

Summary
Hepatitis E is a serious public health problem in developing countries. Most of the patients with Hepatitis E virus (HEV) infection present with typical acute hepatitis symptoms. However, in few patients it may lead to complications such as liver failure and extrahepatic symptoms. One of the rare extrahepatic presentations of this infection is neurological complications such as Guillain-Barré syndrome (GBS) which is observed in 5.5% of HEV infected patients (mainly in developed countries). Moreover, only genotype (gt) 3 HEV was found in association with GBS among patients in developed countries whereas molecular characterisation of HEV cases detected from developing countries have not been reported till now. Here, we are reporting a case of GBS as an extrahepatic complication of HEV associated with gt1 identified by molecular characterization by performing PCR of open-reading frame 2 (ORF2) region of HEV. Phylogenetic analysis by maximum likelihood method revealed that HEV gt1 case reported in this paper rooted closely with other HEV gt1 samples from South-Asian countries with high bootstrap values indicative of fully resolved tree.
Keywords: Hepatitis E virus, Guillain-Barré syndrome, genotype, sofosbuvir
1. Introduction
Hepatitis E is an enterically transmitted viral hepatitis caused by Hepatitis E virus (HEV) infection. It is a non-enveloped, single stranded RNA virus and the most common cause of acute sporadic hepatitis in all age groups (1). According to World Health Organization (WHO), there are 20 million Hepatitis E infections annually with over 3 million cases of acute hepatitis E infections resulting in 56,600 hepatitis E-related deaths, with the highest prevalence in East and Southern Asia (2).
Acute HEV infection is usually a self-limiting disease which usually gets resolved within 1 to 2 months even without treatment. It may cause chronic infection when there is persistence of HEV RNA for more than 3 months after exposure (3). Chronic HEV infection rapidly progress to cirrhosis and Acute-on- Chronic Liver Failure (ACLF), especially in organ transplant recipients and other immunocompromised patients. Numerous extra-hepatic manifestations have been reported in association with acute or chronic HEV infection. However, little data is available regarding HEV-related neurological symptoms and it is observed that only 5.5% HEV infected patients presents with neurological disease like GBS, bell's palsy, neuralgic amyotrophy, acute transverse myelitis and acute meningoencephalitis mainly in developed countries (4). The spectrum of neurological injury is mainly divided into two clinical presentations: dominant clinical presentation in form of GBS and neuralgic amyotrophy; and less frequent presentation in the form of meningitis, encephalitis, transverse myelitis (4-7). Early diagnosis and specific treatment of HEV infected patient with such neurological manifestations is necessary to avoid increased risk of serious long-term complications and mortality of patients. To the best of our knowledge, there have been only four reported cases of GBS as an extrahepatic symptom of HEV in India with no description of its molecular analysis (5-8).
2. Case Report
We report a case of 30-year-old male, presented with high grade intermittent fever (102°F) for 15 days. Fever was followed by jaundice, which was insidious in onset, gradually progressive, not associated with pruritus and clay coloured stools. There was no history of petechiae, ecchymosis, abdominal distention, altered sensorium, decrease in urine output and hematemesis or melena. After one week of jaundice, patient developed shortness of breath which was not associated with chest pain, orthopnoea, and paroxysmal nocturnal dyspnoea. Patient's breathlessness was also accompanied by bilateral lower limb weakness. The patient was transferred to Out-patient Department (OPD) of Institute of Liver and Biliary Sciences for further check-up. There was no history of indigenous medications or any other intoxication. There was no history of major surgeries, blood transfusions, or intravenous drug abuse prior to onset of disease, and other comorbid situations like diabetes mellitus, hypertension, coronary artery disease, tuberculosis, and thyroid disorders.
