

Abstract
Rationale:
Advanced ovarian malignancies are associated with poor overall survival; thus, patients often turn to alternative treatments, despite the controversy surrounding their use. Mistletoe extract has been commonly used as complementary medicine to treat patients with cancer for several decades, and has proven benefits in integrative oncology.
Patient concerns:
A 47-year-old woman with stage IVB ovarian cancer who underwent optimal surgical cytoreduction, but whose disease persisted after adjuvant platinum-based combination chemotherapy and 2nd-line chemotherapy.
Diagnosis and interventions:
The patient discontinued chemotherapy due to her septic condition and acute kidney injury accompanied by acute pyelonephritis, and opted for adjuvant treatment with mistletoe extract.
Outcomes:
The patient has achieved good health without progression of cancer or ascites over the 42 months since the 1st diagnosis and 24 months since the last relapse.
Lessions:
Our case suggests that mistletoe extract can produce favorable outcomes in patients with platinum-refractory ovarian cancer.
Keywords: complementary and alternative medicine, helixor, mistletoe extract, ovarian cancer, platinum-refractory
1. Introduction
Ovarian cancer is widely known as the most lethal disease among gynecological malignancies. Although many treatment methods, including surgery, chemotherapy, radiotherapy, and hormonal and targeted therapy, are well established, these therapies are less effective for advanced-stage disease, and recurrence remains an issue in patients with ovarian cancer due to the side effects and the risk of toxicity to normal cells.[1] Thus, adjuvant options for ovarian cancer treatment must be identified. Complementary and alternative medicine (CAM) has been developed in the recent years and is gaining interest.[2]
Among CAM therapies, mistletoe extracts are the herbal extracts applied most commonly to treat cancer.[3] Helixor is a commonly used mistletoe product that we administered to our patient. It is an aqueous cold extract made from white-berry mistletoe (Viscum album), which grows on various trees. The immunoprotective and tumor-inhibiting properties of mistletoe extract are attributable primarily to the glycoprotein lectin.[4] Mistletoe extracts have been shown anticancer effect reducing cancer cell viability in various in-vitro studies.[4] Mistletoe treatments are used primarily to improve quality of life (QOL) during conventional therapy, to increase tolerability to chemotherapy, and to exert beneficial effects on tumor control and survival.[5,6] Repeated intraperitoneal administration of mistletoe extract can reduce fluid accumulation in patients with malignant ascites.[7] Here, we report the case of a patient with ovarian cancer who developed progressive disease after conventional 2nd-line chemotherapy, but achieved stable disease status after 24 months of treatment with a mistletoe product as an alternative therapy.
2. Case report
A 47-year-old female patient who presented with painless abdominal distension over 2 months was referred to our institution for evaluation and treatment. She had no specific medical history except for abdominal distension and dyspnea. The abdomen was distended with bulging flanks, dullness to percussion, and a positive shifting dullness. Her serum CA 125 level was 768 IU/mL (Fig. 1) and her C-reactive protein level was elevated. Computed tomography (CT) of the abdomen and pelvis revealed cancer peritonitis with peritoneal seeding around both ovaries and the uterus, liver, and spleen, with omental cake formation and ascites (Fig. 2A). Although CT did not reveal the primary origin of the mass, ovarian malignancy was strongly suspected and the patient was referred to the gynecological oncology department for exploratory laparotomy. Both ovaries had irregular cauliflower shapes, and multiple tiny seeding nodular lesions were present on the colon, liver, bladder, omentum, and diaphragm. Approximately 4000 mL clear to pale yellow ascites was present in the abdominal cavity; thus, peritoneal cytological analysis was performed. Pathological analysis of a frozen section of the ovarian surface raised the suspicion of serous carcinoma of the ovary; thus, the patient underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, partial omentectomy, appendectomy, pelvic and para-aortic lymph node dissection, cholecystectomy, falciform ligament excision, and diaphragmatic wedge resection in the departments of thoracic surgery and general surgery. Optimal debulking was achieved.
Figure 1.
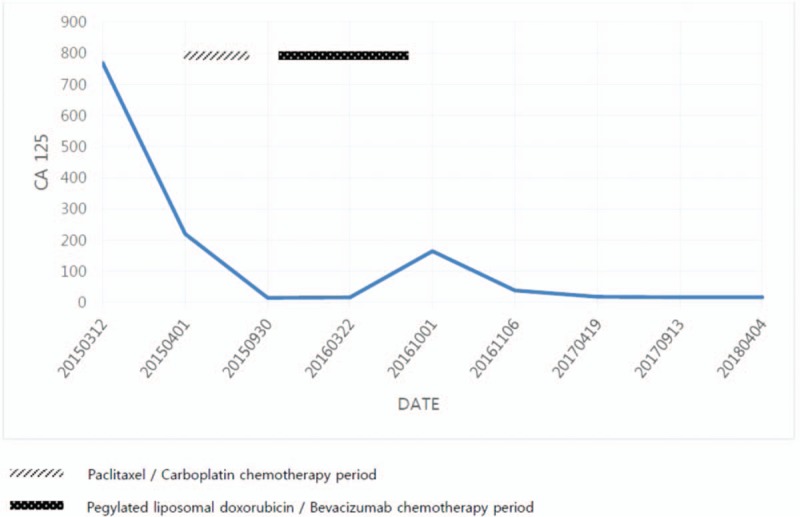
Plot of CA 125 from initial diagnosis (March 2015) through recent date. Paclitaxel/Carboplatin chemotherapy from April 2015 through August 2015 and Pegylated liposomal doxorubicin/Bevacizumab chemotherapy from October 2015 through August 2016.
