

Abstract
Fusobacterium nucleatum is an oral anaerobe prevalent in intrauterine infection associated with a wide spectrum of adverse pregnancy outcomes. We demonstrate here that F. nucleatum triggers placental inflammation through maternal, rather than paternal, TLR4-mediated signaling. Elimination of TLR4 from maternal endothelial cells alleviated placental inflammation and reduced fetal and neonatal death, while elimination of TLR4 in the hematopoietic cells had no effect. The placental inflammatory response followed a spatiotemporal pattern, with NF-κB activation observed first in the maternal endothelial cells and then in the decidual cells surrounding the endothelium, followed by induction of inflammatory cytokines and chemokines. Supplementation of pregnant mice with fish oil as a source of omega-3 fatty acids suppressed placental inflammation, reduced F. nucleatum proliferation in the placenta, and increased fetal and neonatal survival. In vitro analysis illustrates that omega-3 fatty acids inhibit bacterial-induced inflammatory responses from human umbilical cord endothelial cells. Our study therefore reveals a mechanism by which microbial infections affect pregnancy and identifies a prophylactic therapy to protect against intrauterine infections.
Keywords: Microbiology
Keywords: Bacterial infections
Fusobacterium nucleatum induces placental inflammation originating from maternal endothelial cell that is suppressible by omega-3 fatty acids.
Introduction
Intrauterine infection is a leading cause of adverse pregnancy outcomes (APOs), including preterm birth, stillbirth, neonatal sepsis, etc. Fusobacterium nucleatum is among the most prevalent microorganisms in intrauterine infection; it is implicated in 10%–30% of preterm births, with its detection inversely related to the gestational age at birth (1–7). Bacteria detected in intrauterine infection has been conventionally suggested to ascend from the lower genital tract; however, F. nucleatum presents a surprising alternative in that it is absent in the normal vaginal flora and instead is ubiquitous in the oral cavity frequently associated with periodontal disease (1, 8, 9). We have previously reported that F. nucleatum from the subgingival plaque likely translocates to the fetoplacental unit through hematogenous transmission as a result of transient dental bacteremia (2). With pregnancy-associated gingivitis affecting 30%–100% of the pregnant population, transient dental bacteremia is a frequent event during gestation (10–13). When F. nucleatum was injected into the tail veins of pregnant mice to mimic dental bacteremia, it colonized specifically in the murine placenta; first, it was detected in the venous sinuses or at foci adjacent to the venous sinuses in the decidua, and then it spread beyond the decidua to the placental membranes and fetal vessels (13). The bacteria eventually spread to the amniotic fluids and fetuses after 2–3 days, resulting in fetal demise. Although F. nucleatum was detected in the liver and spleen of the dam at 6 hours following tail-vein injection, it was cleared after 24 hours. Thus, F. nucleatum infection was localized within the fetoplacental unit, without causing systemic infection (13). This acute infection model is consistent with a previously reported human case of stillbirth, in which F. nucleatum was isolated from the mother’s placenta and as pure culture from the stillborn infant’s lung and stomach (2). In both mice and the human case, placental colonization by F. nucleatum was accompanied by neutrophil infiltration. In mice lacking TLR4, the fetal death rate was reduced despite bacterial colonization, indicating that inflammation was the cause of fetal demise (14). However, the source of inflammation was unknown. In the present study, we examine the source and mechanism of F. nucleatum–induced placental inflammation and potential therapy to circumvent such inflammation.
Results
TLR4 mediates placental inflammation caused by F. nucleatum.
TLRs play a key role in the host innate immune response to infection. LPS, an endotoxin present on the outer membrane of Gram-negative bacteria, is recognized by TLR4, which then activates NF-κB to initiate transcription of proinflammatory molecules (15). To investigate the host immune responses to F. nucleatum infection, we injected approximately 107 CFU into the tail vein of pregnant wild-type C57BL/6 and Tlr4–/– mice (to mimic dental bacteremia) on day 16–17 of gestation as described previously (14, 16). Using nonpregnant mice, we found that F. nucleatum titers in the blood circulation underwent two phases of killing following tail-vein injection (Supplemental Figure 1; supplemental material available online with this article; https://doi.org/10.1172/jci.insight.125436DS1). The first phase occurred within the first hour, with the live F. nucleatum titer reducing by 3 logs. The titers then remained stable for the next 2 hours, before entering the second (and slower) reduction phase, until F. nucleatum was completely eliminated. As shown previously (16), F. nucleatum was evenly disseminated to the liver, spleen, and placenta at 6 hours after tail-vein injection, when the titer in the circulation was relatively stable at approximately 103 to 104 CFU/ml (Supplemental Figure 1). It has been reported that the bacterial titer in the blood can reach 105 CFU/ml in healthy individuals and 106 CFU/ml in periodontitis patients, with the mean quantities for F. nucleatum reaching 104 CFU/ml in healthy and 105 CFU/ml in diseased individuals (17). Thus, our injection dose was within the biological range. As reported previously, F. nucleatum did not persist in the liver or spleen and was cleared after 24 hours; instead, it proliferated specifically in the placenta (16). A temporal inflammatory activation was observed in the placenta (Figure 1A). At 24 hours following injection, a marked increase in the mRNA levels of the proinflammatory cytokines IL-1α (IL1a), TNF-α (Tnfa), and granulocyte-macrophage CSF (Gmcsf/Csf2); chemokine monocyte chemotactic protein 1 (Mcp1/Ccl2) and chemokine ligand 5 (Ccl5/Rantes); and COX-2 (Cox2), an enzyme mediating prostaglandin production during bacterial infection, was observed in comparison to the saline controls. At 48 hours, substantial induction of IL-1β (IL1b) mRNA, along with continued induction of Mcp1 and Gmcsf, was detected, suggesting a time-dependent exacerbation of inflammation (Figure 1A). IL-12 (IL12), IL-18 (IL18), IL-6 (IL6), keratinocyte chemoattractant (KC/CXCL1), leukemia inhibitory factor (LIF), and hypoxia-inducible factor 1-α (HIF1a) were tested but not significantly induced in either wild-type or TLR4–/– mice (Supplemental Figure 2). H&E staining of the placenta showed tissue necrosis and neutrophil infiltration in the infected placenta at 48 hours after injection but not in the uninfected controls (Figure 1, B and C). The protein levels of IL-1β in the infected placentas were also markedly increased, as shown by immunohistochemical staining (Figure 1, D and E). In contrast, in Tlr4–/– pregnant mice, no induction of inflammatory cytokines and chemokines was detected, even after 48 hours of injection of F. nucleatum (Figure 1A). These results demonstrate that induction of TLR4-mediated inflammatory responses precedes fetal death, which occurs after 48–72 hours following F. nucleatum injection (16).
