

Abstract
Objective:
This study characterized 3- to 6-year-old children’s understanding of death as a function of depression status, suicidal ideation (SI), and media consumption.
Method:
Participants were 79 depressed children (aged 3.0–6.11), who completed a comprehensive psychiatric assessment and experimenter-led death interview, and a comparison group of 60 healthy children (aged 4.0–7.12). The interview assessed children’s understanding of five concepts of death: universality, applicability, irreversibility, cessation, and causality. Children’s mastery of each concept, and overall death understanding, was examined as a function of depression and SI-status: depressed with SI (N=22), depressed without SI (N=57), and healthy (N=60). Children’s observed emotional reactions to hearing about natural death, accidental death, and suicide were assessed via death-themed stories. Parent-reports of children’s television and videogames/internet consumption assessed links between media exposure and death understanding.
Results:
Depressed children with SI scored higher on overall death understanding than depressed without SI and healthy children. They also exhibited more sad and anxious affect listening to death-themed stories and were more likely to describe death as caused by violence. Across our sample, older children were also more likely to depict death as violent. More television use was associated with less understanding of death, including the concept of irreversibility.
Conclusions:
Depressed children with SI have a more advanced understanding of death than their peers dispelling the myth that these ideations arise in the context of poor death understanding. The increase in violence attributions across early childhood may indicate increasing normalization of violence in children’s perceptions of death. A Randomized Controlled Trial of PCIT-ED For Preschool Depression; http://clinicaltrials.gov; NCT00595283
Keywords: early childhood, depression, suicidality, death understanding, media
Lay Summary:
This study characterized 3- to 6-year-old children’s understanding of death in a sample of children with Major Depressive Disorder. The sample included 22 depressed children with suicidal ideation (i.e., children who had expressed passive thoughts of one’s own death such as “I wish I were dead” and/or active thoughts or plans to end one’s life such as “I am going to kill myself”), 57 depressed children without suicidal ideation, and 60 healthy children. Depressed children with suicidal ideation demonstrated a better understanding of death than either peer group, refuting common assumptions that children who express suicidal ideation have a “less mature” understanding of death. Children with suicidal ideation were also 3.57 times more likely to describe death as caused by violence than depressed children without suicidal ideation, potentially indicating the normalization of violence in children’s perceptions of death.
Introduction
Recurrent thoughts of death and suicidal ideation are diagnostic symptoms of Major Depressive Disorder (MDD) in both children and adults.1 Recent research indicates that preschoolers with depression are four times more likely than either healthy or anxious peers to have thoughts of death,2 raising important developmental questions about the content and veracity of young children’s understanding of death in this context. Whereas little is known about how children with depression conceptualize death, there is a substantial basic developmental literature on this topic. This research offers a compelling account of the broad stability and universality of children’s acquisition of concepts that, together, comprise a mature understanding of death in Western culture. Understanding whether depressed young children understand death is an important issue in determining clinical response to expression of suicidal thoughts and behaviors in this age group.
Mature adults recognize that death occurs to all living–and only–living things, is inevitable and irreversible, and fundamentally results from a breakdown of bodily functions. Although children do not demonstrate a full understanding of the biological basis of death until around 7 years of age, by age 4 children begin to distinguish between things that do and do not die, and by 5 or 6 understand that death is a permanent irreversible state.3 Several studies have found that direct personal experiences, such as the death of a grandparent,4,5 or suffering from protracted serious physical illness,4,6 can influence the rate of acquisition of specific relevant concepts. However, in general, the developmental trajectory of death understanding is highly robust, with children demonstrating mastery of each death concept in a relatively fixed sequential order.3,7
Leading work on how children acquire these concepts has focused on children’s integration of death into their developing theories of folk biology. Specifically, children’s understanding of death changes from an initial notion of death as a behavior (e.g., sleeping, going away) to conceptualizing death a biological phenomenon, in parallel to acquiring the knowledge that life is governed by biological processes (see Slaughter, 2005 for a review). However, as children with depression think about death more than their non-depressed peers,2 we sought to investigate whether their death understanding is also more or less advanced than that of their healthy developing peers. This issue is important to understanding whether expressions of suicidal thoughts and behaviors in depression young children might represent a real wish and understanding of ending their lives.
Recent research also indicates links between persistent thoughts of death and/or suicide with later school-age suicidal ideation (SI) in young children.8 Recent reports issued by the Centers for Disease Control indicate that childhood suicide is at a 30 year high,9 and suicide in 10- to 14-year-olds has surpassed motor vehicle injury and homicide to become a leading cause of death in late childhood and early adolescence.10 These statistics highlight the pressing need to understand how young children with SI perceive death. Suicidal thoughts in young children can include detailed plans to end one’s life, and deaths by suicide–although rare at this early developmental period–have been documented in children as young as 5 years of age.11 Although there has been some speculation that children with SI have a “less mature” concept of death,12 to our knowledge this question has not been systematically explored and for reasons outlined above has clinical relevance.
In addition to having a concept of oneself as a biological entity that can die, two death concepts appear particularly relevant to SI–permanence and knowledge that a range of plausible external and/or internal events can cause death. Critically, it is not necessary for children to grasp that death ultimately results from a breakdown of bodily functions to know that events such as choking oneself until breathing ceases will result in the permanent state of death. Indeed, we argue that the ability to detail penultimate events that can cause death is an important–and often overlooked–component of death understanding highly relevant to risk in childhood SI.
