

Abstract
Objectives
Meniscal injuries are often associated with an active lifestyle. The damage of meniscal tissue puts young patients at higher risk of undergoing meniscal surgery and, therefore, at higher risk of osteoarthritis. In this study, we undertook proof-of-concept research to develop a cellularized human meniscus by using 3D bioprinting technology.
Methods
A 3D model of bioengineered medial meniscus tissue was created, based on MRI scans of a human volunteer. The Digital Imaging and Communications in Medicine (DICOM) data from these MRI scans were processed using dedicated software, in order to obtain an STL model of the structure. The chosen 3D Discovery printing tool was a microvalve-based inkjet printhead. Primary mesenchymal stem cells (MSCs) were isolated from bone marrow and embedded in a collagen-based bio-ink before printing. LIVE/DEAD assay was performed on realized cell-laden constructs carrying MSCs in order to evaluate cell distribution and viability.
Results
This study involved the realization of a human cell-laden collagen meniscus using 3D bioprinting. The meniscus prototype showed the biological potential of this technology to provide an anatomically shaped, patient-specific construct with viable cells on a biocompatible material.
Conclusion
This paper reports the preliminary findings of the production of a custom-made, cell-laden, collagen-based human meniscus. The prototype described could act as the starting point for future developments of this collagen-based, tissue-engineered structure, which could aid the optimization of implants designed to replace damaged menisci.
Cite this article: G. Filardo, M. Petretta, C. Cavallo, L. Roseti, S. Durante, U. Albisinni, B. Grigolo. Patient-specific meniscus prototype based on 3D bioprinting of human cell-laden scaffold. Bone Joint Res 2019;8:101–106. DOI: 10.1302/2046-3758.82.BJR-2018-0134.R1.
Keywords: Meniscus, Bioprinting, Cell-laden bio-ink, Scaffold, Mesenchymal stem cells
Article focus
In recent years, researchers have produced bioartificial substitutes that restore the function of damaged organs by combining cells, biomaterials, and growth factors.
Meniscal tissue regeneration strategies have been the subject of significant research interest.
In this article, we report the development of a cellularized human meniscus using 3D bioprinting technology.
Key messages
With 3D bioprinting, it is possible to create a cellularized meniscus substitute.
This technology is emerging as a novel strategy to promote tissue repair for different clinical applications.
Strengths and limitations
No previous study reports the creation of a cellularized custom-made meniscus using 3D bioprinting technology.
Meniscal structure plays a key role in joint load distribution, but this aspect has not been investigated.
Future studies should investigate the maturation of this construct and document the final biomechanical properties obtained, as well as their effectiveness in protecting the joint surfaces.
Introduction
The menisci of the knee consist of two semilunar fibrocartilage structures located at the medial and lateral articular surfaces of the tibial plateau, where they contribute to stabilization, nourishment, and force distribution.1 Meniscal lesions represent the most common surgically treated knee pathology, with 850 000 meniscal procedures performed in the United States every year.2 Meniscectomy procedures, which are carried out to reduce pain and to recover satisfactory knee function, are often unavoidable when treating meniscal tears.3 Since injury or surgery can result in the substantial loss of meniscal tissue, can permanently alter joint homeostasis, and can lead to a high risk of osteoarthritis, alternative surgical options have been developed to restore the biomechanical environment of the knee.4
The management of meniscal pathology is therefore focused on preserving meniscal tissue to the greatest extent possible. Meniscal allografts are currently the preferred treatment for patients who have previously had a total or subtotal meniscectomy, with good results reported at long-term follow-up.5,6 However, there are multiple drawbacks to meniscal allograft transplantation, such as limits in tissue availability, the risk of mismatch and immunoreactivity, impaired cellular infiltration and remodelling capacity, and suboptimal prognosis with results worsening over time.7,8 To overcome the limitations of allografts, several scaffolds have been developed,9 but, despite promising preclinical findings, only two cell-free meniscal substitutes have reached clinical practice and been used to address partial meniscus defects: one collagen-based meniscal implant and one consisting of polyurethane and polycaprolactone.10 Safety and positive clinical results have been reported for both scaffolds, with imaging and, in some cases, arthroscopic evaluation confirming the potential of these bio-engineered devices to stimulate meniscal tissue regeneration, albeit not completely.9,11,12 Further to the limited regenerative potential, the mismatch between these crescent-shaped implants and the patient-specific lesion areas is a key issue, as it has been demonstrated that even small changes in implant positioning may affect contact pressure and joint stress.13 To address the limits of meniscus implantation, and to optimize the restoration of meniscal function and joint integrity over time, implants could be developed with an enhanced biological potential and patient-specific sizing to meet individuals’ joint requirements.
