

Abstract
Aim:
The aim of the study is to compare the efficiency of six-stranded coaxial tubular superelastic nickel–titanium (NiTi) archwire and a single-stranded wire in relieving anterior mandibular crowding.
Materials and Methods:
This double-blind randomized study included 40 patients, categorized into two groups: Sentalloy round group and Speed tubular supercable group (20 each). After taking alginate impressions, the allocated archwire was engaged. With a digital caliper, intercanine, interpremolar, and intermolar width were recorded on the study models, immediately and at 4, 8, and 12 weeks stages. The Statistical Package for the Social Sciences (SPSS) version 20 was used for analysis.
Results:
The measured parameters were increased in both the groups, with the difference being insignificant statistically.
Conclusion:
Superelastic coaxial NiTi wires show better efficiency in relieving anterior crowding than single-stranded NiTi wire.
KEYWORDS: Anterior crowding, digital caliper, intercanine width, nickel–titanium wire, superelastic coaxial nickel–titanium wire
INTRODUCTION
Inadequate arch width or arch perimeter is one of the major causes for crowding of teeth. The intermolar width and intercanine width are considered as clinical indicators for measuring arch expansion and can be easily measured.[1] To achieve arch expansion, either of conventional fixed appliances or rapid maxillary expansion appliances are usually employed. In a few cases, archwires are used for expansion.[2] The properties that influence the clinical performance of wires are low modulus of elasticity, flexibility, resilience, high spring back, corrosion resistance, ease of bracket engagement, and biocompatibility.
Many varieties of archwires are available, each having their own pros and cons when compared to the other. They are available in different configurations, solid, multistranded, looped, or tubular. Each one imparts a distinctive force level, due to variation in elastic modulus. Studies have shown that for initial stages of treatment, nickel–titanium (NiTi) wires are ideal, due to their low stiffness, which produces low-intensity forces. They can be employed as single-stranded archwires or as multistranded archwires, the later showing increased flexibility and reduced load deflection rate.[3,4]
Recently, speed six-stranded coaxial tubular superelastic NiTi is introduced into the market. It has advantage over single-stranded superelastic NiTi in many ways such as shortening of treatment time, increased spring back, deformation resistance, and low-force delivery.[3,4,5]
Our study aims to clinically assess the expansion effectiveness of six-stranded coaxial tubular superelastic NiTi-speed tubular super (STS) cable and single-stranded superelastic NiTi Sentalloy by measuring the change in intermolar width and intercanine width at 4-, 8-, and 12-week interval.
MATERIALS AND METHODS
This double-blind study included 40 patients, between 12 and 18 years reported to the Department of Orthodontics and Dentofacial Orthopaedics, Pushpagiri College of Dental Sciences, Thiruvalla, Kerala. Ethical committee clearance was attained from the institution (Ethical Committee No: PCDS/IEC/S20/12/14) and informed consent was obtained from the participants. Sample size was determined from similar studies using the formula: n=[(z∝+zβ)]. With a confidence interval of 95% and power of 95% for the study, a sample size of 40 was obtained. The mandibular anterior crowding was assessed based on Little's Irregularity Index.[6]
The selected patients were divided into two groups, that is, Sentalloy round (SR) group (Light Archform, Dentsply-GAC, International) and STS cable group (Speed System Orthodontics, Ontario, Canada), 20 in each group. The allocation of archwire was randomized by means of computer software created numbers. Envelops were used to assign archwire for the two groups, thus concealing both the investigator and the participant. Bracket bonding and archwire placement were done by the same orthodontist. No other archwires were used.
INCLUSION CRITERIA
Patients between 12 and 18 years with lower anterior crowding and with mandibular irregularity index more than 6
Class I skeletal pattern
Extraction treatment with two first premolars in mandibular arch
Eruption of all mandibular teeth excluding third molars with no spacing between them
Normal medical history
No recent history of intake of drugs such as nonsteroidal anti-inflammatory drugs
No previous active orthodontic treatment.
EXCLUSION CRITERIA
Developmental anomalies in the dentition
Abnormal root morphology in lower arch
Patients with periodontal disease and loss of attachment.
SAMPLE SIZE DETERMINATION
Number of participants was calculated to select sample for the present study using the formula: n=[(z∝+zβ)].[2] A sample of 36 was obtained with a confidence interval of 95% and power of 95% for the study. It was decided to select 40 participants, with the expectation of dropouts.
