

Abstract
Objectives:
To measure the levels of systemic lupus erythematosus (SLE) awareness among patients in primary health care (PHC) at King Abdulaziz Medical City (KAMC), Riyadh, Kingdom of Saudi Arabia, and to explore the factors which influence the SLE awareness.
Methods:
The study was a cross-sectional study conducted between February and September 2018 in 4 PHC centers at KAMC. The study participants were male and female adult visitors to the centers age from 18-60 years. The sample size was 400 participants. The participants were enrolled via a random convenience sampling method. Study data was collected using a self-administered questionnaire. Analytic statistics were carried out using the Chi-square test for associations or the differences between 2 categorical variables. A p≤0.05 was considered significant.
Results:
Most of the participants in our study were unaware of SLE. This indicates poor knowledge about the disease. There were no statistically significant differences in awareness about SLE between males and females (p=0.304), but there were significant differences according to education levels (p=0.023), and between knowing a person who had been diagnosed with SLE and caring for him or her (p=0.020).
Conclusion:
The study shows that this survey is valuable and beneficial to the community as it helps people to assess their knowledge about SLE and become aware of this disease, as well as awareness of SLE should be promoted among the community.
Systemic lupus erythematosus (SLE) is a chronic inflammatory auto-immune disease that occurs when the immune system assaults the tissues of the body and its organs. Systemic means that SLE can affect the body’s various organs, including the skin, joints, kidneys, lungs, and heart. Lupus refers to the butterfly rash on the patient’s face, which is similar to the whitish outline marking on the middle of wolves’ faces. Erythematosus means the rash is reddish to purplish in color.1,2 The epidemiological studies estimated that the prevalence of SLE was 241 per 100,000 people in North America which is the highest, and the lowest incidence was 0.3 per 100,000 person yearly noticed in South Africa which is the lowest. Systemic lupus erythematosus affects women more than men for all age and ethnic groups. Women of reproductive age (15-45) are often affected, and the rate of females to males is 9 to 1.1-3 Likewise, scientists trust that human genetic studies will structure our understanding of the premise of individual hereditary vulnerability to SLE. These studies will help to detect the person who will have a high probability of having SLE in the future.1 Despite numerous advances in the diagnosis and treatment of SLE and associated comorbid conditions, such as loss of physical, social, and emotional functioning, this disease remains a source of significant morbidity and mortality.4-6 In addition, SLE has a severe and pervasive influence on patients’ self-esteem, resulting in emotional challenges, fear of rejection, stigmatization, social isolation, and loss of independence.7-9 On the other hand, there are some studies that stress on the importance of raising awareness and educating the public about SLE by clarifying the nature of the disease, its direct causes, treatment methods, and control mechanisms. In Riyadh, Kingdom of Saudi Arabia (KSA), a study conducted in 2015 among students at King Saud University showed that the level of awareness about SLE among students was low. Workshops or campaigns are required to enhance awareness and correct misunderstandings.10 In Taif, KSA, a study undertaken in 2017 that involved many of the Kingdom’s regions reported a high prevalence of less than optimal awareness and knowledge of SLE among the Saudi adult population.11 In India, a study conducted in 2017, among the general population to assess their SLE awareness and knowledge, found that the majority of participants had insufficient knowledge of its status as a rare disease that occurs in the population.12
A 2018 study conducted among students at King Faisal University in Al-Hassa, KSA, found that most students have low awareness and some misunderstandings regarding SLE. Awareness programs are presumed to be able to increase awareness about SLE, as these campaigns have confirmed that greater public awareness may be useful in managing and controlling the disease and its associated complications.13
Methods
The study was a cross-sectional study conducted between February and September 2018 in 4 PHC centers at King Abdulaziz Medical City (KAMC, Riyadh, KSA: the Health Care Specialty Center (HCSC); King Abdulaziz Housing clinics (Iskan); the National Guard Comprehensive Specialized Clinic (NGCSC), and King Abdulaziz Housing clinics (Dirab).
Each of the 4 centers delivers primary curative and preventive health services, and consists of walk-in services, a minor emergency room setting, and an appointment booking system for patients to obtain treatment and counseling for acute and chronic medical conditions. The study participants were male and female adult visitors to the centers aged between 18-60 years.