Studies that detail children’s understanding of events that represent penultimate causes of death find that younger children describe primarily external events (e.g., car accidents, getting shot) whereas older children include more internal events (e.g., illness, heart attack).3,13 Interestingly, violent themes such as being shot or stabbed feature prominently in Western children’s responses at all ages.7 Arguably, in most modernized societies, an increasing proportion of children’s exposure to violence comes via media, with new technologies allowing children to engage with a variety of forms of media with increasing frequency and at younger ages than ever before.14,15 Furthermore, the parallel increase between rates of suicidal behaviors and internet and videogame use in children raises questions about whether there are links between these factors. This issue has begun to be explored in adolescent populations,16 but has yet to be investigated in young children, particularly those with or at risk for mood disorders.
The goals of the current analysis are to (1) investigate death understanding in young children with depression with and without SI and age matched healthy controls, and (2) explore associations between media consumption (television, videogames, internet) and young children’s understanding of death as these factors relate to children’s violence attributions and SI. The present measures were added on to the baseline assessment of a clinical trial of a parent-child psychotherapy for preschool depression after higher than expected SI was observed in the sample, thus providing the unique opportunity to assess death understanding in depressed children with and without SI. We sought to investigate whether early childhood depression and/or SI was associated with developmental variation in the understanding of death. This developmental question is relevant to the meaning of expression of SI and therefore may inform clinical response in early childhood.
Method
Study Sample
The sample included baseline data from 79 children (24 girls) between the ages of 3.0 and 6.11 years prior to their randomization in a clinical trial (RCT) for preschool depression (N=239). Death understanding and media measures were added to the baseline assessment in Year 2 of the RCT, after higher than expected rates of SI were observed. For the RCT, children were recruited from primary care and day care sites in St Louis and screened with the Preschool Feelings Checklist17 to ascertain a group of children who met criteria for depression interested in participation in a dyadic psychotherapy. Those with PFC scores >3 and without major chronic medical illness, major neurologic disorder, and not currently receiving an antidepressant medication or psychotherapy were further screened for MDD using the Preschool Age Psychiatric Assessment (PAPA)18 depression module. Children suspected of an Autistic Spectrum Disorder (based on a diagnosis or screen positive on the Social Reciprocity Scale) were excluded. Children passing these screening criteria were then invited to participate in an in-person baseline assessment with their caregiver in the Early Emotional Development Program at the Washington University School of Medicine. Only children who subsequently met all criteria for MDD or MDD not otherwise specified on the KSADS-EC (see below) were included in our analysis.
A comparison group of 60 healthy children between the ages of 4.0 and 7.12 was also added and matched on mean age, gender, and socioeconomic indicators (3-year-olds were not included because ERP measures were also added and were not feasible for 3-year-olds). Caregivers completed the Child Behavior Checklist (CBCL)19 to assess for internalizing and externalizing behavioral problems in children. In order to participate as a healthy control in our study no T scores on internalizing/externalizing psychopathology were above 70. These children completed the death understanding measures; a caregiver completed the media measure. All study procedures were approved by the WUSM institutional review board and informed consent from caregivers and verbal assent from children were obtained.
Measures
Assessment of Psychopathology and Suicidal Ideation
A comprehensive age appropriate psychiatric interview that assessed for the presence of all relevant Axis I disorders, the Kiddie Schedule for Affective Disorders and Schizophrenia-Early Childhood (KSADS-EC),20 was administered to the parent/primary caregiver by a research clinician trained to reliability (kappas ranged from .74—1.0). This measure generated Axis I diagnoses as well as information about suicidal thoughts and behaviors. Specifically, the KSADS-EC-MDD module contains questions that assess parent report of child current and past SI. SI was defined by passive expression of thoughts of one’s own death such as “I wish I were dead” and/or active expression of thoughts or plans to end one’s life such as “I am going to kill myself”. Any suicidal actions were also included (e.g. trying to choke self). Children included in the SI group endorsed clinically significant threshold levels of at least one SI item described above over the past month.
Life Events
Caregivers were administered the Life Events Checklist (LEC)21 to assess children’s exposure to traumatic life events, including death events. The LEC was used in conjunction with the KSADS-EC to create a comprehensive and distinct measure of exposure to violent events for depressed children.
Death Interview
Children’s understanding of death was assessed using a modified version of the Death Interview,22 a validated experimenter-led behavioral measure that captures children’s understanding of five death concepts. Concepts consisted of universality (living things die), applicability (non-living things do not die), irreversibility (death is a permanent state), cessation (bodily functions cease with death), and causality (there are events that can cause death). The respective items were:
Can you tell me some things that die?
Can you tell me some things that never ever die?
Could a dead person at some time become a live person? If a person dies, and they haven’t been buried in their grave for very long, can they become a living person again?
When a person is dead do they need ….food? …air? …water? Can they move around? Do they have dreams?
Can you tell me something that might happen that would make someone die?
Reponses to items 1–4 were scored for accuracy from transcriptions of children’s verbal responses by two researchers blind to children’s SI-status (see Supplement 1 for scoring criteria). For items 1 and 2, the researchers categorized each response given by the child as either a person, animal, plant, electronic, or object; those categories were then used to determine whether children named only living, both living and non-living, or only non-living things for each question (electronics were excluded from these scores). For items 3 and 4, each response was scored independently; responses were then averaged to give each child a single score for each concept. Any discrepancies, which were rare due to the objective nature of the scoring, were resolved by the second author (DJW). Responses to item 5, causality, were coded into five categories–natural/biological (e.g., old age, illness), violent (e.g., shooting, stabbing), accidental/traumatic (e.g., car crashes, tornados), fantasy (e.g., monsters, potions), and nonsensical/no response–by two researchers blind to children’s SI-status (simple agreement reliability=97%; discrepancies resolved by a third blind coder). Children were considered to understand causality if their initial response was either natural/biologic, violent, or accidental/traumatic. This categorical coding also provided a means to investigate children’s attributions of death as having violent causes.