DATA COLLECTION
For each patient, a high-quality alginate impression of the lower dental arch was obtained at the preexpansion phase after placing bonded attachment and bands. The allocated archwire which came in a sterilized opaque cover was taken and then engaged as fully as possible into the bracket using elastomeric modules. At routine follow-up appointment after 4 weeks, participants were recalled, archwires removed, and alginate impressions were taken and poured immediately with stone, to obtain the study models. The archwires were ligated and activated with elastomeric modules or steel ties. Entire process was replicated another time after 8 and 12 weeks, by a single operator.
MEASUREMENT OF STUDY CAST
With a fine tip digital caliper (Digimatic 0–6 inch, Mitutoyo, Japan), measurements were recorded on the study models [Figure 1]. Individual points were noted for molar width and intercanine width [Figures 2 and 3]. All the readings were recorded by a single expert operator in a double-blind manner immediately, at 4, 8, and 12 weeks [Figure 4].
Figure 1.
Digital caliper for recording measurements
Figure 2.
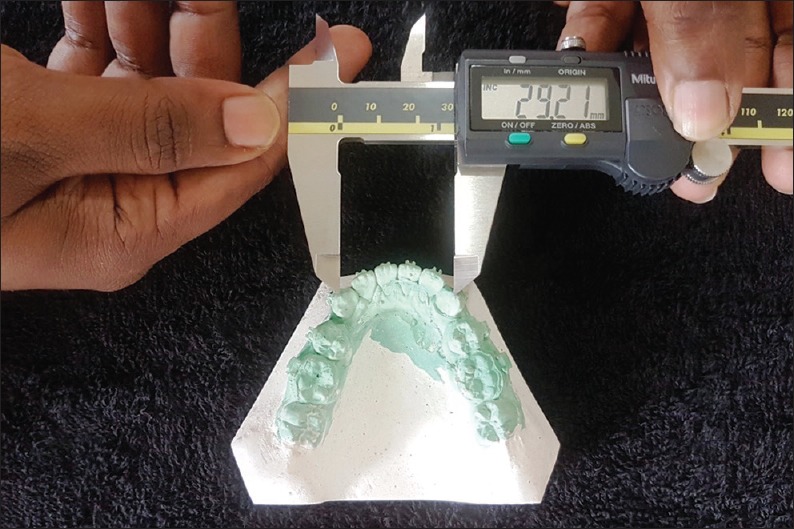
Measuring intercanine width
Figure 3.
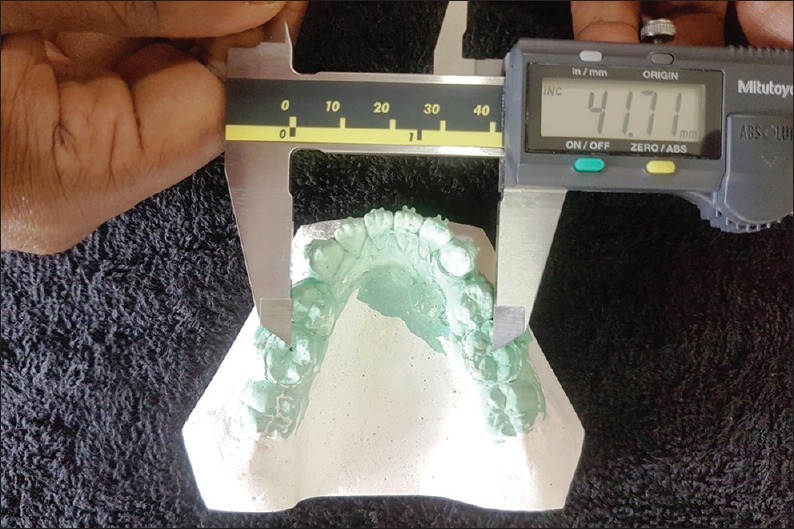
Measuring intermolar width
Figure 4.
Four aligning stages
Duplicate readings were taken on the cast at the commencement and at the end of the study in ten cases to assess intraoperator reliability to get an idea of measurement error in the study. Statistical Package for the Social Sciences (SPSS) version 20 for Windows software was used for analysis.
RESULTS
On Statistical evaluation, the median values of the intercanine, interpremolar, and intermolar width demonstrated a rise with the progression of time from the 1st week to the 12th week. This was consistently seen in all observations except for the intermolar width in the speed tubular group which showed a decrease [Tables 1 and 2].
