

Abstract
Joint attention (JA) and peer interactions are significantly impaired in children with autism spectrum disorder (ASD). Empirically demonstrated interventions exist to address JA with adults, but few with peers. Training peers through instructions, modeling (both live and video models), role play, and feedback may help facilitate JA in children with ASD. We examined the effects of peer training with live and video models on typically developing (TD) peer strategies to facilitate JA and JA behavior in children with ASD. TD peers showed some improvement in prompting and reinforcing JA. Children with ASD showed overall increases in JA with trained and novel peers that were also observed by parents, professionals, and peers. Findings are discussed with respect to variables to consider when teaching JA to children with ASD and their peers as well as the need to further examine the relationship between peer training and JA in children with autism.
Keywords: Autism, Joint attention, Social skills, Peer-video modeling
Joint attention (JA) is a pivotal skill that emerges during early development and provides a critical foundation for the acquisition of language and engagement in social-communicative interactions (Bakeman & Adamson, 1984; Bates, 1979; Ninio & Bruner, 1978; Tomasello & Ferrar, 1986). JA refers to sharing an experience or object with another person through gestures (e.g., pointing), shifting gaze, and vocalizing (Mundy, Sigman, & Kasari, 1994). In typical development, JA is first seen with parents around 9 months of age and then later with peers (Bakeman & Adamson, 1984; Bates, 1979; Ninio & Bruner, 1978). In children with autism spectrum disorder (ASD), impairments in JA are apparent from a very young age (Adamson, Bakeman, Deckner, & Romski, 2009; Barbaro & Dissanayake, 2012; Mundy & Crowson, 1997; Mundy et al., 1994).
As a result of the identification of impairments in JA in children with ASD, there are a number of demonstrations of intervention procedures to teach JA to children with ASD (e.g., Jones, Carr, & Feeley, 2006; Kasari, Freeman, & Paparella, 2006; Whalen & Schreibman, 2003; for reviews, see Meindl & Cannella-Malone, 2011; Murza, Schwartz, Hahs-Vaughn, & Nye, 2016; White, O’Reilly, Streusand, Levine, Sigafoos, Lancioni, Fragale, Pierce, & Aguilar, 2011). In this growing literature, procedures often include breaking down JA into smaller components, modeling, prompting, and positive reinforcement (Meindl & Cannella-Malone, 2011). The partners for JA interactions are largely adult caregivers such as teachers (e.g., Jones et al., 2006; Lawton & Kasari, 2012) or parents (e.g., Jones & Feeley, 2007; Kasari, Gulsrud, Wong, Kwon, & Locke, 2010). But, for children with ASD, social interactions are impaired with both adults and other children. Lack of interest in engaging with peers and difficulty sharing are part of the diagnostic criteria (American Psychiatric Association, 2013). Limited peer interactions mean children with ASD miss many learning opportunities.
In one of the only peer-mediated interventions to address JA in children with ASD, Ferraioli and Harris (2011) taught typically developing (TD) siblings of children with ASD specific strategies to support JA in their siblings with ASD. During training sessions with the TD sibling, the interventionist described and modeled what the TD sibling should do to support JA. Then, the TD sibling role-played with the experimenter and the interventionist provided feedback. After training, the TD sibling participated in teaching sessions with his/her sibling with ASD with the interventionist prompting the TD siblings as needed. TD siblings learned to present JA opportunities, for example, by tapping or showing their sibling with ASD a toy. TD siblings learned skills such as prompting eye contact by touching the chin of his/her sibling with ASD and providing reinforcement by commenting on the objects of JA. All children with ASD demonstrated an increase in responding to JA (RJA), but only one child showed an increase in initiating JA (IJA).
As in Ferraioli and Harris (2011), peer-mediated intervention often involves teaching peers through modeling, role play, and feedback (Chan, Lang, Rispoli, O’Reilly, Sigafoos, & Cole, 2009). Modeling can be live as in Ferraioli and Harris or by video. When models are live, the interventionist shows the TD peer what to do, while the TD peer watches, and then the TD peer has the opportunity to practice that behavior in role play. In video modeling, the child watches a video of a target behavior prior to having an opportunity to engage in that behavior. Growing literature supports the use of video modeling across populations, skills, and settings (e.g., Benzies, Magill-Evans, Kurilova, Nettel-Aguirre, Blahitka, & Lacaze-Masmonteil, 2013; Buggey & Ogle, 2012; Catania, Almeida, Liu-Constant, & Digennaro Reed, 2009; Mason, Davis, Boles, & Goodwyn, 2013; Mason, Ganz, Parker, Burke, & Camargo, 2012). When teaching TD peers, video models can be used in the same way they are used in parent and staff training; the interventionist shows the video models either along with live modeling or in place of, prior to role play and feedback. Combining both live and video models as part of a training package could help to maintain the interest of peers and perhaps help to highlight behaviors observed during training. Showing the video model right before a session with the child with ASD could help prepare the peer for the upcoming social interaction with the child with ASD. The addition of a video model in peer training may also decrease the need for adult mediation during peer interactions with the child with ASD, something that may limit children’s natural interactions.
In the present study, we examined the effects of peer training consisting of verbal instructions, live modeling paired with video modeling, role play, and feedback to teach TD peers to support JA interactions with children with ASD. Peer engagement in strategies to facilitate JA in children with ASD and JA behaviors in children with ASD without adult mediation were examined.
Method
Participants
Children with ASD
Three children with ASD participated. To be included in this study, parents had to provide informed consent and the child had to (a) be between the ages of 6 and 10 years; (b) have a diagnosis of ASD from a physician not associated with this research (given the ages of the children, diagnoses had been made based upon the criteria in the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2000)); (c) demonstrate JA with adults, but not peers; (d) score a minimum rating of 3 for each criterion on a parent-completed questionnaire about prerequisite skills (described shortly); and (e) score a total of 80% correct on the interventionist’s assessment of prerequisite skills (described shortly).
Each parent rated (from 1 [strongly disagree] to 5 [strongly agree]) his/her child’s current imitative and game play repertoire (e.g., “Can imitate modeled gross motor behavior,” “Stays engaged in an activity for at least 5 minutes.”) on a prerequisite skill questionnaire. During the interventionist’s assessment of prerequisite skills, the interventionist played several games with the child with ASD for 5 min, presenting 10 opportunities to examine attending to the game, JA with adults, game play, and imitation. An opportunity for RJA and IJA occurred with each player’s turn during the game. Opportunities to engage in imitative behaviors and follow directions were presented prior to, during, and at the conclusion of game play. The interventionist provided verbal praise and high fives for correct responses.
A 9-year-old boy (Alex), a 10-year-old boy (Thomas), and a 7-year-old girl (Amelia) participated. Amelia was Alex’s sister. All were diagnosed with pervasive developmental disorder not otherwise specified (PDD-NOS) (American Psychiatric Association, 2000). Each demonstrated expressive and receptive language at his/her age level and showed good social interactions with adults, but difficulty with peers. Based on parent report, Alex’s schooling consisted of private 1:1 instruction at an Applied Behavior Analysis (ABA) center during the day and 5 h of in-home ABA services weekly. Thomas attended an inclusion class in a public school setting, where he also received group speech and occupational therapy twice per week for a half hour each and group reading three times per week for 1 h. Amelia attended a collaborative class in a public school and received 4 h of in-home ABA services weekly.
Typically Developing Peers
TD children were recruited as peer partners. One TD peer was paired with each child with ASD to receive peer training, and two additional TD peers participated in interactions with the children with ASD to examine generalization. TD peers had to be at least 6 years of age and within 2 years of age of the child with ASD with whom they were paired. Inclusion criteria were parent report of typical development, general education classroom placement, and parent informed consent. All peers demonstrated language and communication skills at age level.
The three TD peers who received training were Ollie (a 10-year-old girl paired with Alex), Kendra (an 8-year-old girl and Thomas’ sister), and Amanda (a 7-year-old girl paired with Amelia). The two TD peers who helped conduct generalization probes were Jules and Sarah who were 7- and 9-year-old girls, respectively. They were recruited from an ABA center (where some sessions occurred) where they had been peer models for several years. As peer models, they participated in similar activities as during JA sessions during weekly social skills groups with children with ASD.
