

Abstract
Background
Although frailty has been associated with increased risks for hospitalization and mortality in chronic heart failure, the precise average effect remains uncertain. We performed a systematic review and meta‐analysis to summarize the hazards for mortality and incident hospitalization in patients with heart failure and frailty compared with those without frailty and explored the heterogeneity underlying the effect size estimates.
Methods and Results
MEDLINE, EMBASE, and Cochrane databases were queried for articles published between January 1966 and March 2018. Predefined selection criteria were used. Hazard ratios (HRs) were pooled for meta‐analyses, and where odds ratios were used previously, original data were recalculated for HR. Overlapping data were consolidated, and only unique data points were used. Study quality and bias were assessed. Eight studies were included for mortality (2645 patients), and 6 studies were included for incident hospitalization (2541 patients) during a median follow‐up of 1.82 and 1.12 years, respectively. Frailty was significantly associated with an increased hazard for mortality (HR, 1.54; 95% confidence interval, 1.34–1.75; P<0.001) and incident hospitalization (HR, 1.56; 95% confidence interval, 1.36–1.78; P<0.001) in chronic heart failure. The Fried phenotype estimated a 16.9% larger effect size than the combined Fried/non‐Fried frailty assessment for the end point of mortality (HR, 1.80; 95% confidence interval, 1.41–2.28; P<0.001), but not for hospitalization (HR, 1.57; 95% confidence interval, 1.30–1.89; P<0.001). Study heterogeneity was found to be low (I2=0%), and high quality of studies was verified by the Newcastle‐Ottawa scale.
Conclusions
Overall, the presence of frailty in chronic heart failure is associated with an increased hazard for death and hospitalization by ≈1.5‐fold.
Keywords: chronic heart failure, frailty, hospitalization, meta‐analysis, mortality
Subject Categories: Heart Failure
Clinical Perspective
What Is New?
This meta‐analysis is the first to summarize the literature and report on a 1.5‐fold increase in the adverse outcome of death or incident hospitalization associated with frailty in patients with chronic heart failure during a follow‐up of <2 years.
The Fried phenotype, an often‐used frailty assessment scale originally developed from the Cardiovascular Health Study, estimated a higher mortality rate of 16.9% compared with that of the combined (Fried and non‐Fried) assessment, whereas the estimate for incident hospitalization was indistinct between Fried and the combined assessments.
What Are the Clinical Implications?
Since publication of “Knowledge Gaps in Cardiovascular Care of the Older Adult Population: A Scientific Statement From the American Heart Association, American College of Cardiology, and American Geriatrics Society” (2016), and the Geriatric Cardiology Council document of the American College of Cardiology (2018), there have been increasing efforts to tackle heart failure and geriatric cardiovascular disease using multidomain approaches.
The Fried phenotype is simple to use, provides prognostic information, and assesses for domain‐based physiological insufficiencies that may lend itself to daily clinical practice and screening for latent chronic heart failure.
Frailty associated with heart failure may be reversible and a target for intervention.
Introduction
Frailty is a complex systemic syndrome that has been associated with poor outcomes, including increased rates of mortality and hospitalization in frail patients with heart failure (HF) compared with those without frailty.1, 2, 3, 4, 5, 6, 7 More commonly observed in association with advanced age,1 frailty can also affect young patients with HF and can be reversible after heart transplantation8 or heart function replacement.9 Characterizing frailty status in patients with HF may provide clinicians an indicator for gauging disease severity, prognosis, and disease progression or reversal.
Although most studies have shown increased risks for hospitalization and mortality in chronic HF,2, 3, 4, 5, 6, 7 offset by 2 relatively small studies with borderline neutral results,10, 11 the precise average effect of frailty has not previously been summarized with certainty. Recently, a systematic review included a total of 8 articles from 2004 to 2014 and suggested that patients with HF and frailty had increased risks for adverse outcomes.12 However, 2 of 8 articles5, 13, 14, 15 in that study contained data from overlapping studies (ie, double counting), and no meta‐analysis was performed. Since 2014, 6 additional independent studies2, 3, 4, 11, 16, 17 with potential to be included in a meta‐analysis have been published. Recently, a systematic review and meta‐analysis has summarized data on the prevalence of HF‐associated frailty from 26 studies at 44.5% after removal of 14 overlapping studies.18 However, that study did not assess the impact or effect size of frailty on adverse outcomes, including death and hospitalization, and included patients with acute HF and those receiving cardiac resynchronization therapy, left ventricular assist device (LVAD), or heart transplant.18 In this study, we have carefully summarized the existing evidence, explored for heterogeneity, and completed the first meta‐analysis of frailty on the hazards of mortality and incident hospitalization in patients with chronic HF.
Methods
Data Sources and Search Strategy
The data that support the findings of this study are available from the corresponding author on reasonable request. From October 2016 to April 2018, we searched MEDLINE, EMBASE, and the Cochrane databases for articles published between January 1966 and March 2018. Study design (Figure 1 and Figure S1) and data reporting were compliant with MOOSE, as recommended in the EQUATOR Network guidelines.19, 20 Institutional Review Board approval was not required for this systematic review and meta‐analysis.
Figure 1.
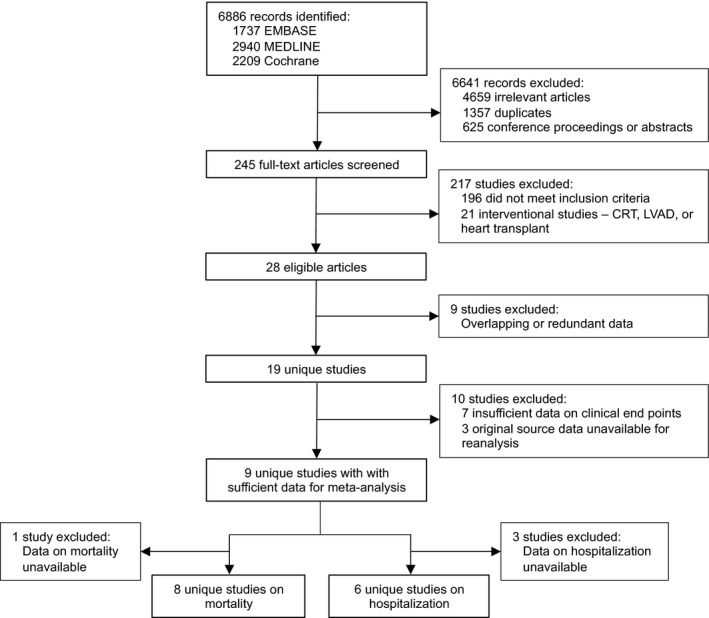
Study identification and selection. CRT indicates cardiac resynchronization therapy; LVAD, left ventricular assist device.
