

Abstract
Introduction
Early detection of Adverse Drug Events (ADEs) from Electronic Health Records (EHRs) is an important, challenging task to support pharmacovigilance and drug safety surveillance. A well-known challenge to use clinical text for detection of ADEs is that much of the detailed information is documented in a narrative manner. Clinical Natural Language Processing (NLP) is the key technology to extract information from unstructured clinical text.
Objective
We present a machine learning-based clinical NLP system - MADEx for detecting medications, ADEs and their relations from clinical notes.
Methods
We developed a Recurrent Neural Network (RNN) model using Long Short-Term Memory (LSTM) strategy for clinical Name Entity Recognition (NER) and compared it with a baseline Conditional Random Fields (CRFs). We developed a modified training strategy for RNN, which outperformed the widely used early stop strategy. For relation extraction, we compared Support Vector Machines (SVMs) and Random Forests on single-sentence relations and cross-sentence relations. We also developed an integrated pipeline to extract entities and relations together by combining RNN and SVMs.
Results
MADEx achieved top three best performance (F1-score of 0.8233) for clinical NER in the 2018 Medication and Adverse Drug Events (MADE1.0) challenge. The post-challenge evaluation showed that the relation extraction module and integrated pipeline (identify entity and relation together) of MADEx are comparable to the best systems developed in this challenge.
Conclusion
This study demonstrated the efficiency of deep learning methods for automatic extraction of medications, ADEs, and their relations from clinical text to support pharmacovigilance and drug safety surveillance.
1. Introduction
Adverse Drug Events (ADEs) are defined as injuries caused by medical intervention related to drugs. [1] ADEs are increasingly common in the United States and around the world. [2, 3] A recent study examined the incidence rate of ADEs using a nationwide inpatient sample dataset of the United States from 2008 to 2011 and reported an average incidence rate of 6.28%, with an increasing trend from 5.97% (at 2008) to 6.82% (at 2011). [4] Similar studies reported an incidence rate around 6-8% in Saudi Arabia, 3.22% for England, and 4.78% for Germany. [3, 5, 6] ADEs are reported to increase the healthcare cost, length of stay, and in-hospital mortality rates. [2] A large majority of ADEs are preventable. Early detection and prevention of ADEs is expected to result in safer and higher quality healthcare, reduce healthcare cost and improve healthcare outcome. [4] Narrative clinical text contains detailed treatment and response information from clinical practice and could be used to detect ADEs for pharmacovigilance and drug safety surveillance.
Unstructured clinical text has been increasingly used for clinical and translational research as it contains detailed patient information that cannot be captured in abstracted medical codes. [7, 8] A well-known challenge to use unstructured clinical text is that much of the detailed information is documented in a narrative manner, which is not directly accessible. Clinical Natural Language Processing (NLP) is the key technology to extract information from unstructured clinical text to support various clinical studies and applications that depend on structured data. To use narrative clinical text for detection of ADEs, the clinical NLP systems need to: (1) identify the mentions of medications, ADEs, and their attributes – a typical clinical Named Entity Recognition (NER) [9] task; and (2) determine their relations (e.g., which medication induced the ADE) – a relation extraction [10] task. The clinical NLP community has organized open challenges such as i2b2 (The Center for Informatics for Integrating Biology and the Bedside) challenges [11, 12], SemEval (International Workshop on Semantic Evaluation) challenges [13] and ShARe/CLEF eHealth challenges [14], to examine current NLP methods for clinical NER and relation extraction. Most NLP systems approach the clinical NER and relation extraction using machine learning-based methods. Researchers have applied various machine learning methods such as Conditional Random Fields (CRFs) [15], Support Vector Machines (SVMs) [16], Structured Support Vector Machines (SSVMs) [17], as well as hybrid methods.
Clinical NER is a fundamental task to extract clinical concepts of interest (e.g., medications, ADEs) from clinical narratives. [9] Researchers have developed various NER algorithms and applied them in general clinical NLP systems. Early clinical NLP systems such as MetaMap [18], MedLEE [19], and KnowledgeMap [20], applied rule-based methods that rely on existing medical vocabularies. Later, many researchers explored machine learning models and reported improved performance. Machine learning models approach clinical NER as a sequence labeling problem – finding the best label sequence (e.g., BIO tag sequence: B - the beginning of a concept, I - words inside of a concept, O - words outside of a concept) for a given input sequence (words from clinical text). The machine learning algorithms sequentially scan each of the input words and determine the best label sequence according to the context features from surrounding words. Most top-performing clinical NER methods are based on machine learning models, where CRFs and SSVMs are among the most popular solutions. For example, de Bruijn el al. [21] developed the best-performing clinical NER system using a semi-Markov Hidden Markov Models (HMM) in 2010 i2b2 challenge, task 1 – a concept extraction task focused on the extraction of problems, treatments and lab tests; Zhang et al. [22] developed the best-performing NER system using an ensemble model of CRFs and SSVMs in 2014 SemEval open challenge, task 7 – analysis of clinical text; Tang et al. [23] contributed the best-performing NER system using SSVMs in the 2013 ShARe/CLEF eHealth Challenges on detection of disorder names from clinical notes. Recently, deep learning methods are emerging as new state-of-the-art solutions for clinical NER. Deep learning-based NER methods applied deep network architectures to learn multiple levels of data representation, which is different from the traditional machine learning methods where features were manually designed by researchers. Researchers have explored deep learning models for information extraction from biomedical literature and narrative clinical notes. For biomedical literature, Le et al. [24] reported an improved performance using a CRF-biLSTM neural network for NER. Habibi et al. [25] also applied a similar LSTM-CRF model and reported good performance. For narrative clinical text, Liu et al. [26] and Jagannatha et al. [27] examined Recurrent Neural Networks (RNNs) for clinical NER. We also have examined Convolutional Neural Networks (CNNs) [28] and RNNs [29] in our previous studies.
