

Abstract
Background:
Religious obligation helps people to develop mental health by creating internal commitment to special rules. This meta-analysis aimed to determine the relationship between religious orientation and anxiety among college students.
Methods:
Major scientific databases including PubMed, Web of Science, Science Direct, EBSCO, ProQuest and PsycINFO were searched for original research articles published 1987–2016. A random effect model was used to combine Correlation coefficient. All analyses were performed using Stata MP.
Results:
After screening of 7235 documents, 13 articles including 5620 participants met inclusion criteria in this meta-analysis. Correlation coefficient was −0.08 (95% CI= −0.19, −0.03) which indicated with increasing religious orientation, anxiety and depression reduced (P<0.001). Characteristics such as sex, geographic region, and type of religions were potential sources of heterogeneity. Based on fill-and-trim method the adjusted pooled r was obtained, −0.06 (95% CI= −0.16, −0.04).
Conclusion:
There was a weakness relationship between religious orientation and mental anxiety and depression. Therefore, it needs to improve knowledge of student about advantages of religious orientation.
Keywords: Religious orientation, Anxiety, Depression, Meta-analysis
Introduction
Religion and faith refer to a set of customs and beliefs manifested in a religious entity (1). While it can be conceptualized as a wide structure without financial goals (2). Coning et al. (3), defined religion to facilitate movement toward God (4). Religion has a positive relationship with physical, mental, and physiological parameters (5, 6).
From religious perspective, there are internal and external religions. In internal religious orientation, faith is a transcendent value considered as inclusive motivation commitment (7). Moreover, internal religion is related to adaptation ability, expectancy (8), ability to find meaning of life in diseases (9), and better adaptation to stressful events (10). However, in external religious orientations, religion is an external tool to satisfy personal needs such as position and security. In other words, religiosity functions to obtain security and social status and those with this orientation, use religion as a tool to reach their wishes (11).
Most of mental disorders that result from psychological distress and bitterness of life are observed among non-religious people (12). Religious beliefs lead to positive emotions and feelings among people who improve physical health by strengthening the immune system (13). Since students constitute sensitive and important members of society with young age, their lifestyle is very important because it improves their health level where religion, is an important factor that promotes physical and mental health of this group (14).
According to the reports by National Mental Health Association (NMHA), 46% of male students and 64% of female students suffer from anxiety (3). The importance of anxiety and depression among students due to expansion of this disorder from initial stages of life (youth) to next stages, in addition to lowering daily activities, creates mental disorders, compliance problems, and crime in the future (6). Due to the importance that religion has in mental health of society, most medical schools in the United States (84 out of 126) are presenting religious courses (15). Studies on religious orientation among students with mental health indexes, such as depression and anxiety, have indicated different results for students in different countries (16, 17). Reviewing 130 studies, 34% of previous studies have pointed to a positive relationship between religious coping, adaptation, and mental health while 4% negatively evaluated this relationship and 62% of studies did not report any relationship between these variables (3, 8, 18). Moreover, by increasing religious orientation among students, depression and anxiety decreased and as a result, mental health increased (2).
Different educational, social, gender, racial, and cultural conditions of students in different countries can be the reasons for the controversial findings. To address this gap, the present study investigated the relationship between religion orientation and mental health among college students.
Methods
Ethic Committee Approval
We received the necessary permissions and obtaining the code of ethics with the characteristic IR.SSU.SPH.REC.1395.5 from the Ethics Committee of Shahid Sadoughi University of Medical Sciences for the necessary coordination.
Search Strategy
This study was conducted according to PRISMA guidelines (http://www.prisma-statement.org/). The literature search was conducted via major online scientific databases including PubMed, Web of Science, Scopus and PsycInfo, EBSCO and ProQuest from Apr 1987 to Sep 2016 using the following keywords: “religion” OR “religiosity” OR “spirituality OR “religiousness” OR “Religious coping” OR ” Islam” OR “Mohammedanism” OR “Christianity” OR “church” OR “Religiousness” AND (“Orientation”) AND (“Anxiety” OR “Stress” OR “Depression “ OR “Mental health”) AND (“Student”).