Eligibility Criteria
The following Medical Subject Headings or MeSH search terms were used: “frailty AND heart failure,” “frail AND heart failure,” “fragility AND heart failure,” “gait speed AND heart failure,” “grip strength AND heart failure,” “weight loss AND heart failure,” and “cognitive frailty AND heart failure.” Fragility is a term used by some European investigators with whom we have individually confirmed about its use in their publications as being synonymous with frailty for the purpose of this study. Literature search was independently performed by 2 reviewers (E.F. and X.Y.), according to a prespecified workflow. Conflicting findings were resolved by a third researcher (J.W.). The inclusion criteria were as follows: (1) frailty assessed using validated assessment instruments; (2) confirmed diagnosis of HF on the basis of international criteria and guideline definitions21, 22; (3) human individuals; and (4) articles in English. The exclusion criteria were as follows: (1) unpublished data, abstracts, conference proceedings, comments, letters, correspondences, editorials, or duplicates; (2) studies without any relevance to the clinical outcomes of hospitalization and mortality; (3) studies that investigated the effects of medical or surgical intervention, including cardiac resynchronization therapy, LVAD, and cardiac transplantation; (4) data on acute HF; and (5) non‐English articles.
Data Extraction
The main clinical outcomes in this meta‐analysis were all‐cause mortality and hospitalization. Where data on all‐cause hospitalization were not available,3 cardiac hospitalization was used. A structured data form was used to organize information2, 3, 4, 5, 6, 7, 10, 11, 13, 14, 15, 16, 17, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37 (Table1). Two reviewers (E.F. and X.Y.) extracted the raw data and independently evaluated study quality (described later).
Table 1.
Characteristics of Studies Reporting on Frailty and Chronic HF
| Source (First Author) | Reference No. | Y | Country | Study Period | Design | Type of Patients | Frailty Assessment | No. of Patients | Age, Mean±SD, y | Men, n (%) | Prevalence of Frailty, % (n/Total) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Unique studies without overlapping data | |||||||||||
| Boxerb | 5 | 2010 | United States | 2004–2005, follow‐up in 2008 | Prospective | Patients with HF, aged ≥60 y | Fried phenotype | 59 | 78±12 | 42 (71.2) | 25.4 (15/59) |
| Cacciatoreb, a | 6 | 2005 | Italy | 1992 | Prospective (secondary analysis) | Outpatients with HF, aged ≥65 y | Frailty staging system | 120 | 75.9±6.7 | 48 (40) | 15 (18/120) |
| Denfeld | 23 | 2017 | United States | 2015–2016 | Cross‐sectional | Inpatients and outpatients with HF | Fried frailty phenotype | 49 | 57.4±9.7 | 33 (67) | 49.0 (24/49) |
| Fergusonb, c | 16 | 2017 | Australia | 2013 | Prospective | Inpatients with HF and AF, 100% | SHARE‐FI | 137 | 72±16 | 87 (63.5) | 63 (58/92) |
| Gastelurrutiab, c | 3 | 2014 | Spain | 2001–2012 | Prospective | Outpatients with HF | CGA | 1314 | 66.7±12.4 | 950 (72.3) | 44.2 (581/1314) |
| González‐Moneo | 17 | 2016 | Spain | 2005–2010 | Prospective | Outpatients with HF | Barber questionnaire | 525 | 71±11 | 320 (61) | 55 (279/509) |
| Khandelwala | 24 | 2012 | India | N/A | Prospective (secondary analysis) | Inpatients with HF | Fried phenotype | 30 | N/A | N/A | 76.7 (23/30) |
| Madanb, c | 11 | 2016 | United States | 2011–2013 | Prospective | Outpatients with advanced HF, aged ≥65 y, with 6‐min walk distance of <300 m | Fried phenotype | 40 | 74.9±6.5 | 17 (42.5) | 65 (26/40) |
| McNallanc | 7 | 2013 | United States | 2007–2011 | Prospective | Inpatients and outpatients with HF | Fried phenotype | 448 | 73.2±13.3 | 257 (57.4) | 18.8 (84/448) |
| McNallanb | 10 | 2013 | United States | 2007–2011 | Prospective | Inpatients and outpatients with HF | Fried phenotype and deficit index | 223 | 71.1±13.9 | 135 (60.5) | 20.6 (46/223) |
| Newmana | 25 | 2001 | United States | 1989–1990 | Prospective, observational (secondary analysis) | Outpatients with HF, aged ≥65 y | Fried phenotype | 181 | N/A | N/A | 22.7 (41/181) |
| Nishiguchi | 26 | 2016 | Japan | N/A | Prospective | Patients with HF, aged ≥60 y | Fried phenotype | 206 | 73.7±7.3 | 143 (69.4) | 16.5 (34/206) |
| Parmar | 27 | 2015 | United Kingdom | N/A | Retrospective | Patients with HF, aged ≥75 y | CSHA | 261 | N/A | N/A | 75.6 (197/261) |
| Reevesa | 28 | 2016 | United States | Prospective (secondary analysis) | Patients with HF, aged ≥60 y | Fried phenotype | 136 | Stable HFpEF, 71±7; stable HFrEF, 69±5 | Stable HFpEF, 16 (20%); stable HFrEF, 37 (66%) | Stable HFpEF, 0%; stable HFrEF, N/A | |
| Rodriguez‐Pascualb, c | 2 | 2017 | Spain | 2010–2012 | Prospective | Patients with HF, aged ≥75 y, who had at least one hospitalization in the past 12 mo | Fried phenotype | 497 | 85.2±7.3 | 194 (39) | 57.5 (286/497) |
| Uchmanowicz | 29 | 2018 | Poland | 2015 | Prospective | Patients with HF, aged ≥60 y | TFI | 330 | 72.1±7.9 | 182 (55.1) | 64.8 (214/330) |
| Vidánb, c | 4 | 2016 | Spain | 2009–2011 | Prospective | Inpatients with HF, aged ≥70 y | Fried phenotype | 416 | 80±6.1 | 210 (50.5) | 76 (316/416) |
| Woodsa | 30 | 2005 | United States | 1993–1998 | Prospective (secondary analysis) | Female outpatients with HF, aged 65–79 y | Fried phenotype | 509 | N/A | 0 | 45.6 (232/509) |
| Yamada | 31 | 2015 | Japan | N/A | Prospective | Patients with HF | Modified Fried phenotype | 181 | 68.1±9.7 | 69.1 (125/181) | N/A |
| Overlapping studies with data redundancy | |||||||||||
| Altimir | 14 | 2005 | Spain | 2001 | Prospective | Outpatients with HF | CGA | 360 | 65.2±10.9 | 261 (72.5) | 41.7 (150/360) |