Setting and Interventionists
Intervention was conducted in both the homes of the children with ASD and in a therapy room (approximately 28 m2) at a center that provides 1:1 ABA intervention, social skills intervention, and parent training. Play areas contained materials that were used for each session with all other potentially distracting stimuli removed. Multiple interventionists implemented intervention with each child. Interventionists included the first author and other therapists at the center who were all graduate students at the Queens College. The therapists all had training in applied behavior analysis and experience facilitating social skills groups at the center and providing in-home ABA services. The first author held a master’s degree in Applied Behavior Analysis and was a Board Certified Behavior Analyst. She was enrolled in a PhD program in psychology with an emphasis in behavior analysis. The first author trained the other interventionists prior to implementation of their first session. Training consisted of review of the intervention procedures, modeling, role play, and feedback.
Materials
Several preferred turn-taking games including board games (e.g., Monopoly Jr©, Candyland™, Sorry!®, Connect4™, Headbandz™, Guess Who®, Zingo®, Pop the Pig®, Smarter than a 5th Grader™, Chutes and Ladders®, Silly Faces™, Pengaloo™), card games (e.g., Uno®, Spot it™), and Wii™ games (e.g., Bowling™, Mario Kart™) were used as materials for peer training and JA interactions. Interventionists used an iPad® with a token economy application to track participants’ tokens (Class Dojo, © 2011–2013 ClassTwist, Inc.) and play the peer videos. A prize box contained stickers, costume jewelry, erasers, mini plastic figurines, rubber balls, whistles, and spinning tops.
A video camera was used to record sessions. Video models were also recorded on the video camera and edited using Apple’s iMovie program©. Six video segments were created for video models, one per training topic. Video segments are described in Table 1. The first five videos highlighted one target behavior. These were shown as each behavior was introduced during training. The sixth and final segment was a longer video with two children demonstrating all the individual skills in the previous video segments while playing a game for 5 min. The sixth video was used in the final training sessions and prior to JA post-training sessions. Each video segment showed two TD children recruited from an existing social group at the same center at which some sessions took place. TD children in the videos were of the same approximate ages as the TD peers and children with ASD. In the video, one child played the role of the TD peer and the other child played the role of the child with ASD, each following a script. Multiple exemplars of games were sampled across videos.
Table 1.
Video model descriptions for each peer behavior
| Topic | Description |
|---|---|
|
Stay in proximity Gain attention |
The video was approximately 30 s consisting of peers playing Wii™ “Just Dance” while demonstrating staying in close proximity to each other and how to gain the other peer’s attention when he/she is not attending to the peer/game. TD Peer: Ask peer acting as child with ASD which game he/she wants to play. Child with ASD: Select a game and join the TD peer independently. TD Peer: Remain within 2 arms lengths of the child with ASD during game play. Take turn and then say, “It’s your turn.” Child with ASD: Stop attending and instead look out the window when it is her turn to play. TD Peer: Tap the child with ASD on the shoulder, gesture to the game piece, and repeat, “Look! It’s your turn!” |
| Initiate sharing |
The video was approximately 1 min. The peers played Uno® for four turns demonstrating several opportunities of turn-taking. The TD peer shared an event about the game on her turn (i.e., “I rolled a six!”). The peer acting as the child with ASD emitted 2 correct RJA responses. TD Peer: Ask peer acting as child with ASD which game he/she wants to play. Child with ASD: Select a game and join the TD peer independently. TD peer takes her turn. TD Peer: Say, “I love playing Uno!” and take turn. Child with ASD: Look at peer, say, “This is my favorite game too!” and take turn. TD Peer: Take turn and say, “I don’t have that color.” Child with ASD: Look at peer and say, “Pick another card.” |
| Respond to sharing |
The video was approximately 1 min. The peers played Sorry!® demonstrating four opportunities of turn-taking. The peer acting as the participant with ASD initiated sharing correctly on her turn and the typical peer responded. TD Peer: Ask peer acting as child with ASD which game she wants to play. Child with ASD: Select a game and join TD peer independently. TD Peer: Allow the child with ASD to go first. Child with ASD: Take turn. Then look at peer and say, “I rolled a six!” TD Peer: Look at child with ASD, say, “Wow! That’s a big move!” and then take turn. Child with ASD: Take turn, look at peer, and say, “I’m going to move this piece this time.” TD Peer: Look at child with ASD, say, “That was a great move,” and then take turn. |
| Reinforce correct response |
The video content was similar to the sharing videos; however, the children played Wii™ “bowling” and reinforcement was delivered upon correct responding of the peer acting as the child with ASD (e.g., peer said, “That’s great looking.”). TD Peer: Ask peer acting as the child with ASD which game she wants to play. Child with ASD: Select a game and join TD peer independently. TD Peer: Say, “Nice joining me.” Child with ASD: Take turn, look at peer and then say, “I knocked down 5 pins!” TD Peer: Say, “Great sharing with me! Wow! Great shot!” and then take turn. Child with ASD: Look at TD peer and point to pins, then look back to TD peer and say, “I hope I throw a strike!” TD Peer: Look at where child with ASD’s pointing and then look at child with ASD and say, “(insert name), Great looking at me! Then point to the pins and say, “I think you can knock down all those pins.” Child with ASD: Follow the peer’s point to the pins and take turn. Game ends TD Peer: Say, “Great playing!” then smile, and give a high five. |
| Allow 5 s to respond | To demonstrate appropriate wait time for responding, peers watched a 30-s segment of the sharing videos with a timer to time waiting for responses. |
| Redirect and prompt |
The video content was similar to sharing videos; however, the children played Go Fish and the peer acting as the child with ASD made incorrect responses to which the TD peer demonstrated gestural, physical, and verbal prompts. The peer acting as the child with ASD turned away from the TD peer or walked away from the activity on two of the four turns and made two incorrect IJA and two incorrect RJA responses. The TD peer demonstrated gestural, physical, and verbal prompts to redirect the peer acting as the child with ASD back to the activity and prompt JA responses. TD Peer: Ask the peer acting as child with ASD which game she wants to play. Child with ASD: Select a game and join the TD peer independently. TD Peer: Say, “Great job joining me.” Then take turn first. Look at child with ASD and say, “Hmmmm, I don’t know what I should do. Child with ASD: Do not respond to peer. TD Peer:, “(insert name), look at me” Child with ASD: Look at TD peer. TD Peer: Say, “That’s better looking at me. I don’t know what card to ask for first.” Child with ASD: Looks at TD peer and say, “What card do you need?” TD Peer: Look at child with ASD and say, “I need a four.” Child with ASD: Do not respond. TD Peer: Point to cards and say again, “I need a four.” Child with ASD: Looks towards the TD peer’s point to the cards and say, “I don’t have a four. Go fish.” TD Peer: Say, “That’s better paying attention to me. Aw, I don’t have a match.” Picks up additional card. Child with ASD: Do not respond. TD Peer: Say, “(insert name), look at me and say better luck next time.” Child with ASD: Look at TD peer and say, “Better luck next time.” TD Peer: Say, “Thanks buddy!” Child with ASD: Take turn, look at peer, and say, “I only have two cards left!” TD Peer: Look at child with ASD and say, “Lucky! I have four cards left. Oh, I have a match!” Child with ASD: Do not respond to TD peer. TD Peer: Say, “(insert name), look at me” and then repeat, “I have a match!” Child with ASD: Look at TD peer and say, “Cool!” TD Peer: Say, “That’s better paying attention to me. I only have three cards left now.” Child with ASD: Do not attend to the game and instead look out window. TD Peer: Tap child with ASD on the shoulder and gesture to her cards, then repeat, “I only have three cards left now.” Child with ASD: Look at peer and say, “Nice! We are almost tied!” TD Peer: Look at child with ASD and say, “Great! That’s better answering me.” |
| Final video of all target behaviors | The final 7-min video included all the previous segments for each target streamed together into one fluid video. |
Response Definition and Data Collection
Sessions were video recorded for later coding of behaviors for each child. The first 5 min or 11 opportunities of each JA session were coded, whichever occurred first. Table 2 provides detailed definitions of behaviors examined for children with ASD and TD peers.
Table 2.
