

Abstract
To measure the correlation between neural response threshold (NRT) and most comfortable level for behavioural response (MCLB) whichever is better for rehabilitation purpose and to calculate the impedance of the electrode in cochlear implant recipient. Mapping may be done by various methods here we did by NRT and behavioral observation audiometry (BOA). NRT is technique by which we measure the response from the auditory nerve using the hi-resolution bionic ear system. Neural response measurement depends on the-neural tissue, stimulus used and recording technique. BOA is used for observing motor response on presenting sound to the implanted child. Most comfortable level for behavioural response (MCLB) is calculated for behavioural response. It measures the useful information about low frequency hearing, it provides more information about the hearing of neurologically immature babies giving indication of uncomfortable loudness levels. The NRT and MCLB is calculated for 2nd, 6th, and 11th electrode for all patients in our study. Auditory response threshold is better for rehabilitations then behavioural observation audiometry for Cochlear implant patients. Mean value and standard deviation of neural response threshold (NRT) (qu) are 10.23, 3.67; 11.27, 4.39; 10.71, 3.88 at 2nd, 6th, and 11th electrode respectively. Mean value and standard deviation of Most comfortable level for behavioral response (qu) are 20.49, 7.08; 21.26, 7.31; 21.01, 6.03 at 2nd, 6th and 11th electrode respectively. NRT is better for post-operative rehabilitations and MCL and threshold vary with different electrode and in different patients.
Keywords: Cochlear Implant, Neural response threshold, Behavioural observation audiometry, Most comfortable level for behavioural response, Impedance
Introduction
Cochlear Implant was not so common in 1980, it was a rare in Bharat and in approach of affluent class of society only. The 1st Cochlear Implant in Bharat was probably done in 1986. Every year 18,000 children are nearly born with deafness in Bharat [1]. Out of this 50% are treatable with cochlear implant. Cochlear Implant is the most beautiful gift of science to hearing DIVAYANG. Cochlear Implant has good success rate in our country.
As soon as implant is done, in the intraoperative period mapping of implant is done for the compatibility, its placement and working status, then and there. In the present study which was carried out in tertiary centre of eastern India.
Long term reliabili™ 18 year from 0.900 to 0.988 for unilateral implant and from 0.9810 to 0.976 for bilateral implant [2].
Cochlear Implant was never done in the Institute before 2014, out of all cases, 30 cases of the implant have been selected for the study.
Materials and Methods
This study was conducted on 30 patients who had gone through cochlear implant surgery in a tertiary care centre of eastern India. The age of patient ranged from 3 year to 12 year, of both sexes of different religion and varying socio-economic status were included in study.
Detailed history was taken followed by clinical examination. Patients were investigated by audiological test name by BOA, PTA, Impedance audiometry and BERA. Radiological imaging which included C.T. Scan temporal bone, 3D Cochlea imaging and MRI Brain. Rest haematological, paediatric, psychological examination was done for fitness of anaesthesia and cochlear implant candidacy. All patient was immunised by pneumococcal and hemophilus influenza B vaccination. This was a time bound study which has been done on patients operated during August 2016 to July 2018.
Inclusion Criteria
Only those cases were registered, who gave consent for the study.
Patients who had prelingual bilateral severe to profound hearing loss, without any congenital anomaly.
Patients below 12 years of age and of both the sexes were included.
Exclusion Criteria
Patients who had bilateral severe hearing loss, prelingually or postlingually above 12 years of age. Also those who had some congenital anomaly.
Out of 30 patients 28 patients had gone through surgery by VERIA technique or transcanal approach, rest are done by posterior tympanotomy approach under general anaesthesia. All cases were uneventful.
In our study Implant with two type of electrode Standard and Flexsoft were used in different patient. It has 12 pair of electrode. Three type of outer processor unit; Opus II, Rondo, sonnet is used in different patient. Intra operative neural response telemetry done to check proper electrode function and all electrode response. For proper function and better response regular mapping was done by NRT and BOA. Software MAESTRO max version 7.0.1 Build 6389.22322 was used.
After 4 week of surgery outer speech processor unit was switched on. NRT at the time of switch on of the implant and regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post switch on then once in year after the switch on was carried out. Patient also underwent behavioral observation audiometry (BOA) at time of switch on and regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year, then once in year post switch on.
