

Abstract
Background
A re-emergent tremor is suggested to be specific to Parkinson’s disease and although a tongue tremor has been reported in levosulpiride-induced parkinsonism (LIP), re-emergence has never been reported.
Case Report
A 59-year-old female presented with a 3-month history of bradykinesia, 2-week history of right-leg tremor, and 10-day history of lip and tongue tremor. A review of the medication revealed a 15-month history of levosulpiride consumption. On examination, asymmetric bradykinesia, rigidity, rest tremor of the right leg, and re-emergent tongue tremor were observed. The parkinsonism subsided after levosulpiride was stopped.
Discussion
This is the first report of re-emergent tongue tremor in LIP.
Keywords: Re-emergent tremor, tongue tremor, levosulpiride, drug-induced parkinsonism
Introduction
Levosulpiride is a benzamide derivative that blocks both central and enteric D2 receptors; therefore, it is frequently used for treatment of dyspepsia and as a prokinetic.1 However, levosulpiride may produce a variety of extrapyramidal symptoms ranging from dystonia to parkinsonism.2 Tremor in levosulpiride-induced parkinsonism (LIP) has been frequently reported and is similar to a classic parkinsonian tremor in distribution, type, and frequency.1–3 This report describes the presence of a re-emergent tongue tremor in a case of LIP. Re-emergent tongue tremors have been reported in association with Parkinson’s disease (PD),4,5 and although tongue tremor has been previously reported in LIP there are no reports of re-emergence.
Case report
A 59-year-old female presented at our movement disorders clinic with a 3-month history of generalized slowness of activities, 2-month history of a right-leg tremor, and a 10-day history of tongue and lip tremors. The right-leg tremor was predominantly observed at rest, i.e. when the patient was sitting with her foot on the floor or when lying in bed, and absent while standing or walking. The tongue and lip tremors were continuously present when the patient’s mouth was closed and were reduced when the patient was eating or talking. Tremors were absent during sleep, and there was no history of tremors in other parts of the body. There were no other significant complaints. The patient was known to have diabetes mellitus, hypothyroidism, and paroxysmal supraventricular tachycardia and had a history of recurrent episodes of gastritis. A review of medications revealed a 15-month history of daily consumption of a combination of levosulpiride (75 mg) and pantoprazole (40 mg).
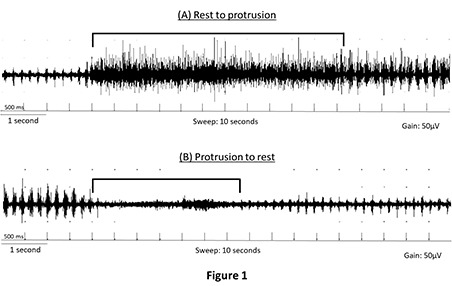
On examination (Video 1, Segment 1), the patient had reduced facial expression and blink rate, and her speech was hypophonic and monotonous. A continuous tremor of the tongue and lips was observed. The tongue tremor transiently subsided when protruded, following which it recurred. A similar re-emergence was observed when the tongue was retracted and placed at rest. There was no rest tremor or postural tremor of either of the upper limbs. A continuous distal rest tremor was observed in the right leg. The patient had asymmetrical rigidity and bradykinesia. Her gait was slow with reduced bilateral arm swing. Her Unified Parkinson’s Disease Rating Scale Part III, OFF state score was 36. The rest of her neurological examination was normal. Routine blood investigations were normal and magnetic resonance imaging (MRI) of the brain revealed diffuse cerebral atrophy and periventricular white matter changes. Surface electromyography of the genioglossus (Figure 1) revealed a 5 Hz re-emergent tremor of the tongue. A latency of 5.5 seconds was observed between the rest tremor and re-emergence when the tongue was protruded (Figure 1A), and a latency of around 3.5 seconds was observed prior to re-emergence when the tongue was at rest. The video of the patient was taken after informed written consent was provided.
Figure 1. Surface Electromyography Recording of the Genioglossus Revealing a Re-emergent Tremor. Horizontal square brackets indicate latent period. (A) Tongue initially at rest, followed by protrusion. A 5 Hz re-emergent tremor is observed with a 5.5 second latency between the rest tremor and re-emergence of tremor after protrusion. (B) Tongue initially protruded, followed by a return to rest. A 5 Hz re-emergent tremor is observed with a 3.5 second latency between the tremor while the tongue was protruded and re-emergence of tremor after return to rest.
