

Abstract
Working conditions of residential roofers expose them to a unique sloped environment. The purpose of this study is to determine in what way traversing across a sloped/roof surface alters lower extremity kinematics of the upslope and downslope legs compared to level walking. College aged males negotiated across a pitched (26 degrees) roof segment during which lower extremity three-dimensional kinematics were calculated. One foot was higher on the slope and one was lower for the duration of cross slope walking. Overall, cross-slope walking on a 26 degree roof significantly altered 77% of the measured lower extremity variables compared to level self-selected pace walking. The data suggest that roof pitch incite significant differences in crossslope walking of the kinematics in the lower extremity between the upslope and down slope limbs when compared to level surface walking. These alterations could temporarily alter proprioception which may in turn lead to increased falls and musculoskeletal injury, though further study is needed.
Keywords: Kinematics, Lower Extremity, Roof, Cross-Slope
1. Introduction
Since 2011, 173 per 10,000 workers in the construction industry experienced non-fatal falls to a lower level (BLS, 2016a). Additionally, most fatal falls (81%) were falls to a lower level, and 40% of those fatal falls were from 15 feet or less. In the private construction industry, falls from height to a lower level were responsible for almost 40% of all deaths (BLS, 2016a). In addition to falls, roofers have the second highest incident rate of work—related musculoskeletal disorders (MSDs) in all construction sectors (BLS, 2013). Most of these MSDs are in the lower back and lower extremity (Holmström and Engholm, 2003). When roofers are burdened with MSDs they face work limitation, missed work, and/or reduced physical functioning, leading to premature departure from the workforce (Welch et al., 2008, 2009). Due to the fact roofers have such high injury risk and it has been shown that changes in lower extremity kinematics, posture and gait variability have all been linked to increased risk for falling (Perry and Burnfield, 2010), the association of cross-slope walking and its influence on gait merits further study.
Additionally, the demand for roofers is increasing, in 2015 there were roughly 140,000 roofers and in 2016 there were 146,000 (BLS, 2015, 2016b). The BLS also estimates that between 2016 and 2026 the job growth is at 11% suggesting that by 2026 there could be over 162,000 roofers (BLS, 2016a). Furthermore, over 90% of roofers work on residential projects, which usually have steeper roof surfaces which range as low as 10°, but can be as steep as 45° (BLS, 2015). According to Liberty Mutual 2018 Workplace Safety Index, direct costs for: repetitive motion injuries was $1.5 billion; falls on the same level was $11.2 billion; and falls from to a lower level was $5.9 billion. Together, these three classifications of occupation injuries accounted for 31.8% of all workplace injuries in 2018 (Mutual, 2018). As a result, the cost of injury and illness for roofers is extremely high (Leigh et al., 2004; Welch et al., 2010). For example, the insurance rates for roof work are nearly three times as high as the average rate of all construction trades in the Washington State (Industries, 2015) and more than three times of the average rate of all trades in the Ohio State (Compensation, 2015).
As it has been shown that individuals are less stable directly after working on a roof (Wade and Davis, 2009; Wade et al., 2014), and sloped working surfaces lead to an increased risk of slipping (OHSA, 2017) which, if on a roof, could lead to a fatal fall from height (BLS, 2016a; b). Furthermore, cross-slope walking induces an asymmetric gait, which might lead to increased risks for MSDs and falling; however much of the asymmetric gait research is focused on asymmetries caused by clinical disorders and aging (Hesse et al., 1997; LaRoche et al., 2012; Yogev et al., 2007). Thus with the immense costs associated with MSD and falling injuries and the increase in roofer employment opportunities in the future, it is important to determine if walking on a sloped surface alters gait characteristics in such a way to increase fall and MSD risk to the workers immediately upon getting on a pitched/sloped residential roof.
Sloped or inclined walking – defined as walking directly up or down a sloped surface (i.e. toward the roof ridge or eave)—has been studied in the laboratory in the past. With slopes as little as ± 10°, there is an increase in hip and knee flexion as well as ankle dorsiflexion (McIntosh et al., 2006; Redfern and DiPasquale, 1997). Upslope walking induced kinematic postural changes that were needed for toe clearance at heel strike, and in addition, to regulate the body during downslope walking (Lay et al., 2006). Ankle, knee, and hip joint kinematics compensated for the gradient at push off and during swing (Kuster et al., 1995). While increasing the slope did decrease the step length and gait period during downslope walking, this did not alter gait speed (Leroux et al., 2002; Redfern and DiPasquale, 1997). Peak foot-floor angles during touchdown in the sagittal plane were smaller during uphill walking compared to level but larger in downhill walking in the frontal plane on a 19-degree laboratory sloped surface (Wannop et al., 2014). Toe-off foot-floor angles were smaller compared to level walking in the sagittal and transverse planes, but small than level walking in the frontal plane on a 19-degree laboratory sloped surface (Wannop et al., 2014).