Table 1.
Mean and standard deviation
| Wire type | ICWP | ICW4 | ICW8 | ICW12 | IPMWP | IPMW4 | IPMW8 | IPMW12 | IMWP | IMW4 | IMW8 | IMW12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SR | ||||||||||||
| Mean | 26.07800 | 27.10850 | 27.58842 | 27.78187 | 36.54842 | 37.03368 | 37.55411 | 36.40533 | 39.15150 | 39.00350 | 38.37263 | 39.24687 |
| SD | 2.727166 | 2.282494 | 2.11256 | 2.244715 | 3.435046 | 3.317604 | 3.134033 | 3.077619 | 2.638381 | 2.666798 | 3.492311 | 2.83331 |
| STS | ||||||||||||
| Mean | 27.16650 | 28.05842 | 28.45722 | 27.29277 | 34.12555 | 34.68647 | 35.09666 | 35.03933 | 39.43842 | 39.09388 | 38.90117 | 38.96125 |
| SD | 4.426094 | 4.27176 | 4.268998 | 8.105666 | 7.202044 | 6.098916 | 6.249233 | 6.065972 | 5.380239 | 5.272335 | 5.383479 | 5.689839 |
SR=Sentalloy round, STS=Speed tubular supercable, ICWP=Intercanine width pretreatment, ICW4=Intercanine width after 4 weeks, ICW8=Intercanine width after 8 weeks, ICW12=Intercanine width after 12 weeks, IPMWP=Interpremolar width pretreatment, IPMW4=Interpremolar width after 4 weeks, IPMW8=Interpremolar width after 8 weeks, IPMW12=Interpremolar width after 12 weeks, IMWP=Intermolar width pretreatment, IMW4=Intermolar width after 4 weeks, IMW8=Intermolar width after 8 weeks, IMW12=Intermolar width after 12 weeks, SD=Standard deviation
Table 2.
Median values
| Wire type | ICWP | ICW4 | ICW8 | ICW12 | IPMWP | IPMW4 | IPMW8 | IPMW12 | IMWP | IMW4 | IMW8 | IMW12 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SR | ||||||||||||
| Median | 26.555 | 27.270 | 27.080 | 27.055 | 36.10 | 36.91 | 37.69 | 36.27 | 39.16 | 39.27 | 38.76 | 39.435 |
| n | 20 | 20 | 19 | 16 | 19 | 19 | 17 | 15 | 20 | 20 | 19 | 16 |
| STS | ||||||||||||
| Median | 26.450 | 26.980 | 27.680 | 28.060 | 35.53 | 36.11 | 36.74 | 36.36 | 41.05 | 40.45 | 39.44 | 39.985 |
| n | 20 | 19 | 18 | 18 | 18 | 17 | 15 | 15 | 19 | 18 | 17 | 16 |
SR=Sentalloy round, STS=Speed tubular supercable, ICWP=Intercanine width pretreatment, ICW4=Intercanine width after 4 weeks, ICW8=Intercanine width after 8 weeks, ICW12=Intercanine width after 12 weeks, IPMWP=Interpremolar width pretreatment, IPMW4=Interpremolar width after 4 weeks, IPMW8=Interpremolar width after 8 weeks, IPMW12=Interpremolar width after 12 weeks, IMWP=Intermolar width pretreatment, IMW4=Intermolar width after 4 weeks, IMW8=Intermolar width after 8 weeks, IMW12=Intermolar width after 12 weeks
In SR group, a highly significant increase was seen in the intercanine width over the 12-week period (P < 0.001). The transverse expansion in the premolar and the molar regions was not statistically significant [Friedman Test: Table 3].
Table 3.