The sample size was calculated by the Openepi website. The population of the KAMC primary health care as per the latest report was found to be approximately 420,000 people in 2017. They were distributed as follows: 200,000 patients in the HCSC; 100,000 patients in the NGCSC; 70,000 patients in King Abdulaziz Housing clinics (Dirab); and 50,000 patients in King Abdulaziz Housing clinics, (Iskan). Using a 95% confidence interval and 5% margin of error, the calculated minimum sample size was expected to be 384, which was modified to 400 to compensate for incomplete questionnaires.
The proportion of participants from each of the 4 centers was based on the clinic catchment area as follows: HCSC serves a population of approximately 200,000 people, (n=190, 47.6%) of the sample size; NGCSC serves approximately 100,000 people, (n=95, 23.8%) of the sample size; Dirab center serves approximately 70,000 people, (n=67, 16.6%) of the sample size; and Iskan serves approximately 50,000 people, (n=48, 11.9%) of the sample size.
Inclusion criteria are adult’s patient from the age of 18-60 years from KAMC primary health care centers and exclusion criteria are cognitive impairment patients.
Study data was collected using a self-administered questionnaire. The questionnaire used was developed by Sullivan,2 and was adopted by the present study to meet the study main objectives after a literature review of similar studies. The questionnaire was written in simple Arabic, and included the following sections: demographic data, and questions regarding knowledge, attitudes, and beliefs regarding SLE. Two research experts revised the questionnaire, and a pilot study was conducted with 10 participants to confirm and verify the instrument’s validity. The participants were enrolled via a random convenience sampling method. Patients to the 4 primary care centers were approached while sitting in the waiting area. The investigator explained the purpose of study to each participant and obtained verbal and documented consent to participate in the study before administering the questionnaire. All data were coded, entered, and analyzed using the Statistical Package for the Social Sciences, version 23 (IBM Corp., Armonk, NY, USA). Continuous variables were reported in terms of means and standard deviation, while categorical variables were described using frequencies and percentages. Analytic statistics were performed using the Chi-squared test for associations or the difference between 2 categorical variables. A p-value of ≤0.05 was considered significant.
Ethical considerations
Approval for the study was obtained from King Abdullah International Medical Research Center, the Ministry of the National Guard, KSA. The participants were fully informed regarding voluntary participation, privacy, anonymity, and confidentiality of the data was ensured and the Declaration of Helsinki ethical rules were followed.
Results
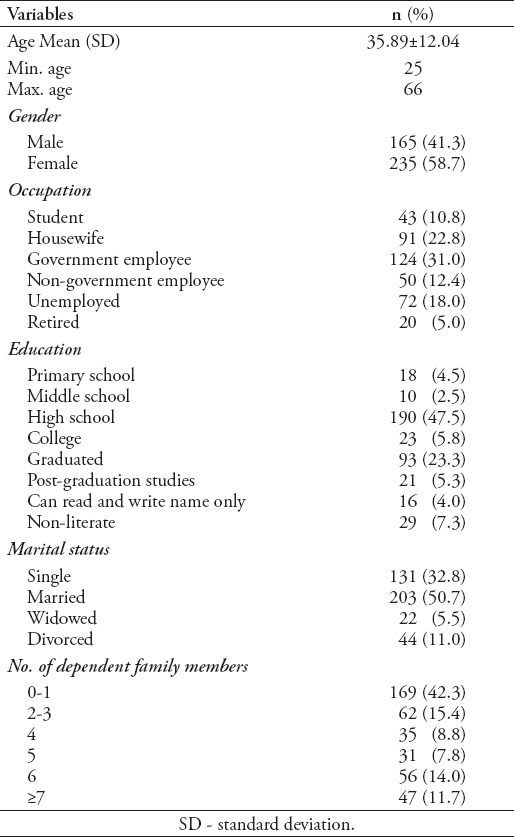
Table 1 shows that the majority of PHC patients included in the study were female (58.7%), while males made up 41.3%. The mean age of patients was 35.98±12.04 years with most being government employees, followed by housewives, the unemployed, non-government employees, students, and the retired. The majority of PHC patients included in the study had some high school; they were followed by graduates, the non-literate, college students, post-graduates, primary school, those able to read and write only their names, and those with middle school. Most study participants were married, followed by single, divorced, and widowed participants. The majority of participants had no or only one dependent family member.
Table 1.
Frequencies, distribution, and percentages of socio-demographic variables.