Death-Themed Narratives
To investigate young children’s emotional responses to hearing about natural death, accidental death, and suicide, their reactions while listening to and discussing four death-themed stories were recorded and subsequently coded from video by researchers blind to children’s SI-status. These four stories were about (1) an elderly grandparent who became sick and died in a hospital, (2) an elderly grandparent who became sick and decided to end her life, (3) a dog who got hit by a car and died, and (4) a boy who was unhappy and upset told his mother he wanted to die (see Supplement 2 for full stories). The stories were modified from Harris and Giménez’s death narratives for children.23 Scenes from the stories were depicted via play figurines in a picture book, which children viewed while being read each narrative. The targeted emotional responses of sadness (α=.82), irritability/frustration (α=.97), anxiety (α=.78), and interest (α=.73), were coded from 1(very low) to 5(high) based on children’s expression of each emotion within each narrative. The scaled codes used to assess emotional response were modified from Lindahl and Malik’s system to code family problem discussions,24 with the general negativity and conflict codes altered to account for behaviors and facial expressions associated with each target category. Children’s verbalizations (e.g., “this is sad” for sadness), overt behaviors (frowning, crying), and emotional tone (whining, sad voice) were equally weighted within these codes.
Children were presented with the Narratives after completing the Death Interview. Two steps were taken to assess and control for potential a priori differences in children’s emotional responses as a function of depression or SI-status. First, we acquired global affect codes (positive, neutral, negative) for all children during the 20–30 seconds prior to the start of the Death Interview. Second, we coded children’s emotional responses (sadness, irritability/frustration, anxiety, interest) during the Death Interview. Both measures were included as covariates in all Narrative analyses to ensure that any group differences detected in emotional responses could be attributed to the stories rather than more general differences in emotional expression between the groups.
Media Exposure
To explore whether children’s media exposure affects their early conceptions of death, we used items from The Media Quotient Questionnaire25 in which caregivers report the frequency of their child’s engagement with different types of media. Composite variables were created to capture the average number of hours/day that children spend watching television, playing computer or videogames or accessing the internet (videogames/internet), and their engagement with alternative activities such as reading books and drawing pictures.
Analyses
For the purposes of this investigation, we compared death understanding between three groups of children: depressed children with suicidal ideation (MDD+SI), depressed children without suicidal ideation (MDD-SI), and the non-depressed healthy comparison group (HC). The presence or absence of SI (and therefore depression subgroup status) was based on the KSADS-EC measure of SI over the past month. The three groups were compared to each other on all demographic factors (Table 1), including age, gender, family income-to-needs, and race/ethnicity, life events, media use, and all death measures.
Table 1.
Study Sample Demographic Characteristics and Media Use as a Function of Group
| MDD+SI (n=22) |
MDD–SI (n=57) |
HC (n=60) |
Statistic | p | |
|---|---|---|---|---|---|
| Demographics | |||||
| Gender (% male) | 86.36 | 63.16 | 61.67 | x(2)2=7.78 | .09 |
| Age in Years (N) | |||||
| 3 | 0 | 13 | 0 | ||
| 4 | 2 | 13 | 27 | ||
| 5 | 8 | 16 | 22 | ||
| 6 | 15 | 11 | |||
| Age (mean) | 5.86(.97) | 5.12(1.13) | 5.16(.80) | F(2)=5.42 | .01 |
| Income-to-needs ratio | 3.36(1.20) | 3.04(1.43) | 2.92(1.3) | F(2)=.841 | .43 |
| Race | |||||
| White | 15 | 50 | 48 | x(2)2=4.10 | .13 |
| Non-White | 7 | 7 | 12 | ||
| Life Events | |||||
| Traumatic | 4.55(3.93) | 2.02(2.00) | 2.16(3.22) | F(2)=3.46 | .03 |
| Death | 2.85(2.31) | 1.98(2.13) | 1.84(2.05) | F(2)=1.47 | .23 |
| Violent | .35(.67) | .22(.46) | – | F(1)=.86 | .36 |
| Media Use | |||||
| Television (hrs/day) |
1.81(1.20) | 2.07(1.52) | 1.78(1.23) | F(2)=.67 | .52 |
| Videogames/Internet (hrs/day) |
1.58(1.52) | 1.22(2.19) | 1.12(1.50) | F(2)=.49 | .61 |
| Alternatives (1=never 5=always) |
3.77(.40) | 3.90(.48) | 4.16(.49) | F(2)=7.20 | .00 |
Note: MDD+SI: depressed with suicidal ideation, MDD-SI: depressed without suicidal ideation, HC: healthy comparison. Means and standard deviations are presented for continuous variables.
Each component of the Death Interview was scaled from 0 to 1 such that a higher number indicates greater understanding. As the components included dichotomous (causality), ordinal (universality, applicability, irreversibility), and continuous (cessation) measures, this uniform scoring allows for direct comparisons between components. A composite score was created by averaging the components for each child. A one-way between-subjects Analysis of Variance (ANOVA) was conducted to test for differences between groups as a function of the death composite, with planned pairwise comparisons used to directly compare groups (two-tailed, α=.05). Age was included in all analyses to assess and/or account for expected increases in children’s understanding of death with age. Logistic, ordinal, and linear regressions were conducted for each type of respective death component to model the relationship between children’s understanding of that component and group. Finally, logistic regressions were performed to independently assess whether type of causality response (natural/biologic, violent, accidental/traumatic, fantasy) could be predicted by age or group. The primary goal of these latter analyses was to investigate factors contributing to children’s conceptualization of death as violent.