When upslope walking was performed on a treadmill (up to 10% grade), an increased flexed posture of the hip, knee, and ankle at initial foot contact was observed. A downslope treadmill grade of 10% decreased flexion of the hip at initial foot contact as well as increased knee flexion during weight acceptance and late stance (Leroux et al., 2002). Toe clearance in young, healthy adults was significantly different between a positive 3% grade and negative 3% grade treadmill walking, but there was not a change from level to the graded walking (Khandoker et al., 2010).
Cross-slope gait, defined as walking along the slope with one foot higher on the slope and one foot lower on the slope (i.e. toward the roof hip), has been far less studied. Cross-slope gait evaluations have been made in low angle conditions ~ 6° in a clinical setting (Dixon and Pearsall, 2010) or railroad ballast in an occupational setting (Andres et al., 2005). Both conditions found significant changes from level conditions including ground reaction forces, joint moments, and sagittal kinematics (Dixon and Pearsall, 2010) as well as frontal kinematics (Andres et al., 2005). Wannop et al. (2014) studied cross-slope gait on a 19-degree slope and determined the foot-floor angles in the downhill foot do not change compared to level, but the uphill foot changed in all three planes. The sagittal plane angles decreased compared to level while the transverse and frontal plane angles increased (Wannop et al., 2014). While walking cross-slope—on a 19-degree surface—the foot-floor angles during toe-off in the downhill foot increased in the sagittal and transverse planes and increased in the frontal compared to level. In the uphill leg, only the transverse plane foot-floor toe-off angles increased compared to level walking (Wannop et al., 2014). Damavandi et al. (2010) investigated the effect on multi-segmented foot kinematics during 10° cross slope walking. Only the frontal plane kinematics were significantly changed from level to cross slope walking in a multi-segmented foot (Damavandi et al., 2010). While these findings are interesting, they do not come close to replicating the steep surfaces encountered by roofers. Although there is not a standard roof pitch—and pitch usually is dependent on geographical location—many modern roofs can have slopes greater than 30° (Myroof.com, 2017; Systems, 2017).
The current study reports on the extent which lower extremity kinematics are altered when individuals are first introduced and traverse across a sloped surface. The purpose of this study is to determine in what way traversing across a sloped/roof surface alters lower extremity kinematics of the upslope and downslope legs compared to level walking. It is hypothesized the introduction of a sloped surface will induce a substantial change in lower extremity kinematics when compared to level walking in healthy young male subjects.
2. Methods
Eleven college-aged male subjects (19.1 ± 1.49yrs, 81.15 ± 15.14 kg, and 180.73 ± 5.89 cm) who were considered inexperienced walking on sloped surfaces participated in the study. Subjects did not report any history or clinical evidence of neurological, musculoskeletal or other medical conditions affecting gait performance, such as stroke, head trauma, neurological disease (i.e., Parkinson’s, diabetic neuropathy), or visual impairment uncorrectable by lenses and dementia. All subjects reviewed and signed University of Mississippi Institutional Review Board approved informed subject consent forms.
Subjects completed two separate testing sessions on different days, at least a week apart: level surface and sloped surface walking in the biomechanics laboratory at the University of Mississippi. The first session was a level surface and the second session was the sloped surface. Due to the complexity and time requirements to install the sloped surface, the testing sessions were not randomized. The level condition consisted of a level ten-meter vinyl covered walk-way. The sloped condition contained a 2.43 m wide x 7.32m long section of 15.24cm/ 30.48 cm pitch (26°) shingled sloped surface—which was designed to simulate a walkable residential roof surface—was attached to the laboratory floor (Fig. 1). A residential roof is considered walkable until a pitch of 20.32cm/30.48 cm (33°); therefore the 26° angle was chosen as a steeper walkable roof, but not to induce any greater risk than normal activities (Roofkey.com, 2017).
Fig. 1.

A) Frontal view of subject on roof segment. B) Sagittal view of 15.24cm/ 30.48 cm pitch roof segment.
Subjects wore spandex clothes and 15.24 cm high work boots for both testing conditions. The subjects were outfitted with thirty-nine 14 mm reflective markers according to the Plug-in-Gait marker set (Vicon Inc. Oxford, UK) and completed both conditions at a comfortable self-selected walking pace. The level condition required the subjects to walk across the ten meter walkway; while the sloped condition asked the subjects to traverse the sloped roof section. By traversing the roof section, one foot was higher on the slope (upslope) and one foot was lower on the slope (downslope), Fig. 1.