Figure 1. F. nucleatum induces placental inflammation through TLR4.

On day 16 or 17 of gestation, each C57BL/6 wild-type or TLR4–/– mouse received approximately 107 CFU of F. nucleatum 12230 or saline. (A) At 24 or 48 hours after injection, the placentas were collected for RNA extraction. The mRNA levels of inflammatory cytokines and chemokines were measured by real-time quantitative PCR and are expressed as fold change compared to the saline-injected control group. At least 4 pregnant mice were included in each group. The results are presented as dot plots with average and SEM. Two-way ANOVA was performed with simple-effects analysis when the interaction was significant. Student-Newman-Keuls was applied for post-hoc comparisons. *P < 0.05, **P < 0.01. (B–E) H&E staining (B and C) and immunohistochemical staining of IL-1β (D and E) in the decidua of wild-type mice at 48 hours after injection with saline (B and D) or approximately 107 CFU of F. nucleatum (C and E). Original magnification, ×100 (B and C); ×500 (D and E); zoom, 3-fold from ×100 image (insets). Representative image from 4 placentas from 2 dams of each group was selected.
F. nucleatum–induced placental inflammation originates from the maternal endothelial cells.
The placenta consists of cells derived from both maternal (decidua and maternal blood vessels) and fetal (cytotrophoblasts, syncytiotrophoblasts, and fetal blood vessels) origins (18). To further dissect TLR4-mediated inflammation, Tlr4+/– chimeric placentas were generated by mating wild-type C57BL/6 (Tlr4+/+) and Tlr4–/– parents, followed by F. nucleatum infection. The fetal and neonatal death rates of Tlr4+/+ dams and Tlr4–/– sires were similar to those whose parents were both Tlr4+/+ (Figure 2A). In contrast, the death rates were substantially lower in Tlr4–/– dams, regardless of the paternal genotypes (Figure 2A). Consistent with the birth outcomes, the expression levels of inflammatory cytokines and chemokines were markedly induced in placentas from Tlr4+/+, but not Tlr4–/–, dams, regardless of the paternal genotypes (Figure 2, B and C). These observations support that fetal and neonatal death results from placental inflammation of the maternal origin.
Figure 2. F.

nucleatum–induced placental inflammation originates from the maternal endothelial cells. Approximately 107 CFU F. nucleatum 12230 or saline was injected into the tail vein of each C57BL/6 pregnant dam on day 16 or 17 of gestation. (A) The fetal and neonatal death rate was calculated as the percentage of dead fetuses and neonates per litter at birth and followed up to 3 days after birth. Genotypes of the mating parents are shown below the x axis. Each geometric symbol represents 1 pregnant mouse. The horizontal lines indicate the average death rates. (B) mRNA levels in the placentas measured by real-time quantitative PCR and expressed as fold changes compared with each genotypes’ own saline-injected control groups. At least 3 pregnant dams were included in each group. (C) Protein levels of IL-1β in the placentas, as determined by ELISA. At least 3 pregnant dams were included in each group. For B and C, the placentas were collected at 48 hours after injection and pooled for each pregnant dam. The results are presented as dot plots with average and SEM. Two-way ANOVA was performed with simple-effects analysis when the interaction was significant. Student-Newman-Keuls was applied for post-hoc comparisons. *P < 0.05, **P < 0.01, ***P < 0.001. D, Dam; S, Sire.
Hematopoietic and endothelial cells express various pattern recognition receptors, such as TLRs, and are active responders to hematogenous infections. To identify the maternal cell type(s) that elicit the inflammatory responses to F. nucleatum, two Cre-LoxP mouse strains were constructed: Vav1-iCre;Tlr4fl/fl, with Tlr4 deleted in 100% of hematopoietic cells (19), and Tie2Cre;Tlr4fl/fl, with Tlr4 deleted in 80% of hematopoietic and 100% of endothelial cells (20, 21). In comparison to the control group of Tlr4fl/fl mice, which were equivalent to Tlr4+/+ mice, fetal and neonatal death rates following F. nucleatum infection were significantly reduced in Tie2-Cre;Tlr4fl/fl mice, whereas no difference was detected in Vav1-iCre;Tlr4fl/fl mice (Figure 2A). Furthermore, the mRNA levels of inflammatory cytokines and chemokines were significantly reduced in F. nucleatum–infected Tie2-Cre;Tlr4fl/fl placentas but not in Vav1-iCre;Tlr4fl/fl placentas (Figure 2B). These results suggest that TLR4 in the endothelial cells is critical for causing placental inflammation and fetal and neonatal demise.
To confirm this finding, we performed immunohistochemical analysis to examine NF-κB activation in the decidua. As soon as 30 minutes after injection, nuclei translocation of the immunoreactive p65 subunit of NF-κB (also known as RelA) was detected in the decidual endothelial cells of the wild-type, Tlr4fl/fl, and Vav1-iCre;Tlr4fl/fl placentas (Figure 3, A, D, and F). After 2 hours, p65 was no longer detected in the endothelial nuclei but was instead in the nuclei of the surrounding cells (Figure 3, G and I). No nuclear translocation of p65 was detected in the saline control or F. nucleatum–infected Tlr4–/– or Tie2-Cre;Tlr4fl/fl placentas (Figure 3, B, C, E, and H), demonstrating that the decidual endothelial TLR4 plays a critical role in NF-κB activation. We therefore conclude that placental inflammation originates from the maternal endothelial cells in this model. Combining the results from Figure 1 and Figure 3, a spatiotemporal pattern of the placental inflammation has emerged, i.e., sequential NF-κB activation in the decidua precedes production of inflammatory cytokines and chemokines.
Figure 3. F. nucleatuminduces nuclear translocation of the p65 subunit of NF-κB in the decidua.

Immunohistochemical staining of the p65 subunit of NF-κB in the decidua of wild-type C57BL/6 (A, B, and G), Tlr4–/– (C), Tlr4f/f (D), Tie2-Cre;Tlr4f/f (E and H), and Vav1-iCre;Tlr4f/f (F and I) mice at 30 minutes (A–F) and 2 hours (G–I) after injection with saline (B) or approximately 107 CFU F. nucleatum (A, C, and D–I). Immunoreactive p65 was detected in the endothelial nuclei in A, D, and F and in the cells surrounding the venous sinuses (V) in G and I (insets). No nuclear p65 was detected in B, C, E, or H. Original magnification, ×500; zoom, 3.5- to 5-fold (insets). Representative image of at least 3 placentas from 1–2 dams of each group was selected.
Dietary omega-3 fatty acids suppress F.
nucleatum–induced placental inflammation and protect fetuses. Dietary supplementation of omega-3 polyunsaturated fatty acids in the form of fish oil has been widely used to reduce inflammation in chronic inflammatory diseases, such as cardiovascular disease and rheumatoid arthritis, and has been safely recommended for use during pregnancy (22–29). Humans consuming a diet rich in fish oil have been shown to harbor increased quantities of omega-3 fatty acids, such as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), in their cellular phospholipid membranes (30) and in breast milk (31). Increase in omega-3 fatty acids in the cellular composition has been associated with antiinflammatory and immunosuppressive properties, although the extent and the mechanism of immune modulation may vary depending on the nature of fatty acids, source of infection and inflammation, and infected tissue or cell types (22, 32–37).
To determine their antiinflammatory effects in endothelial cells, purified omega-3 fatty acids, EPA (20:5n-3) and DHA (22:6n-3), mixed at 3:1, were preincubated with primary cultures of human umbilical vein endothelial cells (HUVECs) prior to addition of F. nucleatum. A common omega-6 fatty acid, arachidonic acid (20:4n-6), was tested as a control. The mRNA expression levels of MCP1, IL8, CCL5, IL1β, and IL6 and the endothelial activation markers intercellular adhesion molecule 1 (ICAM1) and E selectin were induced by F. nucleatum but the induction was substantially suppressed in cells preincubated with omega-3 fatty acids in a dose-dependent manner (Figure 4). In contrast, only a few inflammatory markers were inhibited by omega-6 fatty acids, even at the maximum dose tested (Figure 4).
Figure 4. Purified omega-3 fatty acids suppress endothelial inflammation induced by F. nucleatum.

Purified omega-3 (300 μM or 600 μM) or omega-6 fatty acids (600 μM) were complexed with fatty acid–free BSA at a molar ratio of 4:1 and preincubated with HUVECs for 3 hours prior to bacterial infection. Log-phase F. nucleatum was incubated with primary HUVECs at an MOI of 50:1 for 24 hours. Levels of mRNA were measured by real-time quantitative PCR and are expressed as fold change compared to the uninfected control group. Each experiment was performed in triplicates and repeated at least 3 times. The results are presented as dot plots with average and SEM. One-way ANOVA was performed with Bonferroni post-test. **P < 0.01, ***P < 0.001, ****P < 0.0001.
For in vivo testing, pregnant mice were orally gavaged with fish oil as a source of omega-3 fatty acids throughout the gestation until they were injected with F. nucleatum. The fetal and neonatal death rate was markedly reduced in C57BL/6 mice fed with 33 mg omega-3 fatty acids compared with the water-gavaged controls (Figure 5A). The supplementation did not affect the maternal body weight (Supplemental Figure 3). In order to determine if the observed fetal and neonatal protection was specific to C57BL/6 mice, and because humans are outbred, the outbred CF-1 mice were also tested. Similar results were obtained, and a dose-dependent pattern was observed. A trend of fetal and neonatal death reduction was detected at a lower dose of 3 mg omega-3 fatty acids, which reached significance at a higher dose of 16 mg (Figure 5C). Placental inflammation was suppressed by omega-3 fatty acids in both C57BL/6 and CF-1 mice, as shown by real-time qPCR analysis of inflammatory molecules at 48 hours after F. nucleatum injection (Figure 5, B and D).
Figure 5. Omega-3 fatty acids reduce F. nucleatum–induced fetal and neonatal death, placental inflammation, and bacterial proliferation.

Inbred C57BL/6 mice and outbred CF-1 mice were gavaged with fish oil, water, or nothing throughout the gestation starting day 1 through day 16 or 17, when approximately 107 CFU of F. nucleatum 12230 or saline was injected via tail vein. (A and C) Fetal and neonatal death rates of C57BL/6 (A) and CF-1 mice (C). Death rates are expressed as the percentage of dead fetus and neonates of each litter at birth and followed through 3 days after birth. Each geometric symbol represents 1 pregnant mouse. Treatment is listed below the x axis. The horizontal lines indicate the average death rates, and error bars represent SEM. (B and D) Placental inflammatory mRNA gene expression levels in C57BL/6 (B) or CF-1 mice (D) at 48 hours after injection. Gene expression is presented as fold change in comparison to the saline-injected controls, with average and SEM. At least 5 pregnant mice were included in each group. (E and F) Live F. nucleatum titers in the placentas of C57BL/6 (E) or CF-1 mice (F) at 48 and 72 hours (E) or 24, 48, and 72 hours (F) after injection are expressed as log(CFU per gram tissue). At least 3 pregnant mice were included in each group. The results are presented as dot plots, with average and SEM. Mann-Whitney test (A) or 2-way ANOVA (B–F) was performed with simple-effects analysis when the interaction was significant. Student-Newman-Keuls was applied for post-hoc comparisons. *P < 0.05, **P < 0.01, ***P < 0.001.
Surprisingly, omega-3 fatty acids also suppressed F. nucleatum proliferation in the placenta. In both C57BL/6 and CF-1 mice, the live bacterial titers increased with time in the control placentas, consistent with a previous report (16); however, they remained stagnant in C57BL/6 placentas and decreased in CF-1 placentas following supplementation with omega-3 fatty acids (Figure 5, E and F). Bacteriostatic properties of omega-3 fatty acids have been reported for Helicobacter pylori, both in vitro and in vivo (38–40), suggesting omega-3 fatty acids as potential preventives for H. pylori–associated gastric diseases. However, for F. nucleatum, in vitro testing showed that omega-3 fatty acids exhibited no bactericidal effects in vitro (Supplemental Figure 4). It is likely that the lack of proliferation is secondary to the suppression of inflammation due to the possible inflammophilic nature of F. nucleatum (41). In support of this possibility are the observations that the immune suppression was detected at 48 hours but the stagnation of proliferation in C57BL/6 was not evident until 72 hours after injection (Figure 5, C and E). In addition, F. nucleatum titers in Tlr4–/– placentas exhibited stagnation after 48 hours, with or without fish oil supplementation, further supporting that the lack of inflammation prohibited bacterial proliferation (Supplemental Figure 5).
In order to test if the effect of omega-3 fatty acids is specific for F. nucleatum, HUVECs were infected with methicillin-resistant Staphylococcus aureus (MRSA), a Gram-positive pathogen and a leading cause of health care–associated infections (42). Omega-3 fatty acids more effectively reduced the expression of all inflammatory genes tested than omega-6 fatty acids (Supplemental Figure 6A). To determine if omega-3 fatty acids alleviate the inflammatory responses mediated through TLR signaling, we tested expression of inflammatory cytokines and chemokines in primary HUVECs following incubation with purified E. coli LPS, a TLR4 agonist, and Pam3CSK, a TLR2 agonist (Supplemental Figure 6B). While both LPS and Pam3CSK upregulated expression of the inflammatory genes, cells preincubated with omega-3 fatty acids exhibited markedly lower inflammatory responses to both LPS and Pam3CSK. Omega-6 fatty acids showed no inhibitory effect. These results demonstrate that omega-3 fatty acids effectively suppress endothelial inflammation induced by both Gram-negative and Gram-positive microorganisms.