The Narratives were used to test for differences in children’s observed emotional reactions while listening to death-themed stories as a function of group. Repeated Measures ANOVA’s with story as the within-subjects factor and group as the between-subjects factor were conducted independently for each target emotion (sadness, irritability/frustration, anxiety, interest). Codes for global affect and each respective emotional expression from the Death Interview were used as covariates to control for differences in children’s a priori emotional state.
Media exposure measures were used to explore potential links between children’s understanding of death and type and amount of media they regularly consume. Logistic, ordinal, and linear regressions were conducted to determine whether media exposure (television, videogames/internet, alternative) predicts children’s understanding of each death measure. Logistic regressions were conducted to determine whether media exposure predicts the type of children’s causality responses. Parallel analyses were conducted to explore potential links between children’s understanding of death and exposure to traumatic, death, and violent events. The Benjamini-Hochberg procedure was used to control the false discovery rate within each of our exploratory analyses.
Results
Demographic Characteristics
Our final sample of children with depression consisted of 22 children with suicidal ideation (19 boys), and 57 without (36 boys). Children with SI were significantly older than children without SI. Within the MDD+SI group, 5 children exhibited active SI, 12 exhibited passive SI, and 5 exhibited both passive and active SI. One child had attempted suicide. Of note, all depressed children with a history of clinically significant levels of SI also met the current threshold for SI and were thus effectively captured in this group. Children with SI broadly experienced more traumatic life events, but not more death or violent events (Table 1). These children, and the 60 healthy controls (36 boys), all completed the Death Interview.
Death Interview
Children’s scores on the death composite differed among the three groups, F(2,131)=3.70, p=.027. Specifically, MDD+SI children (M=.79, SE=.04) showed a greater understanding of death than both MDD-SI (M=.66, SE=.03; p<.01) and healthy children (M=.68, SE=.03; p=.03). As expected, there was also a main effect of age, F(1,127)=35.99, p<.001 (Figure 1). Although MDD+SI children experienced more traumatic events than their peers, this variable was not significant when included in the model, F(1,123)=.01, p=.93, and was thus not included in subsequent group analyses (see Supplement 6S for exploratory analyses between death understanding and life events). Together, these findings indicate that older children demonstrated a greater understanding of death than younger children, and that MDD+SI children demonstrated a greater understanding of death than either peer group above the group differences in age and traumatic events.
Figure 1. Children’s Understanding of Death Concepts by Group and Age.
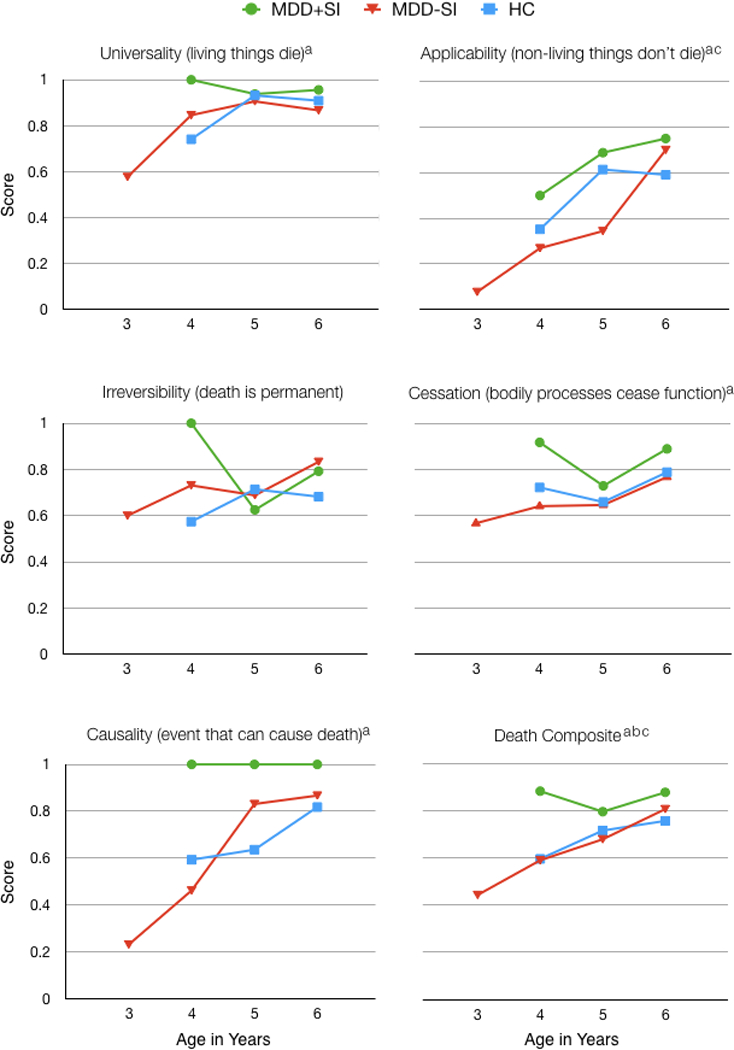
Note: All previously significant findings remain significant when 3-year-olds are removed from the analyses. Group comparisons were not performed for causality because MDD+SI did not vary on this measure. MDD+SI: depressed with suicidal ideation, MDD-SI: depressed without suicidal ideation, HC: healthy comparison.
a indicates significant findings for age
b indicates significant findings for MDD+SI vs HC
c indicates significant findings for MDD+SI vs MDD-SI
Regressions were performed for each death concept, with the concept as the DV and group and age as independent predictors. There were main effects of age for models that predicted universality, applicability, cessation, and causality, such that older children demonstrated greater understanding of these concepts than younger children (Table 2). There was no main effect of age for irreversibility. Group was only a significant predictor for applicability, with MDD+SI children demonstrating better understanding that non-living things do not die than MDD-SI children (B=−1.05, p=.05, ns after controlling for multiple comparisons) after accounting for age.
Table 2.
Children’s Understanding of Death Concepts and Causal Attributions of Death as a Function of Group
| B/Est | SE | t | p | OR | 95% CI | ||
|---|---|---|---|---|---|---|---|
| Concept | |||||||
| Universality | |||||||
| Age | .61 | .26 | .02b | .108–1.11 | |||
| HC vs. MDD+SI | −.45 | .86 | .60 | −2.12–1.23 | |||
| MDD-SI vs. MDD+SI | −.58 | .87 | .51 | −2.28–1.13 | |||
| Applicability | |||||||
| Age | .80 | .20 | .00ab | .397–1.20 | |||
| HC vs. MDD+SI | −.43 | .54 | .42 | −1.49–.62 | |||
| MDD-SI vs. MDD+SI | −1.05 | .54 | .05 | −2.12–.016 | |||
| Irreversibility | |||||||
| Age | .31 | .19 | .10 | −.055–.68 | |||
| HC vs. MDD+SI | −.16 | .51 | .76 | −1.15–.83 | |||
| MDD-SI vs. MDD+SI | .24 | .52 | .64 | −.78–1.26 | |||
| Cessation | |||||||
| Age | .07 | .03 | 2.38 | .02b | .01–.13 | ||
| Group | .02 | .04 | .46 | .64 | −.06–.10 | ||
| Causality | |||||||
| Age | .93 | .24 | .00ab | 2.49 | 1.54–4.02 | ||
| Causal Attribution | |||||||
| Natural/Biologic | |||||||
| Age | .11 | .32 | .73 | 1.12 | .60–2.09 | ||
| HC vs. MDD+SI | −.48 | .81 | .56 | .62 | .13–3.02 | ||
| MDD-SI vs. MDD+SI | −.42 | .81 | .60 | .66 | .14–3.19 | ||
| Violent | |||||||
| Age | −.63 | .22 | .00a | 1.91 | 1.25–2.92 | ||
| HC vs. MDD+SI | −.63 | .54 | .25 | .53 | .18–1.55 | ||
| MDD-SI vs. MDD+SI | −1.26 | .56 | .02b | .28 | .10–.85 | ||
| Accident/Trauma | |||||||
| Age | .16 | .22 | .45 | 1.18 | .77–1.79 | ||
| HC vs. MDD+SI | −.05 | .62 | .94 | .95 | .28–3.21 | ||
| MDD-SI vs. MDD+SI | .31 | .61 | .61 | 1.36 | .41–4.50 | ||
| Fantasy | |||||||
| Age | −.07 | .37 | .85 | .94 | .46–1.91 | ||
Note: MDD+SI: depressed with suicidal ideation, MDD-SI: depressed without suicidal ideation, HC: healthy comparison. All analyses covary for age. Logistic, ordinal, and linear regressions were performed; thus statistical outputs differ across respective measures. Group comparisons were not performed for causality or fantasy because MDD+SI children did not vary on these measures.
indicates findings that remain significant after adjustment for multiple comparisons
indicates significant findings based on a priori predictions
There was no variation in causality responses for MDD+SI children; thus group comparisons could not be performed. However, 100% of MDD+SI children named a cause of death compared to 61% of MDD-SI and 65% of healthy children. Further, both age and SI-status independently predicted children’s attribution of death to violent causes. Specifically, MDD+SI children were 3.57 times more likely to name a violent event when asked to describe an event that can cause death than MDD-SI children (95%CI [1.23–10.88], p=.02), and 1.76 times more likely to name a violent event than healthy children (95%CI [.58–5.32], p=.31). Neither age nor group predicted children’s responses in any other causality category (see Supplement 3S for means and estimates).
Death-Themed Narratives
The majority of children (84%) who completed the Death Interview also completed the Narratives (14 children did not complete the narratives due to refusal/fatigue; 15 children were excluded for missing data or experimenter error). Of the 117 children who completed the Narratives, the majority expressed neutral affect (N=95), relative to positive (N=15) or negative (N=7) affect prior to beginning the Death Interview. There were no significant baseline differences in global affect between MDD+SI, MDD-SI, and healthy children (x2[4, N=117]=8.31, p=.08). Similarly, there were no significant differences in emotional reactions as a function of group for sadness, irritability/frustration, anxiety, or interest (ps>.10) during the Death Interview. However, during the Narratives, there were main effects of group for sadness (F2,88=5.15, p<.01) and anxiety (F2,88=5.29, p<.01; Figure 2), although not for irritability/frustration or interest. Specifically, MDD+SI children displayed more sadness and more anxiety when listening to the Narratives than MDD-SI or healthy children. There were no main effects of story as a function of group, nor interactions between story and group. Thus, these findings suggest that, overall, listening to stories about death elicited these stronger negative emotional reactions in MDD+SI children relative to their peers.