Ten trials from each condition were recorded using a Vicon 612 system at 120 Hz. Subjects were allowed no acclamation time on the sloped surface, and kinematic data were collected immediately after the subjects stepped onto the roof surface. This was done to capture the kinematic change what occurs when individuals are first introduced to a sloped surface, akin to the situation when an individual first ascends a roof. Marker trajectories—referenced to the same global coordinate system for both conditions—were filtered with a Woltering filter and three-dimensional lower extremity kinematics (ankle, knee & hip) were calculated using the Plug-in-Gait pipeline in the Nexus software (Vicon Inc. Oxford, UK). After the ten trials, one gait cycle from each leg was collected. A gait cycle is defined by ipsilateral heel strikes and were determined in this study with two methods. The initial heel strike (HS) was determined with the use of a force plate (FP) when the vertical ground reaction force (GRFv) was equal to 10% of the subject’s weight. A Coordinate-Based Algorithm proposed by (Zeni Jr et al., 2008) was used to define the subsequent ipsilateral HS. An ensemble average of the ten trials would then represent one subject. Outcome measures for this study were the three-dimensional (sagittal, frontal, and transverse) peak lower extremity angles (ankle, knee, and hip), from both conditions (level and sloped), and were compared using paired a repeated measures ANOVA. Level condition peak angles were separated and matched to the corresponding upslope or downslope leg. For example, if the left leg was downslope, the left level leg peak angles would be compared to the left downslope leg peak angles. Data analysis was completed using SPSS v22 and p-values were set to 0.05.
3. Results
As hypothesized, the introduction of a sloped surface considerably altered lower extremity kinematics compared to level surface walking. Of the 26 outcome variables analyzed in the current study, 20—or approximately 77%— of these variables were significantly changed with the introduction of the sloped surface. The results comparing cross-slope (upslope and downslope) walking with level walking are summarized in Tables 1–3 and Figs. 2–5.
Table 1.
Descriptive sagittal plane quantitative statistics and results of hypothesis tests of differences between level and sloped differences in the downslope and upslope legs.
| Peak Joint Angle (deg) | DownSlope | UpSlope | ||||||
|---|---|---|---|---|---|---|---|---|
| Sagittal | Level | Sloped | Mean Difference | p-value | Level | Sloped | Mean Difference | p-value |
| Ankle Plantarflexion | 18.85 ± 12.29 | 13.95 ± 13.55 | 4.90 | 0.02 | 15.09 ± 7.98 | 18.25 ± 8.12 | −3.16 | < 0.001 |
| Ankle Dorsiflexion | 22.06 ± 9.98 | 28.08 ± 7.17 | −6.02 | < 0.001 | 24.54 ± 4.16 | 21.16 ± 5.44 | 3.38 | < 0.001 |
| Knee Flexion | 50.37 ± 9.73 | 63.57 ± 9.21 | −13.20 | < 0.001 | 48.3 ± 7.99 | 37.15 ± 18.84 | 11.15 | < 0.001 |
| Hip Flexion | 17.52 ± 7.58 | 22.6 ± 5.49 | −5.08 | < 0.001 | 15.77 ± 6.25 | 11.14 ± 5.03 | 4.63 | < 0.001 |
| Hip Extension | 22.85 ± 5.45 | 22.03 ± 4.89 | 0.82 | 0.28 | 22.19 ± 4.22 | 24.5 ± 5.11 | −2.31 | < 0.001 |
Table 3.
Descriptive transverse plane quantitative statistics and results of hypothesis tests of differences between level and sloped differences in the downslope and upslope legs.
| Peak Joint Angle (deg) | DownSlope | UpSlope | ||||||
|---|---|---|---|---|---|---|---|---|
| Transverse | Level | Sloped | Mean Difference | p-value | Level | Sloped | Mean Difference | p-value |
| Ankle External Rotation | 21.22 ± 26.27 | 12.12 ± 38.32 | 9.10 | 0.06 | 20.95 ± 41.84 | 0.09 ± 62.57 | 20.86 | 0.01 |
| Knee Internal Rotation | 13.04 ± 30.99 | 14.69 ± 32.77 | −1.65 | 0.72 | 2.25 ± 11.97 | 15.49 ± 69.62 | −13.24 | 0.01 |
| Knee External Rotation | 28.85 ± 15.65 | 32.98 ± 16.98 | −4.13 | 0.72 | 24.81 ± 10.85 | 14.47 ± 47.08 | 10.34 | 0.03 |
| Hip External Rotation | 55.95 ± 9.51 | 52.1 ± 9.31 | 3.85 | < 0.001 | 56.38 ± 8.95 | 59.43 ± 6.88 | −3.05 | < 0.001 |
Fig. 2.

Lower extremity kinematic comparing level walking with slope walking. Grey line and band represent mean ± 1 standard deviation of level walking. Black line and band represent mean ± 1 standard deviation of cross slope walking.
Fig. 5.

Peak transverse kinematic angles equating level and sloped walking. Error bar represent ± 1 standard deviation and * signifies a significant change in kinematics between conditions at p ≤ 0.05.