Response definitions
| Response | Definition |
|---|---|
| Children with ASD responses | |
| RJA | Gaze shift (GS) and vocalization to peer within 5 s of peer initiating sharing |
| IJA | Initiation of GS and vocalization towards peer without peer initiation in preceding 5 s |
| Gaze shift | Child looks at materials and then at the eyes of peer (looking at partner’s eyes for at least 1 s) |
| Vocalization | Commenting about the activity/object of joint attention (e.g., “Wow!” “I got a green square” “Oh man! I have to go back 2 spaces.”) |
| Typical peer-training targets | |
| Initiate JA bid | TD peer shares an event during activity (making comments such as, “Oh, I rolled a six!”) on peer’s turn |
| Respond to IJA from child with ASD | TD peer makes comments in response to initiation from child with ASD (e.g., child with ASD says he/she lost to which TD peer responds, “It’s okay. You played a great game”) |
| Reinforce appropriate response | TD peer provides praise when child with ASD engages in target behaviors (e.g., high fives or saying “Great job looking at me”) |
| Allow 5 s for participant to respond | TD peer allows child with ASD 5 s to respond to a request, comment, or question and to initiate sharing |
| Redirect participant | TD peer provides a gestural, physical, or verbal prompt if child with ASD does not take his/her turn within 5 s (e.g., pointing to an object or saying the name of the child with ASD) |
| Prompt participant | TD peer provides a gestural, physical, or verbal prompt if child with ASD does not orient towards activity or peer or does not emit correct IJA or RJA response within 5 s |
Children with ASD
Both responding to TD peer’s joint attention bids (RJA) and initiating joint attention (IJA) were examined with both responses consisting of gaze shift paired with a vocalization. Opportunities for JA occurred within the turn-taking structure of a game. On the TD peer’s turn, the TD peer made a JA bid (e.g., on the peer’s turn, he/she said, “Look, I rolled a six!”) and the child with ASD had an opportunity to engage in RJA by shifting gaze from the game materials to the TD peer’s eyes while vocalizing (e.g., “Wow! That’s awesome!”) within 5 s of the TD peer’s JA bid. When the child with ASD took his/her turn, he/she had an opportunity to IJA by shifting his/her gaze from the game materials to the TD peer’s eyes while also vocalizing after beginning to take his/her turn and within 5 s of completing his/her turn (e.g., after placing his game piece on the party box in Monopoly Jr©, the child shifted gaze from the game board to the TD peer and said, “I got the party box!”), and before the TD peer said anything to the child with ASD. Percentage of correct independent responses out of the total number of opportunities is reported for RJA and IJA.
TD Peers
A number of behaviors we identified as important for TD peers to demonstrate to facilitate JA are described in Table 2. TD peers needed to be in close proximity to the child with ASD to allow for JA opportunities to occur. Target behaviors for each peer were individualized depending on baseline performance. For all three TD peers, initiating sharing (JA), reinforcing appropriate responses, and prompting responses were targeted during intervention. These behaviors were chosen based on the common components used across adult-mediated JA interventions. For Ollie, responding to sharing was also targeted during intervention because baseline performance for this behavior was low. Percentage of correct responses out of the total number of opportunities across all peer behaviors is reported.
Experimental Design
A multiple baseline probe design across three child with ASD-TD peer dyads was used to examine the effects of TD peer training on TD peer behaviors and JA behaviors in the children with ASD.
Procedure
The interventionist identified preferred games prior to baseline sessions. Once games were identified, baseline JA sessions for TD peers and children with ASD began. Following baseline, TD peers participated in peer training and then JA post-training sessions with the child with ASD similar to baseline. All sessions occurred one time a week with three sessions per day.
Game Identification
Prior to baseline, the interventionist selected games from three categories (five board games, five video games, and five card games) based on age and current popularity. Games were chosen that involved a turn-taking sequence. The interventionist conducted separate multiple-stimulus-without-replacement (MSWO) preference assessments for each category of games to identify games each child with ASD preferred. For example, the five board games were presented to the child with ASD and he/she was asked to, “Pick one.” Once the child with ASD selected a game, the interventionist removed the remaining four games from the table and allowed the child to play the game for 2 min after completing game setup. After 2 min, the interventionist removed the selected game and presented the remaining four games, rotating each game one position to the right from the previous presentation. This procedure was repeated until only one game remained or the child with ASD did not choose a game within 30 s. Each category of games was assessed two times on two separate days. The top three preferred games from each category (for a total of 9 games) were used during JA baseline and JA post-training sessions.
To ensure the peer also preferred the games, the peer chose three of the preferred games as options for play during JA sessions. The peer offered the three games for the child with ASD to choose one to play that session.
JA Baseline Sessions
JA sessions involved the child with ASD and TD peer playing one of the preferred games for 5 min. JA sessions began when the interventionist instructed the TD peer to select three games from the preferred list and present them to the child with ASD as might naturally occur during peer play. To help the TD peers do this, the interventionist modeled game presentation for TD peers prior to JA baseline sessions. The TD peer selected three games of his/her choice from a list of the games identified as preferred by the child with ASD and presented the actual games to the child with ASD at the beginning of each JA session and asked which game he/she would like to play. Once the child with ASD chose a game, he/she participated in a JA session with the peer. Selected games were only played for one of the three sessions conducted in the same day. The played games could be selected again in the following week’s sessions. If children were happily playing at the end of 5 min, interventionists gave them an additional 5 min (only the first 5 min were coded). The interventionist provided a warning (e.g., she said, “Almost time to clean up”) after 3 min.
During JA baseline sessions, the interventionist did not provide prompting or reinforcement. Following the conclusion of all JA baseline sessions for the day, the children engaged in a preferred activity for 5 min or selected a prize from the prize box for their participation. A minimum of five initial JA baseline sessions were conducted prior to implementation of intervention with the first TD peer. One JA baseline probe session was conducted weekly for the TD peer-child with ASD dyads for whom intervention had not yet been introduced. Intervention was introduced for the successive TD peer once the child with ASD in the preceding dyad demonstrated an increase in either IJA or RJA at or greater than 20% above his/her baseline performance during intervention.
TD Peer Training
Following JA baseline sessions, the TD peer participated in a series of 20 min peer-training sessions with the interventionist. During each session, the interventionist introduced one new target peer behavior. Table 3 describes the sequence of instructions, modeling, role play, and feedback during training. At the beginning of each training session, the interventionist stated the definition of the target behavior for the session as in Table 2. After defining the target behavior, the interventionist, acting as the TD peer, modeled the appropriate behavior. Then, the TD peer viewed a video model of the target behavior immediately before practicing the target behavior while playing with the same games as they played during JA sessions and with the interventionist now acting as the child with ASD. Role play lasted approximately 5 min. Immediately after the 5 min of role play, the interventionist provided verbal feedback about what the TD peer did well and what needed improvement (e.g., the interventionist said, “I liked how you stayed close to me and gained my attention. When you see me looking at you, tell me, ‘Great job looking.’”). The sequence of viewing the video model, practicing, and receiving feedback continued until peers met mastery criterion (80% correct responding during role play with the interventionist). A new topic was introduced in the same day when time allowed or on a subsequent day. Since we viewed each target behavior as a prerequisite skill for the next target behavior, each training session involved practice of and feedback about targets already mastered. TD peers mastered training when all target behaviors were performed independently at 80% or greater during role play with the interventionist after viewing the final 7-min video segment.
Table 3.