Discussion
Here, we investigate the placental inflammatory response and its effect on pregnancy outcome using F. nucleatum as stimuli. F. nucleatum–induced placental inflammatory response exhibited a spatiotemporal pattern. TLR4-dependent activation of NF-κB was first detected in the decidual endothelial cells and then in the neighboring tissues, followed by continuous induction of proinflammatory cytokines and chemokines. Inhibition of placental inflammation in mice lacking TLR4 led to protection of the fetuses, suggesting that the TLR4-mediated inflammatory responses are the cause, either direct or indirect, of fetal and neonatal demise. These results contrast with those of numerous other studies demonstrating TLR4 as playing a protective role against bacterial infection (43–48). In fact, TLR4 expression exclusively on endothelial cells has been shown to be sufficient to clear systemic E. coli infection in nonpregnant mice (49). The unusual deleterious role of TLR4 in placental infection possibly reflects the immunological features at the maternal-fetal interface. It appears that placental TLR4, especially the maternal endothelial TLR4, renders the fetoplacental unit highly sensitive to inflammatory responses to infectious microorganisms, causing harm rather than protection.
Elimination of maternal but not paternal TLR4 inhibited placental inflammation. To the best of our knowledge, this is the first demonstration that intrauterine microbial infection triggers inflammation from a maternal source. Our study further identified the maternal endothelium as the origin of inflammation. This is consistent with our previous observation that F. nucleatum infection of the murine placenta is localized primarily in the decidua (16), where the maternal blood is perfused into the placenta through spiral arteries (50). The endothelial cells play an important role in early modulation of immune response against infectious microorganisms, marked by increased permeability, leukocyte adherence, and angiogenesis (51). In our model of hematogenous infection, the endothelial cells are understandably the first to come into contact with the pathogen. Elimination of endothelial TLR4 blocked the downstream placental inflammation and protected the fetuses from F. nucleatum infection. This is consistent with our previous observation of sequential detection F. nucleatum in the blood vessels and adherence and invasion of the endothelial cells, followed by colonization and proliferation in the decidua of infected placentas (13).
The amount of F. nucleatum in the blood of healthy and periodontal disease patients shows a remarkable difference, but the magnitude of live F. nucleatum colonizing the placenta in clinical setting has not yet been reported (17). In consideration of literature that suggests F. nucleatum as a commensal microbe in the placenta (52, 53), our study supports that there may be a concentration dependence, or even a threshold, of the bacterial load in the placenta in causing placental inflammation. This is consistent with our previous report that F. nucleatum–induced murine fetal death rate was dose dependent. At an injection dose of 4 × 105 CFU, the fetal death rate was merely 6% (16). It is plausible that at low doses F. nucleatum either do not colonize or colonize at a very low level without inducing inflammatory responses. Supplementation with omega-3 fatty acids appears to keep the titer of F. nucleatum below that required for activation of inflammatory responses, thus protecting the fetuses.
Having identified the inflammatory origin allowed us to develop intervention therapies. Benefits of omega-3 fatty acids and their metabolites have been studied extensively in infectious diseases (54–60). Our results show that purified omega-3 fatty acids EPA and DHA suppress inflammatory responses in endothelial cells mediated by both TLR2 and TLR4 and protect against inflammation caused by both Gram-positive and Gram-negative bacteria in vitro. EPA and DHA are precursors of proresolving lipid mediators and low-inflammatory eicosanoids whose functions include inhibition of trans-endothelial neutrophil migration, promotion of macrophage clearance of apoptotic neutrophils, and activation of antiinflammatory cytokines and adhesion molecules (61–67). A large body of literature has demonstrated the antiinflammatory properties of omega-3 fatty acids (68–71); nonetheless, some clinical trials of dietary supplementation of omega-3 fatty acids have shown no effect (35, 36, 72). Many supplementation studies have only tested modest doses. However, the present study and other successful human trials suggest that doses higher than currently recommended may be necessary for special conditions (27, 73–77).
Besides suppression of inflammation, omega-3 fatty acids also inhibited F. nucleatum proliferation in the placenta, which appeared to be secondary to the immune suppression. This is likely due to the inflammophilic nature of F. nucleatum. Previous studies have reported that periodontal pathogens, e.g., Porphyromonas gingivalis, are inflammophilic in that inflammation generates a favorable environment for its proliferation due to an abundance of degraded proteins and enrichment of nutrient-rich exudates (78). F. nucleatum is a strong immune stimulator (79–82), consistent with the inflammophilic characteristics. Fetal protection may be a result of immune suppression alone or in combination with inhibition of bacterial proliferation. Regardless, this proof-of-concept study opens a wide door for developing therapies to prevent APOs induced by F. nucleatum and possibly other microorganisms that cause localized intrauterine infections.
The notion that omega-3 fatty acids may protect against bacterial infection during pregnancy is very exciting, especially because there are no safe prophylactic therapies currently available. Given that intrauterine infection may occur at any point during pregnancy, continuous use of antibiotics for preventive purpose is impractical. Dietary supplementation of omega-3 fatty acids has been recommended for pregnant women for its benefits in maternal depression, fetal growth, and childhood neurologic and immune development (83–85). Our results suggest that it may protect against APO. Previous studies suggest that a variety of oral bacteria may colonize the placenta through hematogenous translocation (1, 52, 86). Our study demonstrates that omega-3 fatty acids suppress endothelial inflammatory responses caused by both Gram-positive and Gram-negative bacteria. Future studies should examine the effects of omega-3 fatty acids in reducing APOs caused by different inflammatory stimuli.
Methods
Bacterial and mouse strains.
F. nucleatum 12230 was maintained as previously described (87). S. aureus LAC USA300 CA-MRSA was obtained from Alice Prince (Columbia University, New York, New York, USA) and grown in Lysogeny Broth (BD) or on Tryptic Soy Agar plates (BD). CF-1 wild-type mice were purchased from National Cancer Institute Mouse Repository or Charles River Laboratories. C57BL/6 wild-type mice were purchased from The Jackson Laboratory and bred in-house. Tie2-Cre (20) and Vav1-iCre (19) mice were gifts of Lei Ding (Columbia University). Tlr4–/– mice (88) were obtained from Robert Schwabe (Columbia University). Tlr4fl/fl mice (89) were obtained from David Hackam (Johns Hopkins University, Baltimore, Maryland, USA). All mice were kept in sterilized filtered-topped cages with a 12-hour light cycle, fed autoclaved food (PicoLab Mouse Diet 20 5058; 22 kcal% fat, 55 kcal% carbohydrate, and 23 kcal% protein) and water ad libitum, and handled in a laminar flow hood.