3.1. Sagittal plane
3.1.1. Downslope leg
All but one (hip extension) of the downslope leg sagittal, lower extremity peak, angles significantly changed as a result of traversing the sloped roof segment. There was no set pattern of the change in kinematics— for example ankle plantarflexion was significantly larger in the flat condition (18.85° ± 12.29°) than the sloped condition (13.95° ± 13.55°), while flat ankle dorsiflexion (22.06° ± 9.98°), knee flexion (50.38° ± 9.73°), and hip flexion (17.52° ± 7.58°) were significantly smaller than the sloped condition (28.08° ± 7.18°, 63.57° ± 9.22°, and 22.61° ± 5.49°).
3.1.2. Upslope leg
All of the upslope leg sagittal, lower extremity peak angles significantly (p > 0.001) changed as a result of traversing the sloped roof segment. Completely opposite to the downslope leg, the ankle plantarflexion (15.09° ± 7.99°) and hip extension (22.20° ± 4.22°) were significantly smaller in the flat condition than the sloped condition (18.25° ± 8.13° & 24.50° ± 5.12°), while flat ankle dorsiflexion (24.54° ± 4.16°), knee flexion (48.31° ± 7.99°), and hip flexion (15.78° ± 6.26°) were significantly smaller, then the sloped condition (21.16° ± 5.45°, 37.15° ± 18.85°, and 11.14° ± 5.03°).
3.2. Frontal plane
3.2.1. Downslope leg
All of the included downslope leg frontal lower extremity peak angles significantly changed as a result of traversing the sloped roof segment. Flat condition ankle inversion (13.10° ± 15.99°), knee abduction (35.72° ± 11.23°) and hip abduction (8.39° ± 3.37°) were significantly smaller than the sloped condition (4.23° ± 31.77°, 31.80° ± 13.37° & 4.89° ± 3.02°). Hip adduction (3.54° ± 2.52°) was significantly smaller, then the sloped condition (5.95° ± 2.81°).
3.2.2. Upslope leg
The hip upslope leg lower extremity kinematics were significantly influenced between level and sloped conditions. Level condition hip abduction (7.25° ± 4.22°) was significantly smaller than sloped condition hip abduction (8.40° ± 4.55°), p = 0.02. Hip adduction was significantly larger in the level condition (4.03° ± 4.13°) compared to the sloped condition (1.15° ± 4.17°).
3.3. Transverse
3.3.1. Downslope leg
Only downslope leg hip external rotation was significantly affected by the sloped condition. Level condition average was larger than (55.95° ± 9.51°) the sloped condition (52.10° ± 9.31°). It is important to note that ankle external rotation was trending to a significant change based on the sloped condition, p = 0.06.
3.3.2. Upslope leg
Upslope leg ankle external rotation was significantly larger during the level (20.95° ± 41.84) condition compared to the sloped (0.10° ± 62.57°) condition. Knee internal rotation was significantly smaller in the level (2.26° ± 11.98°) condition compared the sloped (15.49° ± 69.62°) condition. Knee external rotation was significantly larger in the level (24.82° ± 10.86°) condition compared to the sloped (14.47° ± 47.08°) condition. The level condition (56.38° ± 8.95°) was significantly smaller than sloped (59.43° ± 6.89°) condition for the hip external rotation.
4. Discussion
In this study, we determined and documented the extent by which cross-slope walking alters the three-dimensional lower extremity kinematics of the upslope and downslope legs compared to level walking. Overall, cross-slope walking on a 26° roof significantly altered 77% of the measured lower extremity variables compared to level self-selected pace walking. This study was the first to quantify the kinematic changes induced by steep walkable roof cross-slope walking which is commonly encountered by residential roofers.
Cross-slope walking produced significant changes in plantar- and dorsiflexion in both up- and downslope legs. The decreased plantarflexion during cross-slope walking in the downslope leg is suggestive of—given nature of the slope—the downslope foot is in contact with the surface less time than in level walking and therefore less plantarflexion is needed to clear the toe during swing. The opposite is true in the upslope leg where increased push-off is required to initiate swing phase (Houglum and Bertoti, 2011; Perry and Davids, 1992). Dorsiflexion decreased in the downslope leg while increasing in the upslope leg compared to level walking. Our dorsiflexion findings agreed with Dixon and Pearsall (2010) suggesting the sustained change in functional leg length—during cross-slope walking—throughout stance decreases the upslope dorsiflexion (decease in functional leg length) and increases the dorsiflexion in the downslope leg with the need to increase the functional leg length (Dixon and Pearsall, 2010).