On clinical examination, patient was febrile, conscious and well oriented to time, place, person. Blood pressure was normal (125/65 mmHg), pulse rate was increased (130/minute), respiratory rate was normal (20/minute). Pallor was absent; icterus and pedal edema were present. Neurological examination revealed that there was generalized areflexia and decreased power (3/5) in bilateral lower limbs. In view of these clinical findings, a diagnosis of lower motor neuron type paraparesis was made. Laboratory investigations revealed normal blood counts and serum electrolytes levels. Liver function tests showed conjugated hyperbilirubinemia with increased serum aminotransferases (Table 1). In order to detect acute viral hepatitis infection, serological analysis was performed for all viral hepatitis markers (Hepatitis A virus (HAV) IgM antibody, Hepatitis B surface antigen (HBsAg), anti-HCV antibody (anti-HCV) and HEV IgM antibody). All serological markers were negative except HEV IgM antibody. This was suggestive of acute HEV infection. Further, HEV RNA was detected in the serum sample using in-house designed primers with Roche probe master mix (Roche Diagnostics, MA, USA) on Light Cycler 480 (LC480) instrument. HEV viral load was detected to be 3.4 × 103 IU/ml. For phylogenetic analysis, HEV ORF2 was amplified from serum sample (High pure viral RNA kit, Roche Diagnostics, MA, USA) and 10% stool sample in 0.5% NaCl solution (FastRNA Pro™ Soil-Direct Kit, MP Biomedicals, LLC, CA, USA) using ORF2 specific Polymerase Chain Reaction (PCR), generating an amplicon length of 846 bp (HEV_ILBS_GBS). HEV_ ILBS_GBS PCR product was gel purified and Sanger-sequenced followed by genotype search using NCBI genotyping tool program which showed similarity with gt1. The sequence was submitted in Genbank and an accession number was provided, viz, KY067428. Further, phylogenetic tree reconstruction was done using MEGA software v7.0 using KY067428 in conjunction with global HEV sequences using GTR + G model (9). KY067428 aligned with other HEV gt1 sequence from India, Burma, and Pakistan with high bootstrap values indicative of highly resolved tree as shown in Figure 1.
Table 1. Baseline biochemical parameters of patient at the time of admission.
| Biochemical Parameters (Normal Range) | Values |
|---|---|
| HB (13 - 17 g/dL) | 13.4 |
| PCV (36 - 48 g/dL) | 42.1 |
| TLC (4,000 - 11,000/mm3) | 15.2 × 109 |
| PLT (150 × 103 - 400 × 103)/mm3 | 177 |
| AST (5 - 40 IU/mL) | 864 |
| ALT (10 - 40 IU/mL) | 648 |
| Serum Bilirubin direct (0 - 0.2) mg/dL | 16.8 |
| Serum Indirect Bilirubin (0.2 - 0.8) mg/dL | 10.1 |
| Serum total Bilirubin (0.3 - 1.2) mg/dL | 6.7 |
HB, haemoglobin; PCV, packed cell volume; TLC, total leucocyte count; PLT, platelet; AST, aspartate serum transaminases; ALT, alanine aminotransferases.
Figure 1.