Relation extraction is a critical NLP task to understand the semantic relations between clinical concepts. [10] Compared with clinical NER, the feature selection for relation extraction is not that straightforward. Another critical challenge of relation extraction is that the searching space is very large - relation extraction systems have to consider the combinations among all clinical concepts in a document. Researchers have applied both supervised machine learning methods such as SVMs [16], kernel methods [30, 31], tree kernel methods [32], and semi-supervised machine learning methods such as Dual Iterative Pattern Relation Expansion (DIPRE) [33] for relation extraction. Most state-of-the-art relation extraction methods in the medical domain are based on machine learning models. For example, de Bruijn et al. [21] developed the best-performing relation extraction system in the 2010 i2b2 relation challenge using a maximum entropy model; Tang et al. [34] developed the best-performing temporal relation extraction system using a hybrid SVMs model in the 2012 i2b2 challenge on temporal relations; Xu et al. [35] developed the best-performing system using a customized CRFs model in the BioCreative V chemical induced disease relation challenge. Recent studies from the general NLP domain reported that deep learning models, especially CNN models based on word embeddings and positional embeddings, outperformed traditional machine learning methods on relation extraction. [10]
Previous clinical NLP challenges have designed NER tasks to extract clinical concepts such as problems, treatments, and lab tests from clinical text. For relation extraction, the i2b2 2010 challenge [11] examined the extraction of treatment relation, test relation (test conducted to investigate medical problems), and medical problem relation (medical problems that describe or reveal aspects of the same medical problem, e.g., Azotemia presumed secondary to sepsis); the i2b2 2012 challenge [12] examined the temporal relation (how medical events related to each other in the clinical timeline, e.g., before, after). In 2015, the BioCreative V open challenge [36] organized a relation extraction task to extract Chemical Disease Relation (CDR) from biomedical literature. In 2018, the University of Massachusetts Medical School organized an NLP challenge for detecting Medication and Adverse Drug Events from electronic health records (MADE1.0). MADE1.0 challenge has three sub-tasks: 1) a clinical NER task to extract medications, ADEs and their attributes; 2) a relation extraction task to extract relations among the detected clinical concepts; and 3) an integrated task that combines sub-tasks 1) and 2). To the best of our knowledge, this is the first open challenge on extracting medications, ADEs, and their relations from a large clinical corpus. The CDR task of BioCreative V is related to this challenge, but it focused on the chemical induced diseases from biomedical literature. In this article, we present the Medication and Adverse Drug Events Extraction system (MADEx) developed for the MADE1.0 challenge. MADEx consists of two modules: 1) a clinical NER module to recognize medication names and attributes (dosage, frequency, route, duration), as well as ADEs, indications, other signs and symptoms; 2) a relation extraction module to identify relations between medications and attributes, as well as relations between medications and ADEs, indications and other signs and symptoms. MADEx achieved a top three best performance for the NER task using a deep learning method, demonstrating the effectiveness of deep learning approaches.
2. Methods
2.1. Dataset
The MADE1.0 organizers developed a corpus for clinical NER and relations extraction using a total number of 1,089 de-identified clinical notes. Annotators labeled medications and their attributes, ADEs, indications, other signs and symptoms, and relations among them. A total number of 79,114 entities and 27,175 relations were annotated and represented using the BioC format [37]. The relations were annotated at the document level that may cross multiple sentences. The corpus was divided into a training set of 876 notes and a test set of 213 notes. Table 1 shows the overall statistics and Table 2 provides detailed distribution of relations among all relation types for the training set and test set.
Table 1.
Overall statistics of datasets.
| Dataset | Notes | Entities | Relations |
|---|---|---|---|
| Training | 876 | 67,781 | 23,047 |
| Test | 213 | 11,333 | 4,128 |
Table 2.
Distribution of relations in the training and the test.
| Relation | Entity 1 | Entity 2 | Counts |
|
|---|---|---|---|---|
| Training | Testing | |||
| adverse | Drug | ADE | 2,055 | 511 |
| do | Drug | Dose | 5,150 | 863 |
| du | Drug | Duration | 901 | 146 |
| fr | Drug | Frequency | 4,407 | 728 |
| manner/route | Drug | Route | 2,544 | 454 |
| reason | Drug | Indication | 4,530 | 871 |
| severity_type | SSLIF | Severity | 2,909 | 390 |
| severity_type | ADE | Severity | 282 | 37 |
| severity_type | Indication | Severity | 269 | 128 |
do: dose relation between a drug and its dose; du: Duration; fr: Frequency.
2.2. The MADEx system
MADEx applied machine learning methods to extract clinical concepts and their relations. We developed a Recurrent Neural Network (RNN)-based clinical NER module using the Long Short Term-Memory (LSTM) strategy [38] with a CRFs layer – the LSTM-CRFs model. [39] We also implemented standard deep learning techniques including bi-directional LSTM, character-level embedding, and dropout. Using different training strategies, we developed two LSTM-CRFs models and compared them with a CRFs - another widely used machine learning methods for NER. For relation extraction module, we first developed heuristic rules to generate candidate pairs from the detected clinical concepts and then applied a hybrid SVMs model to determine whether there is a relation between the entities and classify the relation types. We compared two widely used machine learning models for relation classification - SVMs and Random Forests (RFs). For the integrated task, we developed an NLP pipeline to integrate the two modules into a unified system. We describe the details in the following sections.
2.2.1. NER Module
The Workflow of NER
Figure 1 shows the workflow of NER module. The NER module consists of a pre-processing pipeline, a machine learning-based clinical NER, and a post-processing pipeline. The pre-processing pipeline performed sentence boundary detection and tokenization to nonnalize the raw clinical notes. Since the sentence boundary detection and tokenization will change the offsets (the start and end position of clinical concepts in the clinical text), the NER module tracked all the entities’ offset using position mapping files. As the training data was provided using the BioC format [37], but the machine learning requires BIO format, we developed a pipeline to convert the annotation from BioC to BIO. The NER algorithm scanned the normalized notes and detected clinical concepts using pre-trained machine learning models. The post-processing pipeline mapped the detected clinical concepts back to its original position, converted the predictions to BioC format, and dumped the results to XML files.
Figure 1.
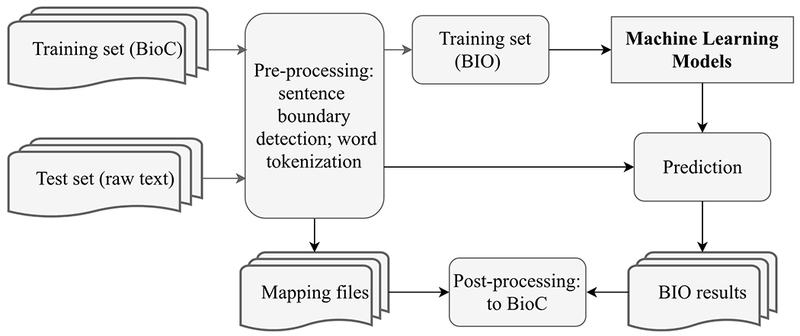
The workflow of NER module.
Machine Learning-based NER Methods
We applied a state-of-the-art deep learning-based NER method - the LSTM-CRFs [39] and compared it with another widely used machine learning method - CRFs.
LSTM-CRFs Model
The LSTM-CRFs model is a special implementation of RNNs designed for sequential data that composed of consecutive vectors. Different from other feed-forward neural networks, RNNs have loops in their network architectures, which enable RNNs to utilize the long-distance dependencies from previous information. Up until now, the RNNs implemented using the LSTM strategy is reported to be the state-of-the-art method for NER. The LSTM implementation designed several computational functions to control the mixing of previous information with current information. In this study, we adopted an LSTM-CRFs architecture from Lample et al. [39] with the following implementation:
| (1) |
| (2) |
| (3) |
| (4) |
The LSTM-CRFs model has a character level embedding layer, a character level bi-directional LSTM layer, a word embedding layer, a word-level bi-directional LSTM layer and a CRFs layer for sequence labeling. To handle unknown words, we collected the low-frequency words (words that appeared only once in the training) and dynamically assigned them as ‘unknown’ according to a probability of 0.5 during training. More specifically, before feeding a sentence for training, we randomly generated a probability between 0 and 1 for each of the low-frequency words. According to the probability, we either replaced the low-frequency word as ‘unknown’ (probability > 0.5) or kept it unchanged (probability <= 0.5). Thus, we were able to train the embedding for ‘unknown’. During prediction, we replaced all the words that not covered by the training corpus as ‘unknown’. For the training of LSTM layers, we didn’t use the sentence start and end paddings. But we considered the transition probability from the sentence start to a word and the transition probability from the last word to the sentence end in the CRFs layer. The training strategy of our system is different from the typical LSTM-CRFs. The typical training procedure split part of the training as a validation and selected the best model according to the performance on the pre-split validation set. We developed a two-stage training procedure, including a stage-1 to optimize the model parameters according to the performance on the pre-split validation set; and stage-2 to merge the pre-split validation set back to the training set and retrain a new model using the parameters and stop iterations optimized by stage-1. The typical training of LSTM-CRFs was able to find a local maximum, but it had less training samples as part of the training samples were split for validation. Our training strategy kept more samples in training (as we merged the validation back to training at stage-2) but the final model may not be at a local maximum. Our assumption is that keeping more samples in training may be important than finding a local maximum.
CRFs Model
CRFs is another popular machine learning model for clinical NER as it is intrinsically designed for sequence labeling problem by modeling the relationships between neighbor tokens in the sequence. In this study, we utilized the CRFs algorithm implemented in the CRFsuite library (http://www.chokkan.org/software/crfsuite/). We used machine learning features that reported to be useful for clinical NER in previous studies, including word n-grams, prefixes, suffixes, word shape (combination patterns of uppercase and lowercase letters, numbers), sentence-level features (sentence length, whether the sentence is a part of list), brown clustering, and discrete word embedding. [40, 41] The discrete word embedding features were derived by converting the real numbers in the word embedding into discrete categories in [POSITIVE, NEGATIVE, NEUTRAL]. For each dimension of word embedding, we calculated the positive mean value – the arithmetic mean among all positive values of this dimension, and the negative mean – the arithmetic mean among all negative values of this dimension. For each value in this dimension, we compared it with the positive mean and negative mean. If the value is bigger than the positive mean, we replaced it as ‘POSITIVE’; if less than the negative mean, we replaced it as ‘NEGATIVE’. The values between the negative mean and the positive mean were replaced as ‘NEUTRAL’. We trained CRFs models using all 876 notes in the training set and optimized the parameters using 5-fold cross-validation.
2.2.2. Relation Extraction Module
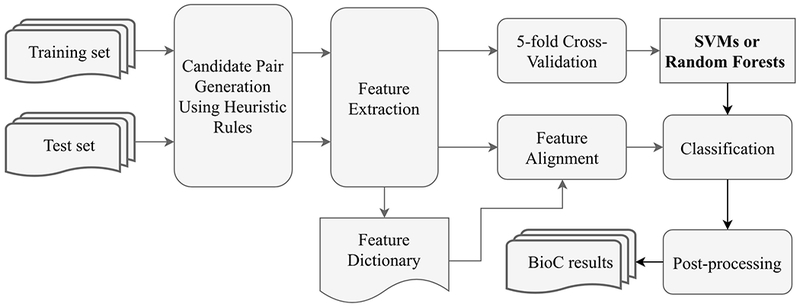
Given clinical concepts, the goal of the relation extraction module is to determine whether there is a relation among the concepts and to identify the relation types. We approached relation extraction as a classification task with each relation type as an individual class. In this study, there are a total number of eight classes, including seven classes shown in table 2 and a ‘non-relation’ class denoting there is no relation between entities. The relation extraction module consists of three parts: a pre-processing pipeline, a classifier, and a post-processing pipeline. Figure 2 shows the workflow of relation extraction module. The pre-processing pipeline generated candidate pairs of clinical concepts using heuristic rules based on the permutation among all concepts. Then, the classifier assigned one of the eight classes for each candidate pair. Next, the post-processing pipeline converted the classification results to BioC format.