Video 1. Video Demonstrating Key Clinical Features. Segment 1. The patient had reduced facial expression and blink rate, and speech was hypophonic and monotonous. A continuous tremor of the tongue and lips was observed. The tongue tremor transiently subsided when protruded, following which it recurred. A similar re-emergence was observed when the tongue was retracted and placed at rest. There was no rest tremor or postural tremor of either of the upper limbs. A continuous distal rest tremor was observed in the right leg. The patient had asymmetrical bradykinesia. Gait was slow with a reduction in bilateral arm swing. Segment 2. Evaluation in the 48 hours OFF state 8 months after stopping levosulpiride. The patient had very minimal hypomimia, and speech was normal. There was no tongue, lip, or lower limb tremor. Bradykinesia was negligible and gait was relatively normal.
Based on the history, clinical findings, investigations, and the background of levosulpiride consumption, a diagnosis of drug-induced parkinsonism was made. Levosulpiride was stopped and the patient was discharged on a combination of levodopa and carbidopa (100 mg and 25 mg respectively) at a total levodopa equivalent dose (TLED) of 400 mg. The patient reported for follow-up 8 months after discharge, at which point she was consuming a TLED of 200 mg. Medication was withheld and was evaluated 48 hours after the last dose of dopaminergic medication. The patient was examined (Video 1, Segment 2); she had very minimal hypomimia, and her speech was normal. There was no tongue, lip, or lower-limb tremor, and no rigidity. Bradykinesia was negligible and gait was relatively normal.
Discussion
Although we did not perform functional imaging to confirm drug-induced parkinsonism, the complete and persistent resolution of tremor and parkinsonism in the OFF state causally implicates levosulpiride in this case. A re-emergent tremor involving the limbs or the tongue has been frequently described in patients with PD.4,5 There is also one report of re-emergent tremor in scans without evidence of dopaminergic deficit, suggesting that this type of tremor is not limited to PD.6 An orolingual tremor has been previously described in LIP; however, the current case is the first report of a re-emergent tongue tremor in this context. Both the frequency and the latency of the observed re-emergent tremor are similar to the characteristics of a PD re-emergent limb tremor that has a reported frequency of 4–10 Hz and latency of 9.20±6.8 seconds.5
In conclusion, a re-emergent tremor is not limited to PD and may be present in LIP. Patients with subacute onset of parkinsonism and a re-emergent tremor should be thoroughly evaluated to rule out the possibility of drug-induced parkinsonism.
Footnotes
Funding: None.
Financial Disclosures: None.
Conflicts of Interest: The authors report no conflict of interest.
Ethics Statement: All patients that appear on video have provided written informed consent; authorization for the videotaping and for publication of the videotape was provided.
References
- 1.Shin HW, Kim MJ, Kim JS, Lee MC, Chung SJ. Levosulpiride-induced movement disorders. Mov Disord. 2009;24:2249–2253. doi: 10.1002/mds.22805. [DOI] [PubMed] [Google Scholar]
- 2.Choudhury S, Chatterjee K, Singh R, Shubham S, Trivedi S, Chatterjee S, Kumar H. Levosulpiride-induced movement disorders. J Pharmacol Pharmacother. 2017;8:177–181. doi: 10.4103/jpp.JPP_32_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kim HJ, Cho JY, Cho YJ, Hong KS. Levosulpiride-induced resting orolingual tremor. Mov Disord. 2009;24:1700–1701. doi: 10.1002/mds.22578. [DOI] [PubMed] [Google Scholar]
- 4.Numao A, Suzuki K, Fujita H, Hirata K. Resting and re-emergent tongue tremor in Parkinson’s disease. BMJ Case Rep. 2017;2017 doi: 10.1136/bcr-2017-221808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fabbri M, Abreu L, Santos T, Ferreira JJ. Resting and reemergent tongue tremor as presenting symptoms of Parkinson’s disease. Movement Disorders Clinical Practice. 2017;4:273–274. doi: 10.1002/mdc3.12408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.de Laat KF, van de Warrenburg BP. Re-emergent tremor in a dystonic SWEDD case. Mov Disord. 2012;27:462–463. doi: 10.1002/mds.24040. [DOI] [PubMed] [Google Scholar]