BOA is used for observing motor response on presenting sound to the implanted child. In BOA most comfortable level for behavioral response (MCLB) of the electrode of implanted patient are recorded. In this study 2nd, 6th and 11th electrode were selected to see the response of various parameters.
In this study impedance (IMP), NRT, most comfortable level for behavioral response (MCLB) of the electrode of implanted patients are selected to see the response of different patient at 2nd, 6th and 11th electrode at above mentioned time.
For statistical analysis mean and standard deviation was calculated for all parameter at 2nd, 6th and 11th electrode. p value and correlation analysis was done for various parameters.
Observation and Results
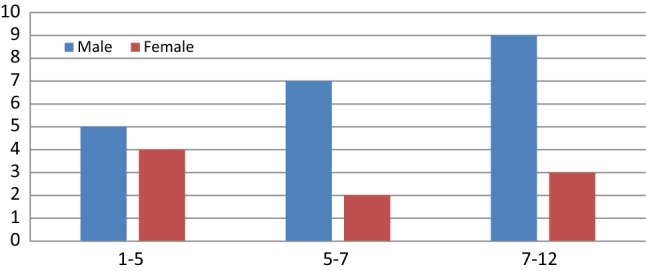
Most commonly patient was age group belonged to age group 7–12 year and males outnumbered females in all age group (Graph 1).
Graph 1.
Age Group Distribution
Most cases operated for cochlear implant were from urban area (Graph 2).
Graph 2.

Residential status
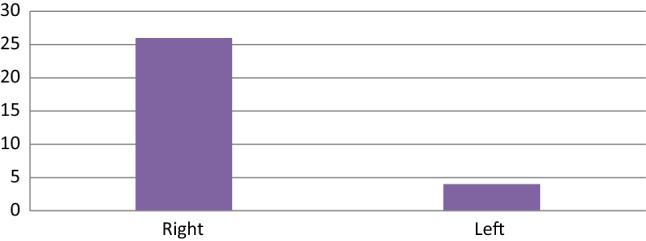
Out of 30 patients, 26 patients were implanted on right side and 4 patients on left side (Graph 3).
Graph 3.
Implanted Site
In our study Implant with two type of electrode Standard and Flexsoft used in different patient. In 12 patients standard electrode and 18 patients Flexsoft electrode were used. Both had 12 pair of electrode (Graph 4).
Graph 4.

Electrode used
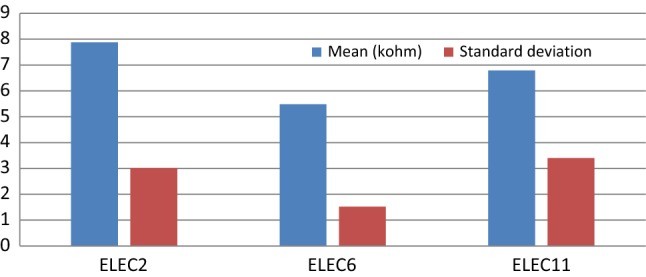
Mean value and standard deviation of impedance at electrode 2nd, 6th, 11th are shown in Table 1 and Graph 5. Mean and SD of impedance are 7.88, 3.01; 5.48, 1.52; 6.79, 3.4 at 2nd, 6th and 11th electrodes respectively.
Table 1.
Impedance (IMP)
| Electrode | Mean (kΩ) | SD |
|---|---|---|
| 2 | 7.88 | 3.01 |
| 6 | 5.48 | 1.52 |
| 11 | 6.79 | 3.40 |
Graph 5.
Impedance (IMP)
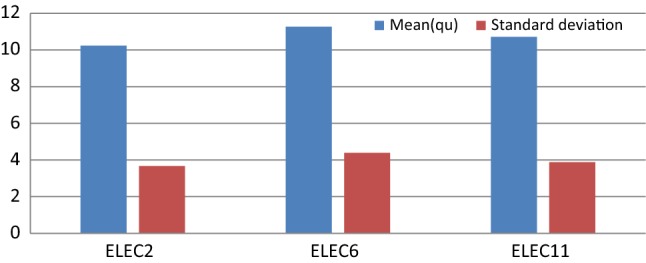
Mean value and SD of NRT at electrode 2nd, 6th, 11th are shown in Table 2 and Graph 6. Mean value and standard deviation of auditory/NRT are 10.23, 3.67; 11.27, 4.39; 10.71, 3.88 at 2nd, 6th, and 11th electrode respectively.