Questions about knowledge, attitudes, and beliefs regarding SLE
As shown in Table 2, 56.8% of the patients had heard the term “SLE”. The most common way participants recognized the disease was from the internet (online resources) as the majority of them had not been diagnosed with SLE. Most of the participants did not know anyone with SLE and the majority did not know that SLE is not contagious but could be fatal. Most believed that SLE was a hereditary disease and classified SLE in this way. The majority did not know SLE mostly affects females. They also did not know that SLE can affect any organs in the body. Indeed 26.8% believed that only the kidney could be affected by SLE. Most of the patients did not know the major symptoms of SLE (28.5%) and 41.5% did not know the main laboratory tests for SLE; 40.5% did not know whether SLE could be prevented although most believed that SLE is a treatable disease (41.2%). The majority of participants did not know the complications of SLE (40.2%) and 26% believed that a treatment of SLE was chemotherapy. Most did not know that SLE can affect the fertility of men and women (44.0%), although they knew that SLE causes fetal abnormalities or recurrent abortions in the affected mother (50.3%). Finally, the majority of participants believed that awareness of SLE should be promoted (86.3%); the score of SLE awareness was (n=400, 64.7%) indicates that participant were unaware of SLE, while 35.3% were aware of SLE.
Table 2.
Awareness of systemic lupus erythematosus frequencies and percentages.
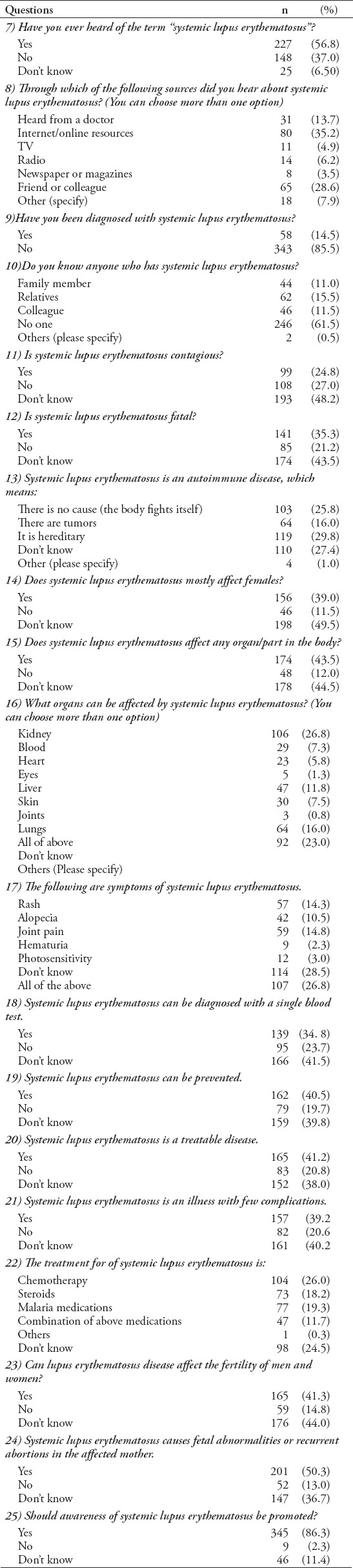
Table 3 shows the correlations between sociodemographic variables (gender, education, do you know anyone who has SLE?) and awareness of SLE. Awareness about SLE by gender was not statistically significant (p=0.304), but there was a statistically significant difference according to education level. Participants with high school education were more aware than those with a lower level of education (primary and middle school) (p=0.023).
Table 3.
Correlations between sociodemographic variables and awareness.