Figure 2.
The workflow of relation extraction module.
Heuristic Rules to Generate Concept Pairs
One of the critical challenges of relation extraction is that it has to consider the permutations among all clinical concepts in the document level. However, this often brings too many negative samples causing imbalanced positive/negative sample sizes. We developed the following heuristic rules to control the generation of candidate pairs:
Rule 1. Two clinical concepts occurred in the same sentence or two consecutive sentences will be considered as a candidate pair and continue to Rule 2; otherwise, stop;
Rule 2. For each of the pairs generated in Rule 1, if the entity types of the two concepts fall into any possible combinations shown in Table 2, it will be a candidate pair for classification; otherwise, stop;
We divided the candidate pairs generated by the heuristic rules into a set of single-sentence pairs and a set of cross-sentence pairs and developed a single-sentence classifier and a cross-sentence classifier, respectively.
Handle single-sentence relations and cross-sentence relations
Since relations were annotated at the document level, they may occur within a single sentence or cross multiple sentences. We compared two relation extraction strategies, including 1) one-classifier model for all relations; and 2) separate-classifier - one classifier for single-sentence relations and another classifier for cross-sentence relations.
Machine Learning-based Relation Extraction Methods
We explored two machine learning methods to classify the relation types, including SVMs and RFs. The two machine learning models were widely used in various classification tasks and demonstrated good performance. We used the SVMs algorithm implemented in the LIBSVM-3.22 package [42] and RFs algorithm implemented in the sciki-learn library (http://scikit-learn.org). We extracted features including 1) the local context information including words inside of each entity; 2) the distance between two clinical concepts in number of characters and in number of words; 3) unigram, bigram, and trigram before and after each entity; 4) semantic information such as the entity types of the two entities in a relation and other entities occurred in this sentence and their entity types. We optimized the features and parameters using a grid searching based on 5-fold cross-validation. For SVMs, we tuned the regularizer c and the tolerance of termination criterion e. All other parameters were set as the default. For RFs, we tuned the number of trees (n_estimators), the maximum features to include (max_features). The Gini impurity method was utilized as the tree splitting function.
2.2.3. Integrated Pipeline
We integrated the NER module and the relation extraction module into a unified pipeline that can extract clinical concepts and their relations together from clinical text. In the integrated pipeline, the relation extraction module performs relation extraction based on clinical concepts detected by the NER module.
2.3. Experiments and Evaluation
Typically, the training of deep learning models requires a validation set to optimize parameters. Therefore, we divided the original training set of 876 notes into a short-training set of 776 notes and a validation set of the rest 100 notes. We trained a LSTM-CRFs model using the short-training set and optimized the parameters according to the performance on the validation set, denoting as RNN-1. Then, we combined the short training set and the validation set and retrained another LSTM-CRFs model according to the parameters optimized in RNN-1, denoting as RNN-2. In the training of LSTM-CRFs, we only used pre-trained word embeddings provided by the MADE1.0 organizers without any feature engineering. The character embedding layer is randomly initialized and updated along the training progress. According to the performance on the validation set, the parameters of LSTM-CRFs model were optimized as: the character embedding dimension was 25, the bidirectional word-level LSTM had an output dimension of 200; and the bi-directional character-level LSTM had an output size of 25; the learning rate fixed at 0.005; the input layer for the word-level LSTM applied a dropout at probability of 0.5; the stochastic gradient descending applied a gradient clapping at [−5.0,5.0]. Using the optimized parameters, we trained another LSTM-CRFs model RNN-2 using the entire training set (876 notes). For relation extraction, we optimized the SVMs using cross validation. We excluded the bigram and trigram features for the RFs model as the cross-validation results showed a drop of 0.08 on the F1-score.
We used F1-score, precision, and recall to evaluate the performance of clinical NER and relation extraction. As both of the two tasks have multiple classes, we calculated the micro-average scores over all classes for evaluation. For clinical NER, we used the strict scores - both the offsets and the semantic type of a concept have to be exactly the same as those in the gold standard. All evaluation scores were calculated using the official evaluation scripts provided by the event organizer.
3. Results
3.1. Clinical NER
Table 3 shows the best performance of LSTM-CRFs and CRFs on the validation set of 100 notes and the test set of 213 notes. Using only the word embeddings provided by the organizer, the RNN-1 achieved the best F1-score of 0.8897, outperforming the CRFs model of 0.8377 on the validation set. We were unable to evaluate RNN-2 model as the validation set was merged in order to train the RNN-2. On the test set, RNN-2 achieved the best F1-score of 0.8233, outperforming the RNN-1 of 0.8134 and the CRFs of 0.7250. Both RNN-1 and RNN-2 outperformed the baseline CRFs model by about 0.1 in terms of strict F1-score. The LSTM-CRFs model improved on both the precision and recall compared with CRFs.
Table 3.
The NER performances on the validation and test.
| Model | Dataset | Performance |
||
|---|---|---|---|---|
| Precision | Recall | F1-score | ||
| CRFs | Validation | 0.8555 | 0.8207 | 0.8377 |
| RNN-1 | 0.8893 | 0.8900 | 0.8897 | |
| CRFs | Test | 0.6618 | 0.8015 | 0.7250 |
| RNN-1 | 0.8034 | 0.8236 | 0.8134 | |
| RNN-2 | 0.8149 | 0.8318 | 0.8233 | |
Table 4 shows detailed evaluation scores of the best performing NER model, RNN-2, for each entity type on the test data. The RNN-2 achieved a good F1-scores for most of the nine entity types. However, the F1-scores (0.6135 and 0.6052, respectively) for Indication and ADE are lower than other entity types. Although the recalls of both Indication and ADE are decent (around 0.75), the precisions are notably low (around 0.5).
Table 4.