Mating, fish oil administration, and i.v. injection of mice.
Mating was conducted as previously described (16). Briefly, mice were caged together at a female-to-male ratio of 2:1. Mating was determined by the presence of a white vaginal plug. The day when the plug was detected was termed day 1 of gestation. Mice were randomly distributed to study groups. The omega-3 group received 3, 16, or 33 mg omega-3 fatty acids from commercial fish oil every other day (for C57BL/6) or every day (for CF-1) from day 1 to day 16 of gestation by oral gavage. The gavage schedule was determined through consultation with the vet. The control group received an equal volume of sterilized water (C57BL/6) or nothing (CF-1). Pregnant mice were injected with approximately 107 CFU of F. nucleatum on day 16 or 17, as described previously (16). The death rates of the fetuses and the neonates were recorded up to 3 days after birth. For measuring the level of inflammatory response, mice were sacrificed at the indicated time after injection, and placentas of each dam were pooled and processed for mRNA expression analysis (see Real-time quantitative PCR for experimental details). The live bacterial titer was determined from placentas or blood collected from tail tips by serial dilutions on blood agar plates. The titer was expressed as log CFU/ml of blood or log CFU/g of tissue.
Endothelial cell cultures.
Primary cultures of HUVECs were isolated as previously described (90). The cells were maintained at 37°C in 5% CO2 in complete medium using EGM-2 Bullet Kit (LONZA). HUVECs were seeded into 6-well plates coated with rat collagen type I (Corning, 354236) and allowed to grow to confluency. For fatty acid treatment, DHA, EPA, arachidonic acid, or an equal volume of absolute ethanol as vehicle control were mixed with 1% low-fatty-acid and endotoxin-free BSA (US Biological, A1311). Growth medium was replaced with antibiotics-free medium containing indicated concentrations of the fatty acids or vehicle control for 3 hours, followed by incubation with F. nucleatum 12230, ultra-pure LPS from E. coli 0111:B4 (Invivogen, tlrl-3pelps), or N-palmitoyl(S)-[2,3-bis(palmitoyloxy)-(2, RS)-propyl]-Cys-Ser-Lys4 (Pam3CSK4) (Invivogen, tlrl-pms) for 24 hours or with S. aureus for 5 hours.
Real-time quantitative PCR.
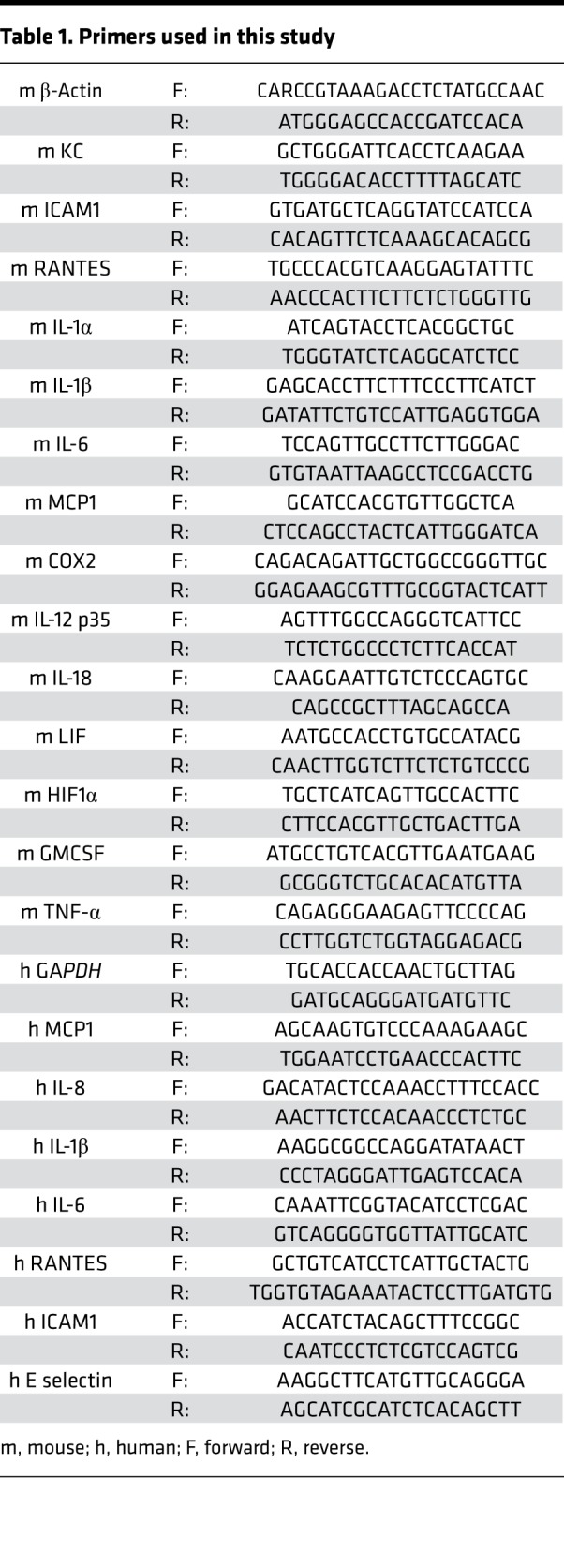
RNA was extracted from HUVECs or mouse placental tissues using a Qiagen RNeasy Mini Kit (Qiagen, 74106). The quantity and quality of extracted RNA were measured using a NanoDrop ND 1000 spectrophotometer (NanoDrop Technologies). cDNA was synthesized by reverse-transcription PCR using the Superscript IV First-Strand Synthesis System (Invitrogen, 18091050) according to the manufacturer’s instructions. Real-time quantitative PCR was performed in duplicates, using StepOnePlus (Applied Biosystems). Each reaction was prepared with the Power SYBR Green PCR Master Mix kit according to the manufacturer’s instructions (Applied Biosystems). Specific forward and reverse primers (Table 1) were used at a concentration of 500 nM. PCR amplifications were performed with 40 cycles of 95°C for 30 seconds, 59°C for 30 seconds, and 72°C for 30 seconds. The results were expressed as 2–ΔCt, where ΔCt is the difference between the mean Ct value of the targeted gene and the endogenous GAPDH or β-actin control. The fold change was calculated in comparison to the saline, PBS, or vehicle-treated control groups.
Table 1. Primers used in this study.
Immunohistochemistry.