Peer training protocol
| Protocol | Description |
|---|---|
| Introduce topic | The interventionist defined the target behavior and provided a verbal example using Table 2 as a guide. |
| Live model | The interventionist engaged in the target behavior/s (e.g., while playing Monopoly, the interventionist initiated sharing by moving a game piece on the board and then saying something like, “Yay! I landed on Go and can collect $200!”). |
| Video model | Interventionist played the video model of the target behavior. |
| Role play | The interventionist and TD peer played a game for 5 min. The interventionist instructed the peer to demonstrate the target behaviors with the interventionist playing the role of the child with ASD (e.g., for prompting, the interventionist did not attend and looked away so the peer could practice tapping the interventionist acting as the child with ASD on the shoulder and reminding him/her it was his/her turn). For each turn, the interventionist provided an opportunity for the peer to engage in the target behavior(s). If the peer did not engage in the target behavior, the interventionist quickly modeled the appropriate behavior and provided another opportunity for the peer to practice the appropriate target behavior. |
| Feedback | The interventionist provided behavior-specific praise for target behaviors the peer demonstrated well and provided corrective feedback for any missed opportunities to engage in the target behavior/s or other ways to improve the target behavior/s. |
Similar to JA baseline sessions, the peers received a preferred activity or choice from the prize box at the conclusion of each session. However, now it was contingent on performance rather than just participation. During peer-training role play (and also JA post-training sessions with the child with ASD), the interventionist introduced a token system for the TD peers. Tokens were recorded and displayed using Class Dojo (© 2011–2013 ClassTwist, Inc.) on an iPad®. Class Dojo© is a reward charting application in which each child is represented by an avatar character. When the TD peer engaged in any of the correct target behaviors, the interventionist selected the target behavior icon to indicate that the peer engaged in that behavior. The application kept a tally of each point accumulated for each target response. TD peers received 1 point each time they appropriately engaged in a target behavior and for each occurrence of RJA or IJA by the child with ASD during JA post-training sessions. The peer had to remain within arm’s length of the child with ASD and take turns during game play for the entire session as well as earn a minimum number of points across the three sessions each day to exchange for access to a preferred activity for 5 min or select a prize from the prize box. The number of points the TD peer needed to earn was determined by her performance at baseline. For example, Ollie’s baseline performance yielded an average of 7 points across the baseline sessions because she engaged in IJA and RJA for a combined average of 7 times. For the first day, Ollie needed to earn 8 points across the three sessions for that day. If Ollie exceeded the minimum number across those three sessions, then 1 point was added to the minimum criterion for the following day. TD peers always met their session point goal and received access to a preferred activity or choice from the prize box.
JA Post-Training Sessions
Upon completion of each peer-training session, the TD peer and child with ASD participated in JA post-training sessions similar to JA baseline sessions, but with several differences. First, just prior to the session, the interventionist presented the final video segment showing all the target behaviors to the TD peer.
Second, a reward system was also in place for the child with ASD. Prior to each session, the interventionist provided several choices of age-appropriate and popular items/activities to the child with ASD. The child with ASD selected the item/activity he/she would like to earn for playing with his/her peer. The child with ASD also used Class Dojo© and received 1 point for each correct independent RJA or IJA response, but no verbal feedback from the interventionist. A pre-determined number of points to be earned was set for each session based on JA baseline session performance in the same way it was for the TD peer. For example, if baseline performance was one RJA response, criterion began at two independent RJA responses. The same determination was made with IJA. If the child with ASD met or exceeded the number of points he/she had to earn, he/she received the pre-selected item/activity at the termination of the session. Criterion was systematically increased based on the average performance the child with ASD demonstrated for two consecutive sessions across 2 days. The new criterion was determined by the average increase observed across a day’s session. For example, if Alex had a minimum criterion of 7 points, but was consistently earning an average of 9 points for two consecutive sessions across 2 days, then the following day’s session would begin at a minimum of 9 points. If the child with ASD did not demonstrate an increase for two consecutive sessions, then criterion was not adjusted. The maximum number of points for a given game was determined based on the total number of turns (opportunities per game) observed during JA baseline sessions. Criterion was not increased above the maximum number of points available to earn. Children met their point goals for at least one session of the three conducted each day and so received access to a preferred activity or choice from the prize box on each day of intervention.
Third, following each JA post-training session of 5 min of play, the interventionist reviewed the session with the TD peer to provide additional feedback. Review consisted of a brief verbal overview of behaviors that were demonstrated well and those that needed improvement (similar to feedback during TD peer-training sessions). Feedback lasted approximately 2 min. The interventionist re-introduced training at the beginning of the next day’s session when TD peer performance decreased below 80% correct responding for two consecutive sessions. Re-training consisted of modeling, role play, and feedback for any targets for which a decline below 80% performance criterion was observed.
Due to a decrease in TD peer prompting and reinforcement during JA sessions compared to training, the interventionist provided an overview of prompting and reinforcement to each TD peer before viewing the final video prior to each post-training JA session. This began in session 43 for Ollie, session 28 for Kendra, and session 58 for Amanda. During the overview, the interventionist defined prompting and reinforcement, presented the video demonstrating the respective behaviors, and then engaged in role play of reinforcement and prompting prior to presenting the final video segment demonstrating all the target behaviors.
Mastery criterion for JA for the child with ASD was set by observing two TD peers (not otherwise involved with this study) playing the same types of games as children played in this study. TD peers participated in two sessions conducted in the same way as JA baseline sessions for the children with ASD and TD peers. After observing the percentage of independent RJA and IJA during peer interactions (average 40%), we set mastery criterion level slightly higher than peers’ performance to increase the probability of maintaining higher levels of performance post-intervention. Mastery criterion was set at 60% or better correct independent responding for RJA and IJA across two consecutive sessions across two consecutive days.
Generalization
Generalization of JA behaviors for each child with ASD was examined during interactions with a novel TD peer. Probes were conducted in the same way as JA baseline sessions. One probe was conducted during JA baseline and one upon mastery of both RJA and IJA.
Maintenance
Maintenance was examined 2 months following the end of intervention. One 5-min JA post-training session was conducted with each TD peer and child with ASD; however, no video model was presented prior to maintenance probes.
Social Validity
Parent Perceptions
Over the course of intervention, parents had observed their children’s sessions in the home and center and so we asked parents to rate statements about the importance and appropriateness of peer-mediated intervention to improve social skills and their perception of the effectiveness of the intervention on their children’s JA skills. Table 4 shows the questions parents were asked. Ratings ranged from 1 to 5: 1 (strongly disagree), 2 (disagree), 3 (neither agree or disagree), 4 (agree), and 5 (strongly agree). One parent of each child with ASD completed the questionnaire within 2 weeks of the end of intervention.
Table 4.
Parent social validity ratings
| Alex | Tyler | Amelia | |
|---|---|---|---|
| I think it is important to teach children how to interact with peers. | 5 | 5 | 5 |
| I think it is important to teach peers how to interact with children with ASD. | 5 | 5 | 5 |
| Peer-mediated teaching improved my child’s joint attention. | 5 | 5 | 5 |
| The intervention improved my child’s play skills with other children. | 5 | 5 | 5 |
Social validity ratings ranged from 1 (strongly disagree) to 5 (strongly agree)
TD Peer Reactions
Within 2 weeks of the end of intervention, each TD peer’s parent interviewed the TD peer about his/her experience. The interventionist provided the interview questions and reviewed them with the parent prior to the interview. The interview was based on that used by Kamps, Kravits, Gonzalez Lopez, Kemmerer, Potucek and Garrison Harrel (1998) with peers in a study of social interactions with children with ASD. The parent read from the materials the interventionist provided. The parent provided the TD peer with brief instructions and presented her with three emoticon cards (a smiley face, a neutral face, and a sad face). The parent asked the TD peer questions regarding her experience. The TD peer answered by selecting one of the emoticons to represent her feelings (e.g., “I had fun learning using video modeling,” “I learned how to help others”). The parent also asked three open-ended questions about the TD peer’s favorite part of the program, what she learned, and anything she would change about the program.
Professional Observations
Three professionals who provide applied behavior analysis therapy to children with ASD reviewed video recordings from intervention and completed a questionnaire. The professionals were graduate students or providers who work in the field of behavior analysis. They viewed video recordings of the first JA baseline session, one final TD peer-training session in which the peer was expected to demonstrate all target behaviors, a session from the middle of JA post-training session (chosen at random), and the last mastery JA post-training session showing independent responding. Professionals were blind to the conditions they viewed. The interventionist randomly assigned one professional to watch the four videos from one peer dyad. Each professional observed and then rated statements about the appropriateness and acceptability of the target behaviors (e.g., “I believe there is a need to implement peer training.”) and intervention procedures (e.g., “I find video modeling to be a useful teaching tool.”), and whether the intervention appeared to have been an effective approach to train peers and increase JA in children with ASD (e.g., “Upon reviewing the peer-training video, I saw improvement in peer behaviors.”). Ratings ranged from 1 (strongly disagree) to 5 (strongly agree).
Interobserver Agreement
All sessions were video recorded. After a session, the interventionist who implemented intervention scored children’s performance for that session. Thirty percent of sessions for each dyad and condition were chosen using a random number generator to examine interobserver agreement (IOA). One of the interventionists who did not implement intervention in the session served as the IOA observer for that session. An agreement occurred if both the observer and interventionist scored an opportunity in the same way (i.e., correct or incorrect). Trial-by-trial IOA was calculated by dividing the number of agreements by the number of agreements plus disagreements multiplied by 100. Mean calculations include outliers.