Inclusion and exclusion criteria
All studies included in this meta-analysis were required to have investigated the relationship between anxiety and religious orientation among student (undergraduate at university or high school) and excluded studies which had other participants.
Observational studies (cross-sectional, case-control) were included. Review articles and conference articles which not included quintile index (correlation coefficient) proceedings were excluded.
Studies with sample size more than 30 participates were included.
Language of studies was limited to English
The correlation coefficient between anxiety and religious orientation was reported, and sample size to calculate effect size (ES) was existed in the results of study.
Data extraction
Information was extracted from the included studies by two independent reviewers (SF and SHT), who had experience with religious orientation and anxiety research and used a standard form to extract data. Any disagreement was resolved by discussion between the two reviewers. If consensus could not be reached, a third reviewer (EM) was consulted.
The standard form consisted of the following variables; title of study, authors’ names, year of publication, type of study, where the study was conducted, type of population, mean and standard deviation of correlation coefficient (19) age range (years), sample size, of study, sex, quality of study (QS) and the correlation coefficient between anxiety and religious orientation of student as a statistical index for using in meta-analysis. Quality of each included studies was assess by independent reviewers using standard checklist, Newcastle-Ottawa Scale (NOS). This tool has eight items and each item include three categories. The Kappa index used to examine agreement of two reviewers.
Statistical analysis
In this meta-analysis, the correlation coefficient (r) was extracted from each study and then standard error (SE) was calculated by the following equation: (where n is the sample size of study). Cochran’s heterogeneity statistic (P<0.1) and the I-squared index (25%: low; 50%: medium and 75%: high) were used to evaluate heterogeneity across effect sizes (ESs).
The results for each factor and pooled estimates were presented in a forest plot in which we reported the results as ES with 95% confidence intervals (CI). Meta-regression and subgroup analysis were used to evaluate source of heterogeneity among studies. Potential publication bias was explored using Funnel plot and Begg’s test. A trim-and-fill method was performed to detect the effect of missing studies on the overall effect of meta-analysis. All statistical analyses were done with the Statistical Software Package Stata MP version 14.
Results
The search yielded 7244 articles of them 707 were duplicate records. After screening titles or abstracts by both authors, 5819 articles were removed as they did not meet all the inclusion criteria. Full text of 709 articles assessed for eligibility of them 696 records were excluded due to: being irrelevant (3176), reported depression, other mental disorders without anxiety (618) or anxiety without religious orientation (78 studies). Finally, 13 studies remained in the systematic review of which 11 studies reported correlation coefficient to be used in meta-analysis (Fig. 1).
Fig. 1:
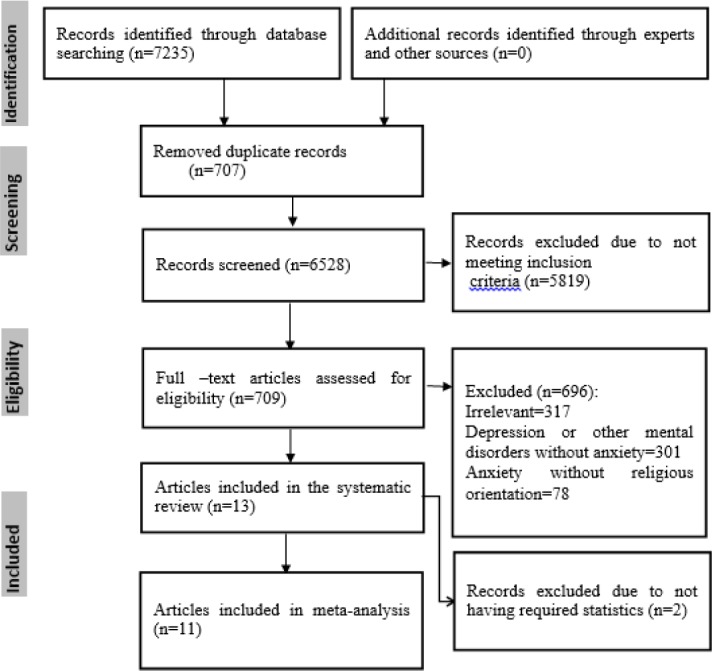
PRISMA flowchart describing the study design process
Two reviewers assessed quality of included studies using a standard checklist; the Kappa index was examined to agreement of reviewers which showed a high agreement (Kappa=79%) between them. All included studies were cross-sectional study and most studies have been conducted in USA and Iran (%23), UK (%15) and Spain (%15). The total number of participants in the included studies was 5620 (range= 45 to 1786). Except for two studies, participates of other studies were undergraduate student at university (REFE). On average 54.1% of cases were male and the mean age of students was 19.9 yr. Six studies undertook on Muslims, two on Christian religions and three studies did not mention any particular religion.
