

Abstract
Purpose:
To evaluate the feasibility and safety of heads-up three-dimensional (3D) vision system for phacoemulsification and intraocular lens (IOL) implantation surgery.
Methods:
In this prospective, randomized controlled study, 20 eyes with age-related cataract received phacoemulsification and IOL implantation and were randomly divided into “heads-up” 3D vision group and conventional surgery group. Ocular and surgical parameters such as surgery time, pre and postoperative best-corrected visual acuity (BCVA), and corneal endothelial cells density were recorded and statistically analyzed.
Results:
The result showed significant postoperative improvement of BCVA in both groups. There was no difference in either mean surgery time or postoperative mean endothelial cell density between the 3D group and the conventional group. No major complication occurred during surgery in either group.
Conclusion:
The heads-up 3D vision system is suitable and safe for cataract phacoemulsification and IOL implantation. This technique can be of widespread use.
Keywords: 3D-surgery, IOL implantation, phacoemulsification
Three-dimensional (3D) digital visualization (NGENUITY 3D) is a newly developed technology in the domain of eye microsurgery. It consists of one 1080 p camera, central processing unit (CPU), monitor, and polarized glasses. The camera is wired to the CPU, which processes the live image and displays overlapping stereo images on the widescreen HD monitor. Three-dimensionality is then experienced by donning the circularly polarized glasses. Advantages of the system involve higher depth of field and working distance at the retinal surface in high magnification, improved field of view, higher dynamic range that reduces instrument glare and illuminates shadows, and digital image filtering to enhance visualization without the use of vital dyes. It was reported to be applied in vitreoretinal surgery by several surgeons.[1,2,3] Up to now, no study aimed at the use of NGENUITY 3D in anterior segment surgery. Here, we sought to evaluate the safety and efficiency of NGENUITY 3D in cataract phacoemulsification and IOL implantation.
Methods
Our study was conducted as a prospective, randomized, controlled, clinical trial from November 2017 to December 2017, and included patients diagnosed with age-related cataract. The study was conducted in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Institutional Review Board approval was obtained. All patients received phacoemulsification and IOL implantation and were randomized into two groups. In one group, the conventional OPMI Lumera T surgical microscope (Carl Zeiss Surgical GmbH, Oberkochen, Germany) was used, and in another group, the NGENUITY 3D visualization system (Alcon Laboratories) was applied. Each step of the surgical technique in NGENUITY 3D group did not differ from the conventional cataract surgery, except that the surgeon looked forward at a monitor during the entire duration of the surgical procedure. All surgeries were performed by one surgeon. Clinical data and surgical parameters such as age, grades of cataracts, surgical time, pre and postoperative best-corrected visual acuity (BCVA), intraocular pressure (IOP), and endothelial cell density (ECD) were recorded. BCVA was measured using a decimal chart and was converted into LogMAR for statistical purposes. Cataracts were divided into soft (I), semi-soft (II), medium hard (III), hard (IV), and rock-hard (V) according to the Emery–Little lens opacities classification system. The follow-up period was 1 month. Paired Student's t-test was used for the comparison within groups while independent sample t-test was used for comparison among groups (SPSS, Inc., Chicago, IL, USA).
visualization system (Alcon Laboratories) was applied. Each step of the surgical technique in NGENUITY 3D group did not differ from the conventional cataract surgery, except that the surgeon looked forward at a monitor during the entire duration of the surgical procedure. All surgeries were performed by one surgeon. Clinical data and surgical parameters such as age, grades of cataracts, surgical time, pre and postoperative best-corrected visual acuity (BCVA), intraocular pressure (IOP), and endothelial cell density (ECD) were recorded. BCVA was measured using a decimal chart and was converted into LogMAR for statistical purposes. Cataracts were divided into soft (I), semi-soft (II), medium hard (III), hard (IV), and rock-hard (V) according to the Emery–Little lens opacities classification system. The follow-up period was 1 month. Paired Student's t-test was used for the comparison within groups while independent sample t-test was used for comparison among groups (SPSS, Inc., Chicago, IL, USA).
Results
Eighteen patients (20 eyes) with an average age of 67 ± 5.2 years (range: 62–75) were included and randomly divided into two groups. In the conventional group, a total of 3, 4, and 3 eyes were classified as grade II, III, and IV, respectively, whereas in the NGENUITY 3D group the number of eyes were 3, 5, and 2, respectively. Mean LogMAR BCVA was 0.53 ± 0.37 before surgery and 0.09 ± 0.14 at 1 month after surgery in the conventional group, while in the NGENUITY 3D group it was 0.53 ± 0.30 before surgery and 0.19 ± 0.25 at 1 month after surgery. No difference was found in the pre and postoperative BCVA between the two groups (P > 0.05). Significant improvement of BCVA after cataract surgery was found in both groups (P < 0.05). After surgery, mean ECD decreased from 2733.29 ± 366.40 cells/mm2 to 2158.96 ± 402.53 cells/mm2 in the conventional group and from 2521.05 ± 386.69 cells/mm2 to 1824.82 ± 497.91 cells/mm2 in the NGENUITY 3D group (P < 0.05). Loss of ECD was observed in both groups, however, there was no significant difference in the pre and postoperative mean ECD between the NGENUITY 3D group and the conventional group (P > 0.05). The mean surgery time in the 3D group was 498 ± 104 s, whereas in the conventional group was 542 ± 88.6 s, and there was no significant difference between the duration of surgery in the two groups (P > 0.05). The clinical characteristics of the patients in the present study is presented in Table 1. No major complications such as posterior capsule rupture, decompensation of corneal endothelium, or suprachoroidal expulsive hemorrhage occurred during and after the surgery in either group. Examples of anterior segment photography of patients from both groups after surgery are shown in Fig. 1.
Table 1.
Clinical characteristics of patients in the present study
| Conventional group | NGENUITY 3D group | P | |
|---|---|---|---|
| Pre-operative BCVA | 0.53±0.37 | 0.53±0.30 | P=0.651 |
| Post-operative BCVA | 0.09±0.14 | 0.19±0.25 | P=0.104 |
| Pre-operative ECD | 2733.29±366.40 | 2521.05±386.69 | P=0.710 |
| Post-operative ECD | 2158.96±402.53 | 1824.82±497.91 | P=0.329 |
| Surgery time | 542±88.6 | 498±104 | P=0.543 |
BCVA=Best corrected visual acuity (LogMAR), ECD=Endothelial cell density (cells/mm2)
Figure 1.

Anterior segment photography of patients presented transparent cornea and silent anterior segment in both groups 24 hours after surgery
Discussion
Until now, most studies using the NGENUITY 3D system focused on its application in vitreoretinal surgery for its advantage of lower endoillumination level and higher depth of field. To our knowledge, the application of this system in cataract surgery has not been reported. Compared with vitreoretinal surgery, the manipulation space in cataract surgery is smaller. Therefore, it is essential to verify whether the use of monitor and polarized glasses instead of a conventional microscope will lead to more surgical trauma and worse postoperative outcome. This small prospective, randomized clinical trial demonstrated the safety and efficacy of NGENUITY 3D system in phacoemulsification and IOL implantation surgery. No difference in the postoperative BCVA or postoperative ECD was found between the conventional and the NGENUITY 3D group. In our experience, the new system was not only reliable during the surgical procedure but also showed good ergonomic qualities. The surgeon felt comfortable with no need to lean forward toward the microscope [Fig. 2]. The surgeon also adapted to the use of the 3D system quickly and without too much effort. Barakat reported an analysis of 32 consecutive cases (retinal surgery) with no increase in surgical times or complication rates when using the 3D digital system.[4] Similarly, in our study, the surgical time did not increase in the NGENUITY 3D system group. The surgeon felt a seamless transition from the use of conventional microscope to the 3D technique. Another advantage of the NGENUITY 3D system is it improved capability in visualization of surgery for teaching purposes. Chhaya et al. recently demonstrated that the use of 3D visualization enhances the learning benefit of intraocular ophthalmic surgeries.[5] In our experience, with the NGENUITY 3D visualization system, the physicians in training were able to see exactly what the surgeon was seeing – at the same depth, with the same focus, and with excellent clarity, which was helpful for surgical training.
Figure 2.
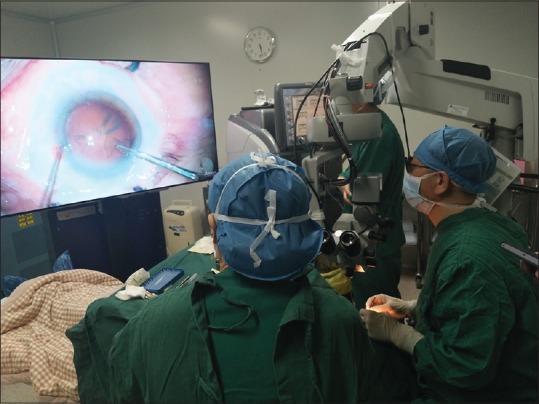
In a case of cataract surgery NGENUITY 3D system was used for capsulorhexis. There was no need for the surgeon to lean forward or even to sit straight up
One potential limitation of NGENUITY 3D system may be the 0.09-s delay of the image shown on the monitor compared to the image seen directly under the microscope. This lag is more obvious in anterior segment maneuvers because surgical manipulations in the anterior chamber are usually faster compared to the ones in the posterior chamber.[6] However, in this study, our impression was that this lag was not too noticeable and did not make much of a difference.
Conclusion
The heads-up 3D vision system is suitable and safe for cataract phacoemulsification and IOL implantation. Further studies with increased number of surgeries using NGENUITY 3D system are required to improve the estimate for safety and efficacy and evaluate long-term results. The learning curve for this system for different surgeons should also be investigated.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The author would like to give our sincere gratitude to Professor Rad Tezkow who gave us great help by providing careful revision and advises of great value. Without his strong support, this thesis could not been the present form.
References
- 1.Yonekawa Y, Thanos A, Abbey AM, Thomas BJ, Todorich B, Faia LJ, et al. Hybrid 25- and 27-gauge vitrectomy for complex vitreoretinal surgery. Ophthalmic Surg Lasers Imaging Retina. 2016;47:352–5. doi: 10.3928/23258160-20160324-08. [DOI] [PubMed] [Google Scholar]
- 2.Yonekawa Y, Thomas BJ, Hassan TS. New self-retaining sutureless cellulose flanged disposable contact viewing system for vitreoretinal surgery. Retina. 2015;35:834–7. doi: 10.1097/IAE.0000000000000522. [DOI] [PubMed] [Google Scholar]
- 3.Eckardt C, Paulo EB. Heads-up surgery for vitreoretinal procedures: an experimental and clinical study. Retina. 2016;36:137–47. doi: 10.1097/IAE.0000000000000689. [DOI] [PubMed] [Google Scholar]
- 4.Barakat M. Learning to use a stereoscopic display with retinal surgery does not increase surgical time or negatively affect outcomes. Poster presented at: 2016 Association for Research in Vision and Ophthalmology annual meeting, Seattle, WA. 2016 May 4; [Google Scholar]
- 5.Chhaya N, Helmy O, Piri N, Palacio A, Schaal S. Comparison of 2D and 3D video displays for teaching vitreoretinal surgery. Retina. 2018;38:1556–61. doi: 10.1097/IAE.0000000000001743. [DOI] [PubMed] [Google Scholar]
- 6.Yoshihiro Y. Seeing the world through 3-D glasses: Grab some pearls for the coming world of 3-D heads-up surgery. Retina Today. 2016:54–60. [Google Scholar]