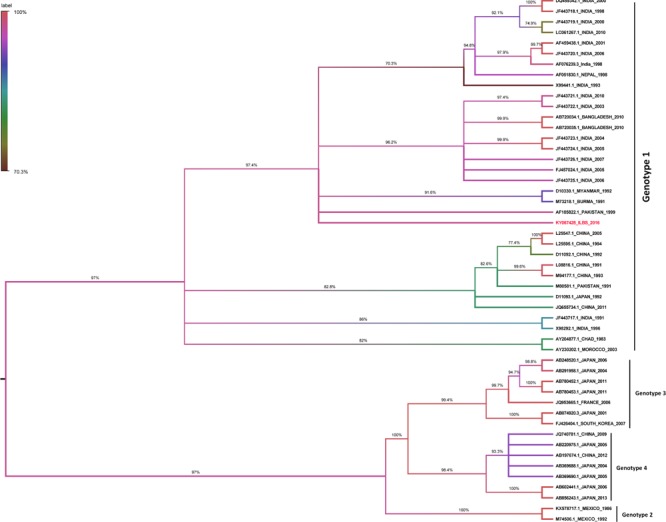
Molecular Phylogenetic analysis of HEV strains by Maximum Likelihood method. The evolutionary history was inferred by using the Maximum Likelihood method based on the General Time Reversible model. Numbers at the nodes indicates bootstrap values in percentage generated by 1,000 replicates. Only bootstrap values greater than 0.70 were considered for constructing tree. Strain sequenced in the study has been highlighted with red. Evolutionary analyses were conducted in MEGA7. The analysis involved 50 nucleotide sequences
On the basis of clinical features and laboratory investigations, diagnosis of acute viral hepatitis E with gt1 was made and patient was managed conservatively and given anti-viral medications; Sofosbuvir 400 mg orally once-a-day for one month, and Ribavirin 200 mg orally twice-a-day for one month. In view of lower limb weakness, nerve conduction studies were performed. They showed alteration in nerve conduction velocity with pure motor axonal neuropathy affecting lower limbs. Cerebrospinal fluid (CSF) analysis showed elevated proteins with normal cell count (CSF proteins, 243 mg/dL (normal range: 15-45 mg/dL); total leukocyte count, < 5 cells/mL), suggestive of albuminocytologic dissociation. Magnetic resonance imaging of brain and spinal cord were normal.
With these neurological findings, the diagnosis of GBS, as sequelae of acute HEV infection was made. Supportive measures, such as administration of intravenous fluids and nutritional therapy, were used for management of GBS. Patient recovered symptomatically after antiviral and supportive therapy. The patient was discharged after 1 week, with significant improvement in clinical symptoms (jaundice, fever) and neurological power. Follow-up of patient was done on out-patient basis. There was complete recovery of neurological power 4 weeks post-treatment. Patient's blood samples were also tested for HEV IgM antibody and HEV RNA. Both tests were found to be negative.
3. Discussion
GBS is an acute immune-mediated polyradiculoneuropathy that results in rapidly progressing symmetric motor paralysis, limb palsy, hypoflexia and areflexia. It is usually preceded by an infection, which evokes an immune response those cross-reacts with peripheral nerve components via molecular mimicry. The presentation of this disorder has several forms, including acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), acute motor-sensory axonal neuropathy (AMSAN), and Miller Fisher syndrome (MFS) (10).
A brief literature review was done using Pubmed database to identify other published cases and describe the clinical characteristics of HEV-associated GBS. With the addition of our patient, 54 cases were included, and the clinical characteristics of these cases are summarized in Table 2. Mean age of the reported patients was 51 years (20-73 years). Most of our reviewed cases were found in Western Europe and Southern and Eastern parts of Asia. These patients developed HEV-associated GBS within an acute onset and experienced hepatitis like symptoms, including nausea, malaise, vomiting and jaundice. This was followed by GBS symptoms which includes motor weakness, sensory disorder, and cranial nerve palsy. In most of the previously published reports, the association between HEV infection and GBS has been based on laboratory detection of HEV IgM antibody in serum and only few case reports have detected HEV RNA along with HEV IgM in serum for confirmation of diagnosis (6,7). Genotyping was performed in only 11 patients and revealed gt3 in ten patients while only one patient from Bangladesh revealed gt1, suggestive of higher HEV gt3 tropism for GBS (11,12). As far as treatment is concerned, treatment details for 31 cases were available, out of which 4 used plasmapheresis, 25 used Intravenous immunoglobulin, whereas 1 patient used Ribavirin. All patients had good clinical outcome with varying duration of recovery period.