In two studies, correlation coefficient was not reported, so were excluded (Table 1).
Table 1:
The characteristics of selected studies for the meta-analysis of the relation between anxiety and religious orientation in college students 1986–2016
| Author | Year of study | Type of study | Country | Type of Population | Type of Religions | Total cases | Mean ±SD | Male (%) | QS | r |
|---|---|---|---|---|---|---|---|---|---|---|
| Maltby J et al ( 1 ) | 1999 | cross-sectional | UK | USU | Not reported | 360 | 20.41±2.5 (18–29) | 47.8 | 21 | 0.11 |
| Amrai K et al ( 2 ) | 2011 | cross-sectional | Iran | USU | Muslim | 347 | NR | 38.9 | 23 | NR |
| Buzdar M.A et al( 3 ) | 2014 | cross-sectional | Iran | USU | Muslim | 502 | NR | 0.0 | 18 | 0.011 |
| García J et al( 4 ) | 2013 | cross-sectional | Spain | USU | Non-Muslim | 180 | 20.91±6.7 (18–55) | 23.3 | 24 | NR |
| Steffen P.R et al ( 5 ) | 2013 | cross-sectional | USA | USU | Non-Muslim | 1025 | 20.91±3.7 (18–31) | NR | 17 | −0.33 |
| Lavrič M et al ( 6 ) | 2007 | cross-sectional | UK | USU | Muslim and Non-Muslim | 1786 | 20.91±1.5 (20–21) | NR | 20 | −0.149 |
| Ghorbani N et al( 7 ) | 2008 | cross-sectional | Iran | USU | Muslim | 131 | 20.91±2.0 (NR) | 38.9 | 25 | −0.05 |
| Khan Z.HP et al ( 8 ) | 2008 | cross-sectional | Pakistan | USU | Muslim | 160 | 21.4±1.8 (NR) | 48.8 | 20 | 0.18 |
| Bergin A et al ( 9 ) | 1987 | cross-sectional | USU | No referred | 151 | NR | 100.0 | 22 | −0.27 | |
| Maltby, J., et al ( 10 ) | 1999 | cross-sectional | Spain | USU | No referred | 474 | 20.3±2.5 (18–29) | 53.0 | 19 | −0.17 |
| Kuyel N et al ( 11 ) | 2012 | cross-sectional | Turkish | USU | Muslim | 341 | 21.05±1.6 (18–26) | 100.0 | 14 | −0.02 |
| Davis T.L et al( 12 ) | 2003 | cross-sectional | USA | HSS | Catholic, Protestant, Mormon, Jewish, other Christian, no religion | 45 | 15.2±0.92 (14–17) | 44.4 | 18 | −0.45 |
| Pierce Jr J.D et al( 13 ) | 2007 | cross-sectional | USA | HSS and HSS | Catholic, Protestant | 118 | 18.8±2.7 (13–25) | 100.0 | 22 | 0.24 |
NR: Not Reported; USU: Undergraduate Student at University; HSS: High School Student; n: sample size; QS=Quality of studies
Generally, eleven studies met the eligibility criteria in this meta-analysis. The results of Q-Cochran and I-squared tests showed an evidence of high heterogeneity among correlation coefficient of studies (I-squared=92.5%, P<0.001). Using random effect meta-analysis pooled estimate of relationship between anxiety and religious orientation was −0.08 (95%CI=−0.19-0.03) which indicated that religious orientation was negatively correlated with anxiety in other words with increasing religious orientation, anxiety significantly reduces (P<0.001). In most studies (seven studies) a negative correlation between anxiety and religious orientation were reported; the highest and lowest correlation coefficients were reported, (r=−0.45) and (r=0.011) respectively (Fig. 2). To explore source of heterogeneity among the included studies meta-regression analysis was performed. Variables such as age, sex, country, type of religion, sample size and year of publication of paper were examined as possible sources of heterogeneity; however, the results of meta-regression indicated none of the variables may cause heterogeneity (P>0.05) ( Table 2 ).