The aim of this study was therefore to develop and document the preliminary findings of an implant prototype based on 3D bioprinting of human, cell-laden, patient-specific collagen scaffold for meniscus regeneration.
Materials and Methods
Isolation and expansion of mesenchymal stem cells (MSCs)
Bone marrow was obtained from the iliac crest of a patient undergoing autologous cell transplantation for the treatment of osteochondral defects. All investigations were conducted in conformity with the ethical principles of research and samples were anonymized. Bone-marrow-derived MSCs were isolated using Ficoll-Hypaque density gradient (d = 1.077 g/ml) from Pharmacia Biotech (Uppsala, Sweden) as previously reported, and were plated at a concentration of 3 × 106 cells/T150 flask.14 After seven days, adherent cells were expanded in vitro and successively plated at 3 × 105 cells/T150 flask under conventional monolayer culture conditions. Once a sufficient number of cells were available, usually after the third to fourth passage, MSCs were used for cell-laden bio-ink preparation.
Cell-laden bio-ink preparation
LifeInk 200 purified, highly concentrated Type I Collagen bio-ink was purchased from Advanced Biomatrix (San Diego, California). The cell-laden bio-ink was realized in accordance with the manufacturer’s instructions. Briefly, highly concentrated collagen was first neutralized by connecting the provided syringe through a sterile coupler to a 3 ml syringe containing 200 μl of sterile 1 M hydrochloric acid (HCl; Fisher Scientific Italia, Rodano, Italy), carefully avoiding introducing air. The plungers of the two syringes were then pushed back and forth at least 40 times to ensure thorough mixing of the collagen and HCl. The same procedure was repeated with the collagen syringe connected to a 3 ml syringe containing 200 μl of sterile 1 M sodium hydroxide (NaOH; Carlo Erba, Milan, Italy). After neutralization, the cell addition process was performed by dispensing concentrated chilled MSCs (38 × 106) to a 3 ml sterile syringe, connected through a sterile coupler to the neutralized collagen syringe. The two plungers were then pushed back and forth 40 times to ensure thorough mixing. The collagen bio-ink was kept chilled at all times.
3D modelling and bioprinting of a meniscal structure
In order to ensure that the bioprinted meniscus mimicked a natural one, the 3D model of bioengineered tissue was based on MRI scans of a human volunteer’s medial meniscus. The images were acquired using the 3Tesla Discovery MR750w GEM Magnetic Resonance imaging system (GE Healthcare, Little Chalfont, United Kingdom) with a 16-element phased-array flexible coil. The knee was scanned in the supine position with a relaxed limb. For image acquisition, a sagittal 3D fast-spin-echo (FSE) Cube scan in proton density (PD) was performed. The 3D-FSE-Cube scan in PD is a volumetric sequence with high spatial and contrast resolution. The image parameters used in the sequences are reported in Table I. The 3D-FSE-Cube sequence uses a 2D reconstruction technique based on parallel imaging (ARC, Auto Calibrating Reconstruction for Cartesian Imaging; GE Healthcare).
Table I.
MRI scan parameters for knee imaging data acquisition
| FOV, mm | Matrice | TR, ms | TE, ms | Slice thickness, mm | Bandwidth, kHz | Echo train length | NEX | Scan time, mins |
|---|---|---|---|---|---|---|---|---|
| 180 × 180 | 320 × 320 | 1500 | 32 | 0.80 | 83.33 | 60 | 1 | 6.32 |
FOV, field of view; TR, repetition time; TE, echo time; NEX, number of excitations
The Digital Imaging and Communications in Medicine (DICOM) data from the MRI imaging of the meniscus were processed using the dedicated software ‘Mimics’ (Materialise, Leuven, Belgium) in order to obtain an STL model of the structure. Starting from an automatic threshold, the model was subsequently adjusted by means of a manual segmentation process, with the help of an orthopaedic surgeon (GF), in order to reconstruct the medial meniscus 3D morphology. During this phase, an extension was added to both meniscal horns. This modification was made with the aim of favouring a possible surgical anchoring of the structure. The resulting STL model is shown in Figure 1. Later, a series of 2D cross-sections were sliced from the STL model, and tool paths were generated using computer-aided manufacturing software (BioCAM; RegenHU, Villaz-St-Pierre, Switzerland). LifeInk 200 bio-ink with embedded MSCs (38 × 106) was loaded into a disposable cartridge. The chosen 3D Discovery printing tool (RegenHU) was a microvalve-based inkjet printhead. This instrument consists of multiple printheads that have the capability to deposit different types of thermoplastic polymers and cell-laden hydrogels. A tri-axis (x,y,z) motion system enables 3D patterning of multiple materials in order to fabricate custom-made tissues in multiple shapes and sizes. An air pressure controller regulates precise dispensing of materials, and separate thermal control circuits allow the cartridge and collector temperatures to be set. Human Machine Interface (HMI) Software (RegenHU) allows different tool printing parameters to be controlled. The valve opening time was set at 190 μs and the dosing distance was set at 0.065 mm. The printing speed was set to 12 mm/s at a pressure of 0.2 bar, setting a height for each layer of 0.25 mm and a rectilinear filling pattern with 50% density. The printing process was performed in culture medium inside a sterile Petri dish, kept at 37°C.
Fig. 1.

STL model of a human meniscus.
Cell viability: LIVE/DEAD assay
Realized cell-laden constructs carrying MSCs were put onto 24-well plates, supplemented with Eagle’s minimum essential medium alpha modification (α-MEM) and cultured under conventional conditions at 37°C in a humidified atmosphere of 5% CO2 for up to 28 days. To differentiate between live and dead cells, at the end of the planned experimental times (five and 28 days), all samples were washed in Dulbecco's phosphate-buffered saline (DPBS) and then incubated in the staining solution of the LIVE/DEAD Cell Imaging Kit (Thermo Fisher Scientific, Waltham, Massachusetts) for 45 minutes. After staining, samples were washed three times in DPBS for 15 minutes and then embedded in organic cation transporter, snap-frozen in liquid nitrogen, cut into 5 µm to 10 µm sections, air-dried, and stored at -20°C. Slides were evaluated using an Eclipse 90i fluorescence microscope (Nikon, Tokyo, Japan) equipped with a digital camera.
Results
3D modelling and bioprinting of a meniscal structure
A custom-made human cell-laden collagen meniscus was realized, using MRI images of a healthy volunteer as a starting point. The selected bio-ink presented good printability and shape fidelity, allowing the fabricated tissue, obtained by means of a microvalve-based inkjet dispensing technique, to mimic the anatomical model morphology (Fig. 2). This ‘cell-friendly’ technology allowed MSCs included in the bio-ink to be homogeneously distributed within the construct.
Fig. 2.
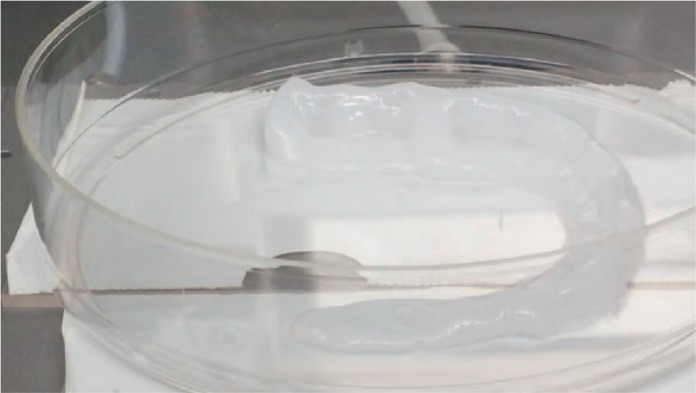
Photograph of a custom-made, human, cell-laden, high-density collagen type I meniscus prototype after mesenchymal stem cells were embedded. The printing process was performed at room temperature in a Petri dish filled with culture medium and kept at 37°C.
