikowski P, Voors AA, Anker SD et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200. doi: 10.1093/eurheartj/ehw128. [DOI] [PubMed] [Google Scholar]
- 21.Tsutamoto T, Wada A, Maeda K et al. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction. Circulation. 1997;96:509–16. doi: 10.1161/01.CIR.96.2.509. [DOI] [PubMed] [Google Scholar]
- 22.Logeart D, Thabut G, Jourdain P et al. Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol. 2004;43:635–41. doi: 10.1016/j.jacc.2003.09.044. [DOI] [PubMed] [Google Scholar]
- 23.Masson S, Latini R, Anand IS et al. Prognostic value of changes in N-terminal pro-brain natriuretic peptide in Val-HeFT (Valsartan Heart Failure Trial) J Am Coll Cardiol. 2008;52:997–1003. doi: 10.1016/j.jacc.2008.04.069. [DOI] [PubMed] [Google Scholar]
- 24.Kociol RD, Horton JR, Fonarow GC et al. Admission, discharge, or change in B-type natriuretic peptide and long-term outcomes: data from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) linked to Medicare claims. Circ Heart Fail. 2011;4:628–36. doi: 10.1161/CIRCHEARTFAILURE.111.962290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Doust JA, Glasziou PP, Pietrzak E, Dobson AJ. A systematic review of the diagnostic accuracy of natriuretic peptides for heart failure. Arch Intern Med. 2004;164:1978–84. doi: 10.1001/archinte.164.18.1978. [DOI] [PubMed] [Google Scholar]
- 26.Wang TJ, Larson MG, Levy D et al. Plasma natriuretic peptide levels and the risk of cardiovascular events and death. N Engl J Med. 2004;350:655–63. doi: 10.1056/NEJMoa031994. [DOI] [PubMed] [Google Scholar]
- 27.McKie PM, Rodeheffer RJ, Cataliotti A et al. Amino-terminal pro-B-type natriuretic peptide and B-type natriuretic peptide: biomarkers for mortality in a large community-based cohort free of heart failure. Hypertension. 2006;47:874–80. doi: 10.1161/01.HYP.0000216794.24161.8c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.von Haehling S, Jankowska EA, Morgenthaler NG et al. Comparison of midregional pro-atrial natriuretic peptide with N-terminal pro-B-type natriuretic peptide in predicting survival in patients with chronic heart failure. J Am Coll Cardiol. 2007;50:1973–80. doi: 10.1016/j.jacc.2007.08.012. [DOI] [PubMed] [Google Scholar]
- 29.Shah RV, Truong QA, Gaggin HK et al. Mid-regional pro-atrial natriuretic peptide and pro-adrenomedullin testing for the diagnostic and prognostic evaluation of patients with acute dyspnoea. Eur Heart J. 2012;33:2197–205. doi: 10.1093/eurheartj/ehs136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Masson S, Latini R, Carbonieri E et al. The predictive value of stable precursor fragments of vasoactive peptides in patients with chronic heart failure: data from the GISSI-heart failure (GISSI-HF) trial. Eur J Heart Fail. 2010;12:338–47. doi: 10.1093/eurjhf/hfp206. [DOI] [PubMed] [Google Scholar]
- 31.Peacock WF, De MT, Fonarow GC et al. Cardiac troponin and outcome in acute heart failure. N Engl J Med. 2008;358:2117–26. doi: 10.1056/NEJMoa0706824. [DOI] [PubMed] [Google Scholar]
- 32.Pascual-Figal DA, Manzano-Fernandez S, Boronat M et al. Soluble ST2, high-sensitivity troponin T- and N-terminal pro-B-type natriuretic peptide: complementary role for risk stratification in acutely decompensated heart failure. Eur J Heart Fail. 2011;13:718–25. doi: 10.1093/eurjhf/hfr047. [DOI] [PubMed] [Google Scholar]
- 33.Felker GM, Mentz RJ, Teerlink JR et al. Serial high sensitivity cardiac troponin T measurement in acute heart failure: insights from the RELAX-AHF study. Eur J Heart Fail. 2015;17:1262–70. doi: 10.1002/ejhf.341. [DOI] [PubMed] [Google Scholar]