Knee flexion was significantly changed in the sloped condition compared to the level in both up- and downslope legs; this differed from previous cross-slope reports—in that only the upslope leg significantly changed (Dixon and Pearsall, 2010). The 20° slope difference between these studies has a marked effect in the lower extremity kinematics. The increase in knee flexion in the current study during swing in the downslope leg is likely compensating for the increased dorsiflexion observed at the ankle. Furthermore, the increased knee flexion—coupled with the increased hip flexion—will allow for proper positioning of the foot for the subsequent heel-strike, similar to stepping down from a height. The decrease in knee flexion in the upslope leg is present due to observations that subjects adopt a limp style gait with the upslope leg. Therefore, leg swing is much quicker than in level gait meaning the knee does not have time to flex as much during the swing phase, which is also supported by the decrease in hip flexion in the upslope leg.
Hip flexion was significantly greater in the downslope leg and significantly less in the upslope leg compared to level walking. The steep roof condition used in the present study introduced changes in the lower extremity kinematics not reported in hip flexion during 6° cross-slope walking in the up- and downslope legs (Dixon and Pearsall, 2010). The increased hip flexion in the downslope leg is likely due to the slope allowing more swing to occur before heel-strike; while the contrary is true during the upslope leg where the decrease in hip flexion is due to the early heel-strike required by the slope. Cross-slope walking significantly increased hip extension in the upslope leg which is needed to compensate for the reduced knee flexion and aid in propelling the body forward.
In the current study, ankle inversion was significantly smaller in sloped condition than the flat condition in the downslope leg, which differs from previously reported data (Dixon and Pearsall, 2010). Ankle eversion did not change as a result of the slope in the upslope leg. It is unclear why the ankle inversion decreased in the sloped condition; however, one possible explanation is the footwear of the subjects. No specific instructions were given on how to tie the boots, the subjects might have tied the boots tighter in the sloped condition in an effort to provide more support. Knee abduction was larger in the flat condition in the downslope leg. This could possibly be due to an increased knee adductor muscle activity while traversing a sloped surface. The necessity for the more active adductor muscles could have multiple causes, such as helping position the shank for heel strike and to act as a preventive measure due to increased shear forces caused by the slope surfaces as seen in the medial-lateral ground reaction forces (Dixon and Pearsall, 2010).
During swing phase, hip abduction is decreased in the sloped downslope leg and increased in the sloped upslope leg when compared to level walking. Because frontal plane hip motions are concomitant with pelvis motion, the decreased downslope abduction is consistent with the gluteus medius not having the proper force to maintain the pelvis in the same orientation as level gait. In the upslope leg, the momentum of the swinging leg and the body trying to maintain the center of mass within the base of support will cause the increase in hip abduction.
Normal ankle rotation motion is not well defined, and there are ongoing investigations (Houglum and Bertoti, 2011). In the current study, both upslope and downslope legs displayed a decrease in external rotation between level and sloped conditions. The foot would want to create a leading edge with the boot parallel (i.e. toward the roof hip or gable) to the slope thereby reducing the chances of slipping.
Upslope leg knee internal rotation increased, and the downslope leg decreased compared to level walking. The increased internal rotation is required during swing phase to assist the swing leg to position for the heel strike. The increased internal rotation is expected with the decreased external rotation from level to slope.
Hip external rotation decreased in the downslope leg from level. This occurs to position the foot in a parallel manner to the roof fascia in order to promote center of mass (COM) movement that is along the line of progression and not downhill. The increased external hip rotation in the upslope leg is positing the foot toward the ridge of the roof to again help the COM stay in progression of the movement as well as ensure that the plantar surface of the foot will fully contact the roof. This is difficult on a slope without the increased external hip rotation in the upslope foot.
A limitation of the current study was all subjects walked the same direction on the slope. Therefore, the right leg was always the upslope leg. Furthermore, it was not determined which leg was the subjects’ dominant leg. Future studies could compare how dominant vs nondominant legs respond as upslope compared to the downslope leg. Another limitation might have been the high boots the participants wore. Given the variability in the outcome measures of this study, some of the variables statistical power might be considered low, however, the statistical power does not diminish the clinical relevance. The high boots, though more common in a work environment – as we tried to mimic a work situation - covered the malleoli which could reduce the accuracy of the lower extremity ankle kinematics, particularly in the transverse plane. Finally, the roofer segment was located on the ground, rather than at an elevation typical of a roof. This change might have negated any possible psychological effects associated with the height which could have influenced the kinematics.
Many of the lower extremity kinematic changes observed in the current study can be related to pathologies (Houglum and Bertoti, 2011; Perry and Davids, 1992) and aging (Kawashima et al., 2004; Kerrigan et al., 2001; Luepongsak et al., 2002; Masani et al., 2007; Province et al., 1995; Romero et al., 2003; Winter 1991) which have increased risks in falling. More importantly, the extreme position induced by cross-slope walking might affect proprioceptors which could lead to in an increase in MSD’s and falling due to the decreased stability (Wade and Davis, 2009; Wade et al., 2014) cross-slope walking imposes in the lower extremity kinematics. For example, the asymmetric nature of cross-slope walking might lead to a greater occurrence of knee compartment involvement leading to osteoarthritis (OA) or unequal distribution in bone mineral density in the lower extremity. Due to the fact that the contact pressure will be moved either medial or lateral—depending if upslope or downslope leg—induced from consistent roof walking, as was similarly found in obese individuals (Wearing et al., 2006). Furthermore, a cross-slope walking condition—which introduces leg-length incongruity—may aggravate MSD risks such as hip pain, lower-back pain, arthritis of the spine, and stress fractures (Gurney, 2002). The asymmetric nature of cross-slope walking might also increase fall risk due to the feet at different elevations. This difference will cause larger upper body motion compared to level walking which has been shown to be related to increased fall risk (Lee and Chou, 2006, 2007; Mandeville et al., 2007).
5. Conclusions
This study established that walking cross-slope on a steep surface, such as a roof, has a profound influence on the three-dimensional lower extremity kinematics. There was not a set pattern to the changes in the lower extremity kinematics—for example, the downslope plantarflexion angle decreased compared to level while the upslope foot increased compared to level. A major challenge to cross-slope gait is the demand of two different functional leg lengths. One side will have to make kinematic changes that might be completely different to the contralateral side to allow gait leading to environmentally induced leg length discrepancy.
It is apparent that cross-slope walking presents many challenges to gait. These changes could lead to increased musculoskeletal disorders in roofers and place them in an increased risk for falling however further research is required to confirm these speculations. Based on the current study’s findings, educational and training procedures—to provide workers with the information and expertise needed to work safely in a sloped environment—are paramount to ensure individuals working on a sloped surface avoid unknown hazards associated with this unique environment.
Fig. 3.

Peak sagittal kinematic angles equating level and sloped walking. Error bar represent ± 1 standard deviation and * signifies a significant change in kinematics between conditions at p ≤ 0.05.
Fig. 4.
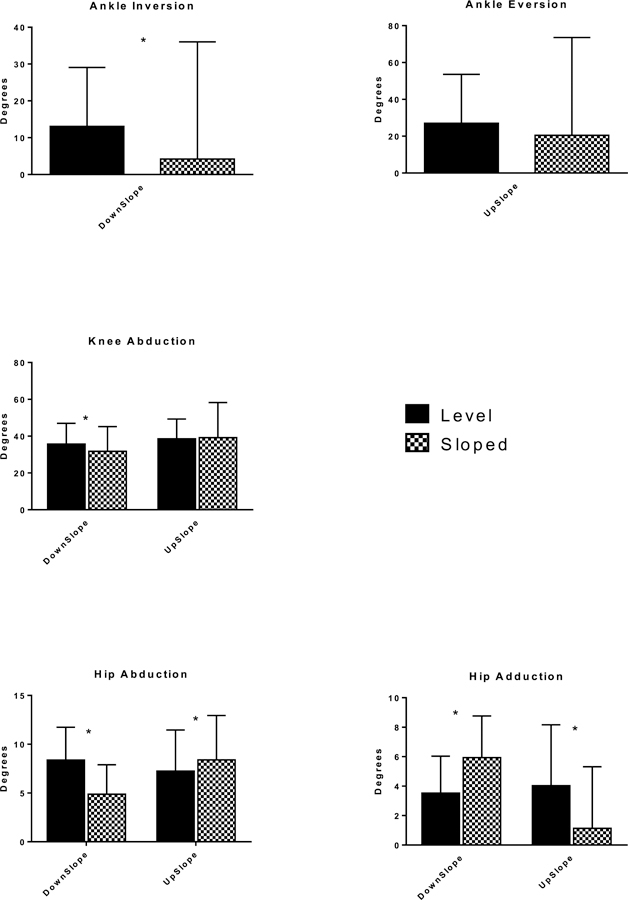
Peak frontal kinematic angles equating level and sloped walking. Error bar represent ± 1 standard deviation and * signifies a significant change in kinematics between conditions at p ≤ 0.05.
Table 2.
Descriptive frontal plane quantitative statistics and results of hypothesis tests of differences between level and sloped differences in the downslope and upslope legs.
| Peak Joint Angle (deg) | DownSlope | UpSlope | ||||||
|---|---|---|---|---|---|---|---|---|
| Frontal | Level | Sloped | Mean Difference | p-value | Level | Sloped | Mean Difference | p-value |
| Ankle Inversion | 13.09 ± 15.98 | 4.23 ± 31.77 | 8.86 | <0.001 | Not Present | |||
| Ankle Eversion | Not Present | 27.06 ± 26.52 | 20.24 ± 53.02 | 6.82 | 0.23 | |||
| Knee Abduction | 35.71 ± 11.23 | 31.79 ± 13.37 | 3.92 | 0.01 | 38.55 ± 10.77 | 39.18 ± 19.06 | −0.63 | 0.76 |
| Hip Abduction | 8.38 ± 3.36 | 4.88 ± 3.01 | 3.50 | < 0.001 | 7.24 ± 4.22 | 8.4 ± 4.54 | −1.16 | 0.02 |
| Hip Adduction | 3.53 ± 2.51 | 5.94 ± 2.82 | −2.41 | < 0.001 | 4.03 ± 4.13 | 1.14 ± 4.17 | 2.89 | < 0.001 |
Acknowledgments
This research was partially funded by the University of Mississippi’s Department of Health, Exercise Science and Recreation Management Graduate Award.