Figure 2.
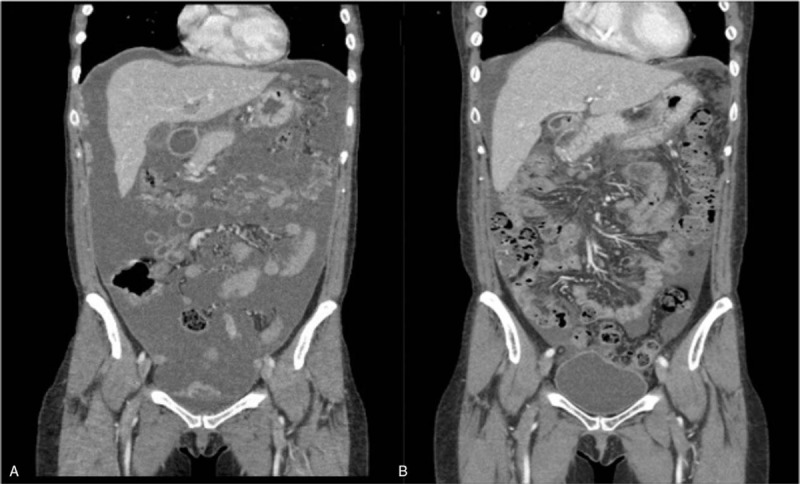
Computed tomography (CT) images. (A) Initial computed tomography images showing cancer peritonitis with massive ascites and peritoneal seeding of unknown primary origin. (B) CT after conventional chemotherapy showing progression of peritoneal carcinomatosis associated with large amount of ascites with increased peritoneal nodularites. CT = computed tomography.
Histopathological examination revealed high-grade (FIGO stage IVB) serous ovarian carcinoma with metastasis involving the diaphragm. The patient underwent adjuvant chemotherapy consisting of paclitaxel (175 mg/m2) and carboplatin (area under curve = 5) every 3 weeks beginning 3 weeks postoperatively. After 6 cycles of platinum-based chemotherapy, abdominopelvic CT revealed that the peritoneal carcinomatosis had progressed, and the patient began a regimen of 12 cycles of doxorubicin (40 mg/m2 every 4 weeks) and 23 cycles of bevacizumab (10 mg/kg every 2 weeks) as 2nd-line chemotherapy. Second-line chemotherapy was also ineffective, and the patient suffered from recurrent pancytopenia. Abdominopelvic CT revealed progression of the peritoneal carcinomatosis, with a large volume of ascites (Fig. 2B).
Repeated intraperitoneal administration of mistletoe extract was performed to reduce the accumulation of malignant ascites. The mistletoe extract was instilled intraperitoneally at doses of 100 to 500 mg/mL, 3 times per week for the 3 months of the patient's admission. The patient exhibited a clinical response and achieved stable disease status with a normal CA 125 level (Fig. 1). Additional chemotherapy was not deemed beneficial to the patient, and the CAM therapy was continued due to sepsis and acute kidney injury accompanied by acute pyelonephritis and an elevated creatinine level.
The patient received subcutaneous injections of mistletoe extract in escalating doses of 1 to 20 mg/mL for nearly 21 months. Because of the elevated creatinine level (3.32 mg/dL), abdominopelvic CT was not performed for 2 years, but the patient is continuing to undergo regular follow-up with pelvic examination, monitoring of tumor markers, and ultrasonography. Recent ultrasound findings demonstrated resolved pyelonephritis in Left kidney with decreased creatinine level of 1.24 to 35 mg/dL. To date, she has shown no evidence of disease recurrence; her CA 125 level has remained normal and she has been in stable condition for 24 months since the last relapse.
3. Discussion
The prognosis of platinum-refractory ovarian cancer is generally unfavorable, with a low response to additional chemotherapy.[8] Whether continued treatment of patients with advanced ovarian cancer who do not respond to conventional chemotherapy confers any advantage has remained a concern. Multiple lines of chemotherapy provide no overall survival advantage over 1 or 2 lines in patients with advanced ovarian cancer.[9]
Patients with gynecological malignancies are the patient group that uses CAM the most.[10] Our case report describes an apparent response to mistletoe extract in a patient who was unable to endure conventional treatment. Mistletoe extract seems to contain oncologically relevant active substances that exert anticancer effects and appear to prolong overall survival and markedly increase QOL, without the recurrence of cancer or ascites.[7,11] Various clinical studies including matched-pair studies, placebo-controlled and even randomized studies suggests that cancer patients treated with the mistletoe extract had a increased survival rate.[12–15]
Moreover, the use of mistletoe extract for cancer therapy appears to have minimal and non–life-threatening side effects.[16] Mistletoe extract use is associated with a low risk of specific concerns, but the patient should be monitored carefully by a physician depending on the dosage, route of application, and individual tolerability.