- 34.Tsutamoto T, Kawahara C, Nishiyama K et al. Prognostic role of highly sensitive cardiac troponin I in patients with systolic heart failure. Am Heart J. 2010;159:63–7. doi: 10.1016/j.ahj.2009.10.022. [DOI] [PubMed] [Google Scholar]
- 35.Klip IT, Voors AA, Anker SD et al. Prognostic value of mid-regional pro-adrenomedullin in patients with heart failure after an acute myocardial infarction. Heart. 2011;97:892–8. doi: 10.1136/hrt.2010.210948. [DOI] [PubMed] [Google Scholar]
- 36.Odermatt J, Meili M, Hersberger L et al. Pro-Adrenomedullin predicts 10-year all-cause mortality in community-dwelling patients: a prospective cohort study. BMC Cardiovasc Disord. 2017;17:178. doi: 10.1186/s12872-017-0605-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dattagupta A, Immaneni S. ST2: Current status. Indian Heart J. 2018;70(Suppl 1):S96–S101. doi: 10.1016/j.ihj.2018.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Anand IS, Rector TS, Kuskowski M et al. Prognostic value of soluble ST2 in the Valsartan Heart Failure Trial. Circ Heart Fail. 2014;7:418–26. doi: 10.1161/CIRCHEARTFAILURE.113.001036. [DOI] [PubMed] [Google Scholar]
- 39.Binas D, Daniel H, Richter A et al. The prognostic value of sST2 and galectin-3 considering different aetiologies in non-ischaemic heart failure. Open Heart. 2018;5:e000750. doi: 10.1136/openhrt-2017-000750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McCullough PA, Olobatoke A, Vanhecke TE. Galectin-3: a novel blood test for the evaluation and management of patients with heart failure. Rev Cardiovasc Med. 2011;12:200–10. doi: 10.3909/ricm0624. [DOI] [PubMed] [Google Scholar]
- 41.Grandin EW, Jarolim P, Murphy SA et al. Galectin-3 and the development of heart failure after acute coronary syndrome: pilot experience from PROVE IT-TIMI 22. Clin Chem. 2012;58:267–73. doi: 10.1373/clinchem.2011.174359. [DOI] [PubMed] [Google Scholar]
- 42.de Boer RA, Lok DJ, Jaarsma T et al. Predictive value of plasma galectin-3 levels in heart failure with reduced and preserved ejection fraction. Ann Med. 2011;43:60–8. doi: 10.3109/07853890.2010.538080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Karatolios K, Chatzis G, Holzendorf V et al. Galectin-3 as a Predictor of Left Ventricular Reverse Remodeling in Recent-Onset Dilated Cardiomyopathy. Dis Markers. 2018;2018:2958219. doi: 10.1155/2018/2958219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gaggin HK, Truong QA, Gandhi PU et al. Systematic evaluation of endothelin 1 measurement relative to traditional and modern biomarkers for clinical assessment and prognosis in patients with chronic systolic heart failure: serial measurement and multimarker testing. Am J Clin Pathol. 2017;147:461–72. doi: 10.1093/ajcp/aqx014. [DOI] [PubMed] [Google Scholar]
- 45.Januzzi JL, Troughton R. Are serial BNP measurements useful in heart failure management? Serial natriuretic peptide measurements are useful in heart failure management. Circulation. 2013;127:500–7. doi: 10.1161/CIRCULATIONAHA.112.120485. [DOI] [PubMed] [Google Scholar]
- 46.Jourdain P, Jondeau G, Funck F et al. Plasma brain natriuretic peptide-guided therapy to improve outcome in heart failure: the STARS-BNP Multicenter Study. J Am Coll Cardiol. 2007;49:1733–9. doi: 10.1016/j.jacc.2006.10.081. [DOI] [PubMed] [Google Scholar]
- 47.Januzzi JL, Jr., Rehman SU, Mohammed AA et al. Use of amino-terminal pro-B-type natriuretic peptide to guide outpatient therapy of patients with chronic left ventricular systolic dysfunction. J Am Coll Cardiol. 2011;58:1881–9. doi: 10.1016/j.jacc.2011.03.072. [DOI] [PubMed] [Google Scholar]