Mean IOA for Ollie was 93% for baseline (range, 83–100%) and 89% for intervention (range, 83–100%). Mean IOA for Kendra was 87% for baseline (range, 83–100%) and 92% for intervention (range, 83–100%). Mean IOA for Amanda was 92% for baseline (range, 83–100%) and 89% for intervention (range, 83–100%).
Mean IOA for Alex for IJA and RJA was 100% for baseline. During intervention, IOA was 80% for IJA (range, 80–100%, with one outlier at 60%) and 94% for RJA (range, 80–100%). Mean IOA for Thomas for IJA and RJA was 90 and 98%, respectively, for baseline (range, 80–100%). During intervention, IOA was 89% for IJA (range, 80–100%) and 92% for RJA (range, 80–100%). Mean IOA for Amelia for IJA and RJA was 88 and 92%, respectively, for baseline (range, 80–100%). During intervention, IOA was 88% for IJA (range, 80–100%) and 85% for RJA (range, 80–100%, with one outlier at 60%).
Intervention Integrity
Intervention integrity was examined for the same sessions as IOA (30% of sessions for each dyad and condition) using the same video recordings and a checklist of the intervention procedures. The observer scored each intervention procedure implemented by the interventionists as correct (“yes”), incorrect (“no”), or (“n/a”). Intervention integrity was calculated as the number of times the interventionist followed the steps correctly divided by the total number of correct and incorrect steps, multiplied by 100. Intervention integrity ranged from 90 to 100%.
Results
TD Peer Performance
Figure 1 displays TD peer percentage of correct target behaviors of each of the three TD peers. All three TD peers showed low and stable baseline levels ranging from 3 to 33%. TD peer performance increased during training sessions with the interventionists (not depicted) to 80% or better (per criterion). During JA post-training sessions, TD peer performance was largely higher than baseline levels but did not reach the 80% performance level seen during training. Ollie’s and Amanda’s performance during JA post-training sessions increased above baseline performance, ranging from 33 to 63% and 34 to 69%, respectively. Kendra’s performance was more variable with performance during some sessions overlapping baseline performance (range, 21–67%). During intervention for the last target behavior, performance leveled off at a mean of 34% (range, 24–52%), only slightly above her mean baseline performance of 25%.
Fig. 1.
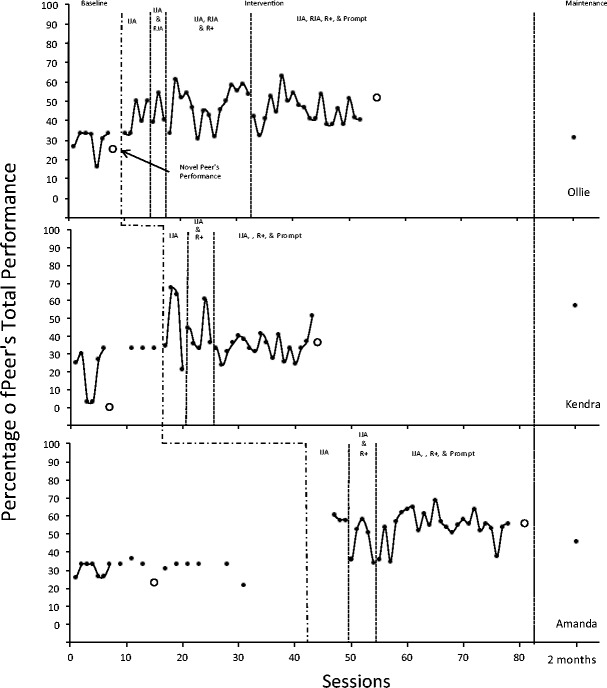
Percentage of opportunities with correct responses for typical peers during JA baseline, post-training sessions, and maintenance. IJA (initiating joint attention), RJA (responding to joint attention) R+ (providing reinforcement), & Prompt are noted to indicate when those respective target behaviors were trained
Children with ASD JA Performance
Figures 2 and 3 show percent independent correct RJA and IJA performance, respectively, of the children with ASD during baseline, intervention, generalization with novel peers, and maintenance. The horizontal line represents the mastery criterion level (60%). Alex’s RJA performance during baseline was stable at a mean of 1% correct responding (range, 0–9.5%) (Fig. 2). During intervention, RJA increased to a mean of 36% (range, 0–100%). Although Alex did not meet mastery criterion for RJA, his performance during six of the intervention sessions (compared to zero sessions during baseline) was above mastery level. During baseline, Alex’s mean IJA performance was 15% and variable (range, 0–17% with one session above mastery level at 64%) (Fig. 3). Alex met mastery criterion for IJA at session 40 (indicated by a star) after which his mean performance was 79% (range, 27–100%). IJA performance was at or above mastery level for 14 sessions during intervention compared to 1 session during baseline.
Fig. 2.
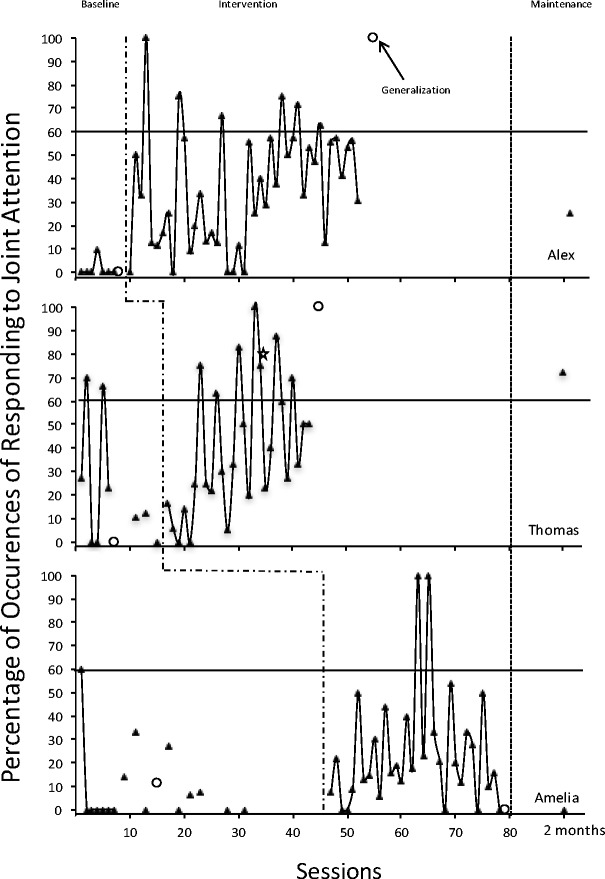
Percentage of opportunities with independent RJA responding for all three children with ASD during JA baseline and JA post-training sessions. The open circle denotes generalization probes. The horizontal line indicates the set mastery criterion level, and the open star denotes when mastery criterion was met
Fig. 3.
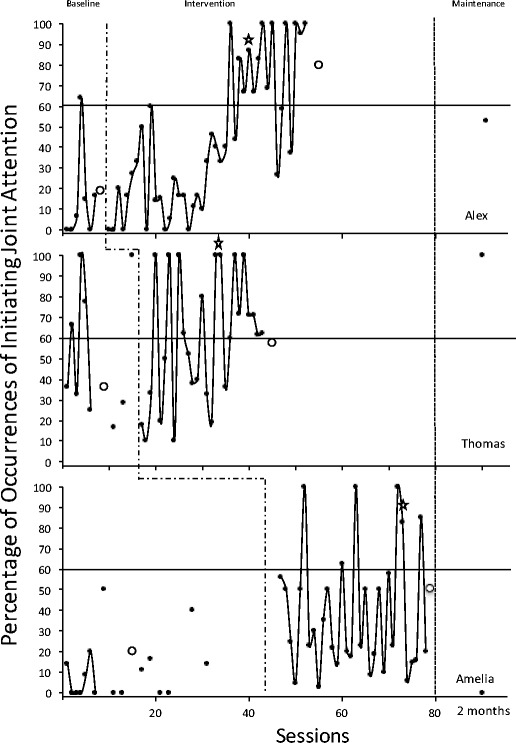
Percentage of opportunities with independent IJA responding for all three children with ASD during JA baseline and JA post-training sessions. The open circle denotes generalization probes. The horizontal line indicates the set mastery criterion level, and the open star denotes when mastery was met
Thomas’ mean performance of RJA during baseline was 23% and variable (range, 0–27% with two sessions above mastery level at 67 and 70%) (Fig. 2). Thomas’ performance of RJA met mastery criterion on session 34. Although his performance of RJA was variable (M = 43%, range, 0–100%), it was at or above mastery level for 7 sessions during intervention compared to 2 sessions during baseline. Thomas’ mean performance of IJA during baseline was 54% and variable (range, 17–100%) (Fig. 3). As with RJA, Thomas’ IJA performance during intervention was variable (M = 61%, range, 10–100%), and he met mastery criterion at session 34. IJA was at or above mastery level for 14 sessions during intervention compared to 3 sessions during baseline.