Fig. 2:

Forest plot of relationship between anxiety and religious orientation. The middle-point in each line indicates the correlation rate and the length of each line indicates the 95% confidence interval of each study. Diamonds indicate the 95% confidence interval for all studies
Table 2:
Meta-regression to assess characteristics effect on relationship between anxiety and religious
| Variables | Coeff. | Std. Err | t | P |
|---|---|---|---|---|
| Age | 0.11 | 0.06 | 2.06 | 0.18 |
| Sex | 0.0005 | 0.003 | 0.01 | 0.99 |
| Country | −0.03 | 0.08 | −0.40 | 0.73 |
| Type of religions | 0.29 | 0.23 | 1.25 | 0.34 |
| Sample size | −0.0009 | 0.0007 | 0.01 | 0.99 |
| Year of publication | 0.04 | 0.02 | 1.64 | 0.24 |
In addition, subgroup analysis was used to identify the possible sources of heterogeneity. Inverse relationship between anxiety and religious orientation among females was larger than males. This relationship among students in the US was significantly larger than students in Europe and Asia. Moreover, non-Muslim students had significantly stronger correlation than Muslim and Non-Muslim students (P<0.001) (Table 3).
Table 3:
Subgroup meta-analysis to compare relationship between anxiety and religious orientation
| Characteristics | Factors | N | r (95%CI) | I-square (%) | P-value |
|---|---|---|---|---|---|
| Sex | Male | 4 | −0.06(−0.1, −0.03) | 93.2 | P <0.001 |
| Female | 7 | −0.22(−0.26, −0.18) | 88.7 | ||
| Geographic region | America | 3 | −0.20(−0.26, 0.16) | 96.5 | P <0.001 |
| Europe | 3 | −0.14(−0.17, 0.10) | 88.4 | ||
| Asia | 5 | −0.008(−0.06, −0.04) | 57.7 | ||
| Religion | Muslim | 4 | −0.01(−0.60, 0.42) | 57.7 | P <0.001 |
| Non-Muslim | 4 | −0.23(−0.27, −0.18) | 96.3 | ||
| Muslim and No-Muslim | 3 | −0.13(−0.16, −0.09) | 88.8 |
The funnel plot for the included studies shows a relatively asymmetric. The results of Begg’s test confirmed these results (z=0.26, P=0.031), therefore, both methods indicated a considerable publication bias. After applying fill-and-trim method, the pooled estimate of relationship between anxiety and religious orientation found −0.060 (95% CI= −0.158, −0.038) and the pooled estimate found slightly larger. In other words, the effect of not included studies in meta-analysis found to be low (Fig. 3).
Fig. 3:

Funnel plot for publication bias among studies
Discussion
Religious orientation has a negative relationship with students’ anxiety. However, in external religion orientation, anxiety level increases. The inverse relationship between anxiety and religious orientation among women was more than men. These values were larger among Americans compared to Europeans and Asians, respectively. Moreover, non-Muslims had stronger correlation compared to Muslims and Christians, respectively. The relationship between religious orientation, mental health, and moral transformation was investigated among 384 students in Qom, Iran; mental health has positive relationship with religious orientation and moral transformation. In addition, religious orientation, gender, and education can predict mental health. By improving internal religious orientation and encouraging education, improving mental health is possible (20). Moreover, religious beliefs, PTSD, depression, and flexibility were investigated in survivors of earthquake in Haiti. About 92% of the participants believed in supernatural powers. There was a significant difference between decreased anxiety scores after the event, PTSD, and increased flexibility in people who believed these events are due to providence of God and those who had different views (21). Remembrance of God is a factor that increases tolerance against pressures that leads to increased self-control and moral development. With increased orientation toward internal religious, self-control ability increases that prevents the effects of external factors or demographic characteristics and preserves mental health. Moreover, performing religious orders and attending religious rituals can be effective in the treatment and prevention of mental diseases such as severe psychosis (22).