Figure 2. Children’s Emotional Reactions to the Death-Themed Narratives as a Function of Group.
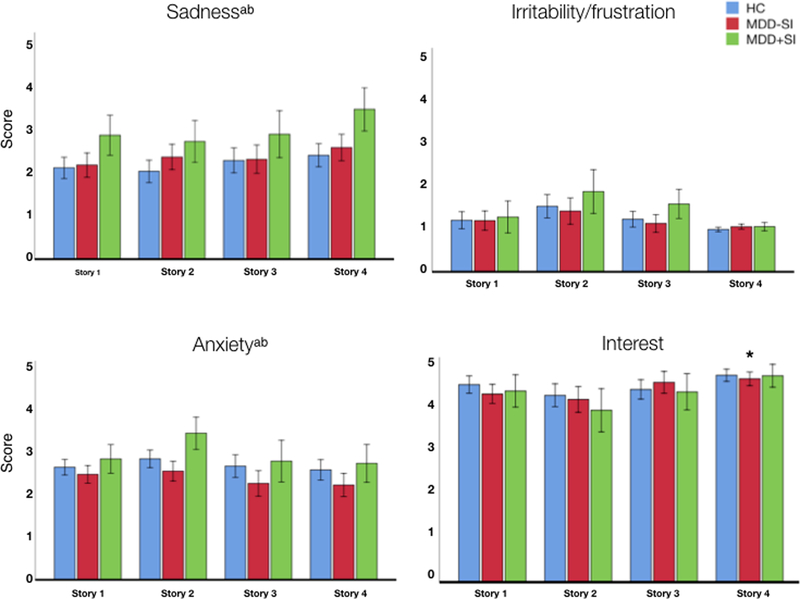
Note: MDD+SI: depressed with suicidal ideation, MDD-SI: depressed without suicidal ideation, HC: healthy comparison.
a indicates significant group differences between HC vs MDD+SI
b indicates significant group differences between MDD-SI vs MDD+SI
Although there was no main effect of interest as a function of SI-status, children’s interest scores were quite high across all four stories, suggesting children were engaged with the stories throughout the task. Further, there was a main effect of story on interest (F3,264=16.70, p<.001) such that children displayed more interest during Story 4 (upset boy with SI) relative to all other stories (ps<.001).
Media Exposure
Caregiver-reported media exposure measures were obtained for 92% of our sample. Across the three groups, children did not differ on amount of television or videogames/internet consumption. However, healthy children spent more time engaged in alternative activities such as reading books and drawing pictures than either depressed group. Across all children, watching more television predicted lower scores on the death composite (B=−.39, p<.001), in addition to the specific concepts of applicability (Est=−.28, p=.05), irreversibility (Est=−.36, p<.01), and cessation (B=−.20, p=.03; Supplement 4S). Applicability and cessation did not remain significant after controlling for multiple comparisons. Neither videogames/internet nor alternative activities predicted any death concept scores.
In addition to SI-status and age, further analyses revealed that, across children, spending more time engaged with videogames/internet uniquely predicted children’s naming a violent event as a cause of death (OR=1.29, p=.032, ns after controlling for multiple comparisons). In contrast, neither watching television nor engaging in alternative activities predicted children’s violence attributions or other causality responses (Supplement 5S).
Discussion
The goals of the current analysis were to investigate whether early childhood depression and/or SI was associated with alterations in death understanding, and to explore other key psychosocial correlates of death understanding. Study findings indicate that MDD+SI children have a more advanced understanding of death than MDD-SI and healthy children. This finding is of clinical interest as it suggests that SI in young children is associated with more advanced understanding of death, refuting a common assumption that such children were expressing regressive distress and were likely to have a less advanced understanding of death. This finding remains significant when age is accounted for, which is striking given the robust age-related increases in death understanding in the present sample of 3- to 6-year-old children. Specifically, across our sample, older children demonstrated an increased understanding of all death concepts except for irreversibility; findings that are largely consistent with previous research.26 Furthermore, although death understanding was more refined in older children, by age 4 the majority of children in the sample demonstrated at least some understanding that death occurs to living things, is permanent, and results in the cessation of bodily functions.
MDD+SI children were, on average, older than either peer group, and there were no 3-year-olds with SI in our sample. The sharp increase in SI at 5 and 6 years among our sample of 3–6-year-olds with depression offers some indication for a change in prevalence of SI across age at this early developmental stage. However, it is important to note that the two 4-year-old MDD+SI children in our sample demonstrated a robust understanding of the death components, including that death is permanent and describing a reasonable event that could cause death. This suggests that by the time children express SI they have at least a rudimentary coherent understanding of death. These findings also raise intriguing questions concerning whether the expression of SI is contingent upon understanding death.
When asked to describe something that could cause someone to die, all MDD+SI children, and roughly two thirds of MDD-SI and healthy children, successfully described a reasonable biological (10%), violent (38%), or accidental (23%) event that could result in death. Interestingly, both age and SI-status uniquely predicted children’s attribution of death to violent causes. That is, both older children, and MDD+SI children (57%), were more likely to describe death as being caused by violent events than their peers. Although children’s broad attributions of death as violent are consistent with previous research,7 the available data has not fully informed how these attributions develop. In the United States, accidents and illness are the leading causes of death across the lifespan,9 indicating a disconnect between children’s perceptions of death and the events that are most likely to cause death. The increase in violence attributions across early childhood may indicate an increasing normalization of violence in children’s perceptions of death. As many violent causes of death can be self-inflicted (e.g., strangulation, stabbing, gunshot) this topic is one of great importance when trying to understand how children with SI conceptualize death. These findings also raise important questions about what factors shape these violence attributions.