Amelia’s mean performance of RJA during baseline was 9% and variable (range, 0–33% with one session at mastery level of 60%) (Fig. 2). She did not meet RJA mastery criterion (M = 27%, range, 0–100%), although her performance during 2 intervention sessions (compared to 1 session during baseline that reached 60%) was at or above mastery level. Amelia’s mean performance of IJA during baseline was 11% and variable (range, 0–50%) (Fig. 3). She met mastery criterion for IJA at session 73. As with RJA performance, Amelia’s IJA performance during intervention was variable (M = 38%, range, 2.9–100%), but at or above mastery for 5 sessions during intervention compared to 0 sessions during baseline. Intervention ended after several sessions with no further improvement in either RJA or IJA behaviors.
Generalization
Figures 1, 2, and 3 also depict generalization performance. On Fig. 1, which shows TD peers’ performance, generalization probes show the novel peers’ performance. Novel peers actually performed similarly to trained peers, showing lower performance during baseline and slight increases at the end of intervention.
Figures 2 and 3 show RJA and IJA performance, respectively, for each child with ASD with a novel peer. Children showed some increases in RJA and IJA from baseline to post-intervention. RJA increased above the mastery criterion level of 60% for Alex and Thomas. IJA increased above the mastery criterion level for Alex; Thomas’ and Amelia’s performance nearly met mastery criterion level (58 and 50%, respectively).
Maintenance
Two-month maintenance probes showed that Alex’s performance declined below the 60% mastery level to 25% for RJA and 53% for IJA. Thomas’ performance, however, was well above the mastery level at 72% for RJA and 100% for IJA. Amelia’s performance declined back down to baseline levels of 0% for both RJA and IJA.
Social Validity
Parent Perceptions
Parents strongly agreed (5) (Table 4) with all statements about the importance and appropriateness of peer-mediated interactions to improve social skills and perceived the intervention to have been effective in increasing their child’s JA skills.
TD Peer Reactions
TD peers selected the smiley faces for all the questions, indicating they “loved it” (Table 5). They had fun learning using video modeling and loved playing with their new friend. The TD peers said they enjoyed the games they played and learning how to help others. They also said they would love to play again. The open-ended questions revealed that TD peers would have liked to have more new games to play each week and include more children in the games. The TD peers also indicated they learned how to wait more for their friends and when to tell their friends they were doing a good job.
Table 5.
Typical peer validity ratings
| Ollie | Kendra | Amanda | |
|---|---|---|---|
| I had fun learning using video modeling. | Smiley | Smiley | Smiley |
| I liked playing with (child with ASD’s name). | Smiley | Smiley | Smiley |
| I liked earning dojo points. | Smiley | Smiley | Smiley |
| I would like to play at the Loft again. | Smiley | Smiley | Smiley |
| I learned how to help others. | Smiley | Smiley | Smiley |
| I enjoyed the games we played. | Smiley | Smiley | Smiley |
Social validity ratings ranged from sad face (I didn’t like it), to neutral face (It was okay), to Smiley face (Loved it)
Professional Observations
All three professionals had positive responses (Table 6). Professionals agreed (4) or strongly agreed (5) with the need for peer training and the usefulness of video models and that both TD peers and children with ASD showed improvements over the course of intervention.
Table 6.
Professional social validity ratings
| Professional 1 | Professional 2 | Professional 3 | |
|---|---|---|---|
| I believe there is a need to implement peer training. | 4 | 4 | 5 |
| I find video modeling to be a useful teaching tool. | 4 | 4 | 5 |
| Upon reviewing peer-training video, I saw improvement in peer behaviors. | 4 | 4 | 5 |
| Upon reviewing the final intervention video, I observed improvement in both peers and children with ASD interactions. | 4 | 5 | 5 |
| I would use video modeling to train social skills behaviors. | 4 | 4 | 5 |
Social validity ratings ranged from 1 (strongly disagree) to 5 (strongly agree)
Discussion
The purpose of the present study was to examine the effects of peer training on peer’s engagement in strategies to facilitate JA in children with ASD and JA behaviors in children with ASD during play sessions without adult mediation. Peer training consisting of verbal instructions, live and video models, role play, and feedback, with the video models presented to the peer just prior to JA sessions with the child with ASD, was associated with some improvement in peer use of strategies to facilitate JA and overall improvements in JA in the children with ASD. Outcomes were judged by parents, professionals, and TD peers themselves as positive.
TD Peer Performance
TD peers showed increases in the behaviors taught to facilitate JA in peers with ASD during training with the interventionists, but only slight increases and very variable performance during JA post-training sessions with the children with ASD. Although, overall, children with ASD showed increases in JA behavior, it is not clear, given the variability and slight increases in TD peer behaviors, that JA behavior increased in association with any change in TD peer behavior. It could be that TD peers already possessed the right or sufficient skills to facilitate interactions with the children with ASD, and given repeated opportunities to do so, JA interactions of the children with ASD improved. Novel peers involved in generalization probes also showed increases in their performance from baseline to the end of intervention. Novel peers received training through the center; their training focused generally on initiating interactions, providing choices during interactions, prompting correct responding, and providing reinforcement to the children with ASD for their participation during interactions. We identified a number of similar target behaviors, but focused on JA responses, as important for peers to engage in to facilitate JA. Perhaps, a general peer-training program is all that is needed or there are other important behaviors such as persistence maintaining interactions that will help support peer JA skills in children with ASD.
The variability in TD peer performance may also relate to several factors. Including video models may decrease the need for additional adult mediation that can disrupt natural peer interactions. We did not prompt, reinforce, or correct TD peer behaviors during JA sessions that involved both the TD peer and child with ASD. However, in many studies of peer-mediated interventions, adults still prompt, reinforce, and correct errors during peer interactions (for review, see Chang & Locke, 2016; Chan et al., 2009; Zhang & Wheeler, 2011). As a result, children may remain dependent upon adults to direct their interactions, and those interactions may not proceed naturally because of adult involvement. Children may also be less likely to generalize to natural interactions in which adults are not present. It could be that adding interventionist prompting during JA post-training sessions would have increased TD peer performance. Isolating the effects of video models, interventionist prompting, and other components of training as well as examining different combinations (e.g., video modeling and prompting during interactions with the child with ASD) could provide more effective training approaches.
Interventionists also implemented a token system in which TD peers received prizes for meeting a minimum number of points each session. During training, the interventionist provided feedback when giving points. During JA post-training sessions, interventionists allocated points but did not provide feedback when points were tallied. This was done so as to not disrupt the children’s ongoing interaction. In doing so, it may be that the interventionists did not create a clear response reinforcement contingency. In fact, TD peer performance during training with the interventionist met mastery criterion, but performance during JA post-training sessions with the children with ASD was variable and never reached the same high levels it did during training. TD peer performance in other peer-training studies is not always at the usual mastery levels such as 80%. For example, Ferraioli and Harris (2011) found that siblings performed some behaviors at much lower levels than others (e.g., praise) and this was with additional prompts from adults during sessions with the sibling and child with ASD. Including feedback, as is often done in peer training, may have improved TD peer performance. Figuring out how to do so without disrupting children’s interactions will be important in future research. Perhaps, teaching TD peers to self-monitor their engagement in strategies to support JA is one way to continue to minimize adult mediation, but improve TD peer performance. Comparisons of combinations of these various components (live and video models, adult prompting, reinforcement clearly indicated during interactions between the children) will be important in future research.