Performances of RNN-2 on the test set for each entity type.
| RNN-2 | Performance |
||
|---|---|---|---|
| Entity Category | Precision | Recall | F1-score |
| Drug | 0.8597 | 0.9003 | 0.8795 |
| Indication | 0.5142 | 0.7605 | 0.6135 |
| Frequency | 0.8467 | 0.8638 | 0.8552 |
| Severity | 0.7509 | 0.7832 | 0.7667 |
| Dose | 0.8815 | 0.8393 | 0.8592 |
| Duration | 0.6466 | 0.7890 | 0.7107 |
| Route | 0.8869 | 0.9274 | 0.9067 |
| ADE | 0.5104 | 0.7432 | 0.6052 |
| SSLIF | 0.8468 | 0.8319 | 0.8232 |
SSLIF: Other sign, symptoms and diseases that is not an ADE or Indication.
3.2. Relation Extraction
Using the heuristic rules, we derived a total number of 64,783 single-sentence relation pairs, where 18,948 of them (29.2%) are positive samples and 45,835 (70.8%) of them are negative samples. For cross-sentence relations, we only considered relations cross two sentences as considering more than two sentences generated too many negative samples. Using the same heuristic rules, we derived a total number of 31,406 cross-sentence relations, where 2,814 of them (9%) are positive samples and 28,592 (91%) of them are negative samples. We compared the one-classifier strategy, where a unified SVMs model was trained to handle all relations, with a separate-classifier strategy, where two SMVs models were trained - one for single-sentence relations and another for cross-sentence relations. The two models were optimized using 5-fold cross-validation on the training set. Table 5 compares the performance of the two strategies on the test set. The separate-classifier outperformed one-classifier. Then, we compared two machine learning models including SVMs and RFs using the separate-classifier strategy. Table 6 summarizes the best micro-average scores for the SVMs and RFs using both 5-fold cross-validation on the training as well as the final scores when applied to the test. The RFs model achieved the best micro-average F1-score of 0.9360 using cross-validation on the training set, outperforming the SVMs model of 0.9247. However, the SVMs model achieved the best micro-average F1-score of 0.8466 on the test set.
Table 5.
Comparison between one-classifier and separate-classifier for relation extraction on test data.
| Model | Performance |
||
|---|---|---|---|
| Precision | Recall | F1-score | |
| One-classifier (SVMs) | 0.8367 | 0.8242 | 0.8304 |
| Separate-classifier (SVMs) | 0.8491 | 0.8441 | 0.8466 |
Table 6.
Relation extraction performances on the training and the test using separate-classifier.
| Model | Expr. | Performance |
||
|---|---|---|---|---|
| Precision | Recall | F1-score | ||
| SVMs | Training | 0.91990 | .92960 | .9247 |
| RFs | 0.9432 | 0.9289 | 0.9360 | |
| SVMs | Test | 0.8491 | 0.8441 | 0.8466 |
| RFs | 0.8174 | 0.8505 | 0.8337 | |
Table 7 shows the precision, recall and F1-score of the SVMs model for each relation type on the test. The SVMs model achieved good F1-scores (~ 0.9) for severity_type, manner/router, do, and fr. Yet, the F1-scores for reason, du, and adverse are relatively lower (between 0.7 and 0.8).
Table 7.
Relation extraction performances for SVMs by relation type on the test set. (do: dose relation between a Drug and its dose; du: Duration; fr: frequency.)
| SVM | Performance |
||
|---|---|---|---|
| Relation Type | precision | Recall | F1-score |
| severity_type | 0.8766 | 0.9333 | 0.9041 |
| manner/route | 0.9231 | 0.8660 | 0.8936 |
| reason | 0.7546 | 0.8051 | 0.7790 |
| do | 0.9342 | 0.8803 | 0.9064 |
| du | 0.8979 | 0.6139 | 0.7293 |
| fr | 0.9096 | 0.9009 | 0.9052 |
| adverse | 0.6774 | 0.7387 | 0.7067 |
3.3. The Integrated System
As the performance of SVMs and RFs are comparable for relation extraction, we developed the integrated pipeline by integrating the best NER model - RNN-2 with both of the two relation extraction methods: RNN-2+SVMs and RNN-2+RFs. Table 8 shows the performance of the two pipelines. The RNN-2+SVMs pipeline achieved a better F1-score of 0.6125, outperforming the RNN-2+RFs pipeline of 0.6033. The experimental result is consistent with relation extraction, where the SVMs model is better than RFs.
Table 8.
Performances of integrated task on the test.
| Method | Performance |
||
|---|---|---|---|
| Precision | Recall | F1-score | |
| RNN-2+SVM | 0.5758 | 0.6542 | 0.6125 |
| RNN-2+RF | 0.5597 | 0.6543 | 0.6033 |
4. Discussion
Early detection and prevention of ADEs are important for a safer and higher quality healthcare. A prerequisite of using narrative clinical text for early prevention of ADEs is to identify mentions of medications, ADEs and their relations. In this study, we presented MADEx, an NLP system to detect medications, ADEs, and their relations from clinical notes. We applied a state-of-the-art method - LSTM-CRFs for clinical NER and compared it with a traditional machine learning method - CRFs. The best LSTM-CRFs model (RNN-2) achieved a micro-average F1-score of 0.8233, outperforming the baseline CRFs model. According to the official evaluation results from organizers, our system achieved a top three best performance among 10 participating teams and 23 submitted runs in the NER task of MADE1.0 open challenge. Our results demonstrated the superior performance of the LSTM-CRFs model for clinical NER. We also developed a hybrid relation extraction module using SVMs and compared it with another widely used machine learning model – RFs. Then, we integrated the best performing NER module - RNN-2, with an SVMs-based relation extraction module into an integrated pipeline. The post-challenge evaluation showed that the SVMs-based relation extraction module achieved a micro-average F1-score of 0.8466, outperforming an RFs-based relation extraction method; the integrated system - RNN-2+SVMs achieved a micro-average F1-score of 0.6125. The relation extraction module and the integrated pipeline of MADEx are comparable to the best performing systems in this challenge (0.8684 and 0.6170, respectively).