The results of a meta-analysis on religious studies and mental health showed that in 44% of studies, positive relationships are tangible and 23% showed negative relationships between religion and mental health and in 35% of studies, no significant relationship can be found (23).
It is possible to find evidence that indicate the positive effect of religion on mental health (24) which is consistent with the results of the present study, because the relationship between religious orientation and anxiety is stronger among Muslims and in Iran, as one of the Muslim countries, various studies have been conducted (25, 26) showed the effect of positive religious orientation on mental health.
A significant relationship was found between religious orientation and mental health dimensions where the highest correlation was observed between religious orientation, depression, and suicide. Whenever religious orientation decreases or becomes external, depression increases and intention to commit suicide increases, too. Religious people feel less depression with lower suicide intention. The relationship between uncontrollable stress and depression for people with external religious behavior was stronger compared to those with internal religious orientation (19). Therefore, people with internal religious orientation and belief in origin and destination of excellence are more hopeful, believe in God, predict pleasant events and in the case of unpleasant events, rely on God. The relationship between internal religious orientation and anxiety was observed (26) showed highest and lowest correlation coefficients, respectively. Evidence were observed based on religious humility and its acceptable correlation with depression symptoms at the level of two variables. By studying the obtained results based on the available evidence, this relationship is observed in both genders, age groups, and different ethnicities (27).
Conducted study on 140 male and female students studying at universities in Tehran, a direct relationship between religiosity and mental health was found. By increased external religious orientation, fatigue and physical symptoms increase. The highest correlation level was related to depression and intention toward suicide. External religious orientation was increasing parallel to increase in depression(23).
People’s health was investigated by scientific and religious views with hope, purpose in life, and fear of death among 474 Muslim students. Religiosity is positively related to all health factors. Scientific views were related to people’s health at higher levels. Hence, belief in science or God positively influences the health condition (28).
The relationship between religious orientation and depression were investigated among 571 students of Islamic Azad University of Azad Shahr. There are an inverse and significant relationship between religious orientation and depression and when students’ religious orientation increases, their depression and anxiety levels decrease. This study showed that there is a close relationship between students’ religious orientation, anxiety, and depression. Therefore, internalization of religious values can lead to increased mental health level of students (29). Despite contradictory and different definitions of religion and spirituality, both are considered as symbolic dimension of human that facilitate understanding of fundamental concepts such as purpose of creation and life. On the other hand, religion/spirituality are positively related to different mental and physiological health parameters. Religious beliefs can lead to positive emotions in people where improved immune system, promotes physical health.
Religion can create meaning; therefore, it gives meaning to life and death, increases life expectancy, and promotes optimism and can compensate decreased self-control. It prescribes a type of healthier lifestyle that positively influences mental health and includes a set of positive social norms that lead to acceptance by others, a type of supernatural feeling that undoubtedly causes psychological effects (30).
Limitations of this study consisted of low number of studies about variables of interest. Therefore, those studies that indirectly pointed to this issue such as studies on the relationship between anxiety, depression, and other psychological problems were used. Authors of this meta-analysis attempted to use all studies done at specific time intervals. Of course, there are different studies ignored by the authors of this study. Therefore, it is suggested to investigate those studies included non-student samples in future meta-analyses. There are numerous factors related to religious orientation and only limited variables are not sufficient to study the relationships and it is suggested to consider other variables in future studies. Such meta-analyses point to the gaps that exist in previous studies and help the author to consider the criteria ignored in previous studies. The limitations of such meta-analyses include access to sources and studies conducted and published in certain areas. Therefore, it is better to welcome repeated subjects to investigate more samples from the population of interest. Moreover, it rarely occurs that all studies which integrate with meta-analysis, show required indexes for analyses. This is considered among fundamental limitations of this meta-analysis.
