

Description
A 53-year-old woman presented with a right nipple non-pruritic lesion of 7 years’ duration, which has been slowly growing over the few months. There was no associated nipple discharge or breast lump. The patient denied any previous breast surgery or trauma. On examination, there was a non-tender, non-pigmented lesion occupying nearly half of the nipple (figure 1). The rest of the breast and systemic examination were unremarkable.
Figure 1.

Close-up view of the right nipple lesion (outlined in black).
Mammogram and right breast ultrasound were normal. In view of the patient’s age and slowly growing nature of the lesion, histological assessment of the lesion was offered. The patient declined a punch biopsy and underwent an excision biopsy of the right nipple lesion. Histology revealed a 9 mm eccrine poroma with no evidence of malignancy (figure 2A,B). She recovered well postoperatively and was hence discharged.
Figure 2.
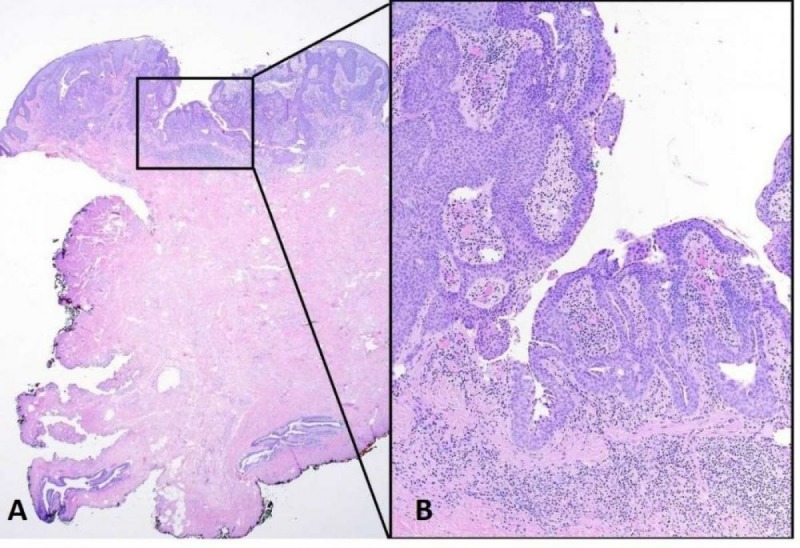
(A) The eccrine poroma showed an epidermal and dermal components of anastomosing trabeculae of epithelial cells containing ductal structures. The epidermis was focally disrupted, exposing the ductal tunnelling structure (H&E; ×20 magnification). (B) The trabeculae of basaloid, rounded and uniform epithelial cells were surmounted by an attenuated layer of cuboidal ductal cells (H&E; ×100 magnification).
Eccrine poroma was first described in 1956.1 It is a rare benign adnexal tumour which arises from sweat glands of eccrine origin. It tends to present as a non-pigmented lesion, typically found on acral sites such as the soles and palms. It is more prevalent in the 40–60 years old age group, with no gender preference.
Its pathogenesis is largely unknown, but may be secondary to trauma, radiation or scars which were not present in our patient.
Histologically, benign eccrine duct tumours are readily recognisable distinct entities.2 They are designated as benign lesions due to their lack of cytologic atypia and mitotic activity, as witnessed in our patient. The three potential differentials within this family are hidroacanthoma simplex, dermal duct tumour and eccrine hidradenoma. Hidroacanthoma simplex consists of discrete circumscribed populations of cells within an irregularly acanthotic epidermis. Unlike eccrine poromas, the ducts are rudimentary and not as prominent. The other differential, the dermal duct tumour is almost histologically similar to eccrine poroma, except for the distinct lack of any communication with the overlying epidermis. Eccrine hidradenoma, also known as eccrine acrospiroma, consists of a similar composition of cells with the exception of the ‘ducts’ appearing as large and small cystic spaces, in contrast to the ‘tunnelling system’ of ducts seen in eccrine poromas.
In view of its rarity, the natural history of eccrine poroma is little known. Rarely, in about 18 % of cases, eccrine poroma may undergo malignant transformation,3 presenting with recent changes of ulceration, bleeding, sudden growth or in a non-specific fashion. Our patient’s presentation was similar to that described in the literature except that it had an atypical site and was slowly growing.
In cases of eccrine porocarcinoma, wide local excision is recommended and have a cure rate of 70%–80%.3 Metastasis can occur in 20%–26% of patients, with the lymph nodes being the most common affected site in 60% of cases.3 In such cases, a clearance of the affected lymph nodes may be required. Histological features such as increased mitosis, lymphovascular invasion and tumour depth >7 mm were correlated to a worse prognosis.4 Metastatic eccrine porocarcinoma tends to be chemotherapy resistant but docetaxel treatment may result in a response.5
Learning points.
This is the first known reported case of eccrine poroma of the nipple.
Eccrine poroma can often be clinically confused with other skin conditions.
Histological diagnosis should be obtained to exclude sinister causes such as Paget’s disease.
Footnotes
Contributors: GHL was the consultant overseeing the care of the patient. FAR contributed to the initial draft writing and AW provided the histological figures and interpretation. All authors contributed to the final editing of the draft.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Obtained.
References
- 1. Bombonato C, Piana S, Moscarella E, et al. . Pigmented eccrine poroma: dermoscopic and confocal features. Dermatol Pract Concept 2016;6:59–62. 10.5826/dpc.0603a12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Kakinuma H, Miyamoto R, Iwasawa U, et al. . Three subtypes of poroid neoplasia in a single lesion: eccrine poroma, hidroacanthoma simplex, and dermal duct tumor. Histologic, histochemical, and ultrastructural findings. Am J Dermatopathol 1994;16:66–72. [DOI] [PubMed] [Google Scholar]
- 3. Salih AM, Kakamad FH, Essa RA, et al. . Porocarcinoma: a systematic review of literature with a single case report. Int J Surg Case Rep 2017;30:13–16. 10.1016/j.ijscr.2016.10.051 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Robson A, Greene J, Ansari N, et al. . Eccrine porocarcinoma (malignant eccrine poroma): a clinicopathologic study of 69 cases. Am J Surg Pathol 2001;25:710–20. [DOI] [PubMed] [Google Scholar]
- 5. Plunkett TA, Hanby AM, Miles DW, et al. . Metastatic eccrine porocarcinoma: response to docetaxel (Taxotere) chemotherapy. Ann Oncol 2001;12:411–4. 10.1023/A:1011196615177 [DOI] [PubMed] [Google Scholar]