| Boxer | 13 | 2008 | United States | N/A | Prospective | Outpatients with HF, aged ≥60 y | Fried phenotype | 60 | 77±10 | 43 (71.7) | 25 (15/60) |
| Gastelurrutia | 32 | 2013 | Spain | 2001–2012 | Prospective | Outpatients with HF | CGA | 1405 | 66.7±12.4 | 1015 (72.2) | 44.2 (621/1405) |
| Kenny | 33 | 2006 | United States | N/A | Prospective | Patients with HF, aged ≥60 y | Fried phenotype | 59 | Men, 76±9; women, 78±12 | 41 (71.7) | 27.6 (16/59) |
| Lupón | 15 | 2008 | Spain | N/A | Prospective | Outpatients with HF | CGA | 622 | 68 (Median) | 451 (72.5) | 39.9 (248/622) |
| Pons | 34 | 2010 | Spain | 2001–2008 | Prospective | Inpatients and outpatients with HF | CGA | 960 | 69 | 681 (70.9) | 35.1 (337/960) |
| Uchmanowicz | 35 | 2015 | Poland | N/A | Prospective | Patients with HF, aged ≥60 y | TFI | 100 | Nonfrail, 62.3±6.2; frail, 67.9±10.7 | 53 (53) | 89 (89/100) |
| Uchmanowicz | 36 | 2015 | Poland | 2014 | Prospective | Patients with HF, aged ≥60 y | TFI | 110 | 66.01±11.4 | 59 (53.64) | N/A |
| Vidán | 37 | 2014 | Spain | N/A | Prospective, observational | Inpatients with HF, aged ≥70 y | Fried phenotype | 450 | 80.1±6.1 | 227 (50.4) | 70.2 (316/450) |
AF indicates atrial fibrillation; CGA, Comprehensive Geriatric Assessment (including Barthel Index, Older Americans Resources and Services Scale, Pfeiffer Test, and the abbreviated Geriatric Depression Scale); CSHA, Canadian Study of Health and Aging; HF, heart failure; HFpEF, HF with preserved ejection fraction; HFrEF, HF with reduced ejection fraction; N/A, not applicable; SHARE‐FI, Survey of Health, Ageing and Retirement in Europe–Frailty Instrument; TFI, Tilburg Frailty Indicator.
Used in meta‐analysis of mortality.
Only patients with HF were analyzed.
Used in meta‐analysis of incident hospitalization.
Data Synthesis and Statistical Analysis
The effect sizes of risks were reanalyzed and recalculated as hazards, pooled, and represented by adjusted or unadjusted hazard ratios (HRs) for the clinical outcomes of all‐cause mortality or hospitalization in frail and nonfrail patients with chronic HF. When available, all‐cause rather than cardiac hospitalization was used. This is justified by evidence in the literature that hospitalizations secondary to HF with preserved left ventricular ejection fraction (EF) are often attributable to complex comorbidities.21, 22 Of 6 studies included in the meta‐analysis of frailty on incident hospitalization, 5 used all‐cause hospitalization and 1 used cardiac hospitalization3 as end points. Where possible, adjusted, rather than unadjusted, HRs were used (Table S1).
To standardize classification of frailty/nonfrailty status, we reclassified prefrailty, a nonexistent category in some frailty assessment scales,38, 39 as nonfrailty. To minimize data redundancy and double counting,40 we contacted authors of the original studies for clarification and data reanalysis, where necessary. Among a total of 10 groups authoring 20 studies, 8 groups responded to our query with clarification and/or assisted in reanalysis (response rate, 80%). Where data redundancy from overlapping studies was suspected or in cases in which the original authors could not be reached, we proceeded to remove those articles from further analysis. The research group of Bayés‐Genís, Lupón, and Gastelurrutia consolidated their cohort data from 3 publications and reanalyzed risk estimates.3, 15, 34 Originally presented as odds ratios in the study of Vidán and colleagues,4 the risk for rehospitalization was recalculated as HRs using data from telephone interviews at 1, 3, 6, and 12 months after hospital discharge. For 66 patients in that study who did not have the exact dates of rehospitalization, the time to hospitalization was imputed using the calculated mean time to hospitalization from the remaining 340 patients. The data on mortality and hospitalization from the original article by Ferguson and colleagues were newly calculated and presented as HRs.16
Results from eligible studies were pooled and meta‐analyzed using a random‐effects model with inverse‐variance weighting. Heterogeneity of studies was assessed using Cochrane's Q statistic and I2. Prespecified I2 threshold values of 25%, 50%, and 75% were used to indicate low, moderate, and high levels of heterogeneity, respectively. A 2‐tailed P<0.05 was considered statistically significant. Analyses were performed using Review Manager 5.3 (The Cochrane Collaboration) and R 3.3.3 (R Foundation).
Assessment of Publication Bias and Study Quality
Publication bias was assessed using funnel plots and Duval‐Tweedie's trim‐and‐fill test (Figure S2).
Results
Search and Study Selection
Our query to EMBASE, MEDLINE, and Cochrane databases returned 6886 records (Figure 1 and Figure S1). After further screening and evaluation, 6641 irrelevant records and 217 ineligible full‐text articles were excluded. Among 28 eligible articles,2, 3, 4, 5, 6, 7, 10, 11, 13, 14, 15, 16, 17, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37 8 and 6 unique studies were finally included in the meta‐analysis for all‐cause mortality and incident hospitalization, respectively (Figure 1 and Table1).
Characteristics of Patients With Chronic HF
Among studies that reported on the prevalence rates of atrial fibrillation, ischemic heart disease (coronary artery disease), hypertension, and/or diabetes mellitus, the respective median prevalence rates were 53% (quartile 1–quartile3, 46.5%–62.2%), 44.5% (quartile 1–quartile 3, 26.9%–54.5%), 80% (quartile 1–quartile 3, 64.0%–87.9%), and 38.4% (quartile 1–quartile 3, 34.8%–47.0%). The median prevalence rate of frailty from 17 of 19 nonoverlapping studies was 49.0% (quartile 1–quartile 3, 21.7–64.9); data were unavailable from 2 studies.