Footnotes
Publisher's Disclaimer: Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health. The mention of trade names, commercial products, or organizations does not imply endorsement by the US Government.
References
- Andres RO, Holt KG, Kubo M, 2005. Impact of railroad ballast type on frontal plane ankle kinematics during walking. Appl. Ergon 36, 529–534. [DOI] [PubMed] [Google Scholar]
- BLS, 2013. Nonfatal Cases Involving Days Away from Work: Selected Characteristics 2011 forward.
- BLS, 2015. Occupational Requirements Survey, Physical Demands Bureau of Labor Statistics; http://www.bls.gov/ncs/ors/physical.htm. [Google Scholar]
- BLS, 2016a. In: Labor D.o. (Ed.), Census of Fatal Occupational Injuries Charts, 1992–2014 (Revised Data [Google Scholar]
- BLS, 2016b. In: Labor D.o. (Ed.), Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work [Google Scholar]
- Compensation, O.B.o.W., 2015. Ohio BWC State Insurance Fund Manual [Google Scholar]
- Damavandi M, Dixon PC, Pearsall DJ, 2010. Kinematic adaptations of the hindfoot, forefoot, and hallux during cross-slope walking. Gait Posture 32, 411–415. [DOI] [PubMed] [Google Scholar]
- Dixon PC, Pearsall DJ, 2010. Gait dynamics of a cross-slope. J. Appl. Biomech 26, 17–25. [DOI] [PubMed] [Google Scholar]
- Gurney B, 2002. Leg length discrepancy. Gait Posture 15, 195–206. [DOI] [PubMed] [Google Scholar]
- Hesse S, Reiter F, Jahnke M, Dawson M, Sarkodie-Gyan T, Mauritz K-H, 1997. Asymmetry of gait initiation in hemiparetic stroke subjects. Arch. Phys. Med. Rehabil 78, 719–724. [DOI] [PubMed] [Google Scholar]
- Holmström E, Engholm G, 2003. Musculoskeletal disorders in relation to age and occupation in Swedish construction workers. Am. J. Ind. Med 44, 377–384. [DOI] [PubMed] [Google Scholar]
- Houglum PA, Bertoti DB, 2011. Brunnstrom’s Clinical Kinesiology FA Davis. [Google Scholar]
- Industries, W.S.D.o.L., 2015. 2015 Base Rates by Business Type and Classification Code
- Kawashima K, Motohashi Y, Fujishima I, 2004. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia 19, 266–271. [DOI] [PubMed] [Google Scholar]
- Kerrigan DC, Lee LW, Collins JJ, Riley PO, Lipsitz LA, 2001. Reduced hip extension during walking: healthy elderly and fallers versus young adults. Arch. Phys. Med. Rehabil 82, 26–30. [DOI] [PubMed] [Google Scholar]
- Khandoker AH, Lynch K, Karmakar CK, Begg RK, Palaniswami M, 2010. Toe clearance and velocity profiles of young and elderly during walking on sloped surfaces. J. NeuroEng. Rehabil 7, 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuster M, Sakurai S, Wood G, 1995. Kinematic and kinetic comparison of downhill and level walking. Clin. BioMech 10, 79–84. [DOI] [PubMed] [Google Scholar]
- LaRoche DP, Cook SB, Mackala K, 2012. Strength asymmetry increases gait asymmetry and variability in older women. Med. Sci. Sports Exerc 44, 2172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lay AN, Hass CJ, Gregor RJ, 2006. The effects of sloped surfaces on locomotion: a kinematic and kinetic analysis. J. Biomech 39, 1621–1628. [DOI] [PubMed] [Google Scholar]
- Lee H-J, Chou L-S, 2007. Balance control during stair negotiation in older adults. J. Biomech 40, 2530–2536. [DOI] [PubMed] [Google Scholar]
- Lee HJ, Chou LS, 2006. Detection of gait instability using the center of mass and center of pressure inclination angles. Arch. Phys. Med. Rehabil 87, 569–575. [DOI] [PubMed] [Google Scholar]
- Leigh JP, Waehrer G, Miller TR, Keenan C, 2004. Costs of occupational injury and illness across industries. Scand. J. Work. Environ. Health 199–205. [DOI] [PubMed]
- Leroux A, Fung J, Barbeau H, 2002. Postural adaptation to walking on inclined surfaces: I. Normal strategies. Gait Posture 15, 64–74. [DOI] [PubMed] [Google Scholar]