Conclusion
Religious teachings and improving beliefs help people to move toward perfection, growth, and mental health. Believe in God creates this ability in person to eliminate factors of anxiety and depression. According to the students’ mental health, universities and society should perform programs to improve religious values. Finally, despite lack of scientific interests in psychological dimension and humanities, religion can provide a framework for mental health. By providing the context and integration of religion with cognitive and emotional dimensions and moving from religious belief to internal religion, can improve mental health.
Ethical considerations
Ethical issues (Including plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, redundancy, etc.) have been completely observed by the authors.
Acknowledgements
This article is part of a Ph.D. by research thesis in Social Determinants of Health Research Center focused on College Students religious orientation, physical and psychological health funded by Vice Chancellor for Research, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. With ethics code of IR.SSU.SPH.REC.1395.51 and registration code of 4997. The authors wish to thank Dr. Mohammad Salehi-Marzijarani for his cooperation in the study.
Footnotes
Conflict of interest
The authors declare that they have no competing interests.
References
- 1. Maltby J, Day L. (2000). Depressive symptoms and religious orientation: Examining the relationship between religiosity and depression within the context of other correlates of depression. Pers Individ Dif, 28( 2): 383– 93. [Google Scholar]
- 2. Amrai K, Zalani HA, Arfai FS, Sharifian MS. (2011). The relationship between the religious orientation and anxiety and depression of students. Procedia Soc Behav Sci, 15: 613– 16. [Google Scholar]
- 3. Buzdar MA, Ali A, Nadeem M, Nadeem M. (2015). Relationship between religiosity and psychological symptoms in female university students. J Relig Health. 54( 6): 2155– 63. [DOI] [PubMed] [Google Scholar]
- 4. García-Alandete J, Bernabé-Valero G. (2013). Religious Orientation and Psychological Well-Being among Spanish Undergraduates [Orientaciones religiosas y bienestar psicológico de los estudiantes universitarios españoles]. Acción Psicológica, 10( 1): 135– 48. [Google Scholar]
- 5. Steffen PR. (2014). Perfectionism and life aspirations in intrinsically and extrinsically religious individuals. J Relig Health, 53( 4): 945– 58. [DOI] [PubMed] [Google Scholar]
- 6. Lavrič M, Flere S. (2010). Trait anxiety and measures of religiosity in four cultural settings. Ment Health Relig Cult, 13( 7–8): 667– 82. [Google Scholar]
- 7. Ghorbani N, Watson P, Shahmohamadi K. (2008). Afterlife Motivation Scale: Correlations with maladjustment and incremental validity in Iranian Muslims. Int J Psychol Religion, 18( 1): 22– 35. [Google Scholar]
- 8. Khan ZH, Watson P, Cothran DL. (2008). Self-control in Pakistani Muslims: relationships with religious orientation, depression and anxiety. Journal of Beliefs & Values, 29( 2): 213– 6. [Google Scholar]
- 9. Bergin AE, Masters KS, Richards PS. (1987). Religiousness and mental health reconsidered: A study of an intrinsically religious sample. J Couns Psychol, 34( 2): 197– 204. [Google Scholar]
- 10. Maltby J, Lewis CA, Day L. (1999). Religious orientation and psychological well-being: The role of the frequency of personal prayer. Br J Health Psychol, 4( 4): 363– 78. [Google Scholar]
- 11. Kuyel N, Cesur S, Ellison CG. (2012). Religious orientation and mental health: A study with Turkish university students. Psychol Rep, 110( 2): 535– 46. [DOI] [PubMed] [Google Scholar]
- 12. Davis TL, Kerr BA, Kurpius SER. (2003). Meaning, Purpose, And Religiosity In At-Risk Youth: The Relationship Between Anxiety And Spirituality. J Psychol Theol, 31( 4): 356– 65. [Google Scholar]