Table 2.
Neural response threshold (NRT)
| Electrode | Mean (qu) | SD |
|---|---|---|
| 2 | 10.23 | 3.67 |
| 6 | 11.27 | 4.39 |
| 11 | 10.71 | 3.88 |
Graph 6.
Neural Response Threshold (NRT)
Mean value and SD of most comfortable level for behavioral response at electrode 2nd, 6th, 11th are shown in Table 3 and Graph 7. Mean value and standard deviation of most comfortable level for behavioral response are 20.49, 7.08; 21.26, 7.31; 21.01, 6.03 at 2nd, 6th and 11th electrode respectively.
Table 3.
Most comfortable level for behavioral response (MCLB)
| Electrode | Mean (qu) | SD |
|---|---|---|
| 2 | 20.49 | 7.08 |
| 6 | 21.26 | 7.31 |
| 11 | 21.01 | 6.03 |
Graph 7.

Most comfortable leval for Behavioral Response (MCLB)
A significant correlation is present between NRT and MCLB at electrode 6th and 11th at 0.01 level, there is no correlation at 2nd electrode. It is shown in Table 4 and Graph 8.
Table 4.
Correlation between NRT and MCLB
| Electrode | Correlation | p value | N |
|---|---|---|---|
| 2 | 0.211 | 0.263 | 30 |
| 6 | 0.505 | 0.004** | 30 |
| 11 | 0.468 | 0.009** | 30 |
**Correlation is significant at 0.01 level
*Correlation is significant at 0.05 level
Graph 8.
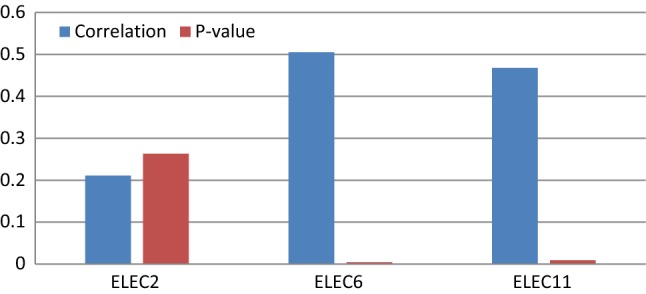
Correlation Between NRT and MCLB
A significant correlation between NRT and MCLB is shown on scatter plot at 2nd, 6th and 11th electrode.
There is no significant between IMP and NRT at 2nd and 11th electrode, negative correlation at 6th electrode as shown in Table 5 and Graph 9.
Table 5.
Correlation between IMP and NRT
| Electrode | Correlation | p value | N |
|---|---|---|---|
| 2 | 0.065 | 0.732 | 30 |
| 6 | − 0.190 | 0.314 | 30 |
| 11 | 0.314 | 0.941 | 30 |
Graph 9.
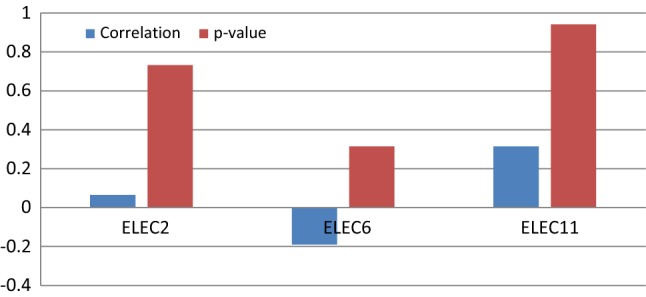
Correlation Between IMP and NRT
Discussion
In our study 22 patients belonged to urban and eight patients belonged to rural residential status. Thus we can say more awareness program are needed for the rural areas.
In Mittal et al. [3] the patients operated for cochlear implant of age group 1–5 year was 10%, 5–7 year was 56%, 7–9 year was 24%. In our study patients of age group 1–5 year was 30%, 5–7 year was 30%, 7–12 year was 40%. In our study predominately males were operated [3].