- 48.Lainchbury JG, Troughton RW, Strangman KM et al. N-terminal pro-B-type natriuretic peptide-guided treatment for chronic heart failure: results from the BATTLESCARRED (NT-proBNP-Assisted Treatment To Lessen Serial Cardiac Readmissions and Death) trial. J Am Coll Cardiol. 2009;55:53–60. doi: 10.1016/j.jacc.2009.02.095. [DOI] [PubMed] [Google Scholar]
- 49.Pfisterer M, Buser P, Rickli H et al. BNP-guided vs symptom-guided heart failure therapy: the Trial of Intensified vs Standard Medical Therapy in Elderly Patients With Congestive Heart Failure (TIME-CHF) randomized trial. JAMA. 2009;301:383–92. doi: 10.1001/jama.2009.2. [DOI] [PubMed] [Google Scholar]
- 50.Eurlings LW, van Pol PE, Kok WE et al. Management of chronic heart failure guided by individual N-terminal pro-B-type natriuretic peptide targets: results of the PRIMA (Can PRo-brain-natriuretic peptide guided therapy of chronic heart failure IMprove heart fAilure morbidity and mortality?) study. J Am Coll Cardiol. 2010;56:2090–100. doi: 10.1016/j.jacc.2010.07.030. [DOI] [PubMed] [Google Scholar]
- 51.Troughton RW, Frampton CM, Brunner-La Rocca HP et al. Effect of B-type natriuretic peptide-guided treatment of chronic heart failure on total mortality and hospitalization: an individual patient meta-analysis. Eur Heart J. 2014;35:1559–67. doi: 10.1093/eurheartj/ehu090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.McLellan J, Heneghan CJ, Perera R et al. B-type natriuretic peptide-guided treatment for heart failure. Cochrane Database Syst Rev. 2016;12:CD008966. doi: 10.1002/14651858.CD008966.pub2. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD008966.pub2/full [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Januzzi JL., Jr ST2 as a cardiovascular risk biomarker: from the bench to the bedside. J Cardiovasc Transl Res. 2013;6:493–500. doi: 10.1007/s12265-013-9459-y. [DOI] [PubMed] [Google Scholar]
- 54.Lubien E, DeMaria A, Krishnaswamy P et al. Utility of B-natriuretic peptide in detecting diastolic dysfunction: comparison with Doppler velocity recordings. Circulation. 2002;105:595–601. doi: 10.1161/hc0502.103010. [DOI] [PubMed] [Google Scholar]
- 55.Tschope C, Kasner M, Westermann D et al. The role of NT-proBNP in the diagnostics of isolated diastolic dysfunction: correlation with echocardiographic and invasive measurements. Eur Heart J. 2005;26:2277–84. doi: 10.1093/eurheartj/ehi406. [DOI] [PubMed] [Google Scholar]
- 56.AbouEzzeddine OF, McKie PM, Dunlay SM et al. Suppression of tumorigenicity 2 in heart failure with preserved ejection fraction. J Am Heart Assoc. 2017;6:e004382. doi: 10.1161/JAHA.116.004382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sanders-van Wijk S, van Empel V, Davarzani N et al. Circulating biomarkers of distinct pathophysiological pathways in heart failure with preserved vs. reduced left ventricular ejection fraction. Eur J Heart Fail. 2015;17:1006–14. doi: 10.1002/ejhf.414. [DOI] [PubMed] [Google Scholar]
- 58.Manzano-Fernandez S, Mueller T, Pascual-Figal D et al. Usefulness of soluble concentrations of interleukin family member ST2 as predictor of mortality in patients with acutely decompensated heart failure relative to left ventricular ejection fraction. Am J Cardiol. 2011;107:259–67. doi: 10.1016/j.amjcard.2010.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.AbouEzzeddine OF, Haines P, Stevens S et al. Galectin-3 in heart failure with preserved ejection fraction. A RELAX trial substudy (Phosphodiesterase-5 Inhibition to Improve Clinical Status and Exercise Capacity in Diastolic Heart Failure) JACC Heart Fail. 2015;3:245–52. doi: 10.1016/j.jchf.2014.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Michalska-Kasiczak M, Bielecka-Dabrowa A, von Haehling S et al. Biomarkers, myocardial fibrosis and co-morbidities in heart failure with preserved ejection fraction: an overview. Arch Med Sci. 2018;14:890–909. doi: 10.5114/aoms.2018.76279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Friedl A, Stoesz SP, Buckley P, Gould MN. Neutrophil gelatinase-associated lipocalin in normal and neoplastic human tissues. Cell type-specific pattern of expression. Histochem J. 1999;31:433–41. doi: 10.1023/A:1003708808934. [DOI] [PubMed] [Google Scholar]
