

Abstract
The disproportionate placement of racial minorities and males into special education for learning disabilities (LDs) raises concerns that classifications occur inaccurately or inequitably. This study uses data from the Education Longitudinal Survey of 2002 to investigate the social etiology of LD classifications that persist into adolescence. Findings suggest the overclassification of racial minorities is largely consistent with (clinically relevant) differences in educational performance. Classifications may occur inconsistently or subjectively, with clinically irrelevant qualities like school characteristics and linguistic- immigration history independently predictive of disability classification. Finally, classifications may be partially biased, with male overclassification largely unexplained by this study’s measures and racial minorities’ risk of classification increased in schools with fewer minorities (the latter not statistically significant).
Keywords: Educational stratification, health disparities, sociology of diagnosis, school context, race, disabilities, gender
Introduction
Around 13% of U.S. youth aged 6 to 17 are classified with disability (Blackorby et al. 2010). Learning disabilities (LDs), the most common federal disability category, comprise around half of the U.S. special education population (Spellings, Knudsen, and Guard 2007), with the other half comprised by 12 different disability categories. LDs broadly describe youth with achievement levels lower than expected given their average or high IQ, including disorders like dyslexia, dyscalculia, and dysgraphia (i.e., problems, respectively, with reading, math, and writing) but not including Down syndrome, attention deficit hyperactivity disorder, or autism. Youth with low IQ, formerly “mentally retarded” and now described as “intellectually disabled” in the United States, are also categorized separately from youth with LDs (U.S. Government Printing Office 2010). The disproportionate overclassification of racial minorities and males with LDs has been a dominant focus for special education researchers but understudied by sociologists of education and health.
Categories and classifications can enable efficient responses to diversity and facilitate extra supports (Kroska and Harkness 2006). Labeling theory, used to explain the experiences of mentally ill, criminal, and homosexual persons, emphasizes the possibility that classifications actually facilitate stigma and stratification by altering how classified persons are perceived by others and themselves (Scheff 1966). Labeling theory is founded in the premise that determinations of deviance vary across space and time (Maynard 2005), with the socially undesirable at heightened risk of classification (Becker 1963). Special education is intended to enable success, particularly for students with more mild disabilities like LDs, yet disproportionality is perceived as problematic, for one because it is not clear that special education improves youths’ outcomes (Morgan et al. 2010; Shifrer 2013; Shifrer, Callahan, and Muller 2013). With racial minorities’ long history of stratification and males’ increasing disadvantage in educational realms (DiPrete and Buchmann 2013; Noguera 2008), special education may actually reproduce disadvantage.
Disproportionality is also problematized because it may represent inaccurate or inequitable classifications (Skiba et al. 2008). LDs share the invisibility of many other conditions included in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (Kokanovic, Bendelow, and Philip 2013). For instance, whereas Down syndrome is associated with clear physical indicators (Korenberg et al. 1990), LDs are typically not marked by notable mannerisms (Coughlin 1997). In addition to a lack of clear physical indicators, there are no objective biological indicators for LDs. Neurological difference is inferred on the basis of subjective and socially rooted criteria such as academic achievement and behaviors (Carrier 1983). The subjectivity and inconsistency of LD diagnostic processes may provide fertile ground for the biased classification processes predicted by labeling theory (Ferri and Connor 2005).
With an emphasis on the potential contributions of bias, policy reform aimed at reducing disproportionality largely focuses on cultural sensitivity training for educators (McDermott, Goldman, and Varenne 2006). Similarly, physicians are trained in “cultural competency” in attempts to reduce disparities in other health conditions (Metzl and Hansen 2014). Metzl and Hansen (2014) argue, however, that health disparities persist in part because of the lack of attention to structural forces that shape diverse persons’ health outcomes, such as inequities in neighborhoods and homes (Pampel 2009). In 2015 the Medical College Admission Test emphasized social factors related to health for the first time, with a main goal of producing physicians who recognize structural determinants of health and health disparities (Heller 2012). For LDs, youth are typically referred for evaluation by their teachers and diagnosed by educational psychologists rather than physicians, but it may be a similar shift in perspective is required to effectively understand and address disproportionality in special education.
The study of the social etiology of disability classifications that persist into adolescence has faced substantial data limitations. Before 2010 studies on youth with an LD classification relied on aggregate level data, small sample sizes, or data without unclassified peers as a base of comparison (Sullivan and Artiles 2011). Moreover, most previous studies did not account for confounders between race, gender, and the LD classification (e.g., Margai and Henry 2003; Sullivan and Artiles 2011). This study benefits from access to a large national dataset with rich measures describing students and their schools, the Education Longitudinal Survey of 2002. Whereas this study, for instance, uses a measure of the official school disability classification, previous studies relied on perceptions of disability or even diagnosed youth through a survey (e.g., Sprung et al. 2009). Other more recent studies using similarly rich student level data have focused on children (e.g., Hibel, Farkas, and Morgan 2010; Morgan et al. 2015; Samson and Lesaux 2009), facilitating the use of measures of achievement that clearly precede disability classification. To date, no datasets exist that longitudinally track youth from their early school years, when most classifications occur, into adolescence. For these reasons, this study’s focus on adolescents necessitates the use of data with cross-sectional measures of achievement and disability status, preventing causal conclusions. Confidence in results is bolstered by indications that special education does not substantially alter students’ achievement trajectories (Morgan et al. 2010; Shifrer 2016; Shifrer, Callahan, and Muller 2013). Ultimately, with nearly half of kindergarteners placed into special education declassified (i.e., “cured”) by the third grade (Blackorby et al. 2010), this study initiates an important research focus on disability classifications that persist into adolescence.
Misalignment between the category and process of LD classification
Kokanovic, Bendelow, and Philip (2013) distinguish between the category and process of diagnosis. The LD category is defined in the American Psychiatric Association’s DSM, a volume with substantial control over the diagnosis of psychiatric disorders (Kokanovic, Bendelow, and Philip 2013). With the publication of the DSM-III in 1980, there was a shift from complex nuanced diagnoses to categorical, symptom-based diagnoses, which essentially represented a shift from social to biological explanations (Kokanovic, Bendelow, and Philip 2013). Similarly, the U.S. Department of Education specifies the LD category should not be used for learning difficulties primarily resulting from “... cultural factors... economic disadvantage. . . or Limited English proficiency” (U.S. Department of Education 2016). In these ways, LDs are defined as a category for learning difficulties rooted in individual neurological difference rather than group or social difference. Researchers similarly describe how LDs, dominantly perceived as stable, internal, and uncontrollable conditions, are framed through the “personal tragedy” model of disability (Clark 1997; Ho 2004).
With LD diagnostic practices contextually variable within both the United States and Europe (Gebhardt et al. 2013; Lester and Kelman 1997), the qualities of students diagnosed with an LD are inconsistent (Singer et al. 1989) and not easily distinguished from those of other low achievers without an LD classification (Fletcher, Denton, and Francis 2005). Response to Intervention was not federally endorsed until 2004 (Bradley, Danielson, and Doolittle 2007), leaving adolescents in this study likely to have been classified with an LD through one of three diagnostic methods, as discussed in Fletcher, Denton, and Francis (2005). (Importantly, Response to Intervention, based in cultural sensitive approaches, has not proven to effectively reduce racial disproportionality [McKinney, Bartholomew, and Gray 2010].) In the ability-achievement discrepancy model, youth are classified with an LD for achievement levels lower than expected given their IQ. In the intraindividual discrepancy model, an uneven cognitive profile, strengths in some areas and weaknesses in others, suggests an LD. The low-achievement model legitimized the classification of any student performing below a certain benchmark. Although none of these diagnostic models involves neurological indicators, LDs are still propagated as biologically rooted conditions (Carrier 1983). The diagnostic criteria for many disorders in the DSM are criticized as socially rooted and subjective (Pickersgill 2012). Although youth classified with LDs may have real neurological or biological distinctions (Mathis et al. 2015), diagnoses occur without explicit confirmation of such difference. Considering the LD category and LD classification process in concert, this study describes characteristics potentially medically linked to neurological difference as clinically relevant. Clinically irrelevant factors may become salient in classification decisions that are biased, inconsistent, or subjective.
Although typically based on results from bivariate or aggregate level analyses (Shifrer, Muller, and Callahan 2011), racial bias is a dominant explanation for the disproportionate classification of racial minorities with LDs (Harry and Klingner 2006). Similar to labeling theory’s predictions that the socially powerless are more susceptible to labels of deviance (Becker 1963), schools are portrayed as using special education classifications to maintain racial segregation (Eitle 2002). With males increasingly disadvantaged within educational realms since the 1970s (DiPrete and Buchmann 2013), some researchers also attribute male disproportionality to gender bias (Oswald, Best, and Coutinho 2006). If classification processes are biased, racial minorities and males should remain more likely to carry an LD classification even when compared with otherwise similar white or female adolescents. Moreover, racially biased classification processes should be more evident in more diverse schools, in which teachers can actually “whiten” their classrooms by placing racial minorities into special education (Ferri and Connor 2006). Racial minority youth may be more likely to be perceived as aberrant in schools with more white children (McKown and Weinstein 2008; Oswald et al. 2001). Racial bias in teachers’ suspicions of disability (Fish 2017) may be enhanced when racial minorities are in a context in which they are more distinctive, such that racial minorities’ risk of classification would be higher in schools serving a lower proportion of racial minorities.
Clinically irrelevant correlates of race and gender
Disproportionality may reflect inconsistent or subjective rather than biased LD classification processes. Racial minorities attend systematically different schools, and classification processes may be inconsistent across schools because of vague federal classification guidelines or variation in resources (Bradley, Danielson, and Doolittle 2007). Racial dispropor- tionality may partially result from the disproportionate classification of linguistic minorities. Although linguistic status is specifically cited as a clinically irrelevant factor in LD classifications, linguistic minorities are disproportionately classified with LDs in some contexts (Sullivan 2011). Achievement standards may be subjectively defined on the basis of English proficient youth, such that learning struggles related to limited English proficiency are misrecognized as neurological difference (Klingner, Artiles, and Barletta 2006).
Disproportionality may also be due to classifications subjectively determined by the qualities of peers. In other words, referral and diagnosis decisions may depend on educators’ perceptions of normative achievement and learning style, with educators’ perceptions a function of the average qualities of students in the school. Hibel, Farkas, and Morgan (2010) find otherwise similar fifth graders are more likely to be classified with an LD in higher-achieving schools, suggesting a higher bar for normative achievement in such schools. If clinically irrelevant correlates of race and gender, including linguistic- immigration history and school characteristics, independently predict adolescents’ likelihood of carrying an LD classification, classification processes may be inconsistent and subjective.
Clinically relevant correlates of race and gender
If disproportionality is explained by clinically relevant correlates of race and gender, that is, characteristics potentially medically linked to neurological difference, disproportionality may reflect accurate classifications. Educational performance is clinically relevant for LD classifications because it is an explicit criterion across all three diagnostic models discussed in the previous section and at least partially reflects neurological difference (Fletcher, Denton, and Francis 2005). The discussion expands on the complication of educational performance also varying as a function of social differences, like social class and linguistic status. Racial minorities and males academically underperform relative to counterparts (Buchmann and DiPrete 2006), such that their disproportionate classification with LDs may be consistent with their lower levels of educational performance. Low socioeconomic status (SES) may be clinically relevant for LD classifications because of evidence that poverty can alter neurology (Shonkoff and Phillips 2000). Poorer academic outcomes generally, and LDs specifically, are linked to preterm births and low birth weight (Lin and Liu 2009), events more prevalent among youth with low SES (Conley and Bennett 2000). Although achievement differences are not considered, previous studies find differences in SES are implicated in racial disproportionality among U.S. and British youth (Shifrer, Muller, and Callahan 2011; Strand and Lindsay 2009).
Purpose of study
If classification processes are biased, racial minorities should remain more likely than white youth to be classified with an LD net of all other measures. Biased classifications are also a possibility if racial minorities who attend a school with few minorities have a higher odds of classification than racial minorities who attend a school with more minorities, net of other student level differences. If clinically irrelevant correlates of race and gender, such as linguistic-immigration history or the qualities of students’ schools, independently predict adolescents’ likelihood of LD classification, classifications may occur inconsistently and subjectively. If the overclassification of racial minorities and males is explained by clinically relevant correlates of race and gender, such as educational performance or social class, disproportionality may represent accurate rather than biased classifications.
Methods
The National Center for Education Statistics (NCES) first surveyed 16,373 10th graders enrolled in approximately 750 schools in 2002 for the Education Longitudinal Survey of 2002. This study uses data from the base year surveys of adolescents and their parents as well as administrative data on adolescents’ academic achievement and the characteristics of their high schools. After excluding adolescents classified with a disability other than an LD (n = 300), who attended a school that did not report any sampled students’ disability statuses (n = 4,210), or who did not have a school identification number (n = 110), the analytic sample includes approximately 11,670 adolescents in 546 schools. (NCES requires unweighted sample frequencies be rounded to the nearest 10.) Consistent with national benchmarks (Spellings, Knudsen, and Guard 2007), about 6% of the adolescents in the analytic sample (n = 690) are classified by their school with an LD. Table 1 provides descriptive statistics on all variables used in this study. Missing values on all independent variables were addressed through multiple imputation by the multiple imputation by chained equations (MICE) system of chained equations (White, Royston, and Wood 2011).
Table 1.
Means and proportions showing correlates of LD classifications, race, and gender.
| Females |
Males |
|||||||
|---|---|---|---|---|---|---|---|---|
| No disability classification | LD classification | White, non-Hispanic |
Black, non-Hispanic |
Hispanic | White, non-Hispanic |
Black, non-Hispanic |
Hispanic | |
| Proportion with LD classification | - | - | 0.04 | 0.05 | 0.05 | 0.08 | 0.11 | 0.10 |
| Relative to white females | - | - | - | + | + | *** | *** | *** |
| Relative to white males | - | - | *** | * | ** | - | * | ** |
| Socioeconomic status | 0.01 | −0.22 | 0.14 | −0.28 | −0.48 | 0.15 | −0.20 | −0.43 |
| (0.73) | (0.65) | (0.70) | (0.66) | (0.70) | (0.68) | (0.67) | (0.70) | |
| Linguistic-immigration history | ||||||||
| Not a native English speaker | 0.13 | 0.15 | 0.03 | 0.04 | 0.57 | 0.02 | 0.07 | 0.48 |
| Degree to which lacks English | 0.23 | (1.43) | (0.36) | (0.72) | (2.00) | (0.50) | (0.71) | (1.81) |
| proficiency | 0.08 | 0.13 | 0.05 | 0.08 | 0.18 | 0.06 | 0.07 | 0.15 |
| Ever been in an English as a Second | ||||||||
| Language program | ||||||||
| Started school in United States: | ||||||||
| In kindergarten | 0.95 | 0.97 | 0.98 | 0.96 | 0.80 | 0.99 | 0.96 | 0.85 |
| Between 1st and 2nd grades | 0.01 | 0.01 | 0.00 | 0.01 | 0.04 | 0.00 | 0.01 | 0.03 |
| Between 3rd and 5th grades | 0.01 | 0.01 | 0.00 | 0.01 | 0.05 | 0.00 | 0.01 | 0.05 |
| Between 6th and 10th grades | 0.03 | 0.01 | 0.01 | 0.03 | 0.12 | 0.01 | 0.02 | 0.08 |
| Educational performance | ||||||||
| Average 10th grade test score | 50.98 | 39.85 | 52.80 | 44.18 | 45.11 | 52.67 | 44.23 | 45.28 |
| (51.22) | (39.74) | (52.98) | (44.78) | (46.16) | (52.68) | (44.73) | (45.84) | |
| School characteristics | ||||||||
| Percent students eligible for free | 21.28 | 21.17 | 15.51 | 33.33 | 34.34 | 15.60 | 35.12 | 32.63 |
| lunch program | (21.62) | (22.50) | (16.59) | (32.44) | (32.84) | (16.45) | (33.18) | (31.94) |
| Percent students racial minorities | 32.52 | 32.10 | 18.87 | 57.94 | 62.13 | 19.19 | 58.92 | 60.10 |
| (33.34) | (33.08) | (19.63) | (56.65) | (58.60) | (19.70) | (56.25) | (57.28) | |
| School type | ||||||||
| Public | 0.94 | 0.99 | 0.93 | 0.98 | 0.97 | 0.93 | 0.98 | 0.97 |
| Catholic | 0.04 | 0.01 | 0.04 | 0.02 | 0.02 | 0.04 | 0.01 | 0.02 |
| Other private | 0.02 | 0.01 | 0.02 | 0.01 | 0.00 | 0.02 | 0.01 | 0.00 |
| School region | ||||||||
| Northeast | 0.19 | 0.22 | 0.20 | 0.17 | 0.15 | 0.21 | 0.18 | 0.17 |
| Midwest | 0.26 | 0.25 | 0.32 | 0.17 | 0.15 | 0.32 | 0.15 | 0.13 |
| South | 0.34 | 0.35 | 0.33 | 0.60 | 0.29 | 0.31 | 0.59 | 0.27 |
| West | 0.20 | 0.19 | 0.15 | 0.05 | 0.40 | 0.16 | 0.08 | 0.43 |
| School urbanicity | ||||||||
| Suburban | 0.51 | 0.48 | 0.54 | 0.44 | 0.41 | 0.53 | 0.43 | 0.45 |
| Urban | 0.27 | 0.26 | 0.18 | 0.45 | 0.49 | 0.19 | 0.45 | 0.45 |
| Rural | 0.22 | 0.27 | 0.28 | 0.11 | 0.10 | 0.28 | 0.12 | 0.10 |
| Adolescents (n) | 10,990 | 690 | 3,460 | 740 | 860 | 3,370 | 710 | 850 |
Note. Standard deviations in parentheses below means.
p < .10,
p < .05,
p < .01,
p < .001 (two-tailed test).
Dependent variables
Schools reported which sampled students were in receipt of special education services during the 10th grade and their qualifying federal disability category. This study focuses on students receiving special education services through the LD category that encompasses conditions like dyslexia, dyscalculia, dysgraphia, and language disorders (American Psychiatric Association 2000). Students with intellectual disabilities, attention deficit hyperactivity disorder, Down syndrome, and autism are excluded from this study, because they qualify for special education services under disability categories other than the LD category (U.S. Department of Education 2004). For reasons that remain unclear, schools did not report the disability status of about 8,210 students. Aggregation to the school level demonstrated that disability status reports were available for no sampled students in 202 schools, some sampled students in 212 schools, and all sampled students in 334 schools. Comparable mean proportions of adolescents were designated with an LD (and with any disability) across the two groups of schools reporting the disability statuses of all and only some of their sampled students, with the average proportion of students designated with disability actually slightly higher in the latter group of schools (see Supplementary Table 1). For this reason, and after consulting with NCES, the 4,000 adolescents without a disability status, who attended schools that reported the disability status of some sampled students, are considered to not be classified with disability. This study only excludes the 4,210 adolescents in schools that reported the disability statuses of no sampled students.
Adolescents excluded from the analytic sample were more likely to be racial minorities and linguistic minorities and had higher average SES (see Supplementary Table 1). There were no consistent differences in educational performance between included and excluded adolescents. Excluded adolescents were more likely than included adolescents to attend Catholic or other private schools. The schools of excluded adolescents also served more racial minorities and were less likely to be in the Midwest or rural areas. The discussion describes additional sensitivity analyses. Ultimately, this study’s analytic sample cannot be described as nationally representative because of distinctions between excluded and included adolescents. Nonetheless, with a large and diverse sample, this study is still an important contribution because of the unavailability of another dataset with measures comparable to those in the Education Longitudinal Survey of 2002.
Independent variables
Because initial assignations of the LD classification likely occurred before the 10th grade (Blackorby et al. 2010), this study focuses on measures most likely to provide insight into adolescents’ earlier years. Adolescents reported whether they were white, non-Hispanic; black, non-Hispanic; Hispanic; or other. The SES composite summarizes parent reports of family income and parents’ occupations and educational attainment. Adolescents’ linguistic- immigration histories are measured with adolescents’ reports on their native language, participation in English as a Second Language, and 10th grade English proficiency (how well they understand spoken English and speak, read, and write English; alpha = 0.95) as well as their parent’s report on the grade level they began school in the United States.
Adolescents’ educational performance is measured by average scores (alpha = 0.75) on the standardized math and reading tests administered by NCES. This average test score may reflect the courses students have the opportunity to complete or may be culturally biased measures of academic ability (McKown and Weinstein 2008). It is important to keep in mind educators rely on similarly culturally biased measures of educational performance to refer students for special education evaluation. Course levels and course grades may be more likely than test scores to have inconsistent meanings across contexts (Willingham, Pollack, and Lewis 2002), and course grades also reflect students’ level of coursework. Because test scores may be less influenced by stratification within schools (particularly stratification produced by the LD classification) than course levels and grades, the analyses presented here focus exclusively on students’ average test scores. Moreover, results from sensitivity analyses including measures describing students’ course-taking and grade point average were substantively identical, and the magnitude of the association between students’ odds of LD classification and average test score dwarfed the associations with course-taking and grades. As already mentioned, this study is limited by the lack of measures of academic achievement that preceded the disability classification. Confidence in results is bolstered by findings from studies that indicate special education does not alter students’ achievement trajectories (Morgan et al. 2010; Shifrer 2016; Shifrer, Callahan, and Muller 2013). Until better data sources are available, this study contributes to laying the foundation for understanding the social origins of disability classifications that persist into adolescence.
Adolescents’ schools are described by the proportion of students eligible for free lunch, proportion of students who are racial minorities, type (public, Catholic, other), region, and urbanicity. Quartile measures of school poverty capture a nonlinear association with the LD classification. Many of the adolescents in this study likely received the LD classification before high school, but most attend high schools evocative of their earlier schools and general social status (Alexander, Entwisle, and Dauber 1996).
Analytic plan
Descriptive statistics showing relationships between the LD classification, adolescents’ race and gender, and other qualities of adolescents and their schools establish disproportion- ality and facilitate interpretation of multivariate analyses. Random effects logistic regression models are used to predict adolescents’ odds of carrying an LD classification as a 10th grader. Random effects models adjust standard errors to account for the clustering of adolescents in schools; including controls for school selection mechanisms increases the likelihood of meeting these models’ assumptions (Clarke et al. 2010). The first model reestablishes baseline race and gender differences in adolescents’ odds of classification; interactions between gender and race were not statistically significant. All measures are included in the second model to understand whether classification processes may be biased, that is, whether race and gender differences persist net of all controls. This second model also investigates potential inconsistencies or subjectivities in classifications by establishing whether clinically irrelevant student and school characteristics independently predict odds of classification. Results from models 1 and 2 are also presented as marginal effects because of issues of scaling that occur when comparing logit coefficients across groups (Breen, Holm, and Karlson 2014). The third model examines potential bias in classifications by interacting student race and proportion of students at the school who are racial minorities. To facilitate interpretation, tabular results are presented as log odds and the interaction is also presented graphically. The graphical representation of the interaction also addressees concerns that the nonlinearity of predicted probabilities can result in group differences in how the probabilities vary across the distribution of the predictor variable of interest (Breen, Holm, and Karlson 2014).
Finally, this study uses a decomposition method developed by Kohler, Karlson, and Holm (2011) to more clearly understand the extent to which racial and gender dispro- portionality relate to differences in clinically relevant correlates (educational performance, SES) and to differences in clinically irrelevant correlates (linguistic-immigration history, school characteristics). Statisticians increasingly criticize the comparison of coefficients across logits as a means of exploring mediation (Mood 2010). In addition to addressing these issues of scaling (Kohler, Karlson, and Holm 2011), this method determines the degree to which each race and gender correlate mediates the estimated effect of adolescents’ race-gender on odds of LD classification, net of other correlates. By producing percentages, this method more clearly summarizes the magnitude of associations than standard regression techniques. It is relatively unproblematic to assume race and gender precede SES, linguistic-immigration history, educational performance, and LD classification. Similarly, it is unproblematic to assume SES and linguistic-immigration history precede LD classification. Racial and gender gaps in performance are evident at kindergarten and remain quite stable throughout children’s school careers (Cheadle 2008), and the median age of special education categorization is 5 (Ong-Dean 2009). Despite this support for the assumption that students’ low educational performance precedes LD classification, this study avoids causal language (excepting references to race and gender) because the data only measure educational performance and LD classification at adolescence.
Results
Correlates of LD classifications, race, and gender
Table 1 first confirms that racial minority and male adolescents, like children, are disproportionately classified with LDs. Gender differences appear to be more marked than racial differences, with 4% to 5% of females classified in contrast to 8% to 11% of males and the differences between white males and females of each race statistically significant. In all, racial disproportionality is most evident among males, with black and Hispanic males classified at significantly higher rates than white males, but differences between white females and minority females only marginally significant. The first two columns of Table 1 show adolescents classified with an LD have lower average SES, are more likely to be linguistic minorities, less likely to be recent immigrants, and exhibit lower levels of educational performance than adolescents without a disability classification. Higher proportions of classified adolescents attend schools that are public, in the Northeast, or in rural areas.
Table 1 also shows race and gender differences in the average qualities of adolescents and their schools. Racial differences in these qualities are more marked than gender differences. Black adolescents are more economically disadvantaged than white adolescents, but Hispanics are the most disadvantaged of all. Hispanic adolescents are more likely to be linguistic minorities and recent immigrants than white or black adolescents. Educational performance levels are generally highest for white adolescents and lowest for black adolescents. Racial minorities attend schools with higher proportions of students eligible for the free lunch program and racial minorities. Racial minorities are more likely than white adolescents to attend public schools and schools in urban areas. White adolescents are more likely to attend schools in the Northeast or Midwest, whereas black adolescents are particularly prevalent in the South and Hispanic adolescents in the West. Disproportionality may be attributable to gender and particularly racial differences in these qualities.
Independent predictors of the LD classification
Model 1 in Table 2 uses results from logistic regression models to first establish the same gender and race differences in LD classification explored with descriptive statistics in Table 1. Although Table 2 provides odds ratios to benchmark with previous studies, discussion of results focus on marginal effects as these predicted values better account for issues of scaling that occur when using logistic regression modeling to examine group differences (Breen, Holm, and Karlson 2014). Model 1 shows the predicted probabilities of classification with an LD are 33 percentage points higher for black adolescents and 40 percentage points higher for Hispanic adolescents than they are for white adolescents, net of gender (model 1). The predicted probability of LD classification, controlling for race, is 79 percentage points higher for males than for females (Table 2, model 1).
Table 2.
Random effects logistic regression models predicting adolescent classified with a LD.