The aim of this case report is to attract attention to the potential benefit of mistletoe extract use, but further clinical investigations are necessary. Although the anti-tumor effects of mistletoe are well documented in vitro, the clinical activity of mistletoe therapy remains controversial. Further qualitative clinical trials should examine antitumor activities in patients with ovarian cancer, and establish safety parameters and a standard dosage. Additional clinical studies will establish the progression-free survival time and potential advantages of mistletoe extract for patients with refractory responses to standard conventional treatments.
We hope that this case report will be of assistance to gynecologists encountering similar cases, as such a favorable prognosis in a patient with advanced-stage platinum-refractory ovarian cancer is unusual.
Acknowledgments
Patient has provided informed consent for publication of the case and the authors thank the patient for permission to publish her case descriptions.
Author contributions
Conceptualization: Ji Su Yeom.
Supervision: Min Hyung Jung.
Writing – original draft: Woo Yeon Hwang.
Writing – review & editing: Mi Hyun Kang, Seul Ki Lee, Ji Su Yeom.
Min Hyung Jung orcid: 0000-0002-1263-8533.
Footnotes
Abbreviations: CAM = complementary and alternative medicine, CT = computed tomography, QOL = quality of life.
The authors have no conflicts of interest to disclose.
References
- [1].Jelovac D, Armstrong DK. Recent progress in the diagnosis and treatment of ovarian cancer. CA Cancer J Clin 2011;61:183–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Swisher EM, Cohn DE, Goff BA, et al. Use of complementary and alternative medicine among women with gynecologic cancers. Gynecol Oncol 2002;84:363–7. [DOI] [PubMed] [Google Scholar]
- [3].Kienle GS, Glockmann A, Schink M, et al. Viscum album L. extracts in breast and gynaecological cancers: a systematic review of clinical and preclinical research. J Exp Clin Cancer Res 2009;28:79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Marvibaigi M, Supriyanto E, Amini N, et al. Preclinical and clinical effects of mistletoe against breast cancer. Biomed Res Int 2014;2014:785479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Kienle GS, Mussler M, Fuchs D, et al. Intravenous mistletoe treatment in integrative cancer care: a qualitative study exploring the procedures, concepts, and observations of expert doctors. Evid Based Complement Alternat Med 2016;2016:4628287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Zwierzina H, Bergmann L, Fiebig H, et al. The preclinical and clinical activity of aviscumine: a potential anticancer drug. Eur J Cancer (Oxford, England: 1990) 2011;47:1450–7. [DOI] [PubMed] [Google Scholar]
- [7].Bar-Sela G, Goldberg H, Beck D, et al. Reducing malignant ascites accumulation by repeated intraperitoneal administrations of a Viscum album extract. Anticancer Res 2006;26(1b):709–13. [PubMed] [Google Scholar]
- [8].Komiyama S, Kugimiya T, Takeya C, et al. Platinum-resistant recurrent ovarian cancer with long survival on bevacizumab and gemcitabine. J Obstet Gynaecol Res 2018;44:1330–4. [DOI] [PubMed] [Google Scholar]
- [9].Stathopoulos GP, Papadimitriou C, Aravantinos G, et al. Maintenance chemotherapy or not in ovarian cancer stages IIIA, B, C, and IV after disease recurrence. J BUON 2012;17:735–9. [PubMed] [Google Scholar]
- [10].Ben-Arye E, Schiff E, Steiner M, et al. Attitudes of patients with gynecological and breast cancer toward integration of complementary medicine in cancer care. Int J Gynecol Cancer 2012;22:146–53. [DOI] [PubMed] [Google Scholar]
- [11].Chase DM, Gibson SJ, Sumner DA, et al. Appropriate use of complementary and alternative medicine approaches in gynecologic cancers. Curr Treat Options Oncol 2014;15:14–26. [DOI] [PubMed] [Google Scholar]
- [12].Ostermann T, Raak C, Bussing A. Survival of cancer patients treated with mistletoe extract (Iscador): a systematic literature review. BMC cancer 2009;9:451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Kienle GS, Berrino F, Bussing A, et al. Mistletoe in cancer - a systematic review on controlled clinical trials. Eur J Med Res 2003;8:109–19. [PubMed] [Google Scholar]
- [14].Ernst E, Schmidt K, Steuer-Vogt MK. Mistletoe for cancer? A systematic review of randomised clinical trials. Int J Cancer 2003;107:262–7. [DOI] [PubMed] [Google Scholar]
- [15].Giordano SH, Buzdar AU, Smith TL, et al. Is breast cancer survival improving? Cancer 2004;100:44–52. [DOI] [PubMed] [Google Scholar]
- [16].Kienle GS, Grugel R, Kiene H. Safety of higher dosages of Viscum album L. in animals and humans--systematic review of immune changes and safety parameters. BMC 2011;11:72. [DOI] [PMC free article] [PubMed] [Google Scholar]