One possibility is that exposure to death via media plays a role in shaping children’s understanding of death. Indeed, across our sample, there is preliminary evidence that children who engaged more with videogames or internet (but not television or books) were more likely to depict death as violent. This association raises the possibility that violence encountered in interactive media leads children to more readily link death with violence than accidental or biological causes. Although media content was not assessed in the present analysis, there is ample evidence that death and violence are pervasive in these mediums.27 For example, videogames typically have death themes that follow clearly defined rules, such as protagonists given finite sets of lives, dying and retrying levels, and harming or killing other characters to advance in the game.28 In older children and adolescents there is a robust literature focused on elucidating contexts in which playing violent videogames desensitizes individuals to violence29 and leads to real-world aggression30. However, little is known about the content of videogames children play, how children spend their time online or how exposure to violence and death themes might affect emotional and behavioral development. Future investigation is thus needed determine the effects of such exposure on children’s perceptions of events that cause death, and also whether children with SI might engage more, or learn differently from, interactive and/or violent media than their peers.
Somewhat unexpectedly, we found that more engagement with television was associated with less understanding of death, including applicability, irreversibility, and cessation across our sample, although we did not find any differences as a function of depression or SI-status. One possible explanation is that children who watch more television are exposed to characters who defy biological principles–such as inanimate objects ‘dying’ and characters coming back to life or continuing to exist after bodily functions ceased. Although there is substantial evidence for a “video deficit” early in development–that is, infants and toddlers have more difficulty learning information from video compared to when that same information is presented live31–by age three children can learn new information solely from video.32 Thus, even the youngest children in the present analysis could have acquired their inaccuracies about death via television. Alternatively, spending more time watching television might deprive children of the experiences necessary to learn about death in the same manner or rate as peers who watch less television. As with violence attribution, future studies are needed to investigate potential causal relationships between events viewed on television and children’s understanding of death, and nuanced associations between learning about death via television and depression/SI not detected in this analysis.
When listening to death-themed stories, MDD+SI children exhibited more sad and anxious affect than their peers. These stronger negative emotional responses appear to reflect a greater sensitivity to death themes. These findings are consistent with the notion that young children who express SI are more emotionally activated by death themes, perhaps given their internal preoccupations with these themes.
Although the inclusion of 22 MDD+SI children in our sample is unprecedented, this is still a relatively small sample from which to draw broad conclusions about the nature of early SI. Specific limitations concern the inability to address differences between active from passive SI, or to detect potential interactions between SI-status and life events or media use. Another limitation concerns the lack of specificity of the media measure, including the conflation of videogame and internet use, and lack of data on content of the videogames played by children and how they spend their time online. Finally, we did not ask children about their understanding of suicide nor death as it pertains to themselves. These topics are fraught with practical, social, and ethical dilemmas. We hope that the present study will pave the way for future research to directly address these important questions about suicide and death in children with SI.
The current study informs the role of depression and suicidal ideation on young children’s understanding of death. The finding that young children with suicidal ideation have a more advanced understanding of death suggests that these ideations are not developmentally regressive with regard to concepts of death. While it remains unclear how to definitely assess risk in these circumstances and what these expressions mean, findings do suggest that these ideations should be taken seriously by clinicians and that detailed risk assessments should be done, including questioning about plans, access to weapons or potentially dangerous materials in children as young as age 4 who express suicidal ideation. From a public health perspective, the preliminary finding that increased consumption of videogames and internet in early childhood was associated with more violent attributions about death is potentially worrisome and raises important questions about causal relationships that should be further investigated in future studies. The finding that that SI was associated with even greater attributions of death to violent events is also a related public health issue for which causality should be investigated. Overall, these findings which are the first to our knowledge to inform the understanding of death in early childhood depression and suicidality, point to the need for clinicians to address suicidal thoughts and behaviors in young children with depression in clinical interviews and to take these phenomena seriously, putting in place appropriate safety precautions and addressing more adaptive coping mechanisms.
Supplementary Material
Acknowledgements
The authors thank the children and caregivers who participated in this study. The authors also thank Paul L. Harris, PhD, Harvard University, for his guidance on this project.
Sources of Grant Support
This study was supported by the National Institutes of Health grant R01 MH098454. Dr. Hennefield’s work was supported by NIH training grants T32 MH100019 and F32 HD093273.
Footnotes
Conflicts of Interest / Financial Disclosures
Dr. Hennefield, Dr. Whalen, Grace Wood, and Mary Chavarria declare no conflicts of interest. Dr. Luby has received royalties from Guilford Press.