Table 2. List of HEV-associated GBS cases with its clinical characteristics.
| Year | No of cases | Age /sex | HEV IgM | HEV RNA | Nerve-conduction | Treatment | Ref. |
|---|---|---|---|---|---|---|---|
| 2018 | 1 | 30Y/M | + | Serum+ | study | Supportive/ Sofosbuvir+ Ribavirin | Present case |
| 2017 | 8 | Mean: 50Y/ 6M, 2F | + | Serum+ (n = 2) Others NT | AMAN AIDP (n = 3) AMSAN (n = 1) Equivocal (n = 1) Demyelinating (n = 2) Sensory neuropathy (n = 1) | IVIG (n = 5) PP (n = 1) Supportive (n = 2) | (11,12,15) |
| 2016 | 4 | Mean: 53Y/M | + | Serum+ (n = 1) Others NT | AIDP (n = ) MSF (n = ) NM (n = 2) | IVIG | (13,14) |
| 2015 | 4 | Mean: 50Y/2M, 2F | + | Serum+ (n = 2) Others NT | AIDP (n = 3) AMSAN (n = 1) | IVIG | (8,16,17) |
| 2014 | 14 | Mean: 60Y/10M,4F | + | Serum+ (n = 3) CSF- (n = 10) | AIDP (n = 9) AMSAN (3) (Equivocal n = 2) | MV/IVIG | (18-22) |
| 2013 | 13 | Mean: 45Y/2M, 1F Others NM | + | Serum+ | AIDP (n = 2) NM | IVIG | (23-25) |
| 2012 | 3 | Mean: 60Y/1M, 2F | + | Serum+ (n = 2), 1 NT | AIDP | IVIG MV/IVIG/Ribavarin | (26-28) |
| 2011 | 2 | 66Y/M, 40Y/F | + | NT | AIDP | IVIG MV/IVIG/PP | (5,29) |
| 2009 | 1 | 60Y/M | + | NT | AIDP | IVIG | (30) |
| 2008 | 1 | 20Y/M | + | NT | AIDP + AMSAN | MV | (31) |
| 2005 | 1 | 58Y/F | + | NT | NT | IVIG/PP | (6) |
| 2002 | 1 | 35Y/M | + | NT | AIDP | MV/IVIG | (32) |
| 2000 | 1 | 50Y/M | + | NT | AIDP | Supportive | (7) |
F, female; M, male; HEV, hepatitis E virus; +, positive; −, negative; CSF, cerebrospinal fluid; AIDP, acute inflammatory demyelinating polyneuropathy; AMAN, acute motor axonal neuropathy; AMSAN, acute motor-sensory axonal neuropathy; MSF, miller fisher syndrome; NM, not mentioned; NT, not tested; MV, mechanical ventilation; IVIG, intravenous immunoglobulin; PP, plasmapheresis.
In the present case report, the patient was diagnosed with acute HEV infection which subsequently developed neurological complications in form of GBS. Detailed molecular analysis showed that the patient was infected with HEV gt1 which is quite common in developing countries including India. To the authors knowledge, this is the first case report of neurological complications (GBS) associated with acute HEV gt1 infection in an Indian patient. Among GBS-HEV cases reported so far, most of them were treated with intravenous immunoglobulin (IVIG) or ribavirin (13,14). This treatment may prolong clinical and neurological recovery in patient up to 18 months. In the present case, antiviral namely sofosbuvir and ribavirin were used in combination which improved clinical and neurological recovery of patient in one week and helped in clearance of viremia in a month's time.
Neurologic disorders as GBS are an emerging extrahepatic manifestation of HEV infection in gt1. This suggests that neurotropic variant HEV may lead to fatal clinical outcome and must be treated with specific antiviral to avoid morbidity and mortality of acute HEV infected patients. Additional case-control prospective studies should confirm this association, which would attribute GBS to HEV infection associated disease burden.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Further, authors wish to acknowledge Mr. Keshav Singh for handling and storage of patient's plasma and stool samples.