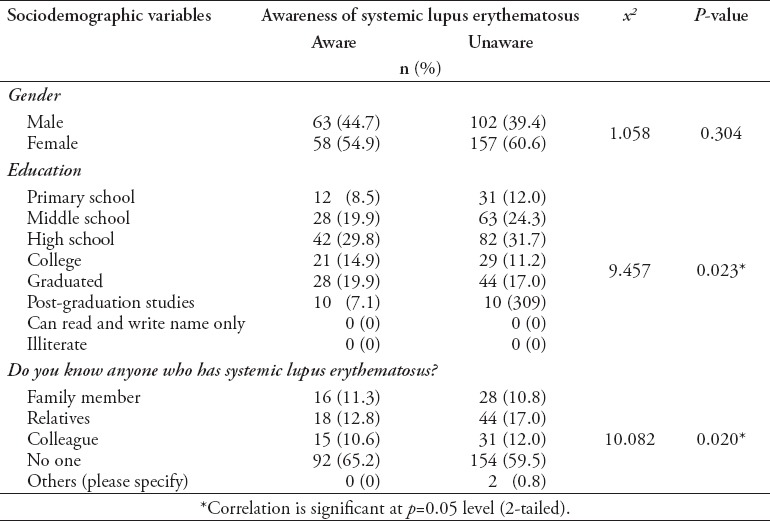
Furthermore, there was a statistically significant correlation between knowing a person with SLE and awareness (p=0.020); this means that if the participants did not know a person with SLE before, they will be unaware of SLE and its nature or manifestations.
Thus, the major factors that affect SLE knowledge and attitude are education level and knowing someone who have been diagnosed previously with SLE and is coping with it.
Discussion
The 400 participants in this study were chosen from the waiting area in the clinics using random convenience sampling. The fact that females are more frequently reported having the disease than males. This is attributable to the fact that women are more expected to get SLE than males. Most of the participants were government employees (31%) and the majority had studied at high school; 50.7% of participants were married with/without dependent family members. The study clarifies that 56.8% of participants had heard the term SLE and the most common way that they recognized the disease was through the internet (online resources). As found in a similar local study, 40% have previously heard the term SLE.10 As well as the second local study, 55.9% have previously heard the term SLE.13 The vast majority had not been diagnosed with SLE and did not know that SLE is not contagious and fatal. However, they believed that the kidney is the only organ that can be affected by SLE. As found in a similar local study, more than 50% of participant believed that SLE do not have renal manifestation while some study conclude that one of the major reasons of death among SLE patients is renal failure.11 The onset of the disease is slow with new symptoms occurring over weeks, months, and sometimes years. The most common initial symptoms of SLE in patients are unspecified complaints of fatigue and health malaise. Many patients experience sporadic or persistent high temperatures with gradual loss of weight and poor appetite. Ultimately, patients progress to developing certain clinical symptoms because one or more parts of the body are affected. Skin and mucous membranes are usually the most affected by the disease. Symptoms may include various forms of skin rash, photosensitivity, and mouth ulcers. In one-third of the affected patients, the characteristic butterfly rash occurs in the center of a patient’s face.4,5
Systemic lupus erythematosus has been found to have serious complications in previous studies, which range from renal failure to death. Early death is common in males with skin manifestations who are under 16 years old at the time of diagnosis while the possibility of late death is frequently seen in patients over 30 years at the time of diagnosis. Overall death was significantly high in older patients and in those with established kidney disease.6,7 In terms of SLE diagnostic patterns, the participants did not know the possible laboratory tests for diagnosing SLE; they believed that SLE is a treatable sickness where the main treatment is chemotherapy. Moreover, a great number did not know the minor or major complications of SLE. Diagnosis depends on the availability of a range of signs and symptoms with some laboratory tests involving blood and urine, and sometimes biopsy to exclude further disease. Symptoms and signs sometimes do not appear observable at any time, which makes it difficult to diagnose the disease in a timely manner. The American College of Rheumatology has listed 11 criteria to differentiate SLE from other diseases; if many of them are reported in clinical settings they may indicate the presence of SLE. This criterion roughly signifies the common clinical symptoms of people with this disease. To diagnose this disease, at least 4 of these 11 criteria must be met at any given time. However, experienced physicians are able to diagnose it even if patients present with fewer than 4 criteria. Most of the participants in our study were unaware of SLE. This indicates poor knowledge about the disease. There were no statistically significant differences in awareness about SLE between males and females (p=0.304), but there was statistically significant differences according to education levels (p=0.023), and between knowing a person who had been diagnosed with SLE and caring for him or her (p=0.020).
Finally, most participants believed that awareness of SLE should be promoted in the community, whether in hospitals or schools, to enhance knowledge about the disease and its nature in a different way; it was recommended that clinical workshops be conducted, short videotapes or medical flyers be used, and face-to-face discussions be held along with support groups and online resources.
Study limitations
This study was geographically limited and only included the patients to PHC clinics at KAMC in Riyadh, KSA. Therefore, it may not be possible to generalize the results. Recall bias is also possible.