- Luepongsak N, Amin S, Krebs D, McGibbon C, Felson D, 2002. The contribution of type of daily activity to loading across the hip and knee joints in the elderly. Osteoarthritis Cartilage 10, 353–359. [DOI] [PubMed] [Google Scholar]
- Mandeville D, Osternig LR, LS C, 2007. The effect of total knee replacement on dynamic support of the body during walking and stair ascent. Clin. BioMech 22, 787–794. [DOI] [PubMed] [Google Scholar]
- Masani K, Vette AH, Kouzaki M, Kanehisa H, Fukunaga T, Popovic MR, 2007. Larger center of pressure minus center of gravity in the elderly induces larger body acceleration during quiet standing. Neurosci. Lett 422, 202–206. [DOI] [PubMed] [Google Scholar]
- McIntosh A, Beatty K, Dwan L, Vickers D, 2006. Gait dynamics on an inclined walkway. J. Biomech 39, 2491–2505. [DOI] [PubMed] [Google Scholar]
- Mutual L, 2018. Liberty Mutual Workplace Safety Index, vol. 2 Myroofcom, 2017. Typical Roof Pitch. [Google Scholar]
- OHSA, 2017. Final Rule to Update General Industry Walking-working Surfaces and Fall Protection Standards Subpart D – Walking-Working Surfaces - OSHA. [Google Scholar]
- Perry J, Burnfield JM, 2010. Gait Analysis: Normal and Pathological Function, second ed. Slack Incorporated [Google Scholar]
- Perry J, Davids JR, 1992. Gait analysis: normal and pathological function. J. Pediatr. Orthop 12, 815. [Google Scholar]
- Province MA, Hadley EC, Hornbrook MC, Lipsitz LA, Miller JP, Mulrow CD, Ory MG, Sattin RW, Tinetti ME, Wolf SL, 1995. The effects of exercise on falls in elderly patients: a preplanned meta-analysis of the FICSIT trials. J. Am. Med. Assoc 273, 1341–1347. [PubMed] [Google Scholar]
- Redfern M, DiPasquale J, 1997. Biomechanics of descending ramps. Gait Posture 6, 119–125. [Google Scholar]
- Romero DH, Van Gemmert AW, Adler CH, Bekkering H, Stelmach GE, 2003. Time delays prior to movement alter the drawing kinematics of elderly adults. Hum. Mov. Sci 22, 207–220. [DOI] [PubMed] [Google Scholar]
- Roofkeycom, 2017. Types of Roofing.
- Systems, M., 2017. Your Home: Determine Roof Pitch
- Wade C, Davis J, 2009. Postural sway following prolonged exposure to an inclined surface. Saf. Sci 47, 652–658. [Google Scholar]
- Wade C, Davis J, Weimar WH, 2014. Balance and exposure to an elevated sloped surface. Gait Posture 39, 599–605. [DOI] [PubMed] [Google Scholar]
- Wannop JW, Worobets JT, Ruiz R, Stefanyshyn DJ, 2014. Footwear traction and three-dimensional kinematics of level, downhill, uphill and cross-slope walking. Gait Posture 40, 118–122. [DOI] [PubMed] [Google Scholar]
- Wearing SC, Hennig EM, Byrne NM, Steele JR, Hills AP, 2006. Musculoskeletal disorders associated with obesity: a biomechanical perspective. Obes. Rev 7, 239–250. [DOI] [PubMed] [Google Scholar]
- Welch L, Haile E, Boden LI, Hunting KL, 2009. Musculoskeletal disorders among construction roofers—physical function and disability. Scand. J. Work. Environ. Health 56–63. [DOI] [PubMed]
- Welch LS, Haile E, Boden LI, Hunting KL, 2008. Age, work limitations and physical functioning among construction roofers. Work 31, 377–385. [PubMed] [Google Scholar]
- Welch LS, Haile E, Boden LI, Hunting KL, 2010. Impact of musculoskeletal and medical conditions on disability retirement—a longitudinal study among construction roofers. Am. J. Ind. Med 53, 552–560. [DOI] [PubMed] [Google Scholar]
- Winter DA, 1991. Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological [Google Scholar]
- Yogev G, Plotnik M, Peretz C, Giladi N, Hausdorff JM, 2007. Gait asymmetry in patients with Parkinson’s disease and elderly fallers: when does the bilateral coordination of gait require attention? Exp. Brain Res 177, 336–346. [DOI] [PubMed] [Google Scholar]
- Zeni J Jr, Richards J, Higginson J, 2008. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 27, 710–714. [DOI] [PMC free article] [PubMed] [Google Scholar]