

Key Clinical Message
Infarction of the anterior myocardial wall results in anterior ST‐elevation. However, ST‐deviation may also appear inferiorly and may aid in localizing the culprit lesion.
Keywords: coronary angiography, coronary circulation, electrocardiography, myocardial infarction, ST‐elevation myocardial infarction
1. CASE HISTORY
A 65‐year‐old man presented with chest pain. 12‐lead ECG showed anterior and inferior ST‐elevation (Figure 1). On coronary angiography, the right coronary system had mild, non‐obstructive disease (Video S1) and the culprit lesion appeared to be an occlusion (with partial recanalization) of the left anterior descending artery (LAD) distal to the first septal (S1) and diagonal (D1) branches (Video S2). Flow was restored during percutaneous coronary intervention (Video S3), leading to significant ST‐resolution (Figure 2).
Figure 1.
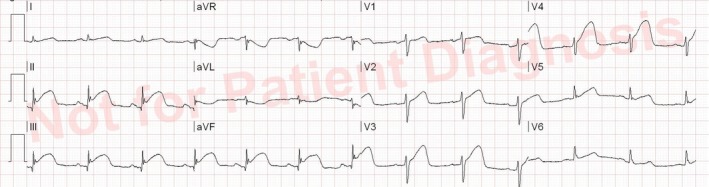
Prehospital 12‐lead ECG showing ST‐segment elevation and hyperacute T‐waves in the anterior (mainly V2‐V4) and inferior (II, III, aVF) leads
Figure 2.
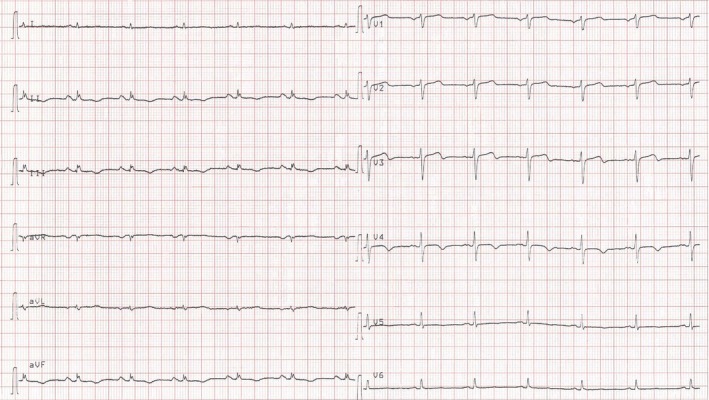
12‐lead ECG after reperfusion showing significant ST‐segment resolution
Anterior myocardial wall infarction results in anterior ST‐elevation.1 However, ST‐deviation may also appear inferiorly.1, 2, 3 Occlusion proximal to S1 and D1 leads to basal anterior wall infarction, associated with reciprocal ST‐depression inferiorly.1, 2, 3 Simultaneous anterior and inferior ST‐elevation may occur if the ST‐vector points more inferiorly.1 This could be due to a wrapped LAD reaching the apex to supply the distal inferior wall and/or an occlusion below S1 and D1, the latter suggesting a smaller ischemic region.1, 2, 3 With an occlusion located between S1 and D1, the ST‐segment in the inferior leads is less predictable.1, 2, 3 Interestingly, in the present case, S1 originated distally to D1. Determining the location of the occlusion and the presence of a wrapped LAD is prognostically important.1
CONFLICT OF INTEREST
None declared.
AUTHOR CONTRIBUTION
AK and SA: wrote the initial draft. CA and MP: provided expertise in ECG and angiography interpretation. All authors participated in collecting patient data (pictures and clinical history), reviewing the literature, interpretation of clinical findings, critical revision of the manuscript for important intellectual content, and approval of the final version.
Supporting information
Kristensen AMD, Amin S, Byrne C, Pareek M. Myocardial infarction with simultaneous anterior and inferior ST‐segment elevation. Clin Case Rep. 2019;7:583–584. 10.1002/ccr3.2023
REFERENCES
- 1. Wagner GS, Macfarlane P, Wellens H, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part VI: Acute ischemia/infarction: A scientific statement from the american heart association electrocardiography and arrhythmias committee, council on clinical cardiology; the american college of cardiology foundation; and the heart rhythm society. endorsed by the international society for computerized electrocardiology. J Am Coll Cardiol. 2009;53:1003‐1011. [DOI] [PubMed] [Google Scholar]
- 2. Sapin PM, Musselman DR, Dehmer GJ, Cascio WE. Implications of inferior ST‐segment elevation accompanying anterior wall acute myocardial infarction for the angiographic morphology of the left anterior descending coronary artery morphology and site of occlusion. Am J Cardiol. 1992;69:860‐865. [DOI] [PubMed] [Google Scholar]
- 3. Engelen DJ, Gorgels AP, Cheriex EC, et al. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute anterior myocardial infarction. J Am Coll Cardiol. 1999;34:389‐395. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials