

Abstract
Objective To quantify the prevalence of adverse childhood experiences (ACEs) among a diverse urban cohort of pregnant women.
Study Design The ACE survey was self-administered to 600 women categorized evenly between the waiting room, private examination rooms, and CenteringPregnancy group spaces. The percentage of women willing to complete the survey per location was compared using chi-square tests, and the mean ACE score per arm was compared using Wilcoxon's rank–sum test.
Results Of the 660 women approached for participation, 5% declined; 67% reported ≥ 1 ACE exposure and 19% reported an ACE score of ≥ 4. By domain, 59% experienced household dysfunction, 25% abuse, and 25% neglect. Women in the waiting room were more likely to decline participation ( p < 0.01), and those participating in the postpartum inpatient arm had a significantly lower proportion affirming 8 of 10 ACE questions, were less likely to report ≥1 ACE, and had a lower mean ACE score when compared with the outpatient arm ( p < 0.01).
Conclusion The prevalence of ACEs in this diverse pregnant cohort was high. The ideal locations to distribute the survey are the outpatient examination rooms.
Keywords: ACE, pregnancy, adverse childhood experiences, CenteringPregnancy
In 1998, Felitti et al published the landmark Adverse Childhood Experiences (ACE) Study, 1 in which they reported a strong dose-dependent relationship between one's exposure to abuse and dysfunction in childhood, as measured by an ACE score, and risk factors for the leading causes of death in adults. This ACE score was calculated based on the number of “yes” responses on a 10-item survey regarding one's exposure to three domains of adverse experiences before the age of 18: abuse, neglect, and household dysfunction. Their original cohort of more than 8,000 participants, who were predominantly older, non-Hispanic White, and well-educated, remains the population from which the majority of subsequent ACE analyses have been reported. This ACE work is critically important for those practicing in the clinical arena, particularly when considered in context to the widely held theory of multiple determinants of health outcomes. This theory suggests that only 10% of all health outcomes may be attributed to actual medical care; in contrast, 40 to 60% are attributed to social and behavioral factors. 2
Given the known association between maternal stress and markers of poor social support with adverse pregnancy outcomes, 3 4 5 the relationship between formal ACE scores and adverse pregnancy outcomes is of key public health interest. Secondary analyses from the original cohort report a dose-dependent relationship between ACE scores and rates of adolescent pregnancy, 6 7 unintended pregnancy, 8 and fetal death. 6 7 However, these scores were obtained from a survey mailed to women who were largely remote from their reproductive years. Other investigators in the United States, Canada, and Switzerland have correlated ACE scores to alcohol use during pregnancy, smoking, and spontaneous preterm birth, but they administered the survey retrospectively after pregnancy. 9 10 11 Very few investigators have administered the survey during pregnancy, 12 13 14 and none have investigated the impact of the location where the survey was administered on a woman's willingness to complete it.
Therefore, the primary objective of our study was to quantify the prevalence of ACE exposures among a racially diverse, low-to-middle socioeconomic status pregnant urban cohort. Secondary objectives were to determine the setting in which women were more likely to complete the survey and whether the setting affected the mean reported ACE score. Furthermore, within the subset of postpartum patients, we sought to determine whether an absolute ACE score or a particular ACE domain was associated with preterm delivery.
Materials and Methods
Eligible patients were those 18 years or older receiving prenatal care from an ambulatory women's health clinic run at a tertiary academic medical center in the American South. This clinic serves a diverse population; of the 1,229 women who came for routine prenatal care over the 3-month study period, 44.9% were Caucasian, 28.6% were African-American, 22.5% were Hispanic, and 1% other. Additionally, 64% received care under Medicaid and 21% were uninsured. The inpatient arm of the study was performed on the postpartum units of the associated large tertiary care teaching hospital.
A convenience sample of 600 was chosen, representing more than 20% of the clinic's annual patient population, and divided by location where the survey was administered as follows: 300 inpatient and 300 outpatient, with the outpatient arm divided equally ( N = 100) between administration in the clinic's waiting rooms, private examination rooms, and the CenteringPregnancy group spaces. In order to prevent duplicative sampling, Participants were not given a survey if they reported having already completed one previously.
For the inpatient arm, a research team member went to each postpartum room and asked the patient if she would be willing to fill out the anonymous 10-question survey on ACEs. Patients were offered a small edible incentive for participating. Completed surveys were then collected in a drop box with the survey questions and answers folded inward. A similar technique was used in the ambulatory setting.
The survey used for this study ( Fig. 1 ) was derived directly from the published ACE survey and was made available in both English and Spanish. Additional questions included patient's age and self-reported race. For postpartum patients, the survey also inquired about gestational age at the time of delivery and the newborn's birth weight (in ounces, which was converted to grams). Preterm delivery was defined as delivery less than 37 weeks' gestational age. No patient identifiers were used for any arm of the study.
Fig. 1.
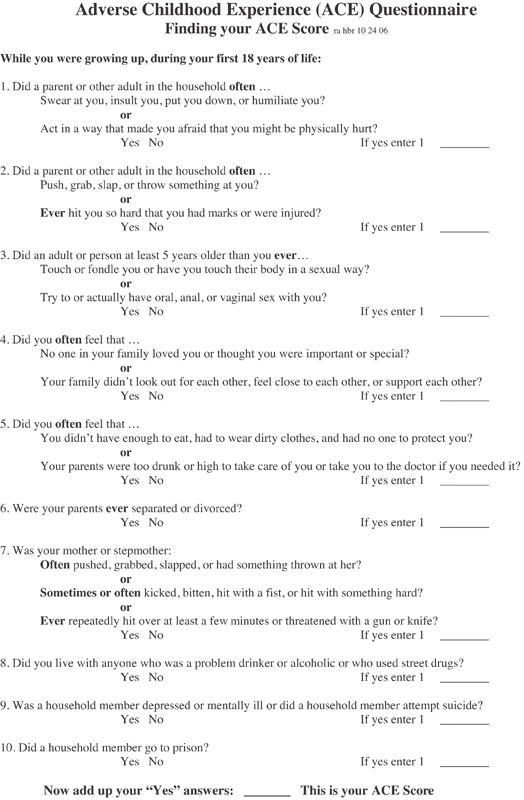
Adverse childhood experience survey.
Both participation rates and the number of complete versus incomplete forms were tracked and categorized by location completed. Consistent with other investigators, for any of the 10 ACE questions that were unanswered, a “no” response was assumed. We then calculated overall ACE scores, defined as the sum of “yes” answers (plausible range: 1–10), and ACE score within each of the three ACE domains (abuse, neglect, and household dysfunction). We compared the proportions of outpatient versus inpatient respondents affirming each ACE domain and ACE category using chi-square tests, and the mean ACE scores using Wilcoxon's rank-sum tests. For those women completing the form in the postpartum setting, we compared the proportions of preterm versus term births affirming each ACE category using chi-square tests (Fisher's exact tests for cell sizes < 5). We also compared mean ACE scores and the proportion of women affirming each ACE domain of preterm versus term births with the Wilcoxon's rank-sum test and chi-square test, respectively. Statistical analysis was performed with Stata version 13 (College Station, TX).
Results
A total of 660 patients were approached for participation in the study ( Fig. 2 ). Of the 660 women asked, 35 (5%) declined. Of those agreeing to complete the survey, 12 women were discharged from the hospital or left the waiting room before the survey could be collected and 12 were determined ineligible after survey completion because they reported being less than 18 years old. The final sample included 601 surveys. Of the final analysis group, 567 (94%) provided an answer to all 10 ACE questions.
Fig. 2.
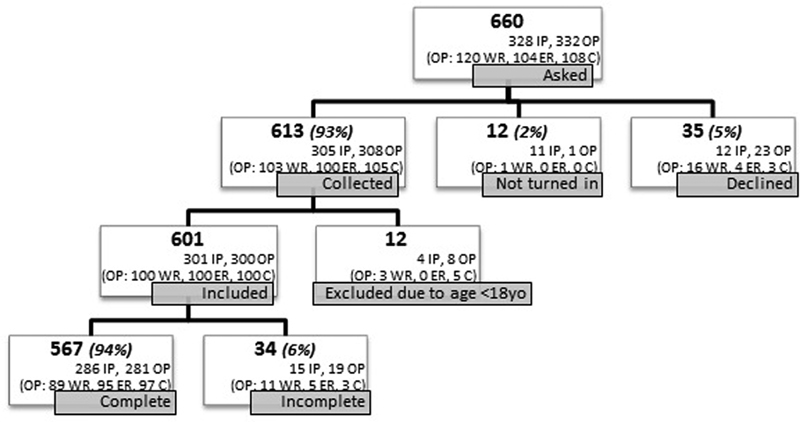
Adverse childhood experience (ACE) study participation. C, centering; ER, examination room; IP, inpatient; OP, outpatient, WR; waiting room. A form was considered complete if all 10 ACE questions were answered, even if there was missing demographic information.
The demographics of the participants were representative of the entire ambulatory clinic population ( Table 1 ). The age of participants ranged from 18 to 43 years, with a mean age of 25.7 years (standard deviation: 5.3 years). Race and age characteristics of the outpatient and inpatient groups did not differ.
Table 1. Demographics of participants.
| All participants, n = 601 | Inpatient, n = 301 | Outpatient, n = 300 | Waiting room, n = 100 | Examination room, n = 100 | Centering, n = 100 | |
|---|---|---|---|---|---|---|
| Age | ||||||
| 18–24 y | 278 (46.3%) | 143 (47.5%) | 135 (45%) | 42 (42%) | 44 (44%) | 49 (49%) |
| 25–34 y | 261 (43.4%) | 129 (42.9%) | 132 (44%) | 45 (45%) | 47 (47%) | 40 (40%) |
| > 35 y | 45 (7.5%) | 23 (7.6%) | 22 (7.3%) | 9 (9%) | 7 (7%) | 6 (6%) |
| Missing | 17 (2.8%) | 6 (2%) | 11 (3.7%) | 4 (4%) | 2 (2%) | 5 (5%) |
| Race | ||||||
| African-American | 188 (31%) | 92 (30.6%) | 96 (32%) | 40 (40%) | 26 (26%) | 30 (30%) |
| Caucasian | 244 (41%) | 124 (41.2%) | 120 (40%) | 37 (37%) | 43 (43%) | 40 (40%) |
| Hispanic | 124 (21%) | 62 (20.6%) | 62 (20.6%) | 16 (16%) | 23 (23%) | 23 (23%) |
| Other | 32 (5%) | 16 (5.3%) | 16 (5.3%) | 7 (7%) | 6 (6%) | 3 (3%) |
| Missing | 13 (2%) | 7 (2.3%) | 6 (2%) | 0 | 2 (2%) | 4 (4%) |
| ACE scores | ||||||
| Range | 0–10 | 0–10 | 0–10 | 0–9 | 0–10 | 0–9 |
| Average | 1.85 | 1.52 | 2.19 | 2.14 | 2.12 | 2.31 |
Abbreviation: ACE, adverse childhood experiences.
Of the analytic sample, 201 (33%) reported no exposure to any ACEs, whereas 116 (19%) reported exposure to four or more ACEs. Overall, the most prevalent experience was parental separation or divorce, as reported by 305 women (50.7%). When viewed by domain of ACE score, 59.4% of the population had experienced household dysfunction, 25.5% experienced abuse, and 25.3% experienced neglect ( Table 2 ). Total ACE scores were comparable to the scores published by Felitti et al in the original ACE study. 1
Table 2. Prevalence of adverse childhood experiences by category.
| ACE Question by domain | No. per ACE question | No. per ACE domain | Percentage per ACE domain | |||
|---|---|---|---|---|---|---|
| CDC, a % | OB/GYN center, % ( n ) | |||||
| Abuse | 1) Emotional abuse | 13.1 | 18.4 | (111) | 153 | 25.5% |
| 2) Physical abuse | 27 | 11.8 | (71) | |||
| 3) Sexual abuse | 24.7 | 14.3 | (86) | |||
| Neglect | 4) Emotional neglect | 16.7 | 22.8 | (137) | 152 | 25.3% |
| 5) Physical neglect | 9.2 | 6.3 | (38) | |||
| Household dysfunction | 6) Parental separation or divorce | 24.5 | 50.7 | (305) | 357 | 59.4% |
| 7) Mother treated violently | 13.7 | 11 | (66) | |||
| 8) Household substance abuse | 29.5 | 20 | (120) | |||
| 9) Household mental illness | 23.3 | 14.3 | (86) | |||
| 10) Incarcerated household member | 5.2 | 15.6 | (94) | |||
Abbreviations: ACE, adverse childhood experiences; CDC, Center for Disease Control; OB-GYN, obstetrics and gynecology.
Center for Disease Control ACE Study: Data and Statistics. 16
The proportion of women agreeing to complete the survey differed by location. Of those women who were approached in the outpatient waiting room, 13.3% declined compared with less than 4% of women approached in the hospital (inpatient) postpartum or in either an outpatient examination room or CenteringPregnancy group ( p < 0.01).
Additionally, the postpartum inpatient arm had a significantly lower proportion affirming 8 out of 10 of the questions ( p < 0.05), a lower proportion of women reporting at least one ACE ( p < 0.001) ( Table 3 ), and a lower mean ACE score ( p < 0.01).
Table 3. ACE scores by location.
| ACE score | Prenatal outpatient, n (%) | Postpartum inpatient, n (%) |
|---|---|---|
| 0 | 80 (27%) | 121 (40%) |
| 1 | 71 (24%) | 91 (30%) |
| 2 | 50 (17%) | 23 (8%) |
| 3 | 32 (11%) | 17 (6%) |
| ≥4 | 67 (22%) | 49 (16%) |
| Total | 300 | 301 |
Abbreviation: ACE, adverse childhood experiences.
Chi-square test, p < 0.001.
Of the 301 surveys completed postpartum, 277 (92%) reported the gestational age at which they delivered. Of those 277, the average gestational age was 38.7 weeks, with 22 (8%) delivered preterm. The prevalence of preterm deliveries captured by this study was lower than that reported for our institution, state, and nation at close to 12%. The preterm and term cohorts did not significantly differ in proportions affirming individual ACE categories or mean ACE scores.
Discussion
In this racially diverse population of pregnant women, the prevalence of ACEs was high, with 67% of the population exposed to at least one ACE. ACE scores of ≥ 4, associated with the highest risk for adverse outcomes in many studies, 1 11 were reported by nearly one in five women. By domain, 59% of women experienced household dysfunction, 25% had been abused, and 25% had been neglected. This represents a significant emotional and physiological burden, 8 and potentially a critical area for counseling and intervention in the prenatal setting.
Ours is the first study to report the location where women are most likely to complete a self-administered ACE survey in the puerperium, providing a helpful framework for future investigations. Women approached in the waiting room setting were more likely to decline participation (13.3% compared with <4%), though overall acceptance of the survey was very high (95%). Those approached in the waiting room have less privacy than in other settings, potentially accounting for their higher refusal rates. For participants in the postpartum arm, the influence of stress and hormones during pregnancy versus after birth may have had an effect on how women responded, especially to questions on neglect and emotional abuse. If the ACE survey is to be used as a screening tool, its use prenatally may be preferred. Due to comparable participation rates in the examination rooms and CenteringPregnancy group spaces, these are the ideal locations to distribute the survey.
Our work confirms and extends the relatively limited literature around ACE ascertainment during an ongoing pregnancy. Smith et al used trained interviewers to administer a modified version of the ACE survey to a large U.S .cohort at 28 weeks' gestation and reported a low refusal and incomplete survey rate (1.2%). 14 However, their study population differed from ours in that their participants were predominantly white (76%) and married or living with a partner (90%). Drevin et al mailed the ACE survey to the homes of a Swedish cohort during the third trimester and reported a modest response rate ( N = 142; 61%). 13 Finally, Bublitz and Stroud reported a small population of patients ( N = 41) who self-administered the survey around 20 weeks' gestation. 15
We were unable to confirm the results of other studies, suggesting a significant association between higher ACE score and lower gestational age at birth. 9 14 The preterm birth rate reported by our postpartum cohort was lower than anticipated, which may have been due in part to an unintended selection bias created by collecting surveys only from participants who were in their postpartum rooms during normal neonatal intensive care unit visiting hours. Another source of bias may have been due to recall bias, as not all patients accurately report their gestational age at delivery. Furthermore, there were 24 (8%) of the 301 participating postpartum patients who did not record their gestational age at delivery, limiting the sample size further.
Overall, this study provides a strong foundation for future studies measuring the association between ACE scores and adverse pregnancy outcomes. We conclude that the ACE survey is readily completed by pregnant women in the ambulatory care setting, particularly in the rooms where they will receive their care, and that the prevalence of ACEs is high in a diverse urban cohort. Finally, we hypothesize that following additional research, this instrument may well provide a simple mechanism to identify women at the highest risk for adverse pregnancy outcomes.
Footnotes
Conflict of Interest None.
References
- 1.Felitti V J, Anda R F, Nordenberg D et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. Am J Prev Med. 1998;14(04):245–258. doi: 10.1016/s0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- 2.Robert Wood Johnson Foundation.Health Policy Brief: The Relative Contribution of Multiple Determinants to Health OutcomesAugust 21, 2014.http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_123.pdf. Accessed June 7, 2017
- 3.Hoffman M C, Mazzoni S E, Wagner B D, Laudenslager M L, Ross R G. Measures of maternal stress and mood in relation to preterm birth. Obstet Gynecol. 2016;127(03):545–552. doi: 10.1097/AOG.0000000000001287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lilliecreutz C, Larén J, Sydsjö G, Josefsson A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth. 2016;16(01):5. doi: 10.1186/s12884-015-0775-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brumberg H L, Shah S I. Born early and born poor: an eco-bio-developmental model for poverty and preterm birth. J Neonatal Perinatal Med. 2015;8(03):179–187. doi: 10.3233/NPM-15814098. [DOI] [PubMed] [Google Scholar]
- 6.Hillis S D, Anda R F, Dube S R et al. The protective effect of family strengths in childhood against adolescent pregnancy and its long-term psychosocial consequences. Perm J. 2010;14(03):18–27. doi: 10.7812/tpp/10-028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hillis S D, Anda R F, Dube S R, Felitti V J, Marchbanks P A, Marks J S. The association between adverse childhood experiences and adolescent pregnancy, long-term psychosocial consequences, and fetal death. Pediatrics. 2004;113(02):320–327. doi: 10.1542/peds.113.2.320. [DOI] [PubMed] [Google Scholar]
- 8.Dietz P M, Spitz A M, Anda R F et al. Unintended pregnancy among adult women exposed to abuse or household dysfunction during their childhood. JAMA. 1999;282(14):1359–1364. doi: 10.1001/jama.282.14.1359. [DOI] [PubMed] [Google Scholar]
- 9.Christiaens I, Hegadoren K, Olson D M. Adverse childhood experiences are associated with spontaneous preterm birth: a case-control study. BMC Med. 2015;13(13):124. doi: 10.1186/s12916-015-0353-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chung E K, Nurmohamed L, Mathew L, Elo I T, Coyne J C, Culhane J F. Risky health behaviors among mothers-to-be: the impact of adverse childhood experiences. Acad Pediatr. 2010;10(04):245–251. doi: 10.1016/j.acap.2010.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Frankenberger D J, Clements-Nolle K, Yang W. The association between adverse childhood experiences and alcohol use during pregnancy in a representative sample of adult women. Womens Health Issues. 2015;25(06):688–695. doi: 10.1016/j.whi.2015.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bublitz M H, Stroud L R. Maternal history of child abuse moderates the association between daily stress and diurnal cortisol in pregnancy: a pilot study. Stress. 2013;16(06):706–710. doi: 10.3109/10253890.2013.825768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Drevin J, Stern J, Annerbäck E M et al. Adverse childhood experiences influence development of pain during pregnancy. Acta Obstet Gynecol Scand. 2015;94(08):840–846. doi: 10.1111/aogs.12674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Smith M V, Gotman N, Yonkers K A. early childhood adversity and pregnancy outcomes. Matern Child Health J. 2016;20(04):790–798. doi: 10.1007/s10995-015-1909-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leeners B, Rath W, Block E, Görres G, Tschudin S. Risk factors for unfavorable pregnancy outcome in women with adverse childhood experiences. J Perinat Med. 2014;42(02):171–178. doi: 10.1515/jpm-2013-0003. [DOI] [PubMed] [Google Scholar]
- 16.Center for Disease Control ACE Study: Data and Statistics.https://www.cdc.gov/violenceprevention/acestudy/index.html. Accessed March 5, 2016