There is a need for public awareness activities to educate people about SLE, its clinical manifestations, diagnosis, treatment, and complications; although it is not a contagious disease that requires isolation, it may be fatal if neglected.
In conclusion, the study shows that this survey is valuable and beneficial to the community as it helps people to assess their knowledge about SLE and become more aware of the disease.
Acknowledgment
The authors gratefully acknowledge eScienta (www.eScienta.com) for the English language editing.
Footnotes
References
- 1.Rees F, Doherty M, Grainge MJ, Lanyon P, Zhang W. The worldwide incidence and prevalence of systemic lupus erythematosus:a systematic review of epidemiological studies. Rheumatology (Oxford) 2017;56:1945–1961. doi: 10.1093/rheumatology/kex260. [DOI] [PubMed] [Google Scholar]
- 2.Sullivan S. [Dissertations] Vol. 1312. Wisconsin (USA): University of Wisconsin-Milwaukee; Development of a systemic lupus erythematosus knowledge questionnaire:The relationship among disease proximity, educational exposure and knowledge; pp. 1–127. [Google Scholar]
- 3.Moriarty T, O'Sullivan M, Tam A, Gonçalves RM, Wall JG. Systemic lupus erythematosus in Portugal:diagnosis and disease awareness from 1970 to 2001. Eur J Epidemiol. 2003;18:995–999. doi: 10.1023/a:1025854611531. [DOI] [PubMed] [Google Scholar]
- 4.Khan A, Shah MH, Nauman M, Hakim I, Shahid G, Niaz P, et al. Clinical manifestations of patients with Systemic Lupus Erythematosus (SLE) in Khyber Pakhtunkhwa. J Pak Med Assoc. 2017;67:1180–1185. [PubMed] [Google Scholar]
- 5.Strand V, Galateanu C, Pushparajah DS, Nikaï E, Sayers J, Wood R, et al. Limitations of current treatments for systemic lupus erythematosus:a patient and physician survey. Lupus. 2013;22:819–826. doi: 10.1177/0961203313492577. [DOI] [PubMed] [Google Scholar]
- 6.Heller T, Ahmed M, Siddiqqi A, Wallrauch C, Bahlas S. Systemic lupus erythematosus in Saudi Arabia:morbidity and mortality in a multiethnic population. Lupus. 2007;16:908–914. doi: 10.1177/0961203307081112. [DOI] [PubMed] [Google Scholar]
- 7.La Paglia GMC, Leone MC, Lepri G, Vagelli R, Valentini E, Alunno A, et al. One year in review 2017:systemic lupus erythematosus. Clin Exp Rheumatol. 2017;35:551–561. [PubMed] [Google Scholar]
- 8.Sutanto B, Singh-Grewal D, McNeil HP, O'Neill S, Craig JC, Jones J, et al. Experiences and perspectives of adults living with systemic lupus erythematosus:thematic synthesis of qualitative studies. Arthritis Care Res (Hoboken) 2013;65:1752–1765. doi: 10.1002/acr.22032. [DOI] [PubMed] [Google Scholar]
- 9.Ippolito A, Petri M. An update on mortality in systemic lupus erythematosus. Clin Exp Rheumatol. 2008;26:S72–S79. [PubMed] [Google Scholar]
- 10.Omair MA, Al Ohali SM, Abdulkarim FA, Madhi HA, Alghamdi LA. Awareness and Misconceptions of Female Students in King Saud University on Systemic Lupus Erythematosus. Rheumatology (Sunnyvale) 2015;5:165. [Google Scholar]
- 11.Althobiti SD, Alharthi TF, Alam SS, Althobiti EO. Awareness and knowledge of saudi population about systemic lupus erythematosus, cross sectional study. World Journal of Pharmaceutical Research. 2017;6:17. [Google Scholar]
- 12.Zaaba N, Gheena To study the awareness of the general public on systemic lupus erythematosus. International Journal of Current Research. 2017;9:46382–46385. [Google Scholar]
- 13.AlKhalaf AA, Ghaleb R, Al Shawaf MH, Abdrabalnabi AA, Al-Shabib AA, Al-Khatem AH, Al Malak YT, Al Qattan HA, Al-Khalaf HE. Awareness of Systemic Lupus Erythematosus among Students in King Faisal University. Egyptian Journal of Hospital Medicine. 2018:70. [Google Scholar]