Variable TD peer performance during JA post-training sessions could also relate to the frequency of training and JA sessions. Sessions occurred only once a week with some missed sessions due to scheduling conflicts (e.g., vacations, illnesses). Although the TD peers were familiar with the children with ASD, they had no prior experience with peer training. The novel generalization peers who had been at the center for some time and received some training through other center activities showed an increase in performance from baseline to generalization sessions conducted at the end of intervention. It could be that the improvements in JA in the children with ASD resulted in overall changes in the interactions with and behaviors of the peers, including the novel peers. It could also be that more frequent training and more time in similar activities with children with ASD results in stronger TD peer performance.
Characteristics of the TD peers (and the children with ASD) may have also impacted their performance. The TD peers and children with ASD were familiar with each other outside of the context of this study. Alex, Amelia, Ollie, and Amanda had previous play dates. Thomas and Kendra were siblings. As siblings, they had a long history of interactions outside of the study context; during JA sessions, they argued about game rules and discussed previous disagreements. Although familiarity may be a good thing, it is important to recognize that this may impact children’s performance. It is likely that TD peers involved in interventions with children with ASD will be familiar to the children—neighbors, family members, etc. In the case of family members such as siblings, it is also important to consider the impact that participation in intervention may have on the sibling who may otherwise be impacted by ASD in the family (e.g., increased expectations, taking on a caregiver role).
All TD peers were similar in age (above 6 years of age as per the criteria) and all girls. It is not clear if there is an appropriate or necessary minimum age for peer training and whether age or gender may have impacted performance in this study. Sisters of a sibling with ASD may take on more of a caregiver role than brothers (e.g., Tomeny, Baker, Barry, Edlred, & Rankin, 2016). This characteristic may also be evident in female peers in general and potentially yield different outcomes compared to male peers.
Children with ASD JA Performance
All three children with ASD met mastery criterion for IJA, though performance for Thomas and Amelia was variable. RJA performance was variable throughout baseline and intervention, and only Thomas met mastery criterion for RJA. Children with ASD also generalized to novel peers (with the exception of RJA for Amelia). The one maintenance probe conducted 2 months after the end of intervention indicated inconsistent performance across children with ASD. One probe of maintenance provides limited information. Future research may include additional maintenance probes to examine long-term performance outcomes and additional measures of generalization (e.g., to other natural contexts with peers such as school or playground).
Because of the slight increases in level and variable TD peer and children with ASD JA performance, this is not the clearest demonstration of the effect of peer training on JA behaviors, warranting further research. However, social validity data and anecdotal observations suggest JA improved in a rather positive way. Parents and professionals both strongly agreed social interactions improved between the TD peers and children with ASD. Anecdotally, interventionists commented about how natural interactions between the TD peers and children with ASD appeared at the end of intervention. Conversations between the TD peers and children with ASD were observed to be less rote and robotic than initially. Children appeared to enjoy interacting; their play and conversations became longer in duration. Perhaps, there are other JA behaviors and/or other social interaction behaviors that would provide a direct observation measure of what parents, professionals, and the TD peers noticed about the behavior of the children with ASD and their interactions.
The variable and sometimes low-level JA performance may relate to the response topography chosen. The target JA behaviors, gaze shift and verbalization, were chosen consistent with the strong verbal repertoires of the children with ASD. Observations of TD peer interactions playing similar games showed this response topography as well as other topographies (e.g., gesture). But, perhaps the gaze shift response is not necessary at such a high level as 60% of opportunities during ongoing interactions with each child in close proximity such as during table top game play. If so, children may not naturally engage in this JA topography as often to reach the 60% mastery level (a level slightly higher than what we observed in TD peer interactions). This may be especially true for RJA when children may be able to share attention on the object of JA because of the verbal content of the RJA directive; for example, when the TD peer says, “Wow, it’s a 2!” the child with ASD looks to the “2” or the relevant game piece because of the verbal content without needing to check in by gazing at the peer. In fact, RJA performance was overall poorer than IJA performance. Deciding what response topography to teach requires careful examination of both RJA and IJA in TD children of a range of ages during different types of interactions (e.g., table top turn-taking games, gross motor activities).
The choice of response topography may also be impacted by the repertoire of the child with ASD. We chose to teach a combination of two components (gaze shift and verbalization) taught simultaneously, something that may also be difficult. Children with ASD who have a different repertoire may benefit from being taught different topographies entirely or one component at a time. For example, focusing on gaze shift and gestures or just gaze shift would be appropriate with children who do not have a similar speech repertoire as the children in this study.
It is also important to point out the difficulty interventionists had judging JA behaviors, even though data were collected from video recordings rather than live. Although average IOA was within an acceptable range, there were three outliers. Lower IOA is consistent with some of the other JA literature (e.g., Ferraioli & Harris, 2011; Whalen & Schreibman, 2003). JA can be challenging to observe. Eye gaze movements can be difficult to see live or from video recordings depending upon the positioning and orientation of the children. Verbalizations can be difficult to hear, understand, and/or determine if they are related to the activity. In addition, the natural peer interactions during game play that were recorded in this study only further contribute to making JA behaviors difficult to observe. It is important that those teaching JA have a clear understanding of the operational definitions and adequate training in judging JA behaviors. In addition, experience recording behavior during natural interactions will be necessary to minimize extra distractions to the observer.
Mastery criterion was based upon observation of two TD children playing similar games as in JA sessions. This 60% mastery criterion was slightly higher than what was observed for the peers, but lower than the 80% criterion used in many JA intervention studies. It is not clear what should be considered the criterion level of JA behavior during ongoing interactions such as while playing games. Instead of setting an absolute value as the criterion level of performance, criterion could be set to incrementally increase based on individual performance.
There are several additional factors to consider in evaluating children’s JA performance and this intervention that may be important in attempting such an intervention to improve outcomes in the future. First, as with TD peer performance, the frequency of sessions may have impacted variability in JA performance and mastery for the children with ASD. In the current study, children only attended sessions one time per week, dictating the frequency of sessions. In contrast, in much of the existing JA intervention literature, sessions occurred daily (typically with caregivers), though there are a few studies in which sessions occurred as little as two or fewer times per week (typically with an interventionist) (Murza et al., 2016). Paparella and Freeman (2015) point out that session frequency may impact JA outcomes. Increasing the frequency of sessions may improve performance of both TD peers and children with ASD.
Second, the peer-training literature suggests that performance of the children with ASD may improve through training multiple peers (e.g., English, Goldstein, Shafer, & Kaczmarek, 1997). Multiple peers could also potentially provide more frequent opportunities in a natural setting. Although an attempt was made to recruit multiple peers, we were unable to identify additional TD peers, an obstacle many practitioners face especially in private clinic settings. Practitioners teaching children in schools that include both TD children and those with disabilities may be at an advantage recruiting multiple peers for peer training.
Third, game choice influenced opportunities for JA. For example, while playing Connect4™, the children actually told the interventionists they were not engaging in JA so as to not give away any information about their game play strategy. In contrast, during Headbandz™, children wear a headband holding a card depicting an object and they must each look at the other’s headband to ask and answer questions relating to the card, increasing the likelihood of JA behavior.
Lastly, as with TD peers, the absence of adult mediation may have also impacted performance of the children with ASD. We know adults can prompt and reinforce JA behaviors in children with ASD. Introducing even a little adult direction, such as prompting JA in the child with ASD and providing additional reinforcement, might have augmented what TD peers were doing and resulted in greater improvements in JA.
Summary
This is one of the few studies to examine peer training to facilitate JA in children with ASD with their TD peers. It is also one of the only studies that focused on peer intervention without the mediation of an adult. Peer training involved instructions, modeling, role play, and feedback; modeling was both live and on video and the video models were presented just prior to JA sessions with the children with ASD. TD peers implemented strategies including presenting opportunities, prompting, and reinforcing JA behaviors during JA sessions with children with ASD. TD peers showed some improvement in strategies to support JA, and children with ASD showed some increases in JA. Importantly, parents and professionals judged the interactions as improved.
The role of video models in peer training, strategies necessary to teach peers, and peer characteristics warrant further investigation. Frequency of sessions, target JA topographies, making observations during natural interactions, and choice of materials must all be considered by practitioners teaching JA to children with ASD and their peers.
Acknowledgements
We would like to thank Alysha Rafeeq and Ridda Sheikh for their assistance with this research.
Funding Information
This research was conducted by the first author as part of the requirements for her graduate program in Psychology and supported in part by a Doctoral Student Research Grant from the Graduate Center of the City University of New York.