Readings recorded in Neo Sentalloy
| Intercanine width | Interpremolar width | Intermolar width | ||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Mean rank | Level of significance | Parameter | Mean rank | Level of significance | Parameter | Mean rank | Level of significance |
| ICWP | 1.59 | 0.000 | IPMWP | 1.71 | 0.018 | IMWP | 2.34 | 0.85 |
| ICW4 | 2.16 | IPMW4 | 2.29 | IMW4 | 2.53 | |||
| ICW8 | 2.84 | IPMW8 | 2.86 | IMW8 | 2.41 | |||
| ICW12 | 3.41 | IPMW12 | 3.14 | IMW12 | 2.72 | |||
ICWP=Intercanine width pretreatment, ICW4=Intercanine width after 4 weeks, ICW8=Intercanine width after 8 weeks, ICW12=Intercanine width after 12 weeks, IPMWP=Interpremolar width pretreatment, IPMW4=Interpremolar width after 4 weeks, IPMW8=Interpremolar width after 8 weeks, IPMW12=Interpremolar width after 12 weeks, IMWP=Intermolar width pretreatment, IMW4=Intermolar width after 4 weeks, IMW8=Intermolar width after 8 weeks, IMW12=Intermolar width after 12 weeks
In the second group (STS cable), a significant increase in the intercanine and the interpremolar widths (P ≤ 0.001) was recorded, while the intermolar width increased, which was insignificant [Table 4]. Although the wires did demonstrate transverse expansion individually, when the two groups were compared using the Mann–Whitney test, there was no significant variation among two wires in relation to the expansion achieved.
Table 4.
Readings recorded in Speed tubular supercable
| Intercanine width | Interpremolar width | Intermolar width | ||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Mean rank | Level of significance | Parameter | Mean rank | Level of significance | Parameter | Mean rank | Level of significance |
| ICWP | 1.22 | 0.000 | IPMWP | 1.57 | 0.001 | IMWP | 2.81 | 0.707 |
| ICW4 | 2.22 | IPMW4 | 2.21 | IMW4 | 2.47 | |||
| ICW8 | 2.94 | IPMW8 | 2.89 | IMW8 | 2.34 | |||
| ICW12 | 3.61 | IPMW12 | 3.32 | IMW12 | 2.38 | |||
ICWP=Intercanine width pretreatment, ICW4=Intercanine width after 4 weeks, ICW8=Intercanine width after 8 weeks, ICW12=Intercanine width after 12 weeks, IPMWP=Interpremolar width pretreatment, IPMW4=Interpremolar width after 4 weeks, IPMW8=Interpremolar width after 8 weeks, IPMW12=Interpremolar width after 12 weeks, IMWP=Intermolar width pretreatment, IMW4=Intermolar width after 4 weeks, IMW8=Intermolar width after 8 weeks, IMW12=Intermolar width after 12 weeks
DISCUSSION
It has been shown that archwires that give light continuous forces over long areas are most effectual in orthodontics.[7] To decrease the load deflection ratio, many attempts were made which lead to the introduction of multistranded steel wires such as superelastic or austenitic active NiTi wires, true shape memory or martensitic active wires, and nonsuperelastic or martensitic stabilized NiTi wires for initial alignment. Studies did not reveal any significant benefit of these wires but showed multiple advantages such as increased flexibility and a reduced load deflection rate.[8,9,10] Berger used a supercable, a seven-stranded round coaxial superelastic NiTi archwire and found this wire exerts only 36%–70% of the force of solid NiTi wires.[5]
In our study, we noticed that with time, there was an increase in intertooth distance, but the variation among the groups was statistically insignificant. Our findings are similar to Biju Sebastian et al., who found a significant difference (P < 0.05) in mean tooth movement between the coaxial superelastic NiTi wire and single-stranded superelastic NiTi in lessening lower anterior crowding.[3]
Serafim et al. and Mahmoudzadeh et al. compared the time required to relieve lower anterior crowding using two types of archwires, conventional NiTi and conventional and NiTi heat-activated wires. They found that heat-activated wires relieved crowding in significantly less time than the conventional one.[11,12]
Pandis et al. did not notice any difference in lessening of lower anterior crowding with copper-NiTi and superelastic NiTi wires.[8] Evans et al. also did not observe any significant variation in alignment capability of medium force active martensitic rectangular NiTi wire, multistranded stainless steel wire, and graded force active martensitic NiTi wire.[13] West et al. after comparing superelastic NiTi and multistranded stainless steel found a significantly better alignment with the former one.[14] Jones et al. found a superior mean enhancement in incisal alignment with superelastic NiTi than coaxial stainless steel one.[15]
Thus, all the studies including ours support the view that lower anterior alignment is superior and quicker with coaxial tubular superelastic NiTi archwire than single-stranded wire. The main advantage of the former archwire is better engagement into the bracket, and furthermore, it engages a fairly large archwire with low-force delivery.
LIMITATIONS
The limitation of the study is smaller sample size.
