

Case Report
A 13-year-old boy presented with complaints of gradual, painless diminution of vision in both eyes for 3 years. On examination, best-corrected visual acuity was the right eye (RE) 6/24 and the left eye (LE) 6/36, with a refractive error of −14.50DS/−0.75DC × 40° and −16.00DS/−1.00DC × 140°, respectively. Intraocular pressure (IOP) was 10 mmHg and 18 mmHg in the RE and LE, respectively (highest baseline IOP of LE was 34 mmHg) on topical prostaglandin-analogue and beta-blocker (fixed dose combination). On slit-lamp examination, both eyes showed prominent Schwalbe's line with a shallow anterior chamber (AC). Bilateral iris showed stromal thinning. The right pupil showed ectropion uveae and corectopia, while the left had ~270° posterior synechiae with corneo-iridic adhesions [Fig. 1a and b]. Angles were not visible on gonioscopy due to shallow AC, however, broad peripheral iris strands were seen in the RE. Fundus examination of the RE showed cup-disc-ratio of 0.4:1 and the LE could not be visualized due to non-dilating pupil, ultrasound B-scan was anechoic. Biometry revealed an axial length of 22.87 mm and 23.01 mm. On ultrasound biomicroscopy, the AC depth was 0.97 mm and 0.55 mm, lens equatorial diameter 6.56 mm and 6.87 mm, lens thickness 4.06 mm and 4.09 mm in the RE and LE, respectively [Fig. 1c and d].
Figure 1.
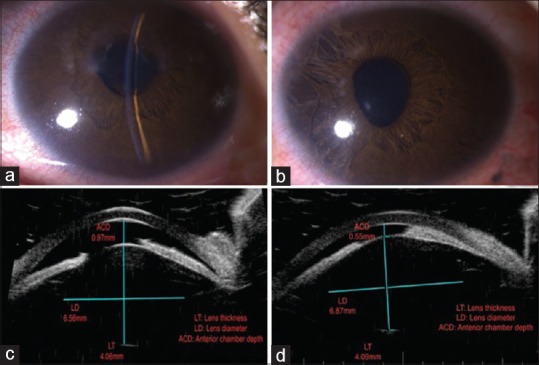
(a) Slit-lamp photograph of the right eye showing shallow anterior chamber and irregular pupil with iris stromal defects temporally. (b) Slit-lamp photograph of the left eye showing shallow anterior chamber with iridocorneal contact temporally and posterior embryotoxon. (c) Ultrasound biomicroscopy picture of the right eye showing anteriorly displaced lens with increased lens thickness (4.06 mm) and decreased equatorial diameter (6.56 mm). (d) Ultrasound biomicroscopy picture of the left eye showing anteriorly displaced lens with increased lens thickness (4.09 mm) and decreased equatorial diameter (6.87 mm)
General examination showed marfanoid habitus, but did not satisfy the Ghent's criteria for Marfan's syndrome.[1] Hence a diagnosis of microspherophakia with Axenfeld-Rieger anomaly with glaucoma was made. RE Nd-YAG peripheral iridotomy and LE lensectomy were performed. The IOP on 4-weeks follow-up was RE 10 mmHg and LE 14–16 mmHg (on topical beta-blocker BD). The fundus of the LE showed a vertical cup-disc-ratio of 0.8:1 on follow-up. The patient was intolerant to aphakic contact lenses.
Discussion
A stout anteriorly displaced lens causing high myopia with normal axial length points to the diagnosis of microspherophakia. Our patient had shallow AC, steep lens curvature, iridolenticular-contact, decreased equatorial diameter, and lenticular myopia, all characteristic of microspherophakia.[2] It causes pupillary block and inverse glaucoma. Axenfeld-Rieger anomaly causes developmental glaucoma, due to angle dysgenesis. Our patient manifested with features of both propounding the heightened risk of this “dual mechanism” glaucoma.[2,3,4,5]
The recent concept of developing lens providing signal for iris and ciliary body development is of interest, implying that maldevelopment of the former could have led to the latter, questioning their independency.[3,4,5]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Loeys BL, Genet JM. Revised Ghent criteria for the diagnosis of Marfan syndrome (MFS) and related conditions. J Med Genet. 2010;47:476–85. doi: 10.1136/jmg.2009.072785. [DOI] [PubMed] [Google Scholar]
- 2.Macken PL, Pavlin CJ, Tuli R, Trope GE. Ultrasound biomicroscopic features of spherophakia. Aust NZ J Ophthalmol. 1995;23:217–20. doi: 10.1111/j.1442-9071.1995.tb00160.x. [DOI] [PubMed] [Google Scholar]
- 3.Rastogi A, Goel S, Kaur S, Vardhan P. Microspherophakia associated with Axenfeld-Rieger syndrome. J AAPOS. 2010;14:364–6. doi: 10.1016/j.jaapos.2010.03.004. [DOI] [PubMed] [Google Scholar]
- 4.Satana B, Altan C, Basarir B, Alkin Z, Yilmaz OF. A new combined surgical approach in a patient with microspherophakia and developmental iridocorneal angle anomaly. Nepalese J Ophthalmol. 2015;7:85–9. doi: 10.3126/nepjoph.v7i1.13178. [DOI] [PubMed] [Google Scholar]
- 5.Thut CJ, Rountree RB, Hwa M, Kingsley DM. A large-scale in situ screen provides molecular evidence for the induction of eye anterior segment structures by the developing lens. Dev Biol. 2001;231:63–76. doi: 10.1006/dbio.2000.0140. [DOI] [PubMed] [Google Scholar]