Cell viability: LIVE/DEAD assay
The LIVE/DEAD assay showed that at five days, only about 50% of the seeded cells were alive (Fig. 3), indicating that the bioprinting procedure could affect cell viability, perhaps due to the partially altered culture conditions occurring during this process (such as temperature and pH). However, after a culture of 28 days, almost all of the remaining cells were viable; these cells were able to grow and to colonize the biomaterial, demonstrating that the bioprinted collagen-based hydrogel scaffold provides a good microenvironment for the viability and proliferation of MSCs.
Fig. 3.

LIVE/DEAD images of cell-laden collagen type I gel scaffolds. Viable cells are in green and dead cells in red. The top row shows slides from total meniscus structure, while the bottom row shows slides from cubical constructs. Images are representative.
Discussion
The development of biomaterials that are able to stimulate meniscus regeneration is promising, and could potentially reduce the need for patients to undergo invasive surgery at a young age.10 Both synthetic and biological materials have been developed: polyurethane meniscus implants,15 silk fibrous protein scaffolds,16 and hyaluronic acid/polycaprolactone scaffold17 have been used to simulate the architecture and function of the meniscus.18 Since no comparative studies have been performed to prove the superiority of one biomaterial over others, and considering that collagen makes up 22% of the normal human meniscus,19 collagen was chosen to develop this tissue-engineered meniscus prototype.
Collagen-based hydrogels can enhance tissue regeneration by providing biochemical signals that induce cellular differentiation and migration.20,21 Cell-free scaffolds are usually preferred as strategies for meniscal replacement, in order to avoid the costs and potential risks related to cell manipulation,9 as well as the regulatory limitations that may hinder a subsequent translation in clinical practice. However, although it is not possible to draw definitive conclusions on the real effectiveness of cell augmentation from the few comparative studies that are currently available, previous animal trials have suggested that cell augmentation might provide superior regenerative potential.17,22 The combination of scaffolds and cells has therefore been investigated,9 with the aim of enhancing tissue quality. This previous research informed the approach used when creating the prototype discussed in this paper. Since inaccurate sizing can adversely affect function of a meniscal substitute,23,24 MRI-guided 3D bioprinting was used to produce a patient-specific implant.
This technology, which is based on additive manufacturing or ‘rapid prototyping’, has the ability to create complex, cellularized structures with anatomical precision, enabling the fabrication of design-specific tissue constructs. In bioprinting, small units of cells and biomaterials are dispensed with micrometre precision to form tissue-like structures. Conventional 3D printing techniques have been utilized to print temporary cell-free scaffolds for use in surgery. However, bioprinting requires a different technical approach that is compatible with depositing living cells, with the advantages of accurate control of cell distribution, high-resolution cell deposition, scalability, and cost-effectiveness. While developing a 3D bioprinted tissue, several aspects must be considered beyond the choice of material. Density is another factor that may affect the final in vivo outcome; inappropriate density might impede cellular and tissue ingrowth within the scaffold, thus delaying its incorporation and promoting an encapsulation response.25 Cell encapsulation inside collagen gels, in which the fibre network allows the physical entrapment of cells, is a commonly used method in tissue engineering. Moreover, collagen gel pore size is dependent on concentration, and therefore it may be adjusted for different applications and cell types.26
The prototype described in this study has been conceived as a 3D bioprinted, collagen-based, cell-laden scaffold. In this setting, one of the challenges faced is that a compromise must be reached in terms of temperature, in order to avoid collagen gel thermal crosslinking within cartridge and needle clogging phenomena, on the one hand, and to favour the geometric fidelity and survival rate of embedded cells, on the other. Biological and printability requirements, which often oppose each other, must both be met (i.e. conditions must fall within the ‘biofabrication window’).27-29 To reach this goal in the current study, the cartridge was kept at room temperature while printing in a support filled with culture medium kept at 37°C, as suggested by the bio-ink producer. Since cell viability is the premise for the development of a tissue-engineering strategy, cells were evaluated for up to four weeks, demonstrating the 3D bioprinter ability to deposit biomaterials in cell-friendly conditions, with the advantage of controlling both overall 3D macrostructure and cell distribution, thus overcoming the limits of other scaffold production technologies.30
This study is not without limitations. The construct should possess sufficient mechanical strength to withstand the stress generated by load in vivo, which is particularly relevant for tissue-engineered meniscus.31 While the requirement of biomechanical property should also be kept in mind for a structure that plays a key role in joint load distribution, this aspect has not been investigated. The bioprinting technology used did not allow the complex structure and organization of the collagenous matrix, which is crucial for the meniscus to withstand the mechanical function of load-bearing under physiological conditions, to be recreated.32 Future application of this prototype in a bioreactor-based tissue engineering strategy should provide the necessary stimuli to induce physiological fibre alignment and zonal organization, as previously shown in other tissue-engineering models.33-35 Finally, while MSCs have been used in this study as meniscal substitute, other cell sources should also be explored and compared to optimize this construct, and to ensure that it is as similar as possible to a native meniscus.36,37
The prototype described in this study showed the biological potential of 3D bioprinting technology in providing an anatomically shaped, patient-specific construct with viable cells on a biocompatible material. This study could act as the starting point for future developments of this custom-made, collagen-based, tissue-engineered structure, which could aid the optimization of implants designed to replace damaged menisci.
Acknowledgments
The authors would like to thank Patrizia Rappini for her assistance in the preparation of the manuscript.
Footnotes
Author contributions: G. Filardo: Designed the study, Carried out the modelling, Wrote the manuscript.
M. Petretta: Carried out the 3D modelling and scaffold fabrication.
C. Cavallo: Responsible for cell cultures.
L. Roseti: Analyzed the data.
S. Durante: Acquired the MRI images.
U. Albisinni: Validated the MRI images.
B. Grigolo: Supervised the study.
Follow us @BoneJointRes
Funding statement
This study was funded by Progetto Regione Emilia-Romagna POR-FESR 2014-2020: CUSTOM IMPLANTS – “Progettazione e realizzazione di tessuti e endoprotesi su misura mediante tecnologie sottrattive e additive custom made” and 5x1000 funds, Italian Ministry of Health “Piattaforma integrata di studi preclinici per lo studio e lo sviluppo di biomateriali multifunzionali e di terapie adiuvanti per la chirurgia ricostruttiva e rigenerativa dell'apparato muscoloscheletrico”.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1. Heijink A, Gomoll AH, Madry H, et al. Biomechanical considerations in the pathogenesis of osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2012;20:423-435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Abrams GD, Frank RM, Gupta AK, et al. Trends in meniscus repair and meniscectomy in the United States, 2005-2011. Am J Sports Med 2013;41:2333-2339. [DOI] [PubMed] [Google Scholar]