4.1. The NER Task
For the NER task, LSTM-CRFs outperformed a baseline CRFs (F1-score of 0.8233 vs 0.7250) using only word embeddings provided by the organizer, demonstrating the efficiency of LSTM-CRFs for clinical NER. Compared with the baseline CRFs, the LSTM-CRFs improved both precision (0.8149 vs 0.6618) and recall (0.8318 vs 0.8015). The baseline CRFs utilized human generated features that reported to be useful for NER by previous studies, however, the LSTM-CRFs only utilized word embeddings, which are numeric vectors trained from large unlabeled medical text without human intervention. The organizers trained this word embedding from three resources, including the English Wikipedia, a set of 99,700 electronic health record notes, and PubMed open access articles. [27] Deep learning models have a promise to automatically learn high-level feature representations in an unsupervised manner. Many studies [41, 43] have shown that word embeddings trained from a large corpus can capture multi-aspect semantic knowledge to improve the performance of clinical NER. Our findings are consistent with previous studies and further demonstrated the advantage of LSTM-CRFs to utilize large unlabeled corpus for clinical NER.
We developed a new modified training strategy for LSTM-CRFs in this study. The typical training of deep learning model requires a validation set to optimize the parameters. During training, researchers use the performance on the validation set to evaluate the models generated at different training iterations, choose the stop point, and select the best models for test. However, there is often no validation set provided in some real-life applications, such as this challenge. A typical solution is to split a proportion of notes from the original training as validation. Thus, the original training becomes a short-training set. This study proposed and examined a new training strategy – after optimizing the parameters using the short-training, we merged the validation set into the short-training set and retrained a new model using the optimized parameters. The traditional training strategy was able to find a local maximum but has less training samples, whereas, our new training strategy was able to explore more training samples, but the final model might not be at a local maximum. The experimental results showed that the RNN-2 model (F1-score of 0.8233) trained using the new strategy outperformed the RNN-1 (F1-score of 0.8134) trained using the traditional short-training, indicating that having more samples in training may be more important than finding a local maximum. Further investigation should examine the effect of corpus size and local maximum selection.
4.2. The Relation Extraction Task
Relation extraction is a critical NLP task to understand the relations between clinical concepts. We developed an SVMs-based relation extraction module and compared it with RFs. Two SVMs-based models were developed for the single-sentence pairs and the cross-sentence pairs. As shown in Table 6, RFs achieves a better F1-score than SVMs using cross-validation on the training. The performance of both SVMs and RFs dropped when applying them to the test set. SVMs outperformed the RFs on the final test set by >0.01 in term of F1-score, indicating that SVMs may be more generalizable than the RFs for relation extraction. Further investigation should examine the differences.
We were not able to finish the relation extraction module and the integrated pipeline during the challenge. The post-challenge evaluation using the official evaluation scripts showed that the relation extraction module of MADEx outperformed the second-best system (about 0.02 lower than the best system [44] on F1-score) on relation extraction task and our integrated system, RNN-2+SVMs, outperformed the second-best system on integrated task (0.0045 lower than the best system [45]). Our MADEx system is comparable to the best performing systems for relation extraction and integrated task in this challenge. The top-performing system for the integrated task in this challenge achieved a micro-average F1-score around 0.61, indicating that the integrated task of extracting entity and relation together from clinical text remains a challenging problem. Relation extraction is challenging for several reasons. First, relations are annotated at document level and there are relations annotated across multiple sentences. Thus, the relation extraction systems have to consider the combinations between all clinical concepts within a document. Second, compared to the word level applications such as clinical NER, the features for relation extraction are not that straightforward. Similar to our previous studies on relation extraction [34], we developed heuristic rules to generate candidate pairs to control the ratio between negative samples and positive samples. For cross-sentence relations, MADEx only considered relations within two consecutive sentences. Although it excluded the relations across >2 sentences, this strategy provided a reasonable positive/negative sample ratio. We also tried to include the relations across >2 sentences, however, it brought more noises to the training set and caused a serious imbalance issue.
4.3. Error Analysis and Future Work
As shown in table 4, the performance scores of NER are notably lower for ADE and Indication compared to other entity types. We analyzed errors for the two entity types. Some false negatives were caused by boundary mismatching or misclassification of semantic types. For example, a common type of error for ADE and Indication is to misclassify them as SSLIF. This may be caused by the limited number of training samples (ADE and Indication only accounted for about 2% and 5% of the total number of entities, respectively). Some entities were annotated with two different semantic categories and our NER module could not handle them correctly. For example, the entity “attention and concentration span has decreased” is annotated both as ADE and SSLIF. There were also complex entities such as “nodular-sclerosing stage IIa Hodgkin disease”, which was annotated as Indication and part of it, “stage IIa, was annotated as Severity. Our NER module was able to extract entities “nodular-sclerosing” as SSLIF, “stage IIa” as Severity, and “Hodgkin disease” as Indication but failed to detect the whole sequence as an Indication.
For relation extraction task, the adverse, reason, and du have notably lower F1-scores compared to other relation types as shown in Table 6. Part of the reason is that clinical concepts from the ‘adverse’ category are very similar to clinical concepts from ‘reason’. Since the entities of ADE, Indication, and SSLIF tend to have similar contexts, it’s hard to discriminate the relation types using only the contextual information. For ‘du’ category, the limit number of training samples is the main problem (‘du’ accounts for only 4% of the total relations).
We will continue to improve the performance of MADEx in our future work. To improve the performance of detecting ADE and Indication concepts, we plan to develop new methods to integrate medical knowledge with corpus-based word embeddings to help distinguish between the two categories. [46] We also plan to design post-processing rules to improve the NER module on detecting complex entities. The new methods to integrate medical knowledge with corpus-based word embedding will also help distinguish among different relation types. The Convolutional Neural Networks (CNNs) have demonstrated good performance for relation extraction, which is our next focus. We will also explore the joint learning models that perform NER and relation extraction in a unified model.
5. Conclusion
In this study, we presented MADEx, a machine learning based NLP system to detect medications, ADEs, and their relations from clinical text. MADEx consists of a clinical NER module implemented using LSTM-CRFs and a relation extraction module implemented using SVMs. MADEx achieved top three best performance on the NER task of MADE1.0 challenge, demonstrating the efficiency of LSTM-CRFs for clinical NER. The post-challenge evaluation showed that the relation extraction module and integrated pipeline of MADEx are comparable to the best-performing systems developed in this challenge.
Key Points.
Combine recurrent neural networks and support vector machines in a hybrid system achieved good performance in detecting medications, adverse drug events, and their relations from clinical notes.
Deep learning models are able to learn high-level feature representations without human intervention.
When there is no validation data provided, having more samples in training may be more important than finding a local maximum.
Acknowledgements
We would like to thank the organizers to provide the annotated corpus and word embeddings for this challenge. We gratefully acknowledge the support of NVIDIA Corporation with the donation of the GPUs used for this research. The authors thank the reviewers for their helpful feedback.
Funding
This study was supported in part by the University of Florida Clinical and Translational Science Institute, which is funded by the National Institutes of Health (NIH) National Center for Advancing Translational Sciences under award number UL1TR001427, and the OneFlorida Clinical Research Consortium, which is funded by the Patient-Centered Outcomes Research Institute (PCORI) under award number CDRN-1501-26692. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Conflict of interest
Xi Yang, Jiang Bian, Yan Gong, William R. Hogan, Yonghui Wu have no conflicts of interest that are directly relevant to the content of this study.
Ethics considerations
This study utilized de-identified clinical notes provided by the University of Massachusetts Medical School through MADE1.0 challenge. This study was approved by the University of Florida Institutional Review Board.
References
- 1.Institute of Medicine (US) Committee on Quality of Health Care in America (2000) To Err is Human: Building a Safer Health System. National Academies Press (US), Washington (DC) [PubMed] [Google Scholar]
- 2.Weiss AJ, Freeman WJ, Heslin KC, Barrett ML (2018) Adverse Drug Events in U.S. Hospitals, 2010 Versus 2014. AHRQ, STATISTICAL BRIEF #234 [Google Scholar]
- 3.Stausberg J (2014) International prevalence of adverse drug events in hospitals: an analysis of routine data from England, Germany, and the USA. BMC Health Serv Res 14:125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Poudel DR, Acharya P, Ghimire S, Dhital R, Bharati R (2017) Burden of hospitalizations related to adverse drug events in the USA: a retrospective analysis from large inpatient database. Pharmacoepidemiol Drug Saf 26:635–641 [DOI] [PubMed] [Google Scholar]
- 5.Aljadhey H, Mahmoud MA, Mayet A, Alshaikh M, Ahmed Y, Murray MD, Bates DW (2013) Incidence of adverse drug events in an academic hospital: a prospective cohort study. Int J Qual Health Care J Int Soc Qual Health Care 25:648–655 [DOI] [PubMed] [Google Scholar]
- 6.Aljadhey H, Mahmoud MA, Ahmed Y, et al. (2016) Incidence of adverse drug events in public and private hospitals in Riyadh, Saudi Arabia: the (ADESA) prospective cohort study. BMJ Open 6:e010831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wang Y, Wang L, Rastegar-Mojarad M, et al. (2018) Clinical information extraction applications: A literature review. J Biomed Inform 77:34–49 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Meystre SM, Savova GK, Kipper-Schuler KC, Hurdle JF (2008) Extracting information from textual documents in the electronic health record: a review of recent research. Yearb Med Inform 128–144 [PubMed] [Google Scholar]
- 9.Nadkarni PM, Ohno-Machado L, Chapman WW (2011) Natural language processing: an introduction. J Am Med Inform Assoc JAMIA 18:544–551 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kumar S (2017) A Survey of Deep Learning Methods for Relation Extraction. ArXiv170503645 Cs [Google Scholar]
- 11.Uzuner Ö, South BR, Shen S, DuVall SL (2011) 2010 i2b2/VA challenge on concepts, assertions, and relations in clinical text. J Am Med Inform Assoc JAMIA 18:552–556 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sun W, Rumshisky A, Uzuner O (2013) Evaluating temporal relations in clinical text: 2012 i2b2 Challenge. J Am Med Inform Assoc JAMIA 20:806–813 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pradhan S, Elhadad N, Chapman W, Manandhar S, Savova G SemEval-2014 Task 7: Analysis of Clinical Text. 9 [Google Scholar]
- 14.Pradhan S, Elhadad N, South BR, Martinez D, Christensen L, Vogel A, Suominen H, Chapman WW, Savova G (2015) Evaluating the state of the art in disorder recognition and normalization of the clinical narrative. J Am Med Inform Assoc JAMIA 22:143–154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lafferty JD, McCallum A, Pereira FCN (2001) Conditional Random Fields: Probabilistic Models for Segmenting and Labeling Sequence Data In: Proc. Eighteenth Int. Conf. Mach. Learn. Morgan Kaufmann Publishers Inc, San Francisco, CA, USA, pp 282–289 [Google Scholar]
- 16.Hearst MA, Dumais ST, Osuna E, Platt J, Scholkopf B (1998) Support vector machines. IEEE Intell Syst Their Appl 13:18–28 [Google Scholar]
- 17.Tsochantaridis I, Joachims T, Hofmann T, Altun Y (2005) Large Margin Methods for Structured and Interdependent Output Variables. J Mach Learn Res 6:1453–1484 [Google Scholar]
- 18.Aronson AR, Lang F-M (2010) An overview of MetaMap: historical perspective and recent advances. J Am Med Inform Assoc JAMIA 17:229–236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Friedman C (1997) Towards a comprehensive medical language processing system: methods and issues. Proc Conf Am Med Inform Assoc AMIA Fall Symp 595–599 [PMC free article] [PubMed] [Google Scholar]
- 20.Denny JC, Irani PR, Wehbe FH, Smithers JD, Spickard A (2003) The KnowledgeMap project: development of a concept-based medical school curriculum database. AMIA Annu Symp Proc AMIA Symp 195–199 [PMC free article] [PubMed] [Google Scholar]
- 21.de Bruijn B, Cherry C, Kiritchenko S, Martin J, Zhu X (2011) Machine-learned solutions for three stages of clinical information extraction: the state of the art at i2b2 2010. J Am Med Inform Assoc JAMIA 18:557–562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhang Y, Wang J, Tang B, Wu Y, Jiang M, Chen Y, Xu H (2014) UTH_CCB: a report for semeval 2014–task 7 analysis of clinical text. SemEval 2014 802 [Google Scholar]
- 23.Tang B, Wu Y, Jiang M, Denny JC, Xu H Recognizing and Encoding Disorder Concepts in Clinical Text using Machine Learning and Vector Space Model. 8 [Google Scholar]
- 24.Le H-Q, Nguyen TM, Vu ST, Dang TH (2018) D3NER: Biomedical named entity recognition using CRF-biLSTM improved with fine-tuned embeddings of various linguistic information. Bioinforma Oxf Engl. doi: 10.1093/bioinformatics/bty356 [DOI] [PubMed] [Google Scholar]
- 25.Habibi M, Weber L, Neves M, Wiegandt DL, Leser U (2017) Deep learning with word embeddings improves biomedical named entity recognition. Bioinforma Oxf Engl 33:i37–i48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Liu Z, Yang M, Wang X, Chen Q, Tang B, Wang Z, Xu H (2017) Entity recognition from clinical texts via recurrent neural network. BMC Med Inform Decis Mak. doi: 10.1186/s12911-017-0468-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jagannatha AN, Yu H (2016) Bidirectional RNN for Medical Event Detection in Electronic Health Records. Proc Conf Assoc Comput Linguist North Am Chapter Meet 2016:473–482 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wu Y, Jiang M, Lei J, Xu H (2015) Named Entity Recognition in Chinese Clinical Text Using Deep Neural Network. Stud Health Technol Inform 216:624–628 [PMC free article] [PubMed] [Google Scholar]
- 29.Wu Y, Jiang M, Xu J, Zhi D, Xu H (2017) Clinical Named Entity Recognition Using Deep Learning Models. AMIA Annu Symp Proc [PMC free article] [PubMed] [Google Scholar]
- 30.Zhao S, Grishman R (2005) Extracting Relations with Integrated Information Using Kernel Methods In: Proc. 43rd Annu. Meet. Assoc. Comput. Linguist. Association for Computational Linguistics, Stroudsburg, PA, USA, pp 419–426 [Google Scholar]
- 31.Tikk D, Thomas P, Palaga P, Hakenberg J, Leser U (2010) A comprehensive benchmark of kernel methods to extract protein-protein interactions from literature. PLoS Comput Biol 6:e1000837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Zelenko D, Aone C, Richardella A (2003) Kernel Methods for Relation Extraction. J Mach Learn Res 3:1083–1106 [Google Scholar]
- 33.Brin S (1999) Extracting Patterns and Relations from the World Wide Web In: Sel. Pap. Int. Workshop World Wide Web Databases. Springer-Verlag, London, UK, UK, pp 172–183 [Google Scholar]
- 34.Tang B, Wu Y, Jiang M, Chen Y, Denny JC, Xu H (2013) A hybrid system for temporal information extraction from clinical text. J Am Med Inform Assoc JAMIA 20:828–835 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Xu J, Wu Y, Zhang Y, Wang J, Lee H-J, Xu H (2016) CD-REST: a system for extracting chemical-induced disease relation in literature. Database. doi: 10.1093/database/baw036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wei C-H, Peng Y, Leaman R, Davis AP, Mattingly CJ, Li J, Wiegers TC, Lu Z (2016) Assessing the state of the art in biomedical relation extraction: overview of the BioCreative V chemical-disease relation (CDR) task. Database J Biol Databases Curation. doi: 10.1093/database/baw032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Comeau DC, Islamaj Doğan R, Ciccarese P, et al. (2013) BioC: a minimalist approach to interoperability for biomedical text processing. Database J Biol Databases Curation. doi: 10.1093/database/bat064 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hochreiter S, Schmidhuber J (1997) Long short-term memory. Neural Comput 9:1735–1780 [DOI] [PubMed] [Google Scholar]
- 39.Lample G, Ballesteros M, Subramanian S, Kawakami K, Dyer C (2016) Neural Architectures for Named Entity Recognition. ArXiv160301360 Cs [Google Scholar]
- 40.Soysal E, Wang J, Jiang M, Wu Y, Pakhomov S, Liu H, Xu H (2017) CLAMP - a toolkit for efficiently building customized clinical natural language processing pipelines. J Am Med Inform Assoc JAMIA. doi: 10.1093/jamia/ocx132 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wu Y, Xu J, Jiang M, Zhang Y, Xu H (2015) A Study of Neural Word Embeddings for Named Entity Recognition in Clinical Text. AMIA Annu Symp Proc AMIA Symp 2015:1326–1333 [PMC free article] [PubMed] [Google Scholar]
- 42.LIBSVM -- A Library for Support Vector Machines. https://www.csie.ntu.edu.tw/~cjlin/libsvm/. Accessed 23 Jun 2018 [Google Scholar]
- 43.Collobert R, Weston J, Bottou L, Karlen M, Kavukcuoglu K, Kuksa P (2011) Natural Language Processing (Almost) from Scratch. J Mach Learn Res 12:2493–2537 [Google Scholar]
- 44.Chapman AB, Peterson KS, Alba PR, DuVall SL, Patterson OV Hybrid system for adverse drug event detection. Proceedings of Machine Learning Research 90:16–24 [Google Scholar]
- 45.Dandala B, Joopudi V, Devarakonda M IBM Research System at MADE 2018: Detecting Adverse Drug Events from Electronic Health Records. Proceedings of Machine Learning Research 90:39–47 [Google Scholar]
- 46.Bengio Y, Courville A, Vincent P (2013) Representation Learning: A Review and New Perspectives. IEEE Trans Pattern Anal Mach Intell 35:1798–1828 [DOI] [PubMed] [Google Scholar]