References
- 1.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5 Washington, DC;2013:1–970. [Google Scholar]
- 2.Luby JL, Belden AC, Pautsch J, Si X, Spitznagel E. The clinical significance of preschool depression: Impairment in functioning and clinical markers of the disorder. J Affect Disord 2009;112(1–1):111–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Slaughter V Young children’s understanding of death. Aust Psychol 2005;40(3):179–186. [Google Scholar]
- 4.Jay SM, Green V, Johnson S, Caldwell S, Nitschke R. Differences in death concepts between children with cancer and physically healthy children. J Clin Child Psychol 1987;16(4):301–306. [Google Scholar]
- 5.Reilly TP, Hasazi JE, Bond LA. Children’s conceptions of death and personal mortality. J Pediatr Psychol 1983;8(1):21–31. [DOI] [PubMed] [Google Scholar]
- 6.O’Halloran CM, Altmaier EM. Awareness of death among children: Does a life-threatening illness alter the process of discovery? J Couns Dev 1996;74(3):259–262. [Google Scholar]
- 7.Panagiotaki G, Nobes G, Ashraf A, Aubby H. British and Pakistani children’s understanding of death: Cultural and developmental influences. Br. J. Dev. Psychol 2014;33(1):31–44. [DOI] [PubMed] [Google Scholar]
- 8.Whalen DJ, Dixon-Gordon K, Belden AC, Barch D, Luby JL. Correlates and consequences of suicidal cognitions and behaviors in children ages 3 to 7 years. J Am Acad Child Adolesc Psychiatry 2015;54(11):926–937.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.National Center for Health Statistics. National Vital Statistics Reports 2016;65(4)1–122 [Google Scholar]
- 10.QuickStats: Death Rates for Motor Vehicle Traffic Injury, Suicide. 06/2018:1–3. [Google Scholar]
- 11.Sheftall AH, Asti L, Horowitz LM, et al. Suicide in elementary school-aged children and early adolescents. Pediatrics 2016;138(4):e20160436–e20160436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cuddy-Casey M, Orvaschel H. Children’s understanding of death in relation to child suicidality and homicidality. Clin Psychol Review 1997;17(1):33–45 [DOI] [PubMed] [Google Scholar]
- 13.Kenyon BL. Current research in children’s conceptions of death: A critical review. Omega (Westport) 2001;43(1):63–91. [Google Scholar]
- 14.Anderson CA, Bushman BJ, Donnerstein E, Hummer TA, Warburton W. SPSSI research summary on media violence. Anal. Soc. Issues Public Policy 2015;15(1):4–19. [Google Scholar]
- 15.American families see tablet as playmate, teacher, and babysitter. http://www.nielsen.com/us/en/insights/news/2012/american-families-see-tablets-as-playmate-teacher-and-babysitter.html. 02/16/12. Accessed 03/01/18.
- 16.Twenge JM, Joiner TE, Rogers ML, Martin GN. Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clin Psychol Sci 2017;6(1):3–17. 10.1177/2167702617723376 [DOI] [Google Scholar]
- 17.Luby JL, Heffelfinger A, Koenig-McNaught AL, Brown K, Spitznagel E. The Preschool Feelings Checklist: A brief and sensitive screening measure for depression in young children. J Am Acad Child Adolesc Psychiatry 2004;43(6):708–717. [DOI] [PubMed] [Google Scholar]
- 18.Egger HL, ascher B, Angold A. The Preschool Age Psychiatric Assessment: Version 1.4. 2003:1–31.
- 19.Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms & Profiles : an Integrated System of Multi-Informant Assessment ; Child Behavior Checklist for Ages 1 1/2–5 ; Language Development Survey ; Caregiver - Teacher Report Form Burlington, Vt.: Univ. of Vermont, Research Center for Children, Youth & Families; 2000. [Google Scholar]
- 20.Gaffrey MS, Luby JL. Kiddie Schedule for Affective Disorders and Schizophrenia—Early Childhood Version (K-SADS-EC) St Louis, MO;2012. [Google Scholar]
- 21.Luby JL. Life Events Checklist-Child (LEC-Child) St Louis, MO;2013. [Google Scholar]
- 22.Slaughter V, Griffiths M. Death understanding and fear of death in young children. Clin Child Psychol Psychiatry 2007;12(4):525–535. [DOI] [PubMed] [Google Scholar]
- 23.Harris PL, Giménez M. Children’s acceptance of conflicting testimony: The case of death. J Cogn and Cult 2005;5(1–2):143–164. [Google Scholar]
- 24.Lindahl K, Malik N. The System for Coding Interactions and Family Functioning In: Kerig P, Lindhal K, eds. Family Observational Coding Systems Resources for Systemic Research Mahwah, NJ;2001:77–91 [Google Scholar]
- 25.Gentile DA, Walsh DA. MediaQuotientTM: National Survey of Family Media Habits, Knowledge, and Attitudes. Minneapolis, MN;1999:1–104. [Google Scholar]
- 26.Hunter SB, Smith DE. Predictors of children’s understandings of death: Age, cognitive ability, death experience and maternal communicative competence. Omega 2008;57(2):143–162. [DOI] [PubMed] [Google Scholar]
- 27.Council on Communications and Media. Media Violence. Pediatrics 2009;124(5):1495–1503. [DOI] [PubMed] [Google Scholar]
- 28.Tocci J “You Are Dead. Continue?”: Conflicts and complements in game rules and fiction. Eludamos 2008;2(2):1–17. [Google Scholar]
- 29.Carnagey NL, Anderson CA, Bushman BJ. The effect of video game violence on physiological desensitization to real-life violence. J Exp Soc Psychol 2007;43(3):489–496. [Google Scholar]
- 30.Calvert SL, Appelbaum M, Dodge KA, et al. The American Psychological Association Task Force assessment of violent video games: Science in the service of public interest. Am Psychol 2017;72(2):126–143. [DOI] [PubMed] [Google Scholar]
- 31.Troseth GL, DeLoache JS. The medium can obscure the message: Young children’s understanding of video. Child Dev 1998;69(4):950–965. [PubMed] [Google Scholar]
- 32.Richert RA, Robb MB, Smith EI. Media as social partners: The social nature of young children’s learning from screen media. Child Dev 2011;82(1):82–95. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.