- 3. Lamplot JD, Brophy RH. The role for arthroscopic partial meniscectomy in knees with degenerative changes: a systematic review. Bone Joint J 2016;98-B:934-938. [DOI] [PubMed] [Google Scholar]
- 4. Hoben GM, Athanasiou KA. Meniscal repair with fibrocartilage engineering. Sports Med Arthrosc Rev 2006;14:129-137. [DOI] [PubMed] [Google Scholar]
- 5. Bin SI, Nha KW, Cheong JY, Shin YS. Midterm and long-term results of medial versus lateral meniscal allograft transplantation: a meta-analysis. Am J Sports Med 2017;1:363546517709777. [DOI] [PubMed] [Google Scholar]
- 6. Smith NA, Parsons N, Wright D, et al. A pilot randomized trial of meniscal allograft transplantation versus personalized physiotherapy for patients with a symptomatic meniscal deficient knee compartment. Bone Joint J 2018;100-B:56-63. [DOI] [PubMed] [Google Scholar]
- 7. Rath E, Richmond JC, Yassir W, Albright JD, Gundogan F. Meniscal allograft transplantation. Two- to eight-year results. Am J Sports Med 2001;29:410-414. [DOI] [PubMed] [Google Scholar]
- 8. Nordberg RC, Charoenpanich A, Vaughn CE, et al. Enhanced cellular infiltration of human adipose-derived stem cells in allograft menisci using a needle-punch method. J Orthop Surg Res 2016;11:132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Di Matteo B, Perdisa F, Gostynska N, et al. Meniscal scaffolds - preclinical evidence to support their use: a systematic review. Open Orthop J 2015;9:143-156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Filardo G, Andriolo L, Kon E, de Caro F, Marcacci M. Meniscal scaffolds: results and indications. A systematic literature review. Int Orthop 2015;39:35-46. [DOI] [PubMed] [Google Scholar]
- 11. Filardo G, Kon E, Perdisa F, et al. Polyurethane-based cell-free scaffold for the treatment of painful partial meniscus loss. Knee Surg Sports Traumatol Arthrosc 2017;25:459-467. [DOI] [PubMed] [Google Scholar]
- 12. Shin YS, Lee HN, Sim HB, Kim HJ, Lee DH. Polyurethane meniscal scaffolds lead to better clinical outcomes but worse articular cartilage status and greater absolute meniscal extrusion. Knee Surg Sports Traumatol Arthrosc 2018;26:2227-2238. [DOI] [PubMed] [Google Scholar]
- 13. Ali AM, Newman SDS, Hooper PA, Davies CM, Cobb JP. The effect of implant position on bone strain following lateral unicompartmental knee arthroplasty: A biomechanical model using digital image correlation. Bone Joint Res 2017;6:522-529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Grigolo B, Lisignoli G, Desando G, et al. Osteoarthritis treated with mesenchymal stem cells on hyaluronan-based scaffold in rabbit. Tissue Eng Part C Methods 2009;15:647-658. [DOI] [PubMed] [Google Scholar]
- 15. Verdonk R, Verdonk P, Huysse W, Forsyth R, Heinrichs EL. Tissue ingrowth after implantation of a novel, biodegradable polyurethane scaffold for treatment of partial meniscal lesions. Am J Sports Med 2011;39:774-782. [DOI] [PubMed] [Google Scholar]
- 16. Mandal BB, Park SH, Gil ES, Kaplan DL. Multilayered silk scaffolds for meniscus tissue engineering. Biomaterials 2011;32:639-651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kon E, Filardo G, Tschon M, et al. Tissue engineering for total meniscal substitution: animal study in sheep model—results at 12 months. Tissue Eng Part A 2012;18:1573-1582. [DOI] [PubMed] [Google Scholar]
- 18. Scotti C, Hirschmann MT, Antinolfi P, Martin I, Peretti GM. Meniscus repair and regeneration: review on current methods and research potential. Eur Cell Mater 2013;26:150-170. [DOI] [PubMed] [Google Scholar]
- 19. Tan GK, Cooper-White JJ. Interactions of meniscal cells with extracellular matrix molecules: towards the generation of tissue engineered menisci. Cell Adhes Migr 2011;5:220-226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Gillette BM, Jensen JA, Tang B, et al. In situ collagen assembly for integrating microfabricated three-dimensional cell-seeded matrices. Nat Mater 2008;7:636-640. [DOI] [PubMed] [Google Scholar]