References
- 1. Mushahwar IK. Hepatitis E virus: Molecular virology, clinical features, diagnosis, transmission, epidemiology, and prevention. J Med Virol. 2008; 80:646-658. [DOI] [PubMed] [Google Scholar]
- 2. Hepatitis E fact sheet (revised August 2004). Wkly Epidemiol Rec. 2004; 79:314-316. [PubMed] [Google Scholar]
- 3. Krain LJ, Nelson KE, Labrique AB. Host immune status and response to hepatitis E virus infection. Clin Microbiol Rev. 2014; 27:139-165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bazerbachi F, Haffar S, Garg SK, Lake JR. Extra-hepatic manifestations associated with hepatitis E virus infection: A comprehensive review of the literature. Gastroenterol Rep (Oxf). 2016; 4:1-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kamar N, Bendall RP, Peron JM, Cintas P, Prudhomme L, Mansuy JM, Rostaing L, Keane F, Ijaz S, Izopet J, Dalton HR. Hepatitis E virus and neurologic disorders. Emerg Infect Dis. 2011; 17:173-179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Kamani P, Baijal R, Amarapurkar D, Gupte P, Patel N, Kumar P, Agal S. Guillain-Barre syndrome associated with acute hepatitis E. Indian J Gastroenterol. 2005; 24:216. [PubMed] [Google Scholar]
- 7. Sood A, Midha V, Sood N. Guillain-Barré syndrome with acute hepatitis E. Am J Gastroenterol. 2000; 95:3667-3668. [DOI] [PubMed] [Google Scholar]
- 8. Bandyopadhyay D, Ganesan V, Choudhury C, Kar SS, Karmakar P, Choudhary V, Banerjee P, Bhar D, Hajra A, Layek M, Mukhopadhyay S. Two uncommon causes of Guillain-Barre syndrome: Hepatitis E and Japanese encephalitis. Case Rep Neurol Med. 2015; 2015:759495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kumar S, Stecher G, Tamura K. MEGA7: Molecular evolutionary genetics analysis version 7.0 for bigger datasets. Mol Biol Evol. 2016; 33:1870-1874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Yuki N, Hartung HP. Guillain-Barre syndrome. N Engl J Med. 2012; 366:2294-2304. [DOI] [PubMed] [Google Scholar]
- 11. Zheng X, Yu L, Xu Q, Gu S, Tang L. Guillain-Barre syndrome caused by hepatitis E infection: Case report and literature review. BMC Infect Dis. 2018; 18:50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Stevens O, Claeys KG, Poesen K, Saegeman V, Van Damme P. Diagnostic challenges and clinical characteristics of hepatitis E virus-associated Guillain- Barre syndrome. JAMA neurol. 2017; 74:26-33. [DOI] [PubMed] [Google Scholar]
- 13. Ji SB, Lee SS, Jung HC, Kim HJ, Kim HJ, Kim TH, Jung WT, Lee OJ, Song DH. A Korean patient with Guillain-Barre syndrome following acute hepatitis E whose cholestasis resolved with steroid therapy. Clin Mol Hepatol. 2016; 22:396-399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Fukae J, Tsugawa J, Ouma S, Umezu T, Kusunoki S, Tsuboi Y. Guillain-Barre and Miller Fisher syndromes in patients with anti-hepatitis E virus antibody: A hospital-based survey in Japan. Neurol Sci. 2016; 37:1849-1851. [DOI] [PubMed] [Google Scholar]
- 15. Lei JH, Tian Y, Luo HY, Chen Z, Peng F. Guillain-Barre syndrome following acute co-super-infection of hepatitis E virus and cytomegalovirus in a chronic hepatitis B virus carrier. J Med Virol. 2017; 89:368-372. [DOI] [PubMed] [Google Scholar]
- 16. Higuchi MA, Fukae J, Tsugawa J, Ouma S, Takahashi K, Mishiro S, Tsuboi Y. Dysgeusia in a patient with Guillain-Barre syndrome associated with acute hepatitis E: A case report and literature review. Intern Med. 2015; 54:1543-1546. [DOI] [PubMed] [Google Scholar]