- 62.Dickstein K, Kjekshus J. Effects of losartan and captopril on mortality and morbidity in high-risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Lancet. 2002;360:752–60. doi: 10.1016/S0140-6736(02)09895-1. [DOI] [PubMed] [Google Scholar]
- 63.Maisel AS, Mueller C, Fitzgerald R et al. Prognostic utility of plasma neutrophil gelatinase-associated lipocalin in patients with acute heart failure: the NGAL EvaLuation Along with B-type NaTriuretic Peptide in acutely decompensated heart failure (GALLANT) trial. Eur J Heart Fail. 2011;13:846–51. doi: 10.1093/eurjhf/hfr087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.van Rooij E, Sutherland LB, Liu N et al. A signature pattern of stress-responsive microRNAs that can evoke cardiac hypertrophy and heart failure. Proc Natl Acad Sci USA. 2006;103:18255–60. doi: 10.1073/pnas.0608791103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Corsten MF, Dennert R, Jochems S et al. Circulating MicroRNA-208b and MicroRNA-499 reflect myocardial damage in cardiovascular disease. Circ Cardiovasc Genet. 2010;3:499–506. doi: 10.1161/CIRCGENETICS.110.957415. [DOI] [PubMed] [Google Scholar]
- 66.Yan H, Ma F, Zhang Y et al. miRNAs as biomarkers for diagnosis of heart failure: A systematic review and meta-analysis. Medicine (Baltimore) 2017;96:e6825. doi: 10.1097/MD.0000000000006825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lanfear DE, Gibbs JJ, Li J et al. Targeted metabolomic profiling of plasma and survival in heart failure patients. JACC Heart Fail. 2017;5:823–32. doi: 10.1016/j.jchf.2017.07.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Toma M, Mak GJ, Chen V et al. Differentiating heart failure phenotypes using sex-specific transcriptomic and proteomic biomarker panels. ESC Heart Fail. 2017;4:301–11. doi: 10.1002/ehf2.12136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Suarez G, Meyerrose G. Heart failure and galectin 3. Ann Transl Med. 2014;2:86. doi: 10.3978/j.issn.2305-5839.2014.09.10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Soni SS, Cruz D, Bobek I et al. NGAL: a biomarker of acute kidney injury and other systemic conditions. Int Urol Nephrol. 2010;42:141–50. doi: 10.1007/s11255-009-9608-z. [DOI] [PubMed] [Google Scholar]
- 71.Potocki M, Ziller R, Mueller C. Mid-regional pro-adrenomedullin in acute heart failure: a better biomarker or just another biomarker? Curr Heart Fail Rep. 2012;9:244–51. doi: 10.1007/s11897-012-0096-6. [DOI] [PubMed] [Google Scholar]
- 72.Rehman SU, Mueller T, Januzzi JL., Jr Characteristics of the novel interleukin family biomarker ST2 in patients with acute heart failure. J Am Coll Cardiol. 2008;52:1458–65. doi: 10.1016/j.jacc.2008.07.042. [DOI] [PubMed] [Google Scholar]
- 73.Boisot S, Beede J, Isakson S et al. Serial sampling of ST2 predicts 90-day mortality following destabilized heart failure. J Card Fail. 2008;14:732–8. doi: 10.1016/j.cardfail.2008.06.415. [DOI] [PubMed] [Google Scholar]
- 74.Morrow DA, Scirica BM, Karwatowska-Prokopczuk E et al. MERLIN-TIMI 36 Trial Investigators. Effects of ranolazine on recurrent cardiovascular events in patients with non-ST-elevation acute coronary syndromes: the MERLIN-TIMI 36 randomized trial. JAMA. 2007;297((16)):1775–83. doi: 10.1001/jama.297.16.1775. [DOI] [PubMed] [Google Scholar]