

Abstract
Objective:
The trial aimed to study the effectiveness of multipurpose health-worker-led exercise therapy on women patients of 30–50 years of age with chronic nonspecific low backache (LBA) in a primary health center.
Materials and Methods:
The multipurpose health worker had undergone 2 days training for exercises to relief chronic nonspecific LBA in the Department of Orthopaedic, Jawaharlal Institute of Post Graduate Medical Education and Research, Puducherry. Patients were allocated to either intervention arm (who received exercise therapy) or control arm (who received pharmacological therapy of analgesics). Patients with less than 3 months of pain, acute onset of pain, localized pain, or straight leg raising test positive were excluded. The pain score on three different positions (motion, sitting, and standing) was assessed on visual analogue scale before starting the exercise therapy or the pharmacological therapy and after 1 month of the exercise therapy or pharmacological therapy.
Statistical Analysis:
Data were analyzed using SPSS Software. Wilcoxon sign-rank test is used to compare the scores before and after intervention depending upon normality of distribution. Difference in difference analysis is used to compare the scores between the two groups.
Results:
Multipurpose health-worker-led exercise therapy is found to be equally effective as compared to pharmacological therapy. Significant difference in reduction of pain score was not obtained between control and intervention arm (P value: 0.343, 0.819, and 0.335 in motion, standing, and sitting position). However, significant reduction in pain score in all the three positions was obtained in intervention (P value < 0.001, <0.001, <0.001 in motion, standing, and sitting, respectively). Therefore, it can be suggested that multipurpose health-worker-led exercise therapy may be implemented in a primary health-care setting which will help to reduce the analgesics load on the health center and prevent the adverse effect profile of the drugs on patients.
Keywords: Analgesics, exercise therapy, multipurpose health worker, nonspecific low backache
Introduction
Low backache (LBA) is a common musculoskeletal disorder, affecting the quality of life (QoL) of patients. Besides affecting individual patients, it is an additional cost for the society owing to loss of work and medical expenses. According to WHO, lifetime prevalence of LBA is 58–84% and the point prevalence is 4–33%.[1] A study conducted in rural Puducherry, India in 2013 reports that 42% of women have LBA.[2] Global Burden of Diseases 2013 shows that the annual years of healthy life lost per 100,000 people from low back pain has increased by 19.3% since 1990 in India.[3] American Physical Therapy Association recommends trunk coordination, strengthening, and endurance exercises to reduce low back pain and disability in patients with chronic LBA based on strong clinical evidence.[4] In a randomized control trial (RCT) evaluating the effectiveness of exercise on pain relief, conducted in 2011 by Murtezani et al., in Republic of Kosovo, the results show that there is a significant reduction in pain score among patients in exercise group when compared with passive modalities.[5]
In majority cases of chronic LBA (LBA for more than 3 months), pathology cannot be identified referred to as nonspecific low backache (NSLBA), which represents about 85% of LBP patients seen in primary care.[6] A study done in Germany in 2009 shows that it costs about €98.66 only for drugs to treat patients with chronic LBA in a primary care setting.[7] With these issues on one side, integrating the physical therapy into primary health care has several advantages, namely, individualized treatment (exercise) programs, and self-management and education for musculoskeletal complaints thus improving the QoL of such patients cost-effectively. In spite of higher burden of chronic nonspecific low backache (CNSLBA) in primary health-care setting, strong clinical evidence suggesting exercises for treating pain due to NSLBA and high cost of treating it with drugs in primary care setting and the advantages as mentioned above, evaluating the feasibility and effect of exercise therapy on pain reduction among such patients in primary care setting was rarely looked upon. Hence, this study was done among adult women patients of age 30–50 years of age with CNSLBA attending Jawaharlal Institute of Post Graduate Medical Education and Research (JIPMER) urban health center, to assess the effect of multipurpose health worker (MHW)-led exercise therapy on pain reduction as compared to those receiving only pharmacological therapy.
Materials and Methods
The study was approved in the Institutional Ethics Committee (Human Studies), JIPMER, Puducherry. This was a single-blinded, parallel arm RCT carried out in JIPMER urban health training center (UHTC). The UHTC of JIPMER caters to a population of about 7900 from 4 areas, namely, Kurusukuppam, Vaithikuppam, Vazhaikkulam, and Chinnayapuram. There is one medical officer, two staff nurses, one public health nurse, and two auxiliary nurse mid-wives working in the center. All patients were examined and treated by the medical officer, who was assisted by medical interns and a junior resident from Department of Preventive and Social Medicine posted at UHTC.