- 17. Perrin HB, Cintas P, Abravanel F, et al. Neurologic disorders i n immunocompetent patients with autochthonous Acute Hepatitis E. Emerg Infect Dis. 2015; 21:1928-1934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. van den Berg B, van der Eijk AA, Pas SD, Hunter JG, Madden RG, Tio-Gillen AP, Dalton HR, Jacobs BC. Guillain-Barre syndrome associated with preceding hepatitis E virus infection. Neurology. 2014; 82:491-497. [DOI] [PubMed] [Google Scholar]
- 19. Chen XD, Zhou YT, Zhou JJ, Wang YW, Tong DM. Guillain-Barre syndrome and encephalitis/ encephalopathy of a rare case of Northern China acute severe hepatitis E infection. Neurol Sci. 2014; 35:1461-1463. [DOI] [PubMed] [Google Scholar]
- 20. Scharn N, Ganzenmueller T, Wenzel JJ, Dengler R, Heim A, Wegner F. Guillain-Barre syndrome associated with autochthonous infection by hepatitis E virus subgenotype 3c. Infection. 2014; 42:171-173. [DOI] [PubMed] [Google Scholar]
- 21. Woolson KL, Forbes A, Vine L, et al. Extra-hepatic manifestations of autochthonous hepatitis E infection. Aliment Pharmacol Ther. 2014; 40:1282-1291. [DOI] [PubMed] [Google Scholar]
- 22. Comont T, Bonnet D, Sigur N, Gerdelat A, Legrand- Abravanel F, Kamar N, Alric L. Acute hepatitis E infection associated with Guillain-Barré syndrome in an immunocompetent patient. Rev Med Interne. 2014; 35:333-336. [DOI] [PubMed] [Google Scholar]
- 23. Santos L, Mesquita JR, Rocha Pereira N, Lima-Alves C, Serrao R, Figueiredo P, Reis J, Simoes J, Nascimento M, Sarmento A. Acute hepatitis E complicated by Guillain- Barre syndrome in Portugal, December 2012--a case report. Euro Surveill. 2013; 18. 20563. [DOI] [PubMed] [Google Scholar]
- 24. Sharma B, Nagpal K, Bakki Sannegowda R, Prakash S. Hepatitis E with Gullain-Barre syndrome: Still a rare association. J Neurovirol. 2013; 19:186-187. [DOI] [PubMed] [Google Scholar]
- 25. Geurtsvankessel CH, Islam Z, Mohammad QD, Jacobs BC, Endtz HP, Osterhaus AD. Hepatitis E and Guillain- Barre syndrome. Clin Infect Dis. 2013; 57:1369-1370. [DOI] [PubMed] [Google Scholar]
- 26. Maurissen I, Jeurissen A, Strauven T, Sprengers D, De Schepper B. First case of anti-ganglioside GM1- positive Guillain-Barré syndrome due to hepatitis E virus infection. Infection. 2012; 40:323-326. [DOI] [PubMed] [Google Scholar]
- 27. Del Bello A, Arne-Bes MC, Lavayssiere L, Kamar N. Hepatitis E virus-induced severe myositis. J Hepatol. 2012; 57:1152-1153. [DOI] [PubMed] [Google Scholar]
- 28. Tse AC, Cheung RT, Ho SL, Chan KH. Guillain-Barre syndrome associated with acute hepatitis E infection. J Clin Neurosci. 2012; 19:607-608. [DOI] [PubMed] [Google Scholar]
- 29. Cronin S, McNicholas R, Kavanagh E, Reid V, O'Rourke K. Anti-glycolipid GM2-positive Guillain-Barre syndrome due to hepatitis E infection. Ir J Med Sci. 2011; 180:255-257. [DOI] [PubMed] [Google Scholar]
- 30. Loly JP, Rikir E, Seivert M, Legros E, Defrance P, Belaiche J, Moonen G, Delwaide J. Guillain-Barre syndrome following hepatitis E. World J Gastroenterol. 2009; 15:1645-1647. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Khanam RA FM, Basunia RA, Ahsan AA. Guillain-Barré syndrome associated with acute HEV hepatitis. Med Coll J. 2008; 1:32-34. [Google Scholar]
- 32. Kumar R, Bhoi S, Kumar M, Sharma B, Singh BM, Gupta BB. Guillain-Barré syndrome and acute hepatitis E: A rare association. JIACM. 2002; 4:389-391. [Google Scholar]