| Model 1: unadjusted race and gender differences |
Model 2: adjusted race and gender differences |
Model 3: race interacted |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| dy/dx | (SE) | Exp(B) | (SE) | dy/dx | (SE) | Exp(B) | (SE) | B | (SE) | ||||||
| Race: | |||||||||||||||
| White, non-Hispanic (ref) | |||||||||||||||
| Black, non-Hispanic | 0.33 | ** | (0.12) | 1.39 | *** | (0.17) | −0.50 | ** | (0.15) | 0.59 | ** | (0.09) | −0.17 | (0.29) | |
| Hispanic | 0.40 | *** | (0.12) | 1.49 | ** | (0.17) | −0.19 | (0.16) | 0.85 | (0.14) | 0.10 | (0.27) | |||
| Other race | −0.16 | (0.13) | 0.85 | (0.11) | −0.25 | (0.16) | 0.79 | (0.13) | −0.19 | (0.25) | |||||
| Male | 0.79 | *** | (0.09) | 2.21 | ** | (0.19) | 0.72 | *** | (0.09) | 2.08 | *** | (0.20) | 0.73 | *** | (0.10) |
| SES | 0.00 | (0.08) | 1.01 | (0.08) | 0.00 | (0.08) | |||||||||
| Linguistic-immigration history | |||||||||||||||
| Not a native English speaker | −0.12 | (0.17) | 0.81 | (0.15) | −0.20 | (0.19) | |||||||||
| Degree lacking English proficiency | 0.05 | (0.05) | 1.06 | (0.05) | 0.06 | (0.05) | |||||||||
| Ever in an English as a Second Language program | 0.23 | (0.14) | 1.17 | (0.19) | 0.15 | (0.16) | |||||||||
| Started school in United States | |||||||||||||||
| In kindergarten (ref) | |||||||||||||||
| Between 1st and 2nd grades | −0.42 | (0.46) | 0.79 | (0.39) | −0.24 | (0.50) | |||||||||
| Between 3rd and 5th grades | −1.52 | ** | (0.50) | 0.25 | ** | (0.13) | −1.40 | ** | (0.53) | ||||||
| Between 6th and 10th grades | −2.32 | *** | (0.42) | 0.08 | ** | (0.06) | −2.52 | ** | (0.69) | ||||||
| Educational performance | |||||||||||||||
| Average 10th grade test score | −0.19 | *** | (0.01) | 0.83 | *** | (0.01) | −0.19 | *** | (0.01) | ||||||
| School characteristic | |||||||||||||||
| School type | |||||||||||||||
| Public (ref) | |||||||||||||||
| Catholic | 0.59 | + | (0.16) | 0.59 | * | (0.16) | −0.57 | * | (0.27) | ||||||
| Private | 0.39 | * | (0.15) | 0.39 | * | (0.15) | −0.98 | * | (0.38) | ||||||
| School region | |||||||||||||||
| Northeast (ref) | |||||||||||||||
| Midwest | 0.75 | + | (0.12) | 0.75 | + | (0.12) | −0.29 | + | (0.16) | ||||||
| South | 0.75 | + | (0.12) | 0.75 | + | (0.12) | −0.34 | * | (0.16) | ||||||
| West | 0.56 | ** | (0.11) | 0.56 | ** | (0.11) | −0.61 | ** | (0.20) | ||||||
| School urbanicity | |||||||||||||||
| Suburban (ref) | |||||||||||||||
| Rural | 1.29 | + | (0.18) | 1.29 | + | (0.18) | 0.26 | + | (0.14) | ||||||
| Urban | 1.08 | (0.16) | 1.08 | (0.16) | 0.08 | (0.15) | |||||||||
| Percent students racial minorities | 1.00 | (0.00) | 1.00 | (0.00) | 0.00 | (0.00) | |||||||||
| Percent students eligible for free lunch program: | |||||||||||||||
| Quartile 1 (least poverty) (ref) | |||||||||||||||
| Quartile 2 | 0.86 | (0.14) | 0.86 | (0.14) | −0.16 | (0.17) | |||||||||
| Quartile 3 | 0.69 | * | (0.12) | 0.69 | * | (0.12) | −0.40 | * | (0.17) | ||||||
| Quartile 4 (most poverty) | 0.54 | ** | (0.11) | 0.54 | ** | (0.11) | −0.61 | ** | (0.21) | ||||||
| Interactions | |||||||||||||||
| Black × proportion racial minority | −0.01 | (0.01) | |||||||||||||
| Hispanic × proportion racial minority | −0.01 | (0.01) | |||||||||||||
| Other race × proportion racial minority | 0.00 | (0.01) | |||||||||||||
Note: These models estimated with 11,670 adolescents in 546 schools. dy/dx = marginal effects. B = log odds. Exp(B) = odds ratios.
p < .10,
p < .05,
p < .01,
p < .001 (two-tailed test).
Model 2 in Table 2, introducing controls for SES, linguistic-immigration history, educational performance, and school characteristics, shows the predicted probabilities of classification with an LD remain significantly higher for males than for females even net of all measured qualities. This may indicate gender bias contributes to male disproportionality (alternate possibilities in Discussion). In contrast, after accounting for average differences across adolescents and their schools, the odds of classification for black adolescents are lower than those for white adolescents (model 2). There is also no evidence to suggest Hispanics are overclassified with LDs relative to whites, net of these controls. These results do not support racially biased classification processes. Although the next section of results specifically narrows in on the student and school qualities that mediate the relationship between race and LD classification, these findings are consistent with other studies that find racial minorities are underclassified with disability in models that account for racial differences in social class (Shifrer, Muller, and Callahan 2011; Strand and Lindsay 2009) or racial differences in academic achievement (Hibel, Farkas, and Morgan 2010; Morgan et al. 2015).
Model 2 in Table 2 also shows which student and school qualities independently predict LD classification. Higher levels of educational performance significantly associate with much lower odds of classification with an LD (Table 2, model 2). Although data limitations prevent causal interpretations, this may indicate classification processes at least partially align with diagnostic criteria. Measures of linguistic status are not significantly associated with LD classification. The odds of classification are significantly lower for recent immigrants than for adolescents who began school in the United States in kindergarten, potentially indicating educators can more easily recognize learning struggles due to recent immigration as clinically irrelevant for disability classifications. The odds of classification are lower for adolescents in Catholic schools than those for otherwise similar adolescents in public schools. The odds of classification are lower for adolescents in schools in the western United States than they are for otherwise similar students in schools in the Northeast. The odds of classification are also lower for adolescents in the highest poverty schools. Because school characteristics are clinically irrelevant for disability classifications, school characteristics retaining a significant association with students’ odds of LD classification after controlling for student level differences may indicate inconsistent and inaccurate classification processes.
In an additional investigation of whether classifications may be racially biased, model 3 in Table 2 interacts the proportion of students at the school who are racial minorities with adolescents’ race. Although the interactions are not statistically significant, again not supporting racially biased classification processes, statistical significance may be harder to achieve because LD classifications are a relatively rare event (Xue et al. 2017) or because of complications related to interactions and logit models (UCLA Statistical Consulting Group 2017). Figure 1, using predicted probabilities to facilitate interpretation of the interactions in model 3, shows that the probability of classification remains higher for white than for racial minority adolescents regardless of the racial composition of the school. In contrast, the probabilities of classification are higher for racial minorities in schools with fewer racial minorities than they are for racial minorities in schools with more racial minorities. It is important to keep in mind that these differences were not statistically significant and that white students retain the highest rates of classification regardless of school racial composition. Nonetheless, these results could indicate racial bias in that racial minorities’ risk of disability increases in schools in which they are more distinctive, where as the predicted probability of classification for white students is relatively unaffected by their school’s racial composition.
Figure 1.
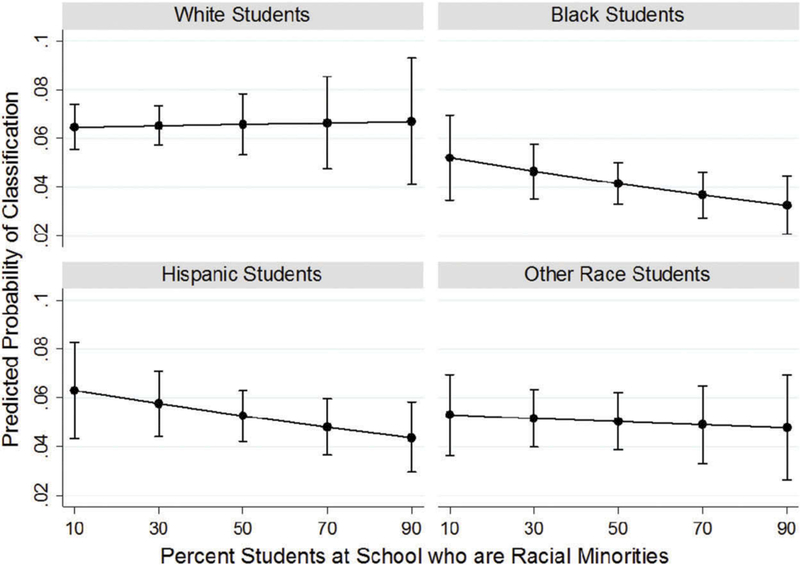
Predicted probabilities of classification with a LD depending on student race and the percent of students at school who are racial minorities.
Disentangling racial and gender disproportionality
Results from decomposition analyses in Table 3 reveal which qualities of adolescents and their schools mediate the estimated effect of race and gender on adolescents’ odds of carrying an LD classification. Because Table 2 showed white females are classified at the lowest rates and that gender differences in classification appear to be larger than race differences, these analyses contrast white males and minority females to white females and minority males to white males. In a first example, Table 3 shows that 7.0% of the estimated effect of being a white male rather than a white female on adolescents’ odds of carrying the LD classification is explained by differences in average test scores. This corresponds with the statistics in Table 1 showing that adolescents with LD classifications have lower test scores on average, and that the average test scores of white females are slightly higher than the scores of white males.
Table 3.
Percentage contribution of each correlate to the estimated effect of race and gender on adolescents’ odds of carrying LD classification.
| Correlates of Race and Gender | White male relative to a white female | Black male relative to a white male | Hispanic male relative to a white male | Black female relative to a white female | Hispanic female relative to a white female |
|---|---|---|---|---|---|
| SES | 0.0% | −0.2% | −0.3% | −0.2% | −0.3% |
| Not a native English speaker | 0.0% | −1.2% | −13.1% | −0.7% | −16.5% |
| Degree to which lacks English proficiency | 0.1% | 0.5% | 6.8% | 0.4% | 9.5% |
| Ever in an English as a Second Language program | 0.1% | 0.3% | 1.8% | 0.4% | 2.9% |
| Grade level started school in United States | 0.7% | −6.2% | −38.0% | −7.7% | −53.1% |
| Linguistic-immigration history subtotal | 1.0% | 0.7% | 8.6% | 0.9% | 12.4% |
| Average 10th grade test score | 7.0% | 226.5% | 219.7% | 216.8% | 244.6% |
| Percent students eligible for free lunch program | 0.4% | −45.7% | −47.9% | −39.9% | −56.1% |
| Percent students racial minorities | 0.0% | 1.4% | 1.7% | 1.3% | 1.9% |
| School type (public, Catholic, other private) | −0.3% | 11.8% | 12.0% | 9.9% | 14.2% |
| School region | 1.0% | −5.9% | −17.6% | −2.6% | −17.5% |
| School urbanicity | 0.2% | −1.2% | −1.6% | −0.8% | −1.0% |
| School characteristics subtotal | 1.6% | 13.3% | 13.7% | 11.2% | 16.1% |
In Table 3, negative percentages indicate that the student or school characteristic does not mediate the relationship between adolescents’ race-gender and odds of LD classification. To facilitate comparison, Table 3 sums the contributions of the various measures of linguistic-immigration history and school characteristics in separate bolded rows. It is evident that average test scores contribute much more to the estimated effect of racial minorities’ odds of LD classification than any other correlate of race-gender in this study. This is consistent with findings from studies focused on young children that achievement was more predictive of disability classification than even behaviors (Hibel, Faircloth, and Farkas 2008; Hibel, Farkas, and Morgan 2010). Percentages larger than 100% indicate an effect not only explained by measured correlates but overexplained. For instance, 226.5% of the estimated effect of being a black male rather than a white male on adolescents’ odds of LD classification is explained by, or consistent with, differences in average test scores. The pattern is similar for Hispanic males, black females, and Hispanic females. In other words, not only is the disproportionate classification of black and Hispanic males relative to white males and that of black and Hispanic females relative to white females, consistent with test score differences, but racial minorities would actually be classified at much higher rates if low achievement were as predictive of classification for minorities as it is for white students.. This finding is consistent with the reversal of the black and Hispanic coefficients between models 1 and 2 in Table 2, that is, the finding that racial minorities are underclassified with LDs after accounting for racial differences in achievement. Race-gender differences in school characteristics and linguistic-immigration histories contribute a small amount to race-gender differences in odds of classification, but gender, and particularly race, differences in educational performance, a clinically relevant of disability classification, make much more substantial contributions.
Discussion
Youth already disadvantaged in educational realms are more likely to be classified with LDs, and evidence that special education may not improve learning outcomes suggests disability classifications may only reproduce disadvantage. Efforts to reduce the disproportionate placement of racial minorities and males into special education have largely focused on reducing bias in the categorization process (Klingner et al. 2005). This study’s findings suggest the overclassification of racial minorities with LDs is largely consistent with a clinically relevant difference across racial groups, differences in educational performance. This study finds some evidence to suggest classifications occur inconsistently or subjectively, with clinically irrelevant qualities like school characteristics and linguistic- immigration history contributing in some part to adolescents’ likelihood of classification. Results may indicate biased classifications, with male overclassification with LDs largely unexplained by this study’s measured correlates. Biased classifications may also be indicated by racial minorities’ increased risk of classification in schools in which they are more distinctive, i.e., schools with fewer racial minorities—this result cannot be generalized to the national population with confidence but it is possible the result was not statistically significant because LD classifications are a relatively rare event (Xue et al. 2017) or because of complications related to interactions in logit models (UCLA Statistical Consulting Group 2017). The following paragraphs expand on these findings and discuss how policy reform aimed at reducing disproportionality should include both a focus on social inequities and classification processes, consistent with the new emphasis on training physicians in the structural determinants of health (Metzl and Hansen 2014). This study’s findings also inform understandings of the contributions of social stratification to disparities in both education and health outcomes.
Racial minorities’ lower likelihood of LD classification relative to white youth, after accounting for racial differences in academic achievement and/or social class, is an increasingly well-established finding, in studies focused on children at least. This study contributes a focus on disability classifications that persist into adolescence. Whereas some have argued this “underclassification” indicates racial minorities should be classified with disabilities at much higher rates (Morgan and Farkas 2015, 2016; Morgan et al. 2015, 2013), this study interprets findings like these as evidence of the importance of inequality outside of schools for education and health outcomes, similar to Shifrer, Muller, and Callahan (2011) and Shifrer, Muller, and Callahan (2010). Low levels of educational performance are a central criterion for disability classification and racial minorities are much more likely to be low achieving for the duration of their schooling careers. In one example, 65% of black fourth graders scored below basic proficiency in reading nationally in 2000 in contrast to 28% of white fourth graders (Grigg et al. 2003). Racial gaps in achievement are evident at kindergarten and remain constant across grade levels (Cheadle 2008), suggesting schools do not create racial gaps but fail to close them (Haertel 2013). In these ways, the practice of diagnosing children with neurological disabilities on the basis of an at least partially socially rooted characteristic like educational performance is central to the problem of racial disproportionality.
Carrier (1983) argued that classifying the low achievement of racial minority and socially disadvantaged youth as disability represents the ‘misrecognition and masking’ of social influences on academic performance. Federal regulations prohibit the classification of adolescents whose learning difficulties arise from “cultural factors” or “economic disadvantage” (Spellings, Knudsen, and Guard 2007), but it remains unclear whether diagnostic methods make these distinctions or if there even are valid distinctions (Bradley, Danielson, and Doolittle 2007). LD classifications symbolically transfer the source for low achievement from social inequities to individual deficiencies (Carrier 1983). This process of “masking and misrecognizing” the social causes for low achievement threatens our clear understanding of how learning ability develops and of processes of social reproduction. U.S. individualism promotes a disregard for the role of social inequality in educational disparities (Berliner and Biddle 1995), whereas neoliberal reform shifts the burden of poverty from the state to the shoulders of teachers and the community itself (Apple 2006). Not only are inequality, poverty, and race unpopular policy topics in the United States (Berliner and Biddle 1995), but, counter to perceptions, educators hesitate to acknowledge the contributions of poverty and race (Skiba et al. 2006), at risk of being perceived as a defeatist or biased (Darling-Hammond, Wilhoit, and Pittenger 2014). Racial disproportionality in LD classifications may be most effectively reduced by targeting inequities outside of schools and the ability of schools to address those inequities.
In contrast, bias becomes a possibility with the increased risk of classification for racial minorities in schools with fewer racial minorities. More objective classifications might be achieved through evaluation teams external to the school who receive information on the students’ background and context but not their race. Parents might be incorporated into classification decisions as advocates for their children and to improve the translation of theory and policy into practice (McKay and Garratt 2013; Nespor and Hicks 2010). Similarly, bias is a possible explanation for the persistence of male disproportionality net of controls—studies focused on younger U.S. children (Hibel, Farkas, and Morgan 2010) and on British youth (Strand and Lindsay 2009) showed similar results. In an alternate explanation, the disproportionate classification of males may also represent masked social causes, such as gendered behavior differences (Beaman, Wheldall, and Kemp 2006). Gendered learning differences may even be biologically sourced (Sauver et al. 2001). A more complete understanding of male disproportionality depends on multidisciplinary investigations using data with measures on both biological and social differences between males and females.
The independent associations of clinically irrelevant qualities like adolescents’ immigrant status and school characteristics present the possibility that LD classifications occur subjectively or inconsistently. Hibel, Farkas, and Morgan (2010) found accounting for school level differences in mean student achievement explained the estimated effect of school level student body poverty on children’s odds of classification with an LD. Although the data used in this study did not support such aggregations, Hibel and colleagues similarly described their findings as evidence for subjective classification. They characterized it as a “frog pond effect” in which a low performer, for instance, in a school in which low performance is prevalent may be less distinctive and less likely to be referred for special education evaluation. Criticisms of subjectivity and inconsistency are also levied at diagnostic processes for other mental conditions (Pickersgill 2012). Conrad (1992) described LDs as an example of “medicalized deviance,” in which human variation previously perceived as natural becomes a medical condition. With a focus on the manifest purposes of classifications (Perry 2011), others counter perspectives from the social model and medicalization trivialize the difficulties of non-normative people (Mulvany 2000), and argue diagnoses or classifications can validate these difficulties (Crosnoe, Riegle-Crumb, and Muller 2007). Social models of disability are criticized for offering few remedies for root issues (Sanders and Rogers 2011). The increasing emphasis on patients’ authority over their own health (Topol 2012) may counterbalance psychiatrists’ and educators’ vested interest in propagating simplistic absolute diagnoses. Efforts to locate biological indicators of LDs should continue, particularly with evidence that classified persons themselves hope for biological legitimation of their experiences (Beard and Neary 2013).
Limitations of this study merit mention. One quarter of sampled students were excluded because schools did not report their disability status. These students’ average differences are discussed in Methods. Although the main analytic sample of this study included adolescents whose schools reported the disability status of at least some sampled students, findings were similar across re-estimations first using all adolescents and then only adolescents whose schools reported the disability status of all sampled students (see Supplementary Table 2). These sensitivity analyses provide some measure of confidence that this study’s results are not an artifact of data limitations and analytic decisions. Nonetheless, although the analytic sample remained large and diverse, these findings cannot be generalized to the national population of students.
Second, although many of the measures used in the study may aptly characterize adolescents’ early lives, the cross-sectional nature of this study prevents a causal interpretation of findings. Although it is relatively unproblematic to assume adolescents’ race and gender precede their SES and linguistic-immigration history, and that these qualities precede youth carrying the LD classification as an adolescent, the dataset used in this study only measures educational performance during high school. In other words, it is possible LD classifications cause lower achievement rather than result from it (Shifrer, Callahan, and Muller 2013). This study uses high school test scores in a best attempt to capture some aspect of the timeless nature of racial and gender gaps in achievement. Confidence in this approach is increased by the constancy of racial and gender disparities in achievement across school careers (Buchmann, DiPrete and McDaniel 2008; Cheadle 2008), and by evidence suggesting schools and special education are ineffective at reducing achievement disparities (Barton and Coley 2009; Shifrer, Callahan, and Muller 2013). Confidence in this study’s results are increased by their similarity to findings from previous studies focused on children. Nonetheless, the associations established in this study cannot be interpreted causally. This study ideally contributes to laying a foundation for research on disability classifications that persist into adolescence, with findings to be replicated once better data is available.
The findings of this study support the notion that learning differences and the LD classification result from a complex interaction of biological and social and individual and structural factors. Some researchers, particularly those drawing on labeling theory, call for the end of classification within schools, arguing the current diagnostic model, Response to Intervention, has not resolved disproportionality (McKinney, Bartholomew, and Gray 2010). Until issues like these are resolved, educators and policymakers should be forthright about remaining gaps in scientific knowledge on conditions like LDs (Rafalovich 2005). In this way, teachers, parents, and students might incorporate useful insights from the LD classification while not feeling it seals youths’ destinies or captures their complexity (Broer and Heerings 2013). An increased understanding of the meaning and subjectivity of the LD classification may promote expectations for classified students more consistent with their achievement levels (Quinn et al. 2011). Future studies might also consider potential social class differences in the social etiology of the LD classification (Mulvany 2000). The paucity of research on this important topic highlights the need for improved data collection and interdisciplinary efforts.
Supplementary Material
Acknowledgments
Funding
This research was supported by the National Science Foundation (HRD-0834177, HRD-0965444, and HRD-1132028). This research was also supported by grants 5 R24 HD042849 and 5 T32 HD007081 awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Health and Child Development. This study benefitted from suggestions from Chandra Muller, Kelly Raley, Robert Hummer, Jo Phelan, and Rose Medeiros.
References
- Alexander Karl L., Entwisle Doris R., and Dauber Susan L.. 1996. “Children in Motion: School Transfers and Elementary School Performance.” The Journal of Education Research 90 (1):3–12. doi: 10.1080/00220671.1996.9944438. [DOI] [Google Scholar]
- American Psychiatric Association. 2000. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Association. [Google Scholar]
- Apple Michael. 2006. “Understanding and Interrupting Neoliberalism and Neoconservatism in Education.” Pedagogies: An International Journal 1 (1):21–26. doi: 10.1207/s15544818ped0101_4. [DOI] [Google Scholar]
- Barton Paul E. and Coley Richard J.. 2009. Parsing the Achievement Gap II (Policy Information Report). Princeton, NJ: Policy Information Center, Educational Testing Service. [Google Scholar]
- Beaman Robyn, Kevin Wheldall, and Coral Kemp. 2006. “Differential Teacher Attention to Boys and Girls in the Classroom.” Educational Review 58 (3):339–66. doi: 10.1080/00131910600748406. [DOI] [Google Scholar]
- Beard Renee L. and Neary Tara M.. 2013. “Making Sense of Nonsense: Experiences of Mild Cognitive Impairment.” Sociology of Health & Illness 35 (1):130–46. doi: 10.1111/j.1467-9566.2012.01481.x. [DOI] [PubMed] [Google Scholar]
- Becker Howard S. 1963. Outsiders: Studies in the Sociology of Deviance. New York, NY: The Free Press. [Google Scholar]
- Berliner David C. and Biddle Bruce C.. 1995. The Manufactured Crisis: Myths, Fraud, and the Attack on America’s Public Schools. Reading, MA: Addison-Wesley Publishing Company, Inc. [Google Scholar]
- Blackorby Jose, Schiller Ellen, Mallik Sangeeta, Hebbeler Kathleen, Huang Tracy, Javitz Harold, Marder Camille, Nagle Katherine, Shaver Debra, Wagner Mary, et al. 2010. Patterns in the Identification of and Outcomes for Children and Youth with Disabilities (NCEE 2010–4005) Washington DC: National Center for Education Evaluation and Regional Assistance, Institute of Education Sciences, U.S. Department of Education. [Google Scholar]
- Bradley Renee, Louis Danielson, and Jennifer Doolittle. 2007. “Responsiveness to Intervention: 1997 to 2007.” Teaching Exceptional Children 39 (5):8–12. doi: 10.1177/004005990703900502. [DOI] [Google Scholar]
- Breen Richard, Holm Anders, and Kristian Bernt Karlson. 2014. “Correlations and Non-Linear Probability Models.” Sociological Methods & Research 43 (4):571–605. doi: 10.1177/0049124114544224. [DOI] [Google Scholar]
- Broer Christian and Marjolijn Heerings. 2013. “Neurobiology in Public and Private Discourse: The Case of Adults with ADHD.” Sociology of Health & Illness 35 (1):49–65. doi: 10.1111/j.1467-9566.2012.01477.x. [DOI] [PubMed] [Google Scholar]
- Buchmann Claudia and Thomas A. DiPrete. 2006. “The Growing Female Advantage in College Completion: The Role of Family Background and Academic Achievement.” American Sociological Review 71 (4):515–41. doi: 10.1177/000312240607100401. [DOI] [Google Scholar]
- Buchmann Claudia, Thomas A. DiPrete, and Anne McDaniel. 2008. “Gender Inequalities in Education.” Annual Review of Sociology 34:319–37. doi: 10.1146/annurev.soc.34.040507.134719. [DOI] [Google Scholar]
- Carrier James G. 1983. “Masking the Social in Educational Knowledge: The Case of Learning Disability Theory.” The American Journal of Sociology 88 (5):948–74. doi: 10.1086/227765. [DOI] [Google Scholar]
- Cheadle Jacob E. 2008. “Educational Investment, Family Context, and Children’s Math and Reading Growth from Kindergarten through the Third Grade.” Sociology of Education 81 (1):1–31. doi: 10.1177/003804070808100101. [DOI] [Google Scholar]
- Clark Margaret D. 1997. “Teacher Response to Learning Disability: A Test of Attributional Principles.” Journal of Learning Disabilities 30 (1):69–79. doi: 10.1177/002221949703000106. [DOI] [PubMed] [Google Scholar]
- Clarke Paul, Claire Crawford, Fiona Steele, and Anna Vignoles. 2010. The Choice between Fixed and Random Effects Models: Some Considerations for Educational Research (DoQSS Working Paper No. 10–10) London, UK: Department of Quantitative Social Science, Institute of Education, University of London. [Google Scholar]
- Conley Dalton and Neil G. Bennett. 2000. “Is Biology Destiny? Birth Weight and Life Chances.” American Sociological Review 65 (3):458–67. doi: 10.2307/2657467. [DOI] [Google Scholar]
- Conrad Peter. 1992. “Medicalization and Social Control.” Annual Review of Sociology 18:209–32. doi: 10.1146/annurev.so.18.080192.001233. [DOI] [Google Scholar]
- Coughlin Dan. 1997. “The Person with a Learning Disability as a Minority Group Member.” Journal of Learning Disabilities 30 (5):572–75. doi: 10.1177/002221949703000514. [DOI] [PubMed] [Google Scholar]
- Crosnoe Robert, Catherine Riegle-Crumb, and Chandra Muller. 2007. “Gender, Self-Perception, and Academic Problems in High School.” Social Problems 54 (1):118–38. doi: 10.1525/sp.2007.54.1.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darling-Hammond Linda, Gene Wilhoit, and Linda Pittenger. 2014. Accountability for College and Career Readiness: Developing a New Paradigm. Stanford, CA: Stanford Center for Opportunity Policy in Education. [Google Scholar]
- DiPrete Thomas A. and Claudia Buchmann. 2013. The Rise of Women: The Growing Gender Gap in Education and What It Means for American Schools. New York, NY: Russell Sage Foundation. [Google Scholar]
- Eitle Tamela McNulty. 2002. “Special Education or Racial Segregation: Understanding Variation in the Representation of Black Students in Educable Mentally Handicapped Programs.” The Sociological Quarterly 43 (4):575–605. doi: 10.1111/j.1533-8525.2002.tb00067.x. [DOI] [Google Scholar]
- Ferri Beth A. and David J. Connor. 2005. “In the Shadow of Brown: Special Education and Overrepresentation of Students of Color.” Remedial and Special Education 26 (2):93–100. doi: 10.1177/07419325050260020401. [DOI] [Google Scholar]
- Ferri Beth A. and David J. Connor. 2006. Reading Resistance: Discourses of Exclusion in Desegregation & Inclusion Debates. New York, NY: Peter Lang Publishing, Inc. [Google Scholar]
- Fish Rachel. 2017. “The Racialized Construction of Exceptionality: Experimental Evidence of Race/ Ethnicity Effects on Teachers’ Interventions.” Social Science Research 62:317–34. doi: 10.1016/j.ssresearch.2016.08.007. [DOI] [PubMed] [Google Scholar]
- Fletcher Jack M., Carolyn Denton, and David J. Francis. 2005. “Validity of Alternative Approaches for the Identification of Learning Disabilities: Operationalizing Unexpected Underachievement.” Journal of Learning Disabilities 38 (6):545–52. doi: 10.1177/00222194050380061101. [DOI] [PubMed] [Google Scholar]
- Gebhardt Markus, Mathias Krammer, Susanne Schwab, Peter Rossmann, Barbara Gasteiger Klicpera, and Susanne Klatten. 2013. “What Is behind the Diagnosis of Learning Disability in Austrian Schools? an Empirical Evaluation of the Results of the Diagnostic Process.” International Journal of Special Education 28 (3):160–67. [Google Scholar]
- Grigg Wendy S., Mary C. Daane, Ying Jin, and Jay R. Campbell. 2003. The Nation’s Report Card: Reading 2002 (NCES 2003–521). Washington, DC: National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. [Google Scholar]
- Haertel, Edward. 2013. “Using Student Test Scores to Compare Teachers.” Presented at the SCOPE Brown Bag Seminars, October 21, Stanford, California, Retrieved June 2018 (https://edstream.stanford.edu/Video/Play/527aa737145543c893a7ea981b913d541d).
- Harry Beth and Janette K. Klingner. 2006. Why are so Many Minority Students in Special Education? Understanding Race and Disability in Schools. New York, NY: Teachers College Press. [Google Scholar]
- Heller Mathias. 2012. “MCAT To Add Pscyh, Sociology, Biochem.” Retrieved August 2014 (www.browndailyherald.com/2012/02/03/mcat-to-add-psych-sociology-biochem/).
- Hibel Jacob, Susan C. Faircloth, and George Farkas. 2008. “Unpacking the Placement of American Indian and Alaska Native Students in Special Education Programs and Services in the Early Grades: School Readiness as a Predictive Variable.” Harvard Educational Review 78 (3):498–528. doi: 10.17763/haer.78.3.8w010nq4u83348q5. [DOI] [Google Scholar]
- Hibel Jacob, George Farkas, and Paul L. Morgan. 2010. “Who Is Placed Into Special Education?” Sociology of Education 83 (4):312–32. doi: 10.1177/0038040710383518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ho Anita. 2004. “To Be Labeled, or Not to Be Labeled: That Is the Question.” British Journal of Learning Disabilities 32 (2):86–92. doi: 10.1111/j.1468-3156.2004.00284.x. [DOI] [Google Scholar]
- Klingner Janette K., Alfredo J. Artiles, and Laura Mendez Barletta. 2006. “English Language Learners Who Struggle with Reading: Language Acquisition or LD?” Journal of Learning Disabilities 39 (2):108–28. doi: 10.1177/00222194060390020101. [DOI] [PubMed] [Google Scholar]
- Klingner Janette K., Alfredo J. Artiles, Elizabeth Kozleski, Beth Harry, Shelley Zion, l Wi liam Tate, Grace Zamora Duran, and David Riley. 2005. “Addressing the Disproportionate Representation of Culturally and Linguistically Diverse Students in Special Education through Culturally Responsive Educational Systems.” Education Policy Analysis Archives 13 (38):1–43. doi: 10.14507/epaa.v13n38.2005. [DOI] [Google Scholar]
- Kohler Ulrich, Kristian Bernt Karlson, and Anders Holm. 2011. “Comparing Coefficients of Nested Nonlinear Probability Models.” The Stata Journal 11 (3):420–38. [Google Scholar]
- Kokanovic Renata, Gillian Bendelow, and Brigid Philip. 2013. “Depression: The Ambivalence of Diagnosis.” Sociology of Health & Illness 35 (3):377–90. doi: 10.1111/j.1467-9566.2012.01486.x. [DOI] [PubMed] [Google Scholar]
- Korenberg Julie R., Hiroko Kawashima, Pulst T Stefan-M Ikeuchi, Ogasawara N, Yamamoto K, Steven A. Schonberg, Ruth West, Leland Allen, Magenis K. Ellen, Ikawa N. Taniguchi, et al. 1990. “Molecular Definitions of a Region of Chromosome 21 that Causes Features of the Down Syndrome Phenotype.” The American Journal of Human Genetics 47:236–46. [PMC free article] [PubMed] [Google Scholar]
- Kroska Amy and Sarah K. Harkness. 2006. “Stigma Sentiments and Self-Meanings: Exploring the Modified Labeling Theory of Mental Illness.” Social Psychology Quarterly 69 (4):325–48. doi: 10.1177/019027250606900403. [DOI] [Google Scholar]
- Lester Gillian and Mark Kelman. 1997. “State Disparities in the Diagnosis and Placement of Pupils with a Learning Disability.” Journal of Learning Disabilities 30 (6):599–606. doi: 10.1177/002221949703000603. [DOI] [PubMed] [Google Scholar]
- Lin Ming-Jen and Jin-Tan Liu. 2009. “Do Lower Birth Weight Babies Have Lower Grades? Twin Fixed Effect and Instrumental Variable Method Evidence from Taiwan.” Social Science & Medicine 68 (10):1780–87. doi: 10.1016/j.socscimed.2009.02.031. [DOI] [PubMed] [Google Scholar]
- Margai Florence and Norah Henry. 2003. “A Community-Based Assessment of Learning Disabilities Using Environmental and Contextual Risk Factors.” Social Science & Medicine 56 (5):1073–85. doi: 10.1016/S0277-9536(02)00104-1. [DOI] [PubMed] [Google Scholar]
- Mathis C, Savier E, Bott JB, Clesse D, Bevins N, Sage-Ciocca D, Geiger K, Gilet A, Laux- Biehlman A, Goumon Y, et al. 2015. “Defective Response Inhibition and Collicular Noradrenaline Enrichment in Mice with Duplicated Retinotopic Map in the Superior Colliculus.” Brain Structure and Function 220 (3):1573–84. doi: 10.1007/s00429-014-0745-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maynard Douglas W. 2005. “Social Actions, Gestalt Coherence, and Designations of Disability: Lessons from and about Autism.” Social Problems 52 (4):499–524. doi: 10.1525/sp.2005.52.4.499. [DOI] [Google Scholar]
- McDermott Ray, Shelley Goldman, and Varenne Herve. 2006. “The Cultural Work of Learning Disabilities.” Educational Researcher 35 (6):12–17. doi: 10.3102/0013189X035006012. [DOI] [Google Scholar]
- McKay Jane and Dean Garratt. 2013. “Participation as Governmentality? the Effect of Disciplinary Technologies at the Interface of Service Users and Providers, Families and the State.” Journal of Education Policy 28 (6):733–49. doi: 10.1080/02680939.2012.752869. [DOI] [Google Scholar]
- McKinney Edward, Charles Bartholomew, and LaReasa Gray. 2010. “RTI and SWPBIS: Confronting the Problem of Disproportionality.” Communique 38 (6):1. [Google Scholar]
- McKown Clark and Rhona S Weinstein. 2008. “Teacher Expectations, Classroom Context, and the Achievement Gap.” Journal of School Psychology 46 (3):235–61. doi: 10.1016/j.jsp.2007.05.001. [DOI] [PubMed] [Google Scholar]
- Metzl Jonathan M. and Helena Hansen. 2014. “Structural Competency: Theorizing a New Medical Engagement with Stigma and Inequality.” Social Science & Medicine 103:126–33. doi: 10.1016/j.socscimed.2013.06.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mood Carina. 2010. “Logistic Regression: Why We Cannot Do What We Think We Can Do and What We Can Do about It.” European Sociological Review 26 (1):67–82. doi: 10.1093/esr/jcp006. [DOI] [Google Scholar]
- Morgan Paul L., and George Farkas. 2015. “Is Special Education Racist?” The New York Times, June 24. [Google Scholar]
- Morgan Paul L. and George Farkas. 2016. “Are We Helping All the Children that We are Supposed to Be Helping?” Educational Researcher 45 (3):226–28. doi: 10.3102/0013189X16644607. [DOI] [Google Scholar]
- Morgan Paul L., Michelle Frisco, George Farkas, and Jacob Hibel. 2010. “A Propensity Score Matching Analysis of the Effects of Special Education Services.” The Journal of Special Education 43 (4):236–54. doi: 10.1177/0022466908323007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan Paul L., Marianne M George Farkas, Richard Mattison Hillemeier, Steve Maczuga, Li Hui, and Michael Cook. 2015. “Minorities are Disproportionately Underrepresented in Special Education Longitudinal Evidence across Five Disability Conditions.” Educational Researcher 44 (5):278–92. doi: 10.3102/0013189X15591157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morgan Paul L., Marianne M Jeremy Staff, George Farkas Hillemeier, and Steven Maczuga. 2013. “Racial and Ethnic Disparities in ADHD Diagnosis from Kindergarten to Eighth Grade.” Pediatrics 132 (1):85–93. doi: 10.1542/peds.2012-2390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mulvany Julie. 2000. “Disability, Impairment or Illness? the Relevance of the Social Model of Disability to the Study of Mental Disorder.” Sociology of Health & Illness 22 (5):582–601. doi: 10.1111/shil.2000.22.issue-5. [DOI] [Google Scholar]
- Nespor Jan and David Hicks. 2010. “Wizards and Witches: Parent Advocates and Contention in Special Education in the USA.” Journal of Education Policy 25 (3):309–34. doi: 10.1080/02680931003671954. [DOI] [Google Scholar]
- Noguera Pedro A. 2008. The Trouble with Black Boys: And Other Reflections on Race, Equity, and the Future of Public Education. San Francisco, CA: John Wiley and Sons. [Google Scholar]
- Ong-Dean Colin. 2009. Distinguishing Disability: Parents, Privilege, and Special Education. Chicago, IL: The University of Chicago Press. [Google Scholar]
- Oswald Donald P., Al M. Best, and Martha J. Coutinho. 2006. “Individual, Family, and School Factors Associated with the Identification of Female and Male Students for Special Education.” International Journal of Special Education 21 (3):120–37. [Google Scholar]
- Oswald Donald P., Martha J. Coutinho, Al M. Best, and Nu Nguyen. 2001. “Impact of Sociodemographic Characteristics on the Identification Rates of Minority Students as Having Mental Retardation.” Mental Retardation 39 (5):351–67. doi: . [DOI] [PubMed] [Google Scholar]