Frailty Is Significantly Associated With Increased Mortality in Chronic HF
On the basis of data from 8 unique studies, the presence of frailty is significantly associated with an increased hazard for mortality in chronic HF (HR, 1.54; 95% confidence interval [CI], 1.34–1.75; P<0.001) (Figure 2A and Table S2). The median duration of follow‐up for 2645 patients in the 8 studies2, 3, 4, 5, 6, 10, 11, 16 was 1.82 years (quartile 1–quartile 3, 1.0–3.9 years). In studies that used only the Fried phenotype for frailty assessment (n=5 studies; Figure 2B), the effect size estimate was increased by 16.9% (HR, 1.80; 95% CI, 1.41–2.28; P<0.001; n=1127 patients).2, 4, 5, 10, 11 Irrespective of the frailty assessment instrument used, the level of study heterogeneity was low (I2=0%) (Figure 2A and 2B).
Figure 2.

Eight unique studies with nonoverlapping data. Inverse variance (IV) weighting and random‐effects model were used in the meta‐analysis. Reference number is shown after year of publication (see References for details). A, Effects of frailty on all‐cause mortality in patients with chronic heart failure (HF). B, Effects of frailty on all‐cause mortality in patients with chronic HF in 5 studies that used the Fried phenotype for frailty assessment. IV weighting and random‐effects model were used in the meta‐analysis. Reference number is shown after year of publication (see References for details). C, Effects of frailty on incident hospitalization in patients with chronic HF. Six unique studies with nonoverlapping data are shown. IV weighting and random‐effects model were used in the meta‐analysis. Reference number is shown after year of publication (see References for details). D, Effects of frailty on incident hospitalization in patients with chronic HF in 4 studies that used the Fried phenotype for frailty assessment. IV weighting and random‐effects model were used in the meta‐analysis. Reference number is shown after year of publication (see References for details). CI indicates confidence interval; df, degrees of freedom; HR, hazard ratio.
Frailty Is Significantly Associated With an Increased Rate of Hospitalization in Chronic HF
During a median follow‐up of 1.12 years (quartile 1–quartile 3, 1–2 years), the presence of frailty was significantly associated with an increased hazard for hospitalization by 56% (adjusted HR, 1.56; 95% CI, 1.36–1.78; P<0.001; n=2541 patients in 6 studies), even after adjusting for factors in the respective studies2, 3, 4, 7, 11, 16 (Figure 2C and Table S1). In 4 studies that used Fried assessment,2, 4, 7, 11 the estimate was, however, similar (adjusted HR, 1.57; 95% CI, 1.30–1.89; P<0.001; n=1142 patients) to the overall pooled estimate (Figure 2D). The level of heterogeneity between studies was also low (I2=0%) (Figure 2C and 2D).
Publication Bias and Study Quality
Although the effect size estimates for mortality fell within the pseudo 95% confidence limits of the funnel plot (Figure S2A), we proceeded to using the trim‐and‐fill test for ascertainment and found no significant difference with or without adjustment (adjusted HR, 1.48 [95% CI, 1.25–1.75] [P<0.001] 1.54 [95% CI, 1.34–1.75] [P<0.001]) (Figure S2C and Figure 2A), thereby ruling out large publication bias effects. The high quality of the included studies2, 3, 4, 5, 6, 7, 10, 11, 16 was indicated by a composite score of ≥7 on the Newcastle‐Ottawa scale41 (Table S3).
Discussion
Frailty is increasingly recognized as an important target for monitoring and intervention in contemporary cardiovascular care and management.42, 43 Clinical pathways using frailty assessment in management decision making and for determination of procedural eligibility have previously been shown to affect patient outcomes and provide prognostic indication of well‐being and survival associated with procedures, ranging from transcatheter and surgical aortic valve replacement to heart transplantation.43, 44, 45 However, the precise negative effects of frailty on chronic HF2, 3, 4, 5, 6, 7, 10, 11 have not been previously established with certainty.
This systematic review and meta‐analysis is the first to summarize the adverse impact of hospitalization and mortality associated with frailty in chronic HF. Mortality and incident hospitalization were both significantly increased by ≈1.5‐fold in >1300 patients with HF with frailty, compared with >1200 patients with HF without frailty (Figure 2). This study has reanalyzed and recalculated risk estimates as HRs, consolidated data from 3 independent sources (study cohorts from Barcelona, Spain; Madrid, Spain; and Sydney, Australia) to minimize or eliminate double counting, and focused on patients with chronic HF. Current available studies in the literature have not included any meta‐analyzed data on mortality and hospitalization associated with frailty in HF,12, 46 and frailty prevalence was the sole focus of another recently published meta‐analysis that included patients with acute decompensated HF, patients with chronic HF, and patients receiving cardiac resynchronization therapy, LVAD, and heart transplant.18
One of the major findings in this study was the higher estimate of hazard for mortality, but not incident hospitalization, by the Fried phenotype compared with the overall pooled (combined Fried and non‐Fried) estimates (Figure 2). The reason for this observation is unclear, but it can be possibly explained by the overlapping characteristics (and pathophysiological features) between functional components of the Fried phenotype (eg, progressive unintentional weight loss and weakness) and cardiac cachexia of advanced chronic HF, which carries a poor prognosis. However, the concept of cardiac cachexia cannot be simply explained by reduced body mass index alone because this relationship is complex,43 depending on the population or patient subset with HF, the cause, the pathogenesis, and the chronicity of the pathophysiological features. For instance, patients waiting for heart transplant tend to be younger, may have developed HF with reduced EF over a relatively shorter period (eg, post–viral dilated cardiomyopathy), and may have different physiological reserve levels and body composition compared with elderly patients with long‐standing, chronic HF. Older adults may have more comorbidities,47 latent chronic HF48 (particularly, HF with preserved EF), and sarcopenic obesity,49 a disorder characterized by low lean skeletal muscle mass relative to abundant intermuscular adiposity. This meta‐analysis was focused on patients with chronic HF and frailty outside the setting of heart function replacement or acute HF, acknowledging the variability in phenotypic expression of (or individuals’ variable resistance to) frailty, and its manifestation and reversibility across the HF spectrum.
The clinical phenotype proposed by Fried and colleagues38 in 2001 is based on the concept of aging‐related failure of homeostasis in physiologic systems (or domains) represented by 5 specific items: low physical activity, fatigue, shrinkage (or unintentional weight loss over a defined period), weakness, and slowness. The 5 items of the Fried phenotype are scored out a total of 5 points, with 1 point awarded for each positive item; scores of ≥3, 1 to 2, and 0 indicate subjects in frail, prefrail, and robust states, respectively. The prefrail state may be a clinically relevant indicator of underlying cardiometabolic disorder, reduced physiological reserve, and a window of opportunity for workup and intervention before development of systemic decompensation. However, the absence of prefrailty in some frailty assessment scales precluded comparison between studies for this condition. Another major frailty concept is centered on the frailty index developed by Rockwood et al.50 The frailty index is based on a cumulative multiple deficit approach, using clinical and laboratory variables with an emphasis on the number rather than type of derangements. As noted, these and other commonly used frailty assessment tools, including the modified Fried‐based FRAIL scale that obviates physical testing (eg, hand grip strength and walking tests51) with improved clinical operationality, have been previously compared in specific settings and found to perform similarly.51, 52 Other surrogate markers of frailty include gait speed,53, 54 which has been reported to offer prognostic information in patients with HF.55 Our search strategy in this study has included individual components of frailty assessment scales (see Methods) to maximize identification of articles in the literature.
A major challenge lies in the harmonization of a wide range of frailty assessment scales used in studies. Woo and coworkers have previously reported that the major frailty scales (frailty index by Rockwood and Mitnitski, Fried phenotype from the Cardiovascular Health Study, FRAIL scale, and the Hubbard modified frailty score) perform similarly in predicting death and physical limitation in a geriatric study population.51 Chong and colleagues found that several frailty assessment instruments (frailty index, FRAIL scale, Tilburg Frailty Index, and Clinical Frailty Scale) tested did not significantly differ in their ability to diagnose frailty.52 Those findings suggest that pooling of studies for meta‐analysis can be feasible and informative for the specific purpose of this study, as supported by available evidence in the literature.
HF and aging‐related frailty share common signs, symptoms, and manifestations, including sarcopenia or skeletal muscle weakness, impaired cardiorespiratory and physical fitness, increased inflammatory burden,56 and central nervous system dysfunction.57, 58 Although definitions and assessment scales do vary, there has been impetus toward a universal definition of frailty in the geriatric professional community.1, 59, 60 Currently, frailty is not routinely assessed for or systematically categorized in patients with HF.1, 21, 22, 42, 61 However, findings from this and other studies encourage the use of frailty assessment for risk stratification of patients with HF to inform prognosis and management decisions. Recent data from the LVAD and heart transplant literature suggest that frailty in patients with advanced HF can be reversed by intervention or organ replacement8, 43 and that frailty is not necessarily age or functional class related,18 suggesting that inclusion of frailty assessment in patients with HF can inform outcomes. Indeed, Jha and colleagues have shown that pre‐LVAD or pretransplant frailty status has a significant impact on survival after LVAD implantation or heart transplantation.43
There are several limitations in this study. First, the competing risks between hospitalization and mortality across time could not be assessed given the limitations inherent in the original studies.62 Second, hospitalization as an outcome measure is complex and may be HF associated, cardiac related, or unrelated to cardiovascular events.63, 64 Details on hospitalization and contemporary metrics (eg, 30‐day readmission and length of stay) for characterizing hospitalization were unavailable from the included studies. Future studies using standardized metrics may improve accuracy of risk estimates. Third, there were insufficient data in the available articles to perform a meta‐analysis on HF subtypes (eg, HF with reduced EF and HF with preserved EF).21, 22 Although some studies have shown that the adjusted survival and hospitalization rates are similar between HF subtypes,47, 65 there is a need for future studies to clarify this.
In conclusion, this meta‐analysis provides the first summary on the effects of frailty on mortality and hospitalization and confirms the significant negative impact of frailty on chronic HF. Stratification of patients with HF by frailty status provides prognostic information and may inform priorities for HF interventions and management.
Sources of Funding
Bayés‐Genís and Gastelurrutia are supported by grants from the Ministerio de Educación y Ciencia (SAF2014‐59892) and Generalitat de Catalunya (Pla estratègic de recerca i innovació en salut Programme, Departament de Salut, SLT002_16_00209), Fundació La MARATÓ de TV3 (201502‐30, 201516‐10), Red de Terapia Celular–TerCel (RD16/0011/0006), and Centro de Investigación en Red en Enfermedades Cardiovasculares (CB16/11/00403) projects as part of the Plan Nacional de I+D+I, and jointly funded by Instituto de Salud Carlos III–Sudirección General de Evaluación y el Fondo Europeo de Desarrollo Regional. Centro Nacional de Investigaciones Cardiovasculares (CNIC) is supported by the Ministerio de Economía, Industria y Competitividad (MINECO), and the Pro‐CNIC Foundation, and is a Severo Ochoa Center of Excellence (MINECO award SEV‐2015‐0505). Ferguson was supported by a University of Technology Sydney, Chancellor's Postdoctoral Research Fellowship (2015001232). Fung is recipient of the Direct Grant award from the Faculty of Medicine, The Chinese University of Hong Kong, and of an investigator‐initiated research grant from the Food and Health Bureau of the Hong Kong Special Administrative Region. Woo is supported by research grants from the Hong Kong Jockey Club and the Research Grants Council.
Disclosures
None.
Supporting information
Table S1. List of Covariates Adjusted for in Calculating Hazard Ratios (Adjusted Hazard Ratios)
Table S2. Actual Numbers of Deaths and/or Hospitalization Episodes in Chronic Heart Failure Patients With and Without Frailty
Table S3. Quality Assessment of Studies Using the Newcastle‐Ottawa Scale*
Figure S1. Detailed CONSORT‐style flow diagram. PubMed unique identifiers shown in squared brackets.
Figure S2. Funnel plots assessing for publication bias in the meta‐analyses of frailty on (A) all‐cause mortality and (B) incident hospitalization in patients with chronic heart failure. C, Data on all‐cause mortality were further subjected to the Duval‐Tweedie's trim and fill test, demonstrating virtually unchanged effect size estimates and statistical significance (adjusted hazard ratio, 1.48; 95% confidence interval 1.25–1.75, P<0.001).
Acknowledgments
We thank William B. Goggins III, ScD, of The Chinese University of Hong Kong, for discussions.
(J Am Heart Assoc. 2018;7:e008251 DOI: 10.1161/JAHA.117.008251)
References
- 1. Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, Cesari M, Chumlea WC, Doehner W, Evans J, Fried LP, Guralnik JM, Katz PR, Malmstrom TK, McCarter RJ, Gutierrez Robledo LM, Rockwood K, von Haehling S, Vandewoude MF, Walston J. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14:392–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rodriguez‐Pascual C, Paredes‐Galan E, Ferrero‐Martinez AI, Gonzalez‐Guerrero JL, Hornillos‐Calvo M, Menendez‐Colino R, Torres‐Torres I, Vilches‐Moraga A, Galan MC, Suarez‐Garcia F, Olcoz‐Chiva MT, Rodriguez‐Artalejo F. The frailty syndrome is associated with adverse health outcomes in very old patients with stable heart failure: a prospective study in six Spanish hospitals. Int J Cardiol. 2017;236:296–303. [DOI] [PubMed] [Google Scholar]
- 3. Gastelurrutia P, Lupon J, Altimir S, de Antonio M, Gonzalez B, Cabanes R, Rodriguez M, Urrutia A, Domingo M, Zamora E, Diez C, Coll R, Bayes‐Genis A. Fragility is a key determinant of survival in heart failure patients. Int J Cardiol. 2014;175:62–66. [DOI] [PubMed] [Google Scholar]
- 4. Vidán MT, Blaya‐Novakova V, Sanchez E, Ortiz J, Serra‐Rexach JA, Bueno H. Prevalence and prognostic impact of frailty and its components in non‐dependent elderly patients with heart failure. Eur J Heart Fail. 2016;18:869–875. [DOI] [PubMed] [Google Scholar]
- 5. Boxer R, Kleppinger A, Ahmad A, Annis K, Hager D, Kenny A. The 6‐minute walk is associated with frailty and predicts mortality in older adults with heart failure. Congest Heart Fail. 2010;16:208–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Cacciatore F, Abete P, Mazzella F, Viati L, Della Morte D, D'Ambrosio D, Gargiulo G, Testa G, Santis D, Galizia G, Ferrara N, Rengo F. Frailty predicts long‐term mortality in elderly subjects with chronic heart failure. Eur J Clin Invest. 2005;35:723–730. [DOI] [PubMed] [Google Scholar]
- 7. McNallan SM, Singh M, Chamberlain AM, Kane RL, Dunlay SM, Redfield MM, Weston SA, Roger VL. Frailty and healthcare utilization among patients with heart failure in the community. JACC Heart Fail. 2013;1:135–141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Jha SR, Hannu MK, Newton PJ, Wilhelm K, Hayward CS, Jabbour A, Kotlyar E, Keogh A, Dhital K, Granger E, Connellan M, Jansz P, Spratt PM, Montgomery E, Smith A, Harkess M, Tunicliff P, Davidson PM, Macdonald PS. Reversibility of frailty after bridge‐to‐transplant ventricular assist device implantation or heart transplantation. Transplant Direct. 2017;3:e167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Dunlay SM, Park SJ, Joyce LD, Daly RC, Stulak JM, McNallan SM, Roger VL, Kushwaha SS. Frailty and outcomes after implantation of left ventricular assist device as destination therapy. J Heart Lung Transplant. 2014;33:359–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. McNallan SM, Chamberlain AM, Gerber Y, Singh M, Kane RL, Weston SA, Dunlay SM, Jiang R, Roger VL. Measuring frailty in heart failure: a community perspective. Am Heart J. 2013;166:768–774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Madan SA, Fida N, Barman P, Sims D, Shin J, Verghese J, Pina I, Jorde U, Patel SR. Frailty assessment in advanced heart failure. J Card Fail. 2016;22:840–844. [DOI] [PubMed] [Google Scholar]
- 12. Jha SR, Ha HS, Hickman LD, Hannu M, Davidson PM, Macdonald PS, Newton PJ. Frailty in advanced heart failure: a systematic review. Heart Fail Rev. 2015;20:553–560. [DOI] [PubMed] [Google Scholar]
- 13. Boxer RS, Dauser DA, Walsh SJ, Hager WD, Kenny AM. The association between vitamin D and inflammation with the 6‐minute walk and frailty in patients with heart failure. J Am Geriatr Soc. 2008;56:454–461. [DOI] [PubMed] [Google Scholar]
- 14. Altimir S, Lupón J, González B, Prats M, Parajón T, Urrutia A, Coll R, Valle V. Sex and age differences in fragility in a heart failure population. Eur J Heart Fail. 2005;7:798–802. [DOI] [PubMed] [Google Scholar]
- 15. Lupón J, González B, Santaeugenia S, Altimir S, Urrutia A, Más D, Díez C, Pascual T, Cano L, Valle V. Prognostic implication of frailty and depressive symptoms in an outpatient population with heart failure. Rev Esp Cardiol. 2008;61:835–842. [PubMed] [Google Scholar]
- 16. Ferguson C, Inglis SC, Newton PJ, Middleton S, Macdonald PS, Davidson PM. Multi‐morbidity, frailty and self‐care: important considerations in treatment with anticoagulation drugs: outcomes of the AFASTER study. Eur J Cardiovasc Nurs. 2017;16:113–124. [DOI] [PubMed] [Google Scholar]
- 17. González‐Moneo MJ, Sánchez‐Benavides G, Verdu‐Rotellar JM, Cladellas M, Bruguera J, Quiñones‐Ubeda S, Enjuanes C, Peña‐Casanova J, Comín‐Colet J. Ischemic aetiology, self‐reported frailty, and gender with respect to cognitive impairment in chronic heart failure patients. BMC Cardiovasc Disord. 2016;16:163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Denfeld QE, Winters‐Stone K, Mudd JO, Gelow JM, Kurdi S, Lee CS. The prevalence of frailty in heart failure: a systematic review and meta‐analysis. Int J Cardiol. 2017;236:283–289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D, Becker BJ, Sipe TA, Thacker SB; Meta‐analysis Of Observational Studies in Epidemiology (MOOSE) group. Meta‐analysis of observational studies in epidemiology: a proposal for reporting. JAMA. 2000;283:2008–2012. [DOI] [PubMed] [Google Scholar]
- 20. Altman DG, Simera I. A history of the evolution of guidelines for reporting medical research: the long road to the EQUATOR Network. J R Soc Med. 2016;109:67–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P; Authors/Task Force Members; Document Reviewers . 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC): developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2016;18:891–975. [DOI] [PubMed] [Google Scholar]
- 22. Writing Committee Members , Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJ, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WH, Tsai EJ, Wilkoff BL; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;128:e240–e327. [DOI] [PubMed] [Google Scholar]
- 23. Denfeld QE, Winters‐Stone K, Mudd JO, Hiatt SO, Chien CV, Lee CS. Frequency of and significance of physical frailty in patients with heart failure. Am J Cardiol. 2017;119:1243–1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Khandelwal D, Goel A, Kumar U, Gulati V, Narang R, Dey AB. Frailty is associated with longer hospital stay and increased mortality in hospitalized older patients. J Nutr Health Aging. 2012;16:732–735. [DOI] [PubMed] [Google Scholar]
- 25. Newman AB, Gottdiener JS, Mcburnie MA, Hirsch CH, Kop WJ, Tracy R, Walston JD, Fried LP. Associations of subclinical cardiovascular disease with frailty. J Gerontol A Biol Sci Med Sci. 2001;56:M158–M166. [DOI] [PubMed] [Google Scholar]
- 26. Nishiguchi S, Nozaki Y, Yamaji M, Oya K, Hikita Y, Aoyama T, Mabuchi H. Plasma brain natriuretic peptide level in older outpatients with heart failure is associated with physical frailty, especially with the slowness domain. J Geriatr Cardiol. 2016;13:608–614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Parmar KR, Xiu PY, Chowdhury MR, Patel E, Cohen M. In‐hospital treatment and outcomes of heart failure in specialist and non‐specialist services: a retrospective cohort study in the elderly. Open Heart. 2015;2:e000095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Reeves GR, Whellan DJ, Patel MJ, O'Connor CM, Duncan P, Eggebeen JD, Morgan TM, Hewston LA, Pastva AM, Kitzman DW. Comparison of frequency of frailty and severely impaired physical function in patients ≥60 years hospitalized with acute decompensated heart failure versus chronic stable heart failure with reduced and preserved left ventricular ejection fraction. Am J Cardiol. 2016;117:1953–1958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Uchmanowicz I, Kusnierz M, Wleklik M, Jankowska‐Polanska B, Jaroch J, Loboz‐Grudzien K. Frailty syndrome and rehospitalizations in elderly heart failure patients. Aging Clin Exp Res. 2018;30:617–623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Woods NF, LaCroix AZ, Gray SL, Aragaki A, Cochrane BB, Brunner RL, Masaki K, Murray A, Newman AB; Women's Health Initiative . Frailty: emergence and consequences in women aged 65 and older in the Women's Health Initiative Observational Study. J Am Geriatr Soc. 2005;53:1321–1330. [DOI] [PubMed] [Google Scholar]
- 31. Yamada S, Kamiya K, Kono Y. Frailty may be a risk marker for adverse outcome in patients with congestive heart failure. ESC Heart Fail. 2015;2:168–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Gastelurrutia P, Lupón J, Altimir S, de Antonio M, González B, Cabanes R, Cano L, Urrutia A, Domingo M, Zamora E, Díez C, Coll R, Bayes‐Genis A. Effect of fragility on quality of life in patients with heart failure. Am J Cardiol. 2013;112:1785–1789. [DOI] [PubMed] [Google Scholar]
- 33. Kenny AM, Boxer R, Walsh S, Hager WD, Raisz LG. Femoral bone mineral density in patients with heart failure. Osteoporos Int. 2006;17:1420–1427. [DOI] [PubMed] [Google Scholar]
- 34. Pons F, Lupón J, Urrutia A, González B, Crespo E, Díez C, Cano L, Cabanes R, Altimir S, Coll R, Pascual T, Valle V. Mortality and cause of death in patients with heart failure: findings at a specialist multidisciplinary heart failure unit. Rev Esp Cardiol. 2010;63:303–314. [DOI] [PubMed] [Google Scholar]
- 35. Uchmanowicz I, Gobbens RJ. The relationship between frailty, anxiety and depression, and health‐related quality of life in elderly patients with heart failure. Clin Interv Aging. 2015;10:1595–1600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Uchmanowicz I, Wleklik M, Gobbens RJ. Frailty syndrome and self‐care ability in elderly patients with heart failure. Clin Interv Aging. 2015;10:871–877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Vidán MT, Sanchez E, Fernandez‐Aviles F, Serra‐Rexach JA, Ortiz J, Bueno H. FRAIL‐HF, a study to evaluate the clinical complexity of heart failure in nondependent older patients: rationale, methods and baseline characteristics. Clin Cardiol. 2014;37:725–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA; Cardiovascular Health Study Collaborative Research Group . Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:146–156. [DOI] [PubMed] [Google Scholar]
- 39. Romero‐Ortuno R, Walsh CD, Lawlor BA, Kenny RA. A frailty instrument for primary care: findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010;10:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Senn SJ. Overstating the evidence: double counting in meta‐analysis and related problems. BMC Med Res Methodol. 2009;9:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Stang A. Critical evaluation of the Newcastle‐Ottawa scale for the assessment of the quality of nonrandomized studies in meta‐analyses. Eur J Epidemiol. 2010;25:603–605. [DOI] [PubMed] [Google Scholar]
- 42. Rich MW, Chyun DA, Skolnick AH, Alexander KP, Forman DE, Kitzman DW, Maurer MS, McClurken JB, Resnick BM, Shen WK, Tirschwell DL; American Heart Association Older Populations Committee of the Council on Clinical Cardiology, Council on Cardiovascular and Stroke Nursing, Council on Cardiovascular Surgery and Anesthesia, Stroke Council; American College of Cardiology; and American Geriatrics Society . Knowledge gaps in cardiovascular care of the older adult population: a scientific statement from the American Heart Association, American College of Cardiology, and American Geriatrics Society. Circulation. 2016;133:2103–2122. [DOI] [PubMed] [Google Scholar]
- 43. Jha SR, Hannu MK, Chang S, Montgomery E, Harkess M, Wilhelm K, Hayward CS, Jabbour A, Spratt PM, Newton P, Davidson PM, Macdonald PS. The prevalence and prognostic significance of frailty in patients with advanced heart failure referred for heart transplantation. Transplantation. 2016;100:429–436. [DOI] [PubMed] [Google Scholar]
- 44. Green P, Woglom AE, Genereux P, Daneault B, Paradis JM, Schnell S, Hawkey M, Maurer MS, Kirtane AJ, Kodali S, Moses JW, Leon MB, Smith CR, Williams M. The impact of frailty status on survival after transcatheter aortic valve replacement in older adults with severe aortic stenosis: a single‐center experience. JACC Cardiovasc Interv. 2012;5:974–981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Afilalo J, Lauck S, Kim DH, Lefevre T, Piazza N, Lachapelle K, Martucci G, Lamy A, Labinaz M, Peterson MD, Arora RC, Noiseux N, Rassi A, Palacios IF, Genereux P, Lindman BR, Asgar AW, Kim CA, Trnkus A, Morais JA, Langlois Y, Rudski LG, Morin JF, Popma JJ, Webb JG, Perrault LP. Frailty in older adults undergoing aortic valve replacement: the FRAILTY‐AVR study. J Am Coll Cardiol. 2017;70:689–700. [DOI] [PubMed] [Google Scholar]
- 46. McDonagh J, Martin L, Ferguson C, Jha SR, Macdonald PS, Davidson PM, Newton PJ. Frailty assessment instruments in heart failure: a systematic review. Eur J Cardiovasc Nurs. 2017;17:23–35. [DOI] [PubMed] [Google Scholar]
- 47. Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population‐based study. N Engl J Med. 2006;355:260–269. [DOI] [PubMed] [Google Scholar]
- 48. Fung E, Hui E, Yang X, Lui LT, Cheng KF, Li Q, Fan KY, Sahota DS, Ma BH, Lee JS, Lee APW, Woo J. Heart failure and frailty in the community‐living elderly population: what the UFO study will tell us. Front Physiol. 2018;9:347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Haykowsky MJ, Kouba EJ, Brubaker PH, Nicklas BJ, Eggebeen J, Kitzman DW. Skeletal muscle composition and its relation to exercise intolerance in older patients with heart failure and preserved ejection fraction. Am J Cardiol. 2014;113:1211–1216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, Mitnitski A. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173:489–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Woo J, Leung J, Morley JE. Comparison of frailty indicators based on clinical phenotype and the multiple deficit approach in predicting mortality and physical limitation. J Am Geriatr Soc. 2012;60:1478–1486. [DOI] [PubMed] [Google Scholar]
- 52. Chong E, Ho E, Baldevarona‐Llego J, Chan M, Wu L, Tay L. Frailty and risk of adverse outcomes in hospitalized older adults: a comparison of different frailty measures. J Am Med Dir Assoc. 2017;18:638.e7–638.e11. [DOI] [PubMed] [Google Scholar]
- 53. Auyeung TW, Lee JS, Leung J, Kwok T, Woo J. The selection of a screening test for frailty identification in community‐dwelling older adults. J Nutr Health Aging. 2014;18:199–203. [DOI] [PubMed] [Google Scholar]
- 54. Woo J. Walking speed: a summary indicator of frailty? J Am Med Dir Assoc. 2015;16:635–637. [DOI] [PubMed] [Google Scholar]
- 55. Pulignano G, Del Sindaco D, Di Lenarda A, Alunni G, Senni M, Tarantini L, Cioffi G, Tinti MD, Barbati G, Minardi G, Uguccioni M; IMAGE‐HF Study Investigators . Incremental value of gait speed in predicting prognosis of older adults with heart failure: insights from the IMAGE‐HF study. JACC Heart Fail. 2016;4:289–298. [DOI] [PubMed] [Google Scholar]
- 56. Tang Y, Fung E, Xu A, Lan HY. C‐reactive protein and ageing. Clin Exp Pharmacol Physiol. 2017;44(suppl 1):9–14. [DOI] [PubMed] [Google Scholar]
- 57. Azad N, Lemay G. Management of chronic heart failure in the older population. J Geriatr Cardiol. 2014;11:329–337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Ogren JA, Fonarow GC, Woo MA. Cerebral impairment in heart failure. Curr Heart Fail Rep. 2014;11:321–329. [DOI] [PubMed] [Google Scholar]
- 59. Abellan van Kan G, Rolland Y, Bergman H, Morley JE, Kritchevsky SB, Vellas B. The I.A.N.A Task Force on frailty assessment of older people in clinical practice. J Nutr Health Aging. 2008;12:29–37. [DOI] [PubMed] [Google Scholar]
- 60. Dent E, Lien C, Lim WS, Wong WC, Wong CH, Ng TP, Woo J, Dong B, de la Vega S, Hua Poi PJ, Kamaruzzaman SBB, Won C, Chen LK, Rockwood K, Arai H, Rodriguez‐Manas L, Cao L, Cesari M, Chan P, Leung E, Landi F, Fried L, Morley JE, Vellas B, Flicker L. The Asia‐Pacific clinical practice guidelines for the management of frailty. J Am Med Dir Assoc. 2017;18:564–575. [DOI] [PubMed] [Google Scholar]
- 61. Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8:24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Austin PC, Lee DS, Fine JP. Introduction to the analysis of survival data in the presence of competing risks. Circulation. 2016;133:601–609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Davis JD, Olsen MA, Bommarito K, LaRue SJ, Saeed M, Rich MW, Vader JM. All‐payer analysis of heart failure hospitalization 30‐day readmission: comorbidities matter. Am J Med. 2017;130:93.e9–93.e28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Newton PJ, Davidson PM, Reid CM, Krum H, Hayward C, Sibbritt DW, Banks E, MacDonald PS. Acute heart failure admissions in New South Wales and the Australian Capital Territory: the NSW HF Snapshot Study. Med J Aust. 2016;204:113.e1–113.e8. [DOI] [PubMed] [Google Scholar]
- 65. Loop MS, Van Dyke MK, Chen L, Brown TM, Durant RW, Safford MM, Levitan EB. Comparison of length of stay, 30‐day mortality, and 30‐day readmission rates in Medicare patients with heart failure and with reduced versus preserved ejection fraction. Am J Cardiol. 2016;118:79–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. List of Covariates Adjusted for in Calculating Hazard Ratios (Adjusted Hazard Ratios)
Table S2. Actual Numbers of Deaths and/or Hospitalization Episodes in Chronic Heart Failure Patients With and Without Frailty
Table S3. Quality Assessment of Studies Using the Newcastle‐Ottawa Scale*
Figure S1. Detailed CONSORT‐style flow diagram. PubMed unique identifiers shown in squared brackets.
Figure S2. Funnel plots assessing for publication bias in the meta‐analyses of frailty on (A) all‐cause mortality and (B) incident hospitalization in patients with chronic heart failure. C, Data on all‐cause mortality were further subjected to the Duval‐Tweedie's trim and fill test, demonstrating virtually unchanged effect size estimates and statistical significance (adjusted hazard ratio, 1.48; 95% confidence interval 1.25–1.75, P<0.001).