Mouse placentas were fixed in 4% paraformaldehyde, dehydrated in ethanol, and embedded in paraffin. Tissue sections of 3 μm were placed on electro-charged slides and heated in a 60°C oven for 1 hour, deparaffinized in xylene, and rehydrated sequentially in 100%, 95%, and 75% ethanol and water. Antigen retrieval was performed in low-pH solution (Dako Omnis) for 30 minutes at 98°C. After washing in tap water, endogenous peroxidase was quenched in 3% hydrogen peroxide, followed by cell permeabilization in 0.3% Triton X-100. Slides were incubated with 10% horse serum and 0.05% Tween 20 for 30 minutes, followed by rabbit anti–IL-1β antibody (Abcam, ab9722), rabbit anti–NF-κB p65 subunit antibody (Cell Signaling Technology, CST8242), or rabbit IgG isotype control for 2 hours at room temperature. After washes, slides were incubated with ImmPRESS HRP anti-rabbit IgG (Vector Lab) for 30 minutes at room temperature. Slides were developed with the DAB Peroxidase Substrate Kit (Vector Lab) and counterstained with 20% hematoxylin followed by 1% ammonium hydroxide.
ELISA.
Placental tissues (50 mg) were homogenized in 500 μl tissue extraction reagent I (Invitrogen, FNN0071) with 5 μl protease inhibitor (Thermo) and 1% Triton (Invitrogen). Total protein concentrations in the supernatants were measured using the BCA kit. IL-1β was measured by ELISA Antibody Pair (Invitrogen, CMC0813) according to the manufacture’s protocol.
Statistics.
All results are expressed as the mean ± SEM. Nonparametric Kruskal-Wallis test with Conover post-test was used for comparison of fetal and neonatal death rates (InfoStat version 2014, Córdoba University, Córdoba, Argentina). One-way ANOVA with Bonferroni post-test or two-way ANOVA with simple-effects analysis and Student-Newman-Keuls post-test were used for group comparisons (GraphPad Prism 5.00 for Windows). All tests were 2 sided, and a P values of less than 0.05 were considered statistically significant.
Study approval.
This study has been approved by the Institutional Animal Care and Use Committee at Columbia University.
Author contributions
JGS, XZ, and XY performed experiments; JGS wrote the manuscript; MRR performed statistical analysis; DYM and JK prepared primary cultures of HUVECs; KL participated in experimental design and manuscript preparation; and YWH conceived, designed, and supervised the study and wrote the manuscript.
Supplementary Material
Acknowledgments
The authors thank Richard Deckelbaum for discussions about the use of purified omega-3 fatty acids, Lei Ding for providing the Vav1-iCre and Tie2Cre mice, Robert Schwabe for the Tlr4–/– mice, and David Hackam for the Tlr4fl/fl mice. This work was supported in part by NIH grants R01s DE014924, DE023332, and CA192111 to YWH and R21OD02329 to KL.
Version 1. 02/07/2019
Electronic publication
Footnotes
Conflict of interest: The authors have declared that no conflict of interest exists.
License: Copyright 2019, American Society for Clinical Investigation.
Reference information: JCI Insight. 2019;4(2):e125436. https://doi.org/10.1172/jci.insight.125436.
Contributor Information
Jeewon Garcia-So, Email: js4530@cumc.columbia.edu.
Xinwen Zhang, Email: xianxinwen@icloud.com.
Xiaohua Yang, Email: judyyang626@gmail.com.
Mara Roxana Rubinstein, Email: mgr2152@cumc.columbia.edu.
Jan Kitajewski, Email: kitaj@uic.edu.
Kang Liu, Email: kl2529@columbia.edu.
References
- 1.Fardini Y, Chung P, Dumm R, Joshi N, Han YW. Transmission of diverse oral bacteria to murine placenta: evidence for the oral microbiome as a potential source of intrauterine infection. Infect Immun. 2010;78(4):1789–1796. doi: 10.1128/IAI.01395-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Han YW, et al. Term stillbirth caused by oral Fusobacterium nucleatum. Obstet Gynecol. 2010;115(2 Pt 2):442–445. doi: 10.1097/AOG.0b013e3181cb9955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Miller JM, Pupkin MJ, Hill GB. Bacterial colonization of amniotic fluid from intact fetal membranes. Am J Obstet Gynecol. 1980;136(6):796–804. doi: 10.1016/0002-9378(80)90458-5. [DOI] [PubMed] [Google Scholar]
- 4.Chaim W, Mazor M. Intraamniotic infection with fusobacteria. Arch Gynecol Obstet. 1992;251(1):1–7. doi: 10.1007/BF02718272. [DOI] [PubMed] [Google Scholar]
- 5.Bearfield C, Davenport ES, Sivapathasundaram V, Allaker RP. Possible association between amniotic fluid micro-organism infection and microflora in the mouth. BJOG. 2002;109(5):527–533. doi: 10.1111/j.1471-0528.2002.01349.x. [DOI] [PubMed] [Google Scholar]
- 6.Cahill RJ, et al. Universal DNA primers amplify bacterial DNA from human fetal membranes and link Fusobacterium nucleatum with prolonged preterm membrane rupture. Mol Hum Reprod. 2005;11(10):761–766. doi: 10.1093/molehr/gah234. [DOI] [PubMed] [Google Scholar]
- 7.Ebersole JL, et al. Systemic immune responses in pregnancy and periodontitis: relationship to pregnancy outcomes in the Obstetrics and Periodontal Therapy (OPT) study. J Periodontol. 2009;80(6):953–960. doi: 10.1902/jop.2009.080464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hill GB. Preterm birth: associations with genital and possibly oral microflora. Ann Periodontol. 1998;3(1):222–232. doi: 10.1902/annals.1998.3.1.222. [DOI] [PubMed] [Google Scholar]
- 9.Offenbacher S, et al. Periodontal infection as a possible risk factor for preterm low birth weight. J Periodontol. 1996;67(10 Suppl):1103–1113. doi: 10.1902/jop.1996.67.10s.1103. [DOI] [PubMed] [Google Scholar]
- 10.Onigbinde O, Sorunke M, Braimoh M, Adeniyi A. Periodontal status and some variables among pregnant women in a Nigeria tertiary institution. Ann Med Health Sci Res. 2014;4(6):852–857. doi: 10.4103/2141-9248.144876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lieff S, et al. The oral conditions and pregnancy study: periodontal status of a cohort of pregnant women. J Periodontol. 2004;75(1):116–126. doi: 10.1902/jop.2004.75.1.116. [DOI] [PubMed] [Google Scholar]
- 12.Carrillo-de-Albornoz A, Figuero E, Herrera D, Cuesta P, Bascones-Martínez A. Gingival changes during pregnancy: III. Impact of clinical, microbiological, immunological and socio-demographic factors on gingival inflammation. J Clin Periodontol. 2012;39(3):272–283. doi: 10.1111/j.1600-051X.2011.01800.x. [DOI] [PubMed] [Google Scholar]
- 13.Ifesanya JU, Ifesanya AO, Asuzu MC, Oke GA. Determinants of good oral hygiene among pregnant women in ibadan, South-Western Nigeria. Ann Ib Postgrad Med. 2010;8(2):95–100. doi: 10.4314/aipm.v8i2.71820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liu H, Redline RW, Han YW. Fusobacterium nucleatum induces fetal death in mice via stimulation of TLR4-mediated placental inflammatory response. J Immunol. 2007;179(4):2501–2508. doi: 10.4049/jimmunol.179.4.2501. [DOI] [PubMed] [Google Scholar]
- 15.Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell. 2010;140(6):805–820. doi: 10.1016/j.cell.2010.01.022. [DOI] [PubMed] [Google Scholar]
- 16.Han YW, Redline RW, Li M, Yin L, Hill GB, McCormick TS. Fusobacterium nucleatum induces premature and term stillbirths in pregnant mice: implication of oral bacteria in preterm birth. Infect Immun. 2004;72(4):2272–2279. doi: 10.1128/IAI.72.4.2272-2279.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Marín MJ, et al. Comparison of the detection of periodontal pathogens in bacteraemia after tooth brushing by culture and molecular techniques. Med Oral Patol Oral Cir Bucal. 2016;21(3):e276–e284. doi: 10.4317/medoral.20842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Frost JM, Moore GE. The importance of imprinting in the human placenta. PLoS Genet. 2010;6(7):e1001015. doi: 10.1371/journal.pgen.1001015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.de Boer J, et al. Transgenic mice with hematopoietic and lymphoid specific expression of Cre. Eur J Immunol. 2003;33(2):314–325. doi: 10.1002/immu.200310005. [DOI] [PubMed] [Google Scholar]
- 20.Koni PA, Joshi SK, Temann UA, Olson D, Burkly L, Flavell RA. Conditional vascular cell adhesion molecule 1 deletion in mice: impaired lymphocyte migration to bone marrow. J Exp Med. 2001;193(6):741–754. doi: 10.1084/jem.193.6.741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Constien R, et al. Characterization of a novel EGFP reporter mouse to monitor Cre recombination as demonstrated by a Tie2 Cre mouse line. Genesis. 2001;30(1):36–44. doi: 10.1002/gene.1030. [DOI] [PubMed] [Google Scholar]
- 22.Gioxari A, Kaliora AC, Marantidou F, Panagiotakos DP. Intake of ω-3 polyunsaturated fatty acids in patients with rheumatoid arthritis: A systematic review and meta-analysis. Nutrition. 2018;45:114–124.e4. doi: 10.1016/j.nut.2017.06.023. [DOI] [PubMed] [Google Scholar]
- 23.Veselinovic M, et al. Clinical Benefits of n-3 PUFA and ɤ-linolenic acid in patients with rheumatoid arthritis. Nutrients. 2017;9(4):E325. doi: 10.3390/nu9040325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Yates CM, Calder PC, Ed Rainger G. Pharmacology and therapeutics of omega-3 polyunsaturated fatty acids in chronic inflammatory disease. Pharmacol Ther. 2014;141(3):272–282. doi: 10.1016/j.pharmthera.2013.10.010. [DOI] [PubMed] [Google Scholar]
- 25.Calder PC. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochem Soc Trans. 2017;45(5):1105–1115. doi: 10.1042/BST20160474. [DOI] [PubMed] [Google Scholar]
- 26.Olsen SF, et al. Randomised controlled trial of effect of fish-oil supplementation on pregnancy duration. Lancet. 1992;339(8800):1003–1007. doi: 10.1016/0140-6736(92)90533-9. [DOI] [PubMed] [Google Scholar]
- 27.Dunstan JA, Simmer K, Dixon G, Prescott SL. Cognitive assessment of children at age 2(1/2) years after maternal fish oil supplementation in pregnancy: a randomised controlled trial. Arch Dis Child Fetal Neonatal Ed. 2008;93(1):F45–F50. doi: 10.1136/adc.2006.099085. [DOI] [PubMed] [Google Scholar]
- 28.Greenberg JA, Bell SJ, Ausdal WV. Omega-3 Fatty Acid supplementation during pregnancy. Rev Obstet Gynecol. 2008;1(4):162–169. [PMC free article] [PubMed] [Google Scholar]
- 29.Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA. Maternal supplementation with very-long-chain n-3 fatty acids during pregnancy and lactation augments children’s IQ at 4 years of age. Pediatrics. 2003;111(1):e39–e44. doi: 10.1542/peds.111.1.e39. [DOI] [PubMed] [Google Scholar]
- 30.Yaqoob P, Pala HS, Cortina-Borja M, Newsholme EA, Calder PC. Encapsulated fish oil enriched in alpha-tocopherol alters plasma phospholipid and mononuclear cell fatty acid compositions but not mononuclear cell functions. Eur J Clin Invest. 2000;30(3):260–274. doi: 10.1046/j.1365-2362.2000.00623.x. [DOI] [PubMed] [Google Scholar]
- 31.Helland IB, Saarem K, Saugstad OD, Drevon CA. Fatty acid composition in maternal milk and plasma during supplementation with cod liver oil. Eur J Clin Nutr. 1998;52(11):839–845. doi: 10.1038/sj.ejcn.1600656. [DOI] [PubMed] [Google Scholar]
- 32.Guo XF, Li X, Shi M, Li D. n-3 Polyunsaturated fatty acids and metabolic syndrome risk: a meta-analysis. Nutrients. 2017;9(7) doi: 10.3390/nu9070703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Saccone G, Berghella V. Omega-3 supplementation to prevent recurrent preterm birth: a systematic review and metaanalysis of randomized controlled trials. Am J Obstet Gynecol. 2015;213(2):135–140. doi: 10.1016/j.ajog.2015.03.013. [DOI] [PubMed] [Google Scholar]
- 34.Kar S, Wong M, Rogozinska E, Thangaratinam S. Effects of omega-3 fatty acids in prevention of early preterm delivery: a systematic review and meta-analysis of randomized studies. Eur J Obstet Gynecol Reprod Biol. 2016;198:40–46. doi: 10.1016/j.ejogrb.2015.11.033. [DOI] [PubMed] [Google Scholar]
- 35.Watanabe Y, Tatsuno I. Omega-3 polyunsaturated fatty acids for cardiovascular diseases: present, past and future. Expert Rev Clin Pharmacol. 2017;10(8):865–873. doi: 10.1080/17512433.2017.1333902. [DOI] [PubMed] [Google Scholar]
- 36.Søyland E, et al. Effect of dietary supplementation with very-long-chain n-3 fatty acids in patients with psoriasis. N Engl J Med. 1993;328(25):1812–1816. doi: 10.1056/NEJM199306243282504. [DOI] [PubMed] [Google Scholar]
- 37.Søyland E, et al. Dietary supplementation with very long-chain n-3 fatty acids in patients with atopic dermatitis. A double-blind, multicentre study. Br J Dermatol. 1994;130(6):757–764. doi: 10.1111/j.1365-2133.1994.tb03414.x. [DOI] [PubMed] [Google Scholar]
- 38.Thompson L, Cockayne A, Spiller RC. Inhibitory effect of polyunsaturated fatty acids on the growth of Helicobacter pylori: a possible explanation of the effect of diet on peptic ulceration. Gut. 1994;35(11):1557–1561. doi: 10.1136/gut.35.11.1557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Correia M, et al. Docosahexaenoic acid inhibits Helicobacter pylori growth in vitro and mice gastric mucosa colonization. PLoS ONE. 2012;7(4):e35072. doi: 10.1371/journal.pone.0035072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Park JM, Jeong M, Kim EH, Han YM, Kwon SH, Hahm KB. Omega-3 polyunsaturated fatty acids intake to regulate Helicobacter pylori-associated gastric diseases as nonantimicrobial dietary approach. Biomed Res Int. 2015;2015:712363. doi: 10.1155/2015/712363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hajishengallis G. The inflammophilic character of the periodontitis-associated microbiota. Mol Oral Microbiol. 2014;29(6):248–257. doi: 10.1111/omi.12065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661. doi: 10.1128/CMR.00134-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Branger J, et al. Role of Toll-like receptor 4 in gram-positive and gram-negative pneumonia in mice. Infect Immun. 2004;72(2):788–794. doi: 10.1128/IAI.72.2.788-794.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Song J, Bishop BL, Li G, Grady R, Stapleton A, Abraham SN. TLR4-mediated expulsion of bacteria from infected bladder epithelial cells. Proc Natl Acad Sci USA. 2009;106(35):14966–14971. doi: 10.1073/pnas.0900527106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Talbot S, et al. Toll-like receptor 4 signalling through MyD88 is essential to control Salmonella enterica serovar typhimurium infection, but not for the initiation of bacterial clearance. Immunology. 2009;128(4):472–483. doi: 10.1111/j.1365-2567.2009.03146.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Bohannon JK, et al. Treatment with TLR4 agonists protect against infection after severe burn injury. J Immunol. 2016;196(1_suppl):200.17 [Google Scholar]
- 47.Faure K, et al. TLR4 signaling is essential for survival in acute lung injury induced by virulent Pseudomonas aeruginosa secreting type III secretory toxins. Respir Res. 2004;5:1. doi: 10.1186/1465-9921-5-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Chassin C, et al. TLR4- and TLR2-mediated B cell responses control the clearance of the bacterial pathogen, Leptospira interrogans. J Immunol. 2009;183(4):2669–2677. doi: 10.4049/jimmunol.0900506. [DOI] [PubMed] [Google Scholar]
- 49.Andonegui G, et al. Mice that exclusively express TLR4 on endothelial cells can efficiently clear a lethal systemic Gram-negative bacterial infection. J Clin Invest. 2009;119(7):1921–1930. doi: 10.1172/JCI36411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Choudhury RH, Dunk CE, Lye SJ, Aplin JD, Harris LK, Jones RL. Extravillous trophoblast and endothelial cell crosstalk mediates leukocyte infiltration to the early remodeling decidual spiral arteriole wall. J Immunol. 2017;198(10):4115–4128. doi: 10.4049/jimmunol.1601175. [DOI] [PubMed] [Google Scholar]
- 51.Al-Soudi A, Kaaij MH, Tas SW. Endothelial cells: From innocent bystanders to active participants in immune responses. Autoimmun Rev. 2017;16(9):951–962. doi: 10.1016/j.autrev.2017.07.008. [DOI] [PubMed] [Google Scholar]
- 52.Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Sci Transl Med. 2014;6(237):237ra65. doi: 10.1126/scitranslmed.3008599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Cao B, Stout MJ, Lee I, Mysorekar IU. Placental microbiome and its role in preterm birth. Neoreviews. 2014;15(12):e537–e545. doi: 10.1542/neo.15-12-e537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Sun M, Zhou Z, Dong J, Zhang J, Xia Y, Shu R. Antibacterial and antibiofilm activities of docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA) against periodontopathic bacteria. Microb Pathog. 2016;99:196–203. doi: 10.1016/j.micpath.2016.08.025. [DOI] [PubMed] [Google Scholar]
- 55.Caron E, et al. Impact of fish oils on the outcomes of a mouse model of acute Pseudomonas aeruginosa pulmonary infection. Br J Nutr. 2015;113(2):191–199. doi: 10.1017/S0007114514003705. [DOI] [PubMed] [Google Scholar]
- 56.Honda KL, Lamon-Fava S, Matthan NR, Wu D, Lichtenstein AH. EPA and DHA exposure alters the inflammatory response but not the surface expression of Toll-like receptor 4 in macrophages. Lipids. 2014;50(2):121–129. doi: 10.1007/s11745-014-3971-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Svahn SL, et al. Dietary omega-3 fatty acids increase survival and decrease bacterial load in mice subjected to Staphylococcus aureus-induced sepsis. Infect Immun. 2016;84(4):1205–1213. doi: 10.1128/IAI.01391-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Sharma S, Chhibber S, Mohan H, Sharma S. Dietary supplementation with omega-3 polyunsaturated fatty acids ameliorates acute pneumonia induced by Klebsiella pneumoniae in BALB/c mice. Can J Microbiol. 2013;59(7):503–510. doi: 10.1139/cjm-2012-0521. [DOI] [PubMed] [Google Scholar]
- 59.Spite M, et al. Resolvin D2 is a potent regulator of leukocytes and controls microbial sepsis. Nature. 2009;461(7268):1287–1291. doi: 10.1038/nature08541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Chiang N, Dalli J, Colas RA, Serhan CN. Identification of resolvin D2 receptor mediating resolution of infections and organ protection. J Exp Med. 2015;212(8):1203–1217. doi: 10.1084/jem.20150225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Oh DY, et al. A Gpr120-selective agonist improves insulin resistance and chronic inflammation in obese mice. Nat Med. 2014;20(8):942–947. doi: 10.1038/nm.3614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Fujita T, Matsuoka T, Honda T, Kabashima K, Hirata T, Narumiya S. A GPR40 agonist GW9508 suppresses CCL5, CCL17, and CXCL10 induction in keratinocytes and attenuates cutaneous immune inflammation. J Invest Dermatol. 2011;131(8):1660–1667. doi: 10.1038/jid.2011.123. [DOI] [PubMed] [Google Scholar]
- 63.Sethi S, Ziouzenkova O, Ni H, Wagner DD, Plutzky J, Mayadas TN. Oxidized omega-3 fatty acids in fish oil inhