

Overview
Introduction
In our experience, a supramalleolar osteotomy with or without calcaneal osteotomy and midfoot osteotomy has been an effective treatment for sequelae resulting from overcorrected clubfoot deformity.
Step 1: Preoperative Assessment and Planning
Determine the treatment using the decisional algorithm in Figure 3.






Step 2: Patient Positioning
Use spinal or general anesthesia, administer intravenous antibiotics, position the patient supine, apply a tourniquet.
Step 3: Medial Approach to the Distal Part of the Tibia
Use a medial approach to expose the distal part of the tibia.



Step 4: Supramalleolar Osteotomy
Remove the bone wedge, close the osteotomy, and use rigid plate fixation to secure the correction.



Step 5: Additional Procedures (If Necessary)
If necessary, perform fibular osteotomy, calcaneal osteotomy, and/or plantar flexion osteotomy of the first cuneiform.



Step 6: Closure of All Incisions and Postoperative Care
A short leg splint is worn for two days, followed by partial weight-bearing with the ankle protected in a splint at night and a walking boot during the day for eight weeks.
Results
Between 2002 and 2009, fourteen adult patients (mean age, thirty-seven years; range, nineteen to sixty-six years) who presented with a symptomatic overcorrected clubfoot deformity were treated with a supramalleolar osteotomy.
What to Watch For
Introduction
In our experience, a supramalleolar osteotomy with or without calcaneal osteotomy and midfoot osteotomy has been an effective treatment for sequelae resulting from overcorrected clubfoot deformity.
The prevalence of ankle valgus in patients treated for clubfoot deformity has been reported to be up to 67%1. Clinically, patients with overcorrected clubfoot deformity often present with calcaneofibular impingement, anterior ankle impingement due to a flat-top talus, and flatfoot deformity. Options for surgical treatment of symptomatic overcorrected clubfoot deformity include epiphysiodesis1,2 in skeletally immature patients and hindfoot fusions3,4 or corrective osteotomies5,6 in mature patients. Our technique for surgical correction of overcorrected clubfoot deformity is completed in six stages:
Step 1: Preoperative assessment and planning
Step 2: Patient positioning
Step 3: Medial approach to the distal part of the tibia
Step 4: Supramalleolar osteotomy
Step 5: Additional procedures (if necessary)
Step 6: Closure of all incisions and postoperative care
Step 1: Preoperative Assessment and Planning
Determine the treatment using the decisional algorithm in Figure 3.
Measure the angle of the distal tibial articular surface7 (normal, 91° to 93°), the tibiotalar angle8 (normal, 91.5° ± 1.2°), and the tibial lateral surface angle9,10 (normal, 83° ± 3.6°11) on weight-bearing radiographs.
- Distinguish two groups of patients according to the location of the deformity:
- ○ valgus deformity below the ankle joint
- ○ valgus deformity of the distal tibial articular surface angle
Determine the treatment using the decisional algorithm in Figure 3.
- Plan the surgical correction on anteroposterior, lateral, and hindfoot radiographs (Figs. 4-A, 4-B, and 4-C):
- ○ Draw the distal plane on the basis of the desired amount of correction. The height of the wedge to be removed is determined using the equation: tan α1 × W, where α1 is the amount of valgus deformity with the desired overcorrection and W is the width of the distal part of the tibia15.
- ○ Plan for an overcorrection of 3° to 5°.
Fig. 3.

Decisional algorithm for the treatment of overcorrected clubfoot deformity. TAS = tibial articular surface angle, OT = osteotomy, and SMOT= supramalleolar osteotomy.
Fig. 1.

Illustration of subfibular impingement in a patient with overcorrected clubfoot deformity.
Fig. 2.

Illustration of anterior impingement in the ankle joint due to the flattened dome of the talus in a patient with clubfoot deformity.
Fig. 4-A.

Preoperative anteroposterior weight-bearing radiograph showing valgus deviation.
Fig. 4-B.

Preoperative lateral weight-bearing radiograph showing a flat-top talus.
Fig. 4-C.

Preoperative hindfoot weight-bearing radiograph showing lateral offset of the calcaneus.
Fig. 5.
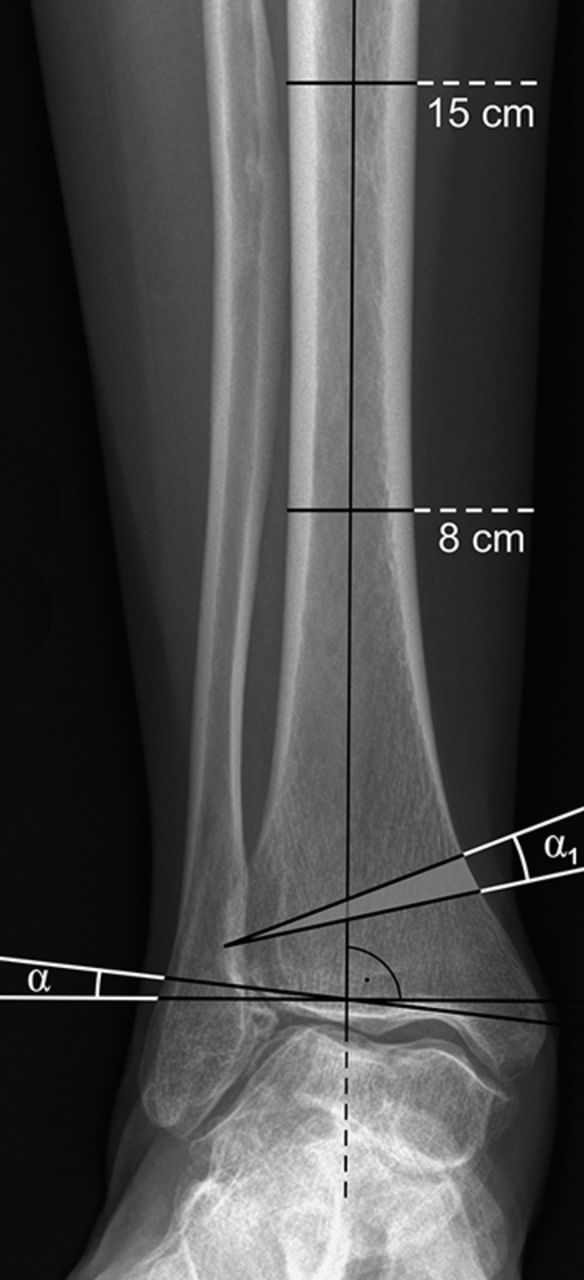
Preoperative radiograph used for the planning of a medial closing-wedge osteotomy in a patient with an overcorrected flatfoot deformity. The angle of the distal tibial joint surface (α) and the tibiotalar angle are shown. The angle α1 is the planned surgical correction.
Fig. 6.

Preoperative radiograph showing the tibial lateral surface angle (β) and the planned anterior wedge removal (gray wedge).
Step 2: Patient Positioning
Use spinal or general anesthesia, administer intravenous antibiotics, position the patient supine, apply a tourniquet.
Use spinal or general anesthesia for the reconstruction.
Use a single prophylactic dose of intravenous antibiotics within twenty minutes prior to the start of surgery.
Position the patient supine on a radiolucent operating table.
Apply a tourniquet on the ipsilateral thigh and exsanguinate the limb prior to inflating the tourniquet.
Step 3: Medial Approach to the Distal Part of the Tibia
Use a medial approach to expose the distal part of the tibia.
Use a medial approach to expose the distal part of the tibia posterior to the greater saphenous vein and the saphenous nerve (Fig. 7).
Protect the posterior tibial tendon, which lies directly behind (posterior to) the medial malleolus. Retract the tendon posteriorly without opening the tendon sheath to visualize the dorsal surface of the distal part of the tibia.
Determine the plane of the osteotomy under fluoroscopy. Place a Kirschner wire from the medial to the lateral cortex, exiting the bone slightly proximal to the former growth plate, respecting the anatomical axis of the ankle joint (anteromedial to posterolateral).
Use a second Kirschner wire to mark the second cut based on the preoperative planning (Fig. 8).
For biplanar osteotomies in ankles with anterior and subfibular impingement, use anterior and medial closing-wedge osteotomies.
Incise the periosteum at the level of the osteotomy and elevate it off the bone using a scalpel or periosteal elevator (Fig. 9).
Fig. 7.

Marking of the location of the approach to the distal part of the tibia.
Fig. 8.

Intraoperative radiograph of the guidewires for the tibial osteotomy.
Fig. 9.

Intraoperative image of the guides and the subperiosteal placement of the Hohmann retractors.
Step 4: Supramalleolar Osteotomy
Remove the bone wedge, close the osteotomy, and use rigid plate fixation to secure the correction.
Perform the cuts with a wide saw blade and continuous irrigation.
Pay attention to preserving the lateral tibial cortex as a hinge.
Remove the bone wedge (Fig. 10) and close the osteotomy.
Use rigid plate fixation with interlocking screws (such as TIBIAXYS; Integra LifeSciences/Newdeal, Lyon, France) to secure the correction (Figs. 11 through 12-C). Alternatively, a 3.5-mm LCP T-plate (distal radial plate) can be used.
Fix the plate first distally. Then apply compression (manually or with a compression device [Integra LifeSciences/Newdeal]) to the osteotomy site and secure the plate proximally.
Close the periosteum over the osteotomy site with number-2-0 absorbable sutures.
Fig. 10.

Removal of the bone wedge after the osteotomy.
Fig. 11.

Fixation of the correction with a plate with interlocking screws.
Fig. 12-C.

Intraoperative lateral radiograph showing the correction of the distal part of the tibia in plantar flexion.
Fig. 12-A.

Intraoperative radiograph showing correction of the distal articular surface angle in the patient shown in Figs. 4-A, 4-B, and 4-C.
Fig. 12-B.

Intraoperative lateral radiograph showing the correction of the distal part of the tibia in dorsiflexion.
Step 5: Additional Procedures (If Necessary)
If necessary, perform fibular osteotomy, calcaneal osteotomy, and/or plantar flexion osteotomy of the first cuneiform.
Fibular Osteotomy
Check the congruency of the ankle mortise under fluoroscopy after correction of the distal tibial joint surface.
Osteotomize the fibula in cases of joint incongruency due to inadequate length or position of the fibula (i.e., if the fibula is too short or there is increased lateral clear space), or if the talus does not follow the medial malleolus (increased medial clear space)12,16,17.
Expose the distal part of the fibula through a longitudinal, slightly curved incision.
Visualize the anterior syndesmosis at the distal end of the incision.
The lateral branch of the sural nerve and the short saphenous vein run posterior to the line of the incision and are usually not seen during this procedure.
Incise and mobilize the periosteum carefully with a scalpel or the periosteal elevator.
Using an oscillating saw, create an oblique cut starting from the insertion of the anterior syndesmosis of the fibula and exiting the fibula posteriorly (Fig. 13).
Adjust the length of the fibula under fluoroscopic control until a congruent joint is achieved (equal medial and lateral clear spaces), and secure the correction with a one-third tubular plate.
Fig. 13.

Orientation of the fibular osteotomy.
Calcaneal Osteotomy
Clinically reassess the alignment of the heel after the supramalleolar correction.
Add an osteotomy of the calcaneus when the heel remains in a valgus position after the supramalleolar correction18.
Use a lateral approach to the calcaneus. Place the incision approximately 1 cm posterior and parallel to the peroneal tendons (Fig. 14).
Pay attention to avoiding the branches of the sural nerve.
Insert a small Hohmann retractor on the plantar aspect of the calcaneus and a second one over the calcaneus in the dorsal concavity.
Use an oscillating saw to create the osteotomy.
Medialize the tuberosity with a Hohmann retractor after mobilizing it with a laminar spreader (Fig. 15).
Secure the correction with one or two cannulated 5.5 or 7.5-mm screws.
Fig. 14.

Marking of the location of the approach for the calcaneal displacement osteotomy.
Fig. 15.

Intraoperative image showing the medial displacement of the calcaneal tuberosity.
Plantar Flexion Osteotomy of the First Cuneiform
Consider a plantar flexion osteotomy of the first cuneiform19 in a patient with fixed forefoot supination.
Incise the skin at the dorsal aspect of the first cuneiform. Place the incision medial to the extensor hallucis longus tendon.
Using a small saw blade, complete the osteotomy in the oblique direction from the distal and dorsal aspect of the foot to the proximal and plantar aspect.
Greenstick the plantar cortex and plantar flex the medial column gently.
Use the wedge of bone obtained from the correction of the tibia to fill the resulting gap.
Secure the correction with cannulated 3.0-mm screws placed from proximal dorsal to distal plantar.
Step 6: Closure of All Incisions and Postoperative Care
A short leg splint is worn for two days, followed by partial weight-bearing with the ankle protected in a splint at night and a walking boot during the day for eight weeks.
Close all incisions with interrupted, nonabsorbable sutures and apply a well-padded short leg splint to support the foot in a neutral position for two days.
Allow partial weight-bearing with the ankle protected in a splint at night and in a walking boot during the day for eight weeks.
After eight weeks, allow full weight-bearing and initiate physiotherapy.
Results
Between 2002 and 2009, fourteen adult patients (mean age, thirty-seven years; range, nineteen to sixty-six years) who presented with a symptomatic overcorrected clubfoot deformity were treated with a supramalleolar osteotomy20. Five patients underwent an additional calcaneal osteotomy and five patients required an additional plantar flexion osteotomy of the first cuneiform in order to achieve a well-aligned and plantigrade foot. At a mean of 50.6 ± 27.8 months (range, 24.0 to 98.8 months) after surgery, the mean American Orthopaedic Foot & Ankle Society (AOFAS) score, visual analogue scale (VAS) score for pain, and range of motion were significantly improved (p < 0.05). In all cases, the orientation of the distal tibial articular surfaces was normalized and calcaneofibular/anterior ankle impingement was resolved.
What to Watch For
Indications
Medial Closing-Wedge Supramalleolar Osteotomy
Lateral ankle joint impingement with valgus malalignment of the tibiotalar joint line
Anterior ankle joint impingement
Early stages of lateral ankle joint arthritis
Calcaneal Osteotomy
Valgus malalignment below the ankle joint line
Remaining subtalar valgus deformity after correction of the supramalleolar alignment
Plantar Flexion Osteotomy of the First Cuneiform
Supinated forefoot after correction of the supramalleolar alignment (preexisting deformity may be amplified by the correction of the hindfoot)
Collapse of the medial arch of the foot
Concomitant flatfoot deformity
Contraindications
Absolute
Acute localized soft-tissue infection
Severe vascular or neurological deficiency in the affected extremity
Neuropathic disorders (e.g., Charcot foot)
Severe hindfoot instability that cannot be stabilized
Relative
End-stage ankle joint arthritis
Altered bone quality (due to medication, large cysts, or osteopenia or osteoporosis)
Age of more than seventy years
Insulin-dependent diabetes
Smoking
Pitfalls & Challenges
Supramalleolar Osteotomy
Tendon laceration. Protect the extensor tendons and the posterior tibial tendon by subperiosteal placement of a Hohmann retractor during the saw cut. If the posterior tibial tendon is extensively scarred due to the previous procedures, expose the tendon through a minimal incision and then retract it posteriorly13.
Accidental saw cut through the lateral cortex. Particularly in biplanar corrections, it may not be possible to preserve the lateral cortex as a hinge for the medial closing-wedge osteotomy. This increases the risk of malrotation or secondary loss of correction. Mark the rotation of the distal fragment prior to the osteotomy with an electrocautery to avoid malrotation. Secondary loss of correction is avoided by the use of implants with interlocking screws or adding a second plate in a second plane.
Malpositioning of the joint line. Use careful preoperative planning and fluoroscopy during the surgery to ensure proper closure of the osteotomy site and joint congruency.
Calcaneal Osteotomy
Sural nerve injury. Expose the lateral wall of the calcaneus carefully to avoid damage to the nerve. In our experience, it is usually not necessary to expose the nerve.
Postoperative irritation of the peroneal tendons and wound-healing problems. After the displacement, impact the lateral rim of the tuberosity to reduce the bleeding surface of the bone and soft-tissue strain.
Clinical Comments
In our original paper20, the osteotomy of the fibula was not included. Newer findings suggest that a main risk factor for failure after a supramalleolar osteotomy is an incongruent ankle joint12,17. In the future, we will pay more attention to the length and position of the fibula and consider an additional corrective fibular osteotomy in patients with an incongruent joint after the correction of the distal articular surface angle.
Overcorrection after surgical treatment for clubfoot deformity has been reported to occur in up to 67% of patients1. Furthermore, 70% of the inferior results after surgical correction of clubfoot deformity are reported to be due to overcorrection.
Not recognizing the origin of the deformity may lead to inappropriate flatfoot surgery.
The closing-wedge type of osteotomy may not be adequate for large deformities as this may lead to excessive translation of the calcaneal tuberosity. In these cases, the use of a dome-shaped osteotomy should be considered.
Patients with an overcorrected clubfoot frequently present with a flatfoot. It is currently unknown how aggressively medial arch collapse should be addressed in these patients.
Based on an original article: J Bone Joint Surg Am. 2012 Aug 1;94(15):e110.
Disclosure: One or more of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of an aspect of this work. In addition, one or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission of this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. No author has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article.
References
- 1. Stevens PM Otis S. Ankle valgus and clubfeet. J Pediatr Orthop. 1999 Jul-Aug;19(4):515-7. [DOI] [PubMed] [Google Scholar]
- 2. Burghardt RD Herzenberg JE Standard SC Paley D. Temporary hemiepiphyseal arrest using a screw and plate device to treat knee and ankle deformities in children: a preliminary report. J Child Orthop. 2008 Jun;2(3):187-97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Scott SM Janes PC Stevens PM. Grice subtalar arthrodesis followed to skeletal maturity. J Pediatr Orthop. 1988 Mar-Apr;8(2):176-83. [PubMed] [Google Scholar]
- 4. Brodsky JW. The adult sequelae of treated congenital clubfoot. Foot Ankle Clin. 2010 Jun;15(2):287-96. [DOI] [PubMed] [Google Scholar]
- 5. Uglow MG Kurup HV. Residual clubfoot in children. Foot Ankle Clin. 2010 Jun;15(2):245-64. [DOI] [PubMed] [Google Scholar]
- 6. Becker AS Myerson MS. The indications and technique of supramalleolar osteotomy. Foot Ankle Clin. 2009 Sep;14(3):549-61. [DOI] [PubMed] [Google Scholar]
- 7. Hall R. The use of osteotomy to correct foot and ankle disorders. : Myerson M, editor Foot and ankle disorders. Philadelphia: WB Sanders; 2000. p 999-1016. [Google Scholar]
- 8. Tanaka Y Takakura Y Fujii T Kumai T Sugimoto K. Hindfoot alignment of hallux valgus evaluated by a weightbearing subtalar x-ray view. Foot Ankle Int. 1999 Oct;20(10):640-5. [DOI] [PubMed] [Google Scholar]
- 9. Takakura Y Tanaka Y Kumai T Tamai S. Low tibial osteotomy for osteoarthritis of the ankle. Results of a new operation in 18 patients. J Bone Joint Surg Br. 1995 Jan;77(1):50-4. [PubMed] [Google Scholar]
- 10. Lee WC Moon JS Lee K Byun WJ Lee SH. Indications for supramalleolar osteotomy in patients with ankle osteoarthritis and varus deformity. J Bone Joint Surg Am. 2011 Jul 6;93(13):1243-8. [DOI] [PubMed] [Google Scholar]
- 11. Magerkurth O Knupp M Ledermann H Hintermann B. Evaluation of hindfoot dimensions: a radiological study. Foot Ankle Int. 2006 Aug;27(8):612-6. [DOI] [PubMed] [Google Scholar]
- 12. Knupp M Stufkens SA Bolliger L Barg A Hintermann B. Classification and treatment of supramalleolar deformities. Foot Ankle Int. 2011 Nov;32(11):1023-31. [DOI] [PubMed] [Google Scholar]
- 13. Knupp M Stufkens S Pagenstert G Hintermann B Valderrabano V. Supramalleolar osteotomy for tibiotalar varus malalignment. Tech Foot Ankle Surg. 2009;8(1):17-23. [Google Scholar]
- 14. Knupp M Pagenstert G Valderrabano V Hintermann B. [Osteotomies in varus malalignment of the ankle]. Oper Orthop Traumatol. 2008 Sep;20(3):262-73. [DOI] [PubMed] [Google Scholar]
- 15. Warnock KM Johnson BD Wright JB Ambrose CG Clanton TO McGarvey WC. Calculation of the opening wedge for a low tibial osteotomy. Foot Ankle Int. 2004 Nov;25(11):778-82. [DOI] [PubMed] [Google Scholar]
- 16. Knupp M Stufkens SA van Bergen CJ Blankevoort L Bolliger L van Dijk CN Hintermann B. Effect of supramalleolar varus and valgus deformities on the tibiotalar joint: a cadaveric study. Foot Ankle Int. 2011 Jun;32(6):609-15. [DOI] [PubMed] [Google Scholar]
- 17. Stufkens SA van Bergen CJ Blankevoort L van Dijk CN Hintermann B Knupp M. The role of the fibula in varus and valgus deformity of the tibia: a biomechanical study. J Bone Joint Surg Br. 2011 Sep;93(9):1232-9. [DOI] [PubMed] [Google Scholar]
- 18. Stufkens S Knupp M Hintermann B. Medial displacement calcaneal osteotomy. Tech Foot Ankle Surg. 2009;8(2):85-90. [Google Scholar]
- 19. Hirose CB Johnson JE. Plantarflexion opening wedge medial cuneiform osteotomy for correction of fixed forefoot varus associated with flatfoot deformity. Foot Ankle Int. 2004 Aug;25(8):568-74. [DOI] [PubMed] [Google Scholar]
- 20. Knupp M Barg A Bolliger L Hintermann B. Reconstructive surgery for overcorrected clubfoot in adults. J Bone Joint Surg Am. 2012 Aug 1;94(15):e110. [DOI] [PubMed] [Google Scholar]