CONCLUSION
Coaxial tubular superelastic NiTi wires showed significant effectiveness than single-stranded NiTi in reducing lower anterior crowding after 4, 8, and 12 weeks. The obtained knowledge regarding the preference of archwire can be utilized for better orthodontic treatment.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Consolaro A, Cardoso MA. Mandibular anterior crowding: Normal or pathological? Dental Press J Orthod. 2018;23:30–6. doi: 10.1590/2177-6709.23.2.030-036.oin. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Aydın B, Şenışık NE, Koşkan Ö. Evaluation of the alignment efficiency of nickel-titanium and copper-nickel-titanium archwires in patients undergoing orthodontic treatment over a 12-week period: A single-center, randomized controlled clinical trial. Korean J Orthod. 2018;48:153–62. doi: 10.4041/kjod.2018.48.3.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sebastian B, Abraham M. Alignment efficiency of superelastic coaxial nickel-titanium. J Community Med Health Educ. 2016;6:432. [Google Scholar]
- 4.Fang CY, Tsai YY, Yu JH. Improved superelastic NiTi wire for the treatment of adult skeletal class III malocclusion in a surgery-first case. Int J Exp Dent Sci. 2016;5:133–8. [Google Scholar]
- 5.Al-Shahrani I. Study cast measurements in the assessment of incisor crowding among patients attending dental clinics in Abha city, Saudi Arabia. J Dent Res Rev. 2016;3:5–7. [Google Scholar]
- 6.Little RM. The irregularity index: A quantitative score of mandibular anterior alignment. Am J Orthod. 1975;68:554–63. doi: 10.1016/0002-9416(75)90086-x. [DOI] [PubMed] [Google Scholar]
- 7.Dalstra M, Melsen B. Does the transition temperature of Cu-NiTi archwires affect the amount of tooth movement during alignment? Orthod Craniofac Res. 2004;7:21–5. doi: 10.1046/j.1601-6335.2003.00275.x. [DOI] [PubMed] [Google Scholar]
- 8.Pandis N, Polychronopoulou A, Eliades T. Alleviation of mandibular anterior crowding with copper-nickel-titanium vs. nickel-titanium wires: A double-blind randomized control trial. Am J Orthod Dentofacial Orthop. 2009;136:152–e1-7.. doi: 10.1016/j.ajodo.2009.03.030. [DOI] [PubMed] [Google Scholar]
- 9.Ong E, Ho C, Miles P. Alignment efficiency and discomfort of three orthodontic archwire sequences: A randomized clinical trial. J Orthod. 2011;38:32–9. doi: 10.1179/14653121141218. [DOI] [PubMed] [Google Scholar]
- 10.Kusy RP, Dilley GJ. Elastic modulus of a triple-stranded stainless steel arch wire via three – And four-point bending. J Dent Res. 1984;63:1232–40. doi: 10.1177/00220345840630101401. [DOI] [PubMed] [Google Scholar]
- 11.Serafim CM, Gurgel Jde A, Tiago CM, Tavarez RR, Maia Filho EM. Clinical efficiency of two sequences of orthodontic wires to correct crowding of the lower anterior teeth. ScientificWorldJournal. 2015;2015:690280. doi: 10.1155/2015/690280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mahmoudzadeh M, Farhadian M, Alijani S, Azizi F. Clinical comparison of two initial arch wires (A-NiTi and heat activated NiTi) for amount of tooth alignment and perception of pain: A randomized clinical trial. Int Orthod. 2018;16:60–72. doi: 10.1016/j.ortho.2018.01.007. [DOI] [PubMed] [Google Scholar]
- 13.Evans TJ, Jones ML, Newcombe RG. Clinical comparison and performance perspective of three aligning arch wires. Am J Orthod Dentofacial Orthop. 1998;114:32–9. doi: 10.1016/s0889-5406(98)70234-3. [DOI] [PubMed] [Google Scholar]
- 14.West AE, Jones ML, Newcombe RG. Multiflex versus superelastic: A randomized clinical trial of the tooth alignment ability of initial arch wires. Am J Orthod Dentofacial Orthop. 1995;108:464–71. doi: 10.1016/s0889-5406(95)70046-3. [DOI] [PubMed] [Google Scholar]
- 15.Jones ML, Staniford H, Chan C. Comparison of superelastic NiTi and multistranded stainless steel wires in initial alignment. J Clin Orthod. 1990;24:611–3. [PubMed] [Google Scholar]