- 13. Pierce JD, Jr, Cohen AB, Chambers JA, Meade RM. (2007). Gender differences in death anxiety and religious orientation among US high school and college students. Ment Health Relig Cult, 10( 2): 143– 50. [Google Scholar]
- 14. Wills TA, Yaeger AM, Sandy JM. (2003). Buffering effect of religiosity for adolescent substance use. Psychol Addict Behav, 17( 1): 24– 31. [DOI] [PubMed] [Google Scholar]
- 15. Fortin AH, 6th, Barnett KG. (2004). STUDENTJAMA. Medical school curricula in spirituality and medicine. JAMA, 291( 23): 2883. [DOI] [PubMed] [Google Scholar]
- 16. Abdel-Khalek AM, Lester D. (2012). Constructions of religiosity, subjective well-being, anxiety, and depression in two cultures: Kuwait and USA. Int J Soc Psychiatry, 58( 2): 138– 45. [DOI] [PubMed] [Google Scholar]
- 17. Cokley KON, Beasley S, Holman A, et al. (2013). The moderating role of gender in the relationship between religiosity and mental health in a sample of black American college students. Ment Health Relig Cult, 16( 5): 445– 62. [Google Scholar]
- 18. Pargament KI. (2001). The psychology of religion and coping: Theory, research, practice. Revised 1st ed Guilford Press, New York, pp.: 150– 161. [Google Scholar]
- 19. Darvyri P, Galanakis M, Avgoustidis AG, et al. (2014). The Revised Intrinsic/Extrinsic Religious Orientation Scale in a Sample of Attica’s Inhabitants. Psychology, 5( 13): 1557– 67. [Google Scholar]
- 20. Etesaminia H. (2015). Relationship between religious orientation and mental health and moral development. Psychology and Religion, 8( 1): 115– 28. [Google Scholar]
- 21. Blanc J, Rahill GJ, Laconi S, Mouchenik Y. (2016). Religious beliefs, PTSD, depression and resilience in survivors of the 2010 Haiti earthquake. J Affect Disord, 190: 697– 703. [DOI] [PubMed] [Google Scholar]
- 22. Jung CG. (2001). Modern man in search of a soul. 2nd ed Psychology Press, New York, pp.: 196– 208. [Google Scholar]
- 23. Mahmodi G, Hassanzadeh R, Heidari G. (2007). The effect of sex education on family health on Mazandran medical university students. The Horizon of Medical Sciences, 13( 2): 64– 70. [Google Scholar]
- 24. Kendler KS, Liu X-Q, Gardner CO, et al. (2003). Dimensions of religiosity and their relationship to lifetime psychiatric and substance use disorders. Am J Psychiatry, 160( 3): 496– 503. [DOI] [PubMed] [Google Scholar]
- 25. Ghaderi D. (2011). The Survey of Relationship Between Religious Orientation and Happiness Among the Elderly Man and Woman in Tehran. Ira J Ageing, 5( 4): 64– 71. (In Persian) [Google Scholar]
- 26. Büssing A, Ostermann T, Matthiessen PF. (2005). Role of religion and spirituality in medical patients: confirmatory results with the SpREUK questionnaire. Health Qual Life Outcomes, 3: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Smith TB, McCullough ME, Poll J. (2003). Religiousness and depression: evidence for a main effect and the moderating influence of stressful life events. Psychol Bull, 129( 4): 614– 34. [DOI] [PubMed] [Google Scholar]
- 28. Aghababaei N, Sohrabi F, Eskandari H, et al. (2016). Predicting subjective well-being by religious and scientific attitudes with hope, purpose in life, and death anxiety as mediators. Pers Individ Dif, 90: 93– 8. [Google Scholar]
- 29. Bayani A. (2008). The relationship between the religious orientation and anxiety and depression of university students. Journal of Fundamentals of Mental Health, 10( 39): 209– 14. [Google Scholar]
- 30. Rippentrop AE, Altmaier EM, Chen JJ, et al. (2005). The relationship between religion/spirituality and physical health, mental health, and pain in a chronic pain population. Pain, 116( 3): 311– 21. [DOI] [PubMed] [Google Scholar]