In this study, adult women patients of age 30–50 years with chronic low back pain (pain more than 3 months) who attended JIPMER urban health center were screened by the investigator. Patients with history, signs, and symptoms suggestive of any organic cause for LBA, that is, history of acute onset of LBA when it started, localized pain, or straight leg raising test (SLRT) positive were excluded. Such patients without the aforementioned exclusion were labeled as patients with CNSLBA and a written informed consent for participation in the study was requested from them. Those patients who gave consent for the study were interviewed by the investigator with a structured questionnaire to obtain information on sociodemographic details, symptoms, and pain score measured using visual analog scale (VAS). Patients were then randomized into intervention or control arm based on random number sequence generated using random allocation software by simple randomization technique. Allocation was done by the junior resident in-charge of JIPMER Urban health center. Allocation concealment was ensured using Sequentially Numbered, Opaque Sealed Envelopes technique. Consecutive sampling was done till the desired sample size was reached. The sample size was calculated using OpenEpi software version 3.0. With expected mean difference of pain score between the intervention group (2 ± 1.7) and control group (4 ± 2.7) to be 2, the sample size was estimated at 40 (20 in each group), with 95% confidence interval, 80% power, and ratio between 2 groups as 1.
The patients allocated to intervention arm were given multivitamin tablets (placebo) and referred to a MPW already trained in teaching certain exercises for CNSLBA by Department of Orthopaedics, JIPMER. The control group received pharmacological therapy (analgesics). After learning the exercises from MPW, patients were asked to review after 1 week, when the MPW ensured the compliance of the patient to the exercises and reinforced the patient to continue them. They were also instructed not to take any medication for pain. The patients in the control arm received the pharmacological therapy of analgesics for 5 days. The investigator visited all the patients at their home at the end of 1-month duration and assessed for reduction in pain using VAS score. The investigator was blinded for allocation of patients to intervention or control arm [Figure 1].
Figure 1.
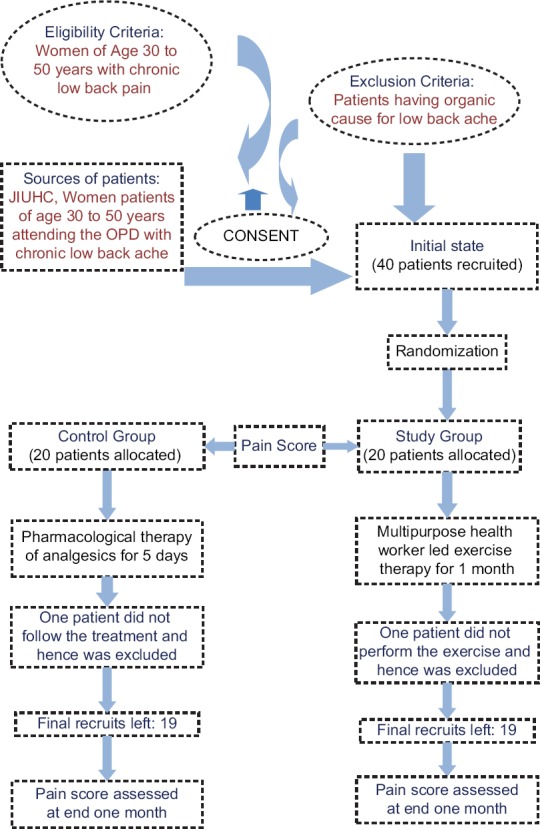
Flow diagram showing study procedure in brief
Statistical analysis
Data were entered in MS Excel 2013 and was analyzed using SPSS software version 20.0. Continuous variables such as age, duration of pain, and discrete variables like VAS score are expressed either as mean (SD) or median (IQR) depending upon the normality of distribution. Categorical variables such as education status and occupation are expressed as proportion. Wilcoxon sign-rank test was used to compare the scores before and after intervention. Difference in difference analysis was used to compare the scores between the two groups.
Result
In this present study, we have contacted 90 women between 30 and 50 years of age attending at UHTC of a tertiary care institute at Puducherry, with LBA. Out of 90 women, 50 patients with localized pain, acute onset pain, or SLRT positive were excluded. Remaining 40 patients were then recruited and randomized into intervention and control arm by using randomization software. Twenty patients were allocated to control arm which received only pharmacological therapy whereas the other 20 patients to intervention arm which received MHW-led exercise therapy. After randomization, one patient each in control and intervention arm was not willing to participate in the study due to personal reasons.