- 21. Park JY, Choi JC, Shim JH, et al. A comparative study on collagen type I and hyaluronic acid dependent cell behavior for osteochondral tissue bioprinting. Biofabrication 2014;6:035004. [DOI] [PubMed] [Google Scholar]
- 22. Kang SW, Son SM, Lee JS, et al. Regeneration of whole meniscus using meniscal cells and polymer scaffolds in a rabbit total meniscectomy model. J Biomed Mater Res A 2006;78:659-671. [DOI] [PubMed] [Google Scholar]
- 23. Dienst M, Greis PE, Ellis BJ, Bachus KN, Burks RT. Effect of lateral meniscal allograft sizing on contact mechanics of the lateral tibial plateau: an experimental study in human cadaveric knee joints. Am J Sports Med 2007;35:34-42. [DOI] [PubMed] [Google Scholar]
- 24. Sekaran SV, Hull ML, Howell SM. Nonanatomic location of the posterior horn of a medial meniscal autograft implanted in a cadaveric knee adversely affects the pressure distribution on the tibial plateau. Am J Sports Med 2002;30:74-82. [DOI] [PubMed] [Google Scholar]
- 25. Mironov V, Kasyanov V, Markwald RR. Organ printing: from bioprinter to organ biofabrication line. Curr Opin Biotechnol 2011;22:667-673. [DOI] [PubMed] [Google Scholar]
- 26. Mandal BB, Park SH, Gil ES, Kaplan DL. Multilayered silk scaffolds for meniscus tissue engineering. Biomaterials 2011;32:639-651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Malda J, Visser J, Melchels FP, et al. 25th anniversary article: engineering hydrogels for biofabrication. Adv Mater 2013;25:5011-5028. [DOI] [PubMed] [Google Scholar]
- 28. Markstedt K, Mantas A, Tournier I, et al. 3D bioprinting human chondrocytes with nanocellulose-alginate bioink for cartilage tissue engineering applications. Biomacromolecules 2015;16:1489-1496. [DOI] [PubMed] [Google Scholar]
- 29. Murphy SV, Skardal A, Atala A. Evaluation of hydrogels for bio-printing applications. J Biomed Mater Res A 2013;101:272-284. [DOI] [PubMed] [Google Scholar]
- 30. Nakamura M, Iwanaga S, Henmi C, Arai K, Nishiyama Y. Biomatrices and biomaterials for future developments of bioprinting and biofabrication. Biofabrication 2010;2:014110. [DOI] [PubMed] [Google Scholar]
- 31. Zhang ZZ, Jiang D, Ding JX, et al. Role of scaffold mean pore size in meniscus regeneration. Acta Biomater 2016;43:314-326. [DOI] [PubMed] [Google Scholar]
- 32. López-Calzada G, Hernandez-Martínez AR, Cruz-Soto M, et al. Development of meniscus substitutes using a mixture of biocompatible polymers and extra cellular matrix components by electrospinning. Mater Sci Eng C 2016;1:893-905. [DOI] [PubMed] [Google Scholar]
- 33. Puetzer JL, Ballyns JJ, Bonassar LJ. The effect of the duration of mechanical stimulation and post-stimulation culture on the structure and properties of dynamically compressed tissue-engineered menisci. Tissue Eng Part A 2012;18:1365-1375. [DOI] [PubMed] [Google Scholar]
- 34. Puetzer JL, Bonassar LJ. Physiologically distributed loading patterns drive the formation of zonally organized collagen structures in tissue-engineered meniscus. Tissue Eng Part A 2016;22:907-916. [DOI] [PubMed] [Google Scholar]
- 35. Huey DJ, Athanasiou KA. Tension-compression loading with chemical stimulation results in additive increases to functional properties of anatomic meniscal constructs. PLoS One 2011;6:e27857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. McCorry MC, Puetzer JL, Bonassar LJ. Characterization of mesenchymal stem cells and fibrochondrocytes in three-dimensional co-culture: analysis of cell shape, matrix production, and mechanical performance. Stem Cell Res Ther 2016;12:7:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Moradi L, Vasei M, Dehghan MM, et al. Regeneration of meniscus tissue using adipose mesenchymal stem cells-chondrocytes co-culture on a hybrid scaffold: in vivo study. Biomaterials 2017;126:18-30. [DOI] [PubMed] [Google Scholar]