26 patients were operated on right side and 4 patients were operated on left side of ear.
In our study 28 cases were operated by VERIA technique and two cases operated by posterior tympanotomy approach with electrode insertion at anterio-inferior to round window membrane.
Kim et al. [4] stated that regular habilitation programs including regular mapping, auditory and speech therapy and periodic evaluation of development should be done with active participation of parents and family member. In our study regular Mapping is done by software MAESTRO max version 7.0.1 Build 6389.22322. After 4 week of surgery Implant was switched on and outer speech processor unit is installed. Auditory response threshold (ART) time of switch on of the implant and follow up regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post operatively then once in year after the switch on [5].
BOA is used for observing motor response on presenting sound to the implanted child. In BOA most comfortable level for behavioral response (MCLB) of the electrode of implanted patient was recorded same as above time duration postoperatively.
Driver et al. [4] sated children will need regular reviewing and reprogramming as they adapt to the stimulation which is delivered through the external speech processor called mapping. In our study regular mapping is done post operatively regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post operatively then once in year after the switch on [4].
Telmesani et al. [6] Mapping includes the regular programming of minimum and maximum stimulation levels that are based and based on subjective measurements of threshold and most comfortable levels. In our study mapping was done and following parameters were recorded Most comfort level, NRT, Most comfort level for behavioral response, Threshold and Impedance of the 2nd, 6th and 11th electrode [6].
Koch et al. [7], neural response telemetry is the method by which one can measure responses from the auditory nerve using the high-resolution bionic ear system i.e. cochlear implant. Electrical auditory brainstem responses were recorded at electrode of apical, middle and basal area of cochlea using medical implant. In our study mapping is done to record the most comfort level, NRT, most comfort level for behavioral response, threshold and impedance at 2nd, 6th and 11th electrode [7].
Mittal et al. [3], the threshold level were based on consistent response to the conditioning activities. However, the most comfortable levels were measured by loudness-scaling procedure.
Cochlear et al. [8], intra-operative NRT in conjunction with electrode impedance data indicate the integrity of the implanted electrode and the electrode/auditory nerve interface, confirming on the OT table that the implant is functioning correctly. In our study intra-operative NRT is done to check all electrode threshold and their response at all electrode [8].
Cochlear et al. [8], the post-operative T-NRT levels also significantly correlated with behavioral T and C-levels, with the T-NRT levels usually lying between the T- and C-levels. In our study there is significant correlation is present between NRT and most comfortable level for behavioral response at electrode 6th and 11th at 0.01 level, there is no correlation at 2nd electrode [8].
Kasim et al. [9], intra-operative NRT in conjunction with electrode impedance data help to indicate the integrity of the implanted electrode confirming that the implants are working correctly. In our study intraoperative NRT is done to check the response of all electrode just after fixing and insertion of the electrode [9].
Kasim et al. [9], mapping was done at periodic intervals until a stable map was achieved. In our study regular mapping is done post operatively regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post operatively then once in year after the switch on [9].
Kasim et al. [9] show that significant correlation between NRT and predicated T and C-levels. In our study there is significant correlation between most comfortable level and NRT at 0.01 level at 11th electrode, at 0.05 level at 2nd and 6th electrode and there is no correlation between threshold and NRT at 6th and 11th electrode, there is negative correlation at 2nd electrode [9].
Kasim et al. [9] has reported that the correlation between NRT level and behavioral T and C-levels improved with time in children. In our study a significant correlation is present between NRT and most comfortable level for behavioral response at electrode 6th and 11th at 0.01 level, there is no correlation at 2nd electrode [9].
Summary and Conclusion
Our findings are summarized as follows:
In our study 22 patient belonged to urban and 18 patients belonged to rural residential status. Thus we can say more awareness program about implant are needed for the rural areas.
In our study patients of age group 1–5 year was 30%, 5–7 year was 30%, 7–12 year was 40%. In our study predominately males were operated.
26 patients were operated on right side and 4 patients were operated on left side of ear.
In our study multichannel 12 pair electrodes, including standard and Flexsoft type electrode was used. 12 patients implanted with standard electrode and 18 patients by Flexsoft electrode.