The 38 subjects participated in the study. Out of 38 study subjects, all are women in the age group of 30–50 years. Age distribution of study participants (N = 38) is shown in Table 1. Mean age of participants (in years) is 38.9 (5.6). There is no significant difference in age between intervention and control arm (P value: 0.951). Distribution of study participants based on education status (N = 38): 4 out of 19 were not formally educated in the intervention group, whereas 3 out of 19 were not formally educated in control group. Similarly, 4 out of 19 in intervention group received up to primary schooling, whereas 3 out of 19 received primary schooling in control group. Nine out of 19 received up to high school education in the intervention group, whereas in control group, 8 had received the same. Only one patient was educated till secondary level in intervention group whereas three received the same in control group. There was one graduate included in the control group whereas no graduates were in intervention group. There was one postgraduate in each control and intervention arm. There is no significant difference in between intervention and control arm with respect to education status (P value = 0.923) [Table 2]. Table 3 shows the distribution of study participants based on occupation status (N = 38). 9 out of 19 were unemployed including housewives in intervention group, whereas 7 out of 19 were unemployed in control group. Ten out of 19 were employed in intervention group, whereas 12 out of 19 were employed in control group. There is no significant difference in between intervention and control arm with respect to employment status (P = 0.511).
Table 1.
Age distribution of study participants (n=38)
| Age category (in years) | Frequency (%) | P* | |
|---|---|---|---|
| Intervention arm (n=19) | Control arm (n=19) | ||
| 30-35 | 6 (31.6) | 4 (21.1) | 0.951 |
| 36-40 | 8 (42.1) | 10 (52.6) | |
| 41-45 | 1 (5.3) | 1 (5.3) | |
| 46-50 | 4 (21.1) | 4 (21.1) | |
*Fischer exact test
Table 2.
Distribution of study participants based on education status (n=38)
| Education status | Frequency (%) | P* | |
|---|---|---|---|
| Intervention arm (n=19) | Control arm (n=19) | ||
| No formal education | 4 (21.1) | 3 (15.8) | 0.923 |
| Primary school | 4 (21.1) | 3 (15.8) | |
| High school | 9 (47.4) | 8 (42.1) | |
| Secondary school | 1 (5.3) | 3 (15.8) | |
| Graduate | 0 | 1 (5.3) | |
| Postgraduate | 1 (5.3) | 1 (5.3) | |
*Fischer exact test
Table 3.
Distribution of study participants based on occupation status (n=38)
| Occupation status | Frequency (%) | P* | |
|---|---|---|---|
| Intervention arm (n=19) | Control arm (n=19) | ||
| Unemployed | 9 (47.4) | 7 (36.8) | 0.511 |
| Employed | 10 (52.6) | 12 (63.2) | |
*Chi-square test
Overall, the median (IQR) pain duration was found to be 4 (2–10) years. Median pain duration was not found to be statistically significant (P value: 0.420) between intervention and control groups, which was found to be 3 (1–6) years and 4 (2–10) years, respectively.
The median pain score of women with low back pain before and after exercise therapy in the intervention arm is in motion: 4 (2–5) and 2 (1–3), in standing: 4 (3–5) and 2 (2–3), in sitting: 5 (3–6) and 2 (2–3). The reduction in pain score among various positions motion, standing, and sitting is found to be significant (P value: <0.001, <0.001, <0.001, respectively) [Table 4].
Table 4.
Pain score before and after treatment in intervention and control arm
| Pain | Intervention arm (n=19), median (IQR) | Control arm (n=19), median (IQR) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | P | Pre | Post | P | |
| During motion | 4 (2-5) | 2 (1-3) | <0.001 | 3 (0-6) | 1 (0-4) | 0.0031 |
| During standing | 4 (3-5) | 2 (2-3) | <0.001 | 4 (0-6) | 2 (0-4) | 0.0012 |
| During sitting | 5 (3-6) | 2 (2-3) | <0.001 | 5 (4-6) | 4 (2-4) | <0.001 |
Among control, group median pain score before and after medication during motion: 3 (0–6) and 1 (0–4), during standing: 4 (0–6) and 2 (0–4), and during sitting: 5 (4–6) and 4 (2–4). The reduction in pain score among various positions motion, standing, and sitting is significant (P value: 0.0031, 0.0012, <0.001) [Table 4].
The difference in difference of pain score between control group and intervention group during motion, standing, or sitting was not found statistically significant (P values: 0.343, 0.819, 0.335, respectively) [Table 5].
Table 5.
Effectiveness of MPW-led exercise therapy in reducing pain among women patients with CNSLBA in an urban health center, Puducherry (n=38)
| Pain | Intervention arm (n=19), median (IQR) | Control arm (n=19), median (IQR) | P* | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Difference | Pre | Post | Difference | ||
| During motion | 4 (2-5) | 2 (1-3) | −1 (-2-0) | 3 (0-6) | 1 (0-4) | 0 (−2-0) | 0.343 |
| During standing | 4 (3-5) | 2 (2-3) | −2 (−2-0) | 4 (0-6) | 2 (0-4) | −1 (−2-0) | 0.819 |
| During sitting | 5 (3-6) | 2 (2-3) | −2 (−3-0) | 5 (4-6) | 4 (2-4) | −1 (−2-0) | 0.335 |
*Mann-Whitney test between intervention and control group for difference in pre and postscores
Discussion
The burden of LBA among women in this region was found to be 42%. However, no effective intervention was planned to curtail the above burden. The present study is to measure the effectiveness of MHW-led exercise therapy in comparison to pharmacological treatment in CNSLBA. This study found that the reduction of pain score for NSLBA was reduced from 4 (2–5) to 2 (1–3) during motion, 4 (3–5) to 2 (2–3) during standing, and 5 (3–6) to 2 (2–3) in intervention group. Similarly, it was reduced from 3 (0–6) to 1 (0–4) during motion, 4 (0–6) to 2 (0–4) during standing, and 5 (4–6) to 4 (2–4) during sitting in control group and the reduction was more in intervention compared to control arm. However, the difference in difference in reduction of pain score was not statistically significant. This implies that exercise therapy alone could minimize the sufferings due to NSLBA, as equivalent to pharmacological therapy, and this exercise therapy will be more cost-effective and drug-induced side effects can be prevented. A study conducted by Takahashi et al. in Fukushima, Japan, on adult patients with CNSLBA also found that the therapeutic efficacy of an NSAID and exercise seemed to be almost equivalent with regard to pain relief.[8] Study conducted by van Middelkoop et al. found that exercise therapy is effective at reducing pain and function in the treatment of chronic low back pain.[9] However, a meta-analysis conducted by Hayden et al. found that exercise therapy seems to be slightly effective at decreasing pain and improving function in adults with chronic low back pain.[10]
Therefore, MHW-led exercise therapy can be implemented for CNSLBA patients as it's a nonpharmacological method which will help in reducing the cost of health care provided and it may improve the QoL of patients by reducing pain. In addition, the adverse effect profile of analgesics can be prevented.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81:646–56. [PMC free article] [PubMed] [Google Scholar]
- 2.Ahdhi GS, Subramanian R, Saya GK, Yamuna TV. Prevalence of low back pain and its relation to quality of life and disability among women in rural area of Puducherry, India. Indian J Pain. 2016;30:111–15. [Google Scholar]
- 3.Naghavi M, Wang H, Lozano R, Davis A, Liang X, Zhou M, et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–71. doi: 10.1016/S0140-6736(14)61682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Powers CM, Bolgla LA, Callaghan MJ, Collins N, Sheehan FT. Patellofemoral pain: Proximal, distal, and local factors, 2nd International Research Retreat. J Orthop Sports Phys Ther. 2012;42:A1–54. doi: 10.2519/jospt.2012.0301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Murtezani A, Hundozi H, Orovcanec N, Sllamniku S, Osmani T. A Comparison of high intensity aerobic exercise and passive modalities for the treatment of workers with chronic low back pain: A randomized, controlled trial. Eur J Phys Rehabil Med. 2011;47:359–66. [PubMed] [Google Scholar]
- 6.Wand BM, O’Connell NE. Chronic non-specific low back pain-sub-groups or a single mechanism? BMC Musculoskelet Disord. 2008;25:11–7. doi: 10.1186/1471-2474-9-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Becker A, Held H, Redaelli M, Strauch K, Chenot JF, Leonhardt C, et al. Low back pain in primary care: Costs of care and prediction of future health care utilization. Spine. 2010;35:1714–20. doi: 10.1097/brs.0b013e3181cd656f. [DOI] [PubMed] [Google Scholar]
- 8.Takahashi N, Omata J, Iwabuchi M, Fukuda H, Shirado O. Therapeutic efficacy of nonsteroidal anti-inflammatory drug therapy versus exercise therapy in patients with chronic nonspecific low back pain: A prospective study. Fukushima J Med Sci. 2017;63:8–15. doi: 10.5387/fms.2016-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Pract Res Clin Rheumatol. 2010;24:193–204. doi: 10.1016/j.berh.2010.01.002. [DOI] [PubMed] [Google Scholar]
- 10.Hayden JA, van Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: Exercise therapy for nonspecific low back pain. Ann Intern Med. 2005;142:765–75. doi: 10.7326/0003-4819-142-9-200505030-00013. [DOI] [PubMed] [Google Scholar]