- Pampel Fred C. 2009. “The Persistence of Educational Disparities in Smoking.” Social Problems 56 (3):526– 42. doi: 10.1525/sp.2009.56.3.526. [DOI] [Google Scholar]
- Perry Brea L. 2011. “The Labeling Paradox: Stigma, the Sick Role, and Social Networks in Mental Illness.” Journal of Health and Social Behavior 52 (4):460–77. doi: 10.1177/0022146511408913. [DOI] [PubMed] [Google Scholar]
- Pickersgill Martyn. 2012. “Standardising Antisocial Personality Disorder: The Social Shaping of a Psychiatric Technology.” Sociology of Health & Illness 34 (4):544–59. doi: 10.1111/j.1467-9566.2011.01404.x. [DOI] [PubMed] [Google Scholar]
- Quinn Neil, Michael Smith, Susan Fleming, Amanda Shulman, and Lee Knifton. 2011. “Self and Others: The Differential Impact of an Anti-Stigma Programme.” Stigma Research and Action 1 (1):36–43. doi: 10.5463/sra.v1i1.20. [DOI] [Google Scholar]
- Rafalovich Adam. 2005. “Exploring Clinician Uncertainty in the Diagnosis and Treatment of Attention Deficit Hyperactivity Disorder.” Sociology of Health & Illness 27 (3):305–23. doi: 10.1111/shil.2005.27.issue-3. [DOI] [PubMed] [Google Scholar]
- Samson Jennifer F. and Nonie K. Lesaux. 2009. “Language-Minority Learners in Special Education: Rates and Predictors of Identification for Services.” Journal of Learning Disabilities 42 (2):148–62. doi: 10.1177/0022219408326221. [DOI] [PubMed] [Google Scholar]
- Sanders Caroline and Anne Rogers. 2011. “Bodies in Context: Potential Avenues of Inquiry for the Sociology of Chronic Illness and Disability within a New Policy Era” Pp. 483–504 in Handbook of the Sociology of Health, Illness, and Healing: A Blueprint for the 21st Century, edited by Bernice A. Pescosolido, Jack K. Martin, Jane D. McLeod, and Anne Rogers. New York, NY: Springer Science+Business Media, LLC, [Google Scholar]
- Sauver Jennifer L., St. Slavica K. Katusic, William J. Barbaresi, Robert C. Colligan, and Steven J. Jacobsen. 2001. “Boy/Girl Differences in Risk for Reading Disability: Potential Clues?” American Journal of Epidemiology 154 (9):787–94. doi: 10.1093/aje/154.9.787. [DOI] [PubMed] [Google Scholar]
- Scheff Thomas J. 1966. Being Mentally Ill: A Sociological Theory. Piscataway, NJ: Aldine Transaction. [Google Scholar]
- Shifrer Dara. 2013. “Stigma of a Label: Educational Expectations for High School Students Labeled with a Learning Disability.” Journal of Health and Social Behavior 54 (4):462–80. doi: 10.1177/0022146513503346. [DOI] [PubMed] [Google Scholar]
- Shifrer Dara. 2016. “Stigma and Stratification Limiting the Math Course Progression of Adolescents Labeled with a Learning Disability.” Learning and Instruction 42 (1):47–57. doi: 10.1016/j.learninstruc.2015.12.001. [DOI] [Google Scholar]
- Shifrer Dara, Rebecca Callahan, and Chandra Muller. 2013. “Equity or Marginalization? the High School Course-Taking of Students Labeled with a Learning Disability.” American Educational Research Journal 50 (4):656–82. doi: 10.3102/0002831213479439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shifrer Dara, Chandra Muller, and Rebecca Callahan. 2010. “Disproportionality: A Sociological Perspective on the Identification by Schools of Students with Learning Disabilities” Pp. 279–308 in Research in Social Science and Disability Series, edited by Altman Barbara M and Barnartt Sharon. Bingley, United Kingdom: Emerald Group Publishing Limited, [Google Scholar]
- Shifrer Dara, Chandra Muller, and Rebsecca Callahan. 2011. “Disproportionality and Learning Disabilities: Parsing Apart Race, Socioeconomic Status, and Language.” Journal of Learning Disabilities 44 (3):246–57. doi: 10.1177/0022219410374236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shonkoff Jack P. and Deborah A. Phillips. 2000. From Neurons to Neighborhoods: The Science of Early Childhood Development Washington, DC: National Research Council and Institute of Medicine, National Academies. [PubMed] [Google Scholar]
- Singer Judith D., Judith S. Palfrey, John A. Butler, and Deborah Klein Walker. 1989. “Variation in Special Education Classification across School Districts: How Does Where You Live Affect What You are Labeled?” American Educational Research Journal 26 (2):261–81. doi: 10.3102/00028312026002261. [DOI] [Google Scholar]
- Skiba Russell, Ada Simmons, Shana Ritter, Kristin Kohler, Michelle Henderson, and Wu Tony. 2006. “The Context of Minority Disproportionality: Practitioner Perspectives on Special Education Referral.” Teachers College Record 108 (7):1424–59. doi: 10.1111/j.1467-9620.2006.00699.x. [DOI] [Google Scholar]
- Skiba Russell J., Ada B. Simmons, Ashley C. Shana Ritter, Gibb M. Karega Rausch, Jason Cuadrado, and Choong-Geun Chung 2008. “Achieving Equity in Special Education: History, Status, and Current Challenges.” Exceptional Children 74 (3):264–88. doi: 10.1177/001440290807400301. [DOI] [Google Scholar]
- Spellings Margaret, William W. Knudsen, and Patricia J. Guard. 2007. 27th Annual (2005) Report to Congress on the Implementation of the Individuals with Disabilities Education Act, Vol. 1 Washington, DC: Office of Special Education Programs, Office of Special Education and Rehabilitative Services, U.S. Department of Education. [Google Scholar]
- Sprung Juraj, Randall P. Flick, Robert T. Wilder, Slavica K. Katusic, Tasha L. Pike, Mariella Dingli, Stephen J. Gleich, Darrell R. Schroeder, William J. Barbaresi, Andrew C. Hanson, et al. 2009. “Anesthesia for Cesarean Delivery and Learning Disabilities in a Population-Based Birth Cohort.” Anesthesiology 111 (2):302–10. doi: 10.1097/ALN.0b013e3181adf481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strand Steve and Geoff Lindsay. 2009. “Ethnic Disproportionality in Special Education: Evidence from an English Population Study.” Journal of Special Education 43 (3):174–90. doi: 10.1177/0022466908320461. [DOI] [Google Scholar]
- Sullivan Amanda L. 2011. “Disproportionality in Special Education Identification and Placement of English Language Learners.” Exceptional Children 77 (3):317–34. doi: 10.1177/001440291107700304. [DOI] [Google Scholar]
- Sullivan Amanda L. and Alfredo J. Artiles. 2011. “Theorizing Racial Inequity in Special Education: Applying Structural Inequity Theory to Disproportionality.” Urban Education 46 (6):1526–52. doi: 10.1177/0042085911416014. [DOI] [Google Scholar]
- Topol Eric. 2012. The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care. New York, NY: Basic Books. [Google Scholar]
- U.S. Department of Education. 2004. “Part 300 - Assistance to States for the Education of Children with Disabilities, Subpart A General, Sec. 300.8 Child with A Disability, (C) Definitions of Disability Terms.” Retrieved December 2013 (http://idea.ed.gov/explore/view/p/,root,regs,300,A,300%252E8,c,).
- U.S. Department of Education. 2016. “Topic: Identification of Specific Learning Disabilities.” Retrieved February 2016 (http://idea.ed.gov/explore/view/p/,root,dynamic,TopicalBrief,23).
- U.S. Government Printing Office. 2010. “S. 2781 (111th): Rosa’s Law.” Retrieved January 2014 (https://www.govtrack.us/congress/bills/111/s2781/text).
- UCLA Statistical Consulting Group. 2017. “Deciphering Interactions in Logistic Regression.” Retrieved September 2017 (https://stats.idre.ucla.edu/stata/seminars/deciphering-interactions-in-logistic-regression/).
- White Ian R., Patrick Royston, and Angela M. Wood. 2011. “Multiple Imputation Using Chained Equations: Issues and Guidance for Practice.” Statistics in Medicine 30 (4):377–99. doi: 10.1002/sim.4067. [DOI] [PubMed] [Google Scholar]
- Willingham Warren W., Judith M. Pollack, and Charles Lewis. 2002. “Grades and Test Scores: Accounting for Observed Differences.” Journal of Educational Measurement 39 (1):1–37. doi: 10.1111/j.1745-3984.2002.tb01133.x. [DOI] [Google Scholar]
- Xue Xiaonan, Mimi Y. Kim, Tao Wang, Mark H. Kuniholm, and Howard D. Strickler. 2017. “A Statistical Method for Studying Correlated Rare Events and Their Risk Factors.” Statistical Methods in Medical Research 26 (3):1416–28. doi: 10.1177/0962280215581112. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.