In our study 28 cases were operated by VERIA technique and two cases operated by posterior tympanotomy approach with electrode insertion at anterio-inferior to round window membrane.
In our study regular Mapping is done by software MAESTRO max version 7.0.1 Build 6389.22322. After 4 week of surgery Implant was switched on and outer processor unit is installed. Auditory response threshold (ART) time of switch on of the implant and follow up regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post operatively then once in year after the switch on.
BOA is used for observing motor response on presenting sound to the implanted child. In BOA most comfortable level for behavioral response (MCLB) of the electrode of implanted patient was recorded same as above time duration postoperatively.
Mapping was done post operatively regularly at 1 week, 2 weeks, 4 weeks, 6 weeks, 10 weeks, 18 weeks, 3 months, 6 months, 1 year post operatively then once in year after the switch on.
Complete insertion of electrode into scala tympani through cochleostomy anterio-inferior to round window membrane was done which bypassed the damaged inner ear to stimulate the auditory nerve.
Intraoperative NRT is done to check the response of all electrode just after fixing and insertion of the electrode.
Mapping was done and following parameters were recorded NRT, most comfort level for behavioral response, and impedance of the 2nd, 6th and 11th electrode.
Mean and SD of NRT, most comfort level for behavioral response and impedance are calculated at 2nd, 6th and 11th electrode.
Mean and SD of impedance are 7.88, 3.01; 5.48, 1.52; 6.79, 3.4 at 2nd, 6th and 11th electrodes respectively.
Mean value and SD of NRT are 10.23, 3.67; 11.27, 4.39; 10.71, 3.88 at 2nd, 6th, and 11th electrode respectively.
Mean value and SD of most comfortable level for behavioral response are 20.49, 7.08; 21.26, 7.31; 21.01, 6.03 at 2nd, 6th and 11th electrode respectively.
There is significant correlation present between NRT and most comfortable level for behavioral response at electrode 6th and 11th at 0.01 level, there is no correlation at 2nd electrode.
References
- 1.Singh V. Newborn hearing screening: present scenario. Indian J Community Med. 2015;40(1):62–65. doi: 10.4103/0970-0218.149274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Soli SD, Zheng Y. Long-term reliability of pediatric cochlear implants. Otol Neurotol. 2010;31(6):899–901. doi: 10.1097/MAO.0b013e3181d2f069. [DOI] [PubMed] [Google Scholar]
- 3.Mittal R, Panwar SS, Nair S, Sinha VR, Ramesh AV, Nilkanthan A, Raj P. Mapping of pediatric cochlear implant recipients using electrical auditory brainstem responses as a tool. Int Otol. 2015;21:14–18. doi: 10.4103/0971-7749.152852. [DOI] [Google Scholar]
- 4.Driver S, Jiang D. Paediatric cochlear implantation factors that affect outcomes. Eur J Paediatr Neurol. 2017;21:104–108. doi: 10.1016/j.ejpn.2016.07.012. [DOI] [PubMed] [Google Scholar]
- 5.Kim L-S, Jeong S-W, Lee Y-M, Kim J-S. Cochlear implantation in children. Auris Nasus Larynx. 2009;37(1):6–17. doi: 10.1016/j.anl.2009.09.011. [DOI] [PubMed] [Google Scholar]
- 6.Telmesani LM, Said NM. Electrically evoked compound action potential (ECAP) in cochlear implant children: changes in auditory nerve response in first year of cochlear implant use. Int J Pediatr Otorhinolaryngol. 2016;82:28–33. doi: 10.1016/j.ijporl.2015.12.027. [DOI] [PubMed] [Google Scholar]
- 7.Koch DB, Overstreet EH. Neural response imaging: measuring auditory-nerve responses from the cochlea with the hi-resolution bionic ear system. Bengaluru: Advanced Bionics Corporation; 2003. [Google Scholar]
- 8.Clinical applications of nucleus NRT (2011) Neural Response Telemetry. Cochlear, Australia
- 9.Kasim KS, Abdullah AB, Hashim WF. Correlation between neural response telemetry (NRT) measurement level and behavioral (T-level and C-level) in prelingual cochlear implant patients. J Atolarynol. 2013;3:3. [Google Scholar]