Compliance with Ethical Standards
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
• Effective intervention procedures to teach JA to children with autism spectrum disorder (ASD) can be applied to interactions between children with ASD and their typically developing (TD) peers.
• Peer training involving instructions, live and video models, role play, and feedback resulted in some improvement in peer prompting and reinforcing JA and overall increases in JA in children with ASD.
• Future research and clinical application should consider characteristics of the children, strategies to teach TD peers, frequency of sessions, and choice of materials when teaching JA to children with ASD and their peers.
References
- Adamson L, Bakeman R, Deckner D, Romski M. Joint engagement and the emergence of language in children with autism and Down syndrome. Journal of Autism and Developmental Disorders. 2009;39(1):84–96. doi: 10.1007/s10803-008-0601-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 2000. [Google Scholar]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5. Washington, DC: Author; 2013. [Google Scholar]
- Bakeman R, Adamson LB. Coordinating attention to people and objects in mother-infant and peer-infant interaction. Child Development. 1984;55(4):1278–1289. doi: 10.2307/1129997. [DOI] [PubMed] [Google Scholar]
- Barbaro J, Dissanayake C. Early markers of autism spectrum disorders in infants and toddlers prospectively identified in the social attention and communication study. Autism. 2012;17(1):64–86. doi: 10.1177/1362361312442597. [DOI] [PubMed] [Google Scholar]
- Bates E. The emergence of symbols: cognition and communication in infancy. New York: Academic; 1979. [Google Scholar]
- Benzies K, Magill-Evans M, Kurilova J, Nettel-Aguirre A, Blahitka L, Lacaze-Masmonteil T. Effects of video modeling on the interaction skills of first-time fathers of late pre-term infants. Infants and Young Children. 2013;26(4):333–348. doi: 10.1097/IYC.0b013e3182a4ed5e. [DOI] [Google Scholar]
- Buggey T, Ogle L. Video self-modeling. Psychology in the Schools. 2012;49(1):52–70. doi: 10.1002/pits.20618. [DOI] [Google Scholar]
- Catania C, Almeida D, Liu-Constant B, Digennaro Reed F. Video modeling to train staff to implement discreet trial instruction. Journal of Applied Behavior Analysis. 2009;42(2):387–392. doi: 10.1901/jaba.2009.42-387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chan JM, Lang R, Rispoli M, O’Reilly M, Sigafoos J, Cole H. Use of peer-mediated interventions in the treatment of autism spectrum disorders: a systematic review. Research in Autism Spectrum Disorders. 2009;3:876–889. doi: 10.1016/j.rasd.2009.04.003. [DOI] [Google Scholar]
- Chang YC, Locke J. Research in autism spectrum disorders: a systematic review of the effects of choice on academic outcomes for students with autism spectrum disorder. Research in Autism Spectrum Disorders. 2016;27:1–16. doi: 10.1016/j.rasd.2016.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- English K, Goldstein H, Shafer K, Kaczmarek L. Promoting interactions among preschoolers with and without disabilities; effects of a buddy skills-training program. Exceptional Children. 1997;63(2):229–244. doi: 10.1177/001440299706300206. [DOI] [Google Scholar]
- Ferraioli SJ, Harris SL. Teaching joint attention to children with autism through a sibling-mediated behavioral intervention. Behavior Interventions. 2011;26:261–281. doi: 10.1002/bin.336. [DOI] [Google Scholar]
- Jones EA, Feeley KM. Parent implemented joint attention intervention for preschoolers with autism. Journal of Speech-Language Pathology and Applied Behavior Analysis. 2007;2(3):253–268. [Google Scholar]
- Jones EA, Carr EG, Feeley KM. Multiple effects of joint attention intervention for children with autism. Behavior Modification. 2006;30:782–834. doi: 10.1177/0145445506289392. [DOI] [PubMed] [Google Scholar]
- Kamps DM, Kravits T, Gonzalez Lopez A, Kemmerer K, Potucek J, Garrison Harrel L. What do you the peers think? Social validity of peer-mediated programs. Education and Treatment of Children. 1998;21(2):107–134. [Google Scholar]
- Kasari C, Freeman S, Paparella T. Joint attention and symbolic play in young children with autism: a randomized controlled intervention study. Journal of Child Psychology and Psychiatry. 2006;47:611–620. doi: 10.1111/j.1469-7610.2005.01567.x. [DOI] [PubMed] [Google Scholar]
- Kasari C, Gulsrud AC, Wong C, Kwon S, Locke J. Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. Journal of Autism and Developmental Disorders. 2010;40(9):1045–1056. doi: 10.1007/s10803-010-0955-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lawton K, Kasari C. Brief report: longitudinal improvements in the quality of joint attention in preschool children with autism. Journal of Autism and Developmental Disorders. 2012;42(2):307–312. doi: 10.1007/s10803-011-1231-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason RA, Ganz JB, Parker RI, Bruke MD, Camargo SP. Moderating factors of video-modeling with other as model: a meta-analysis of single-case studies. Research in Developmental Disabilities. 2012;33:1076–1086. doi: 10.1016/j.ridd.2012.01.016. [DOI] [PubMed] [Google Scholar]
- Mason RA, Davis HS, Boles MB, Goodwyn F. Efficacy of point-of-view video modeling: a meta-analysis. Remedial and Special Education. 2013;34:333–345. doi: 10.1177/0741932513486298. [DOI] [Google Scholar]
- Meindl JN, Cannella-Malone HI. Initiating and responding to joint attention bids in children with autism. A review of the literature. Research in Developmental Disabilities. 2011;32:1441–1454. doi: 10.1016/j.ridd.2011.02.013. [DOI] [PubMed] [Google Scholar]
- Mundy P, Crowson M. Joint attention and early social communication: implications for research on intervention with autism. Journal of Autism and Developmental Disorders. 1997;27(6):653–676. doi: 10.1023/A:1025802832021. [DOI] [PubMed] [Google Scholar]
- Mundy P, Sigman M, Kasari C. Joint attention, developmental level, and symptom presentation in autism. Development and Psychopathology. 1994;6:389–401. doi: 10.1017/S0954579400006003. [DOI] [Google Scholar]
- Murza KA, Schwartz JB, Hahs-Vaughn DL, Nye C. Joint attention interventions for children with autism spectrum disorder: a systematic review and meta-analysis. International Journal of Language and Communication Disorders. 2016;51(3):235–251. doi: 10.1111/1460-6984.12212. [DOI] [PubMed] [Google Scholar]
- Ninio A, Bruner J. The achievement and antecedents of labeling. Journal of Child Language. 1978;5:1–16. doi: 10.1017/S0305000900001896. [DOI] [Google Scholar]
- Paparella T, Freeman FN. Methods to improve joint attention in young children with autism: a review. Pediatric Health, Medicine, Therapeutics. 2015;6:65–78. doi: 10.2147/PHMT.S41921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomasello M, Ferrar MJ. Joint attention and early language. Society for Research in Child Development. 1986;57(6):1454–1463. doi: 10.2307/1130423. [DOI] [PubMed] [Google Scholar]
- Tomeny TS, Baker LK, Barry TD, Eldred SW, Rankin JA. Emotional and behavioral functioning of typically-developing sisters of children with autism spectrum disorder: the roles of ASD severity, parental stress, and marital status. Research in Autism Spectrum Disorders. 2016;32:130–142. doi: 10.1016/j.rasd.2016.09.008. [DOI] [Google Scholar]
- Whalen C, Schreibman L. Joint attention training for children with autism using behavior modification procedures. Journal of Child Psychology and Psychiatry. 2003;44:456–468. doi: 10.1111/1469-7610.00135. [DOI] [PubMed] [Google Scholar]
- White PJ, O’Reilly M, Streusand W, Levine A, Sigafoos J, Lancioni G, Fragale C, Pierce N, Aguilar J. Best practices for teaching joint attention: a systematic review of the intervention literature. Research in Autism Spectrum Disorders. 2011;5:1283–1295. doi: 10.1016/j.rasd.2011.02.003. [DOI] [Google Scholar]
- Zhang J, Wheeler JJ. A meta-analysis of peer-mediated interventions for young children with autism spectrum disorders. Education and Training in Autism and Developmental Disabilities. 2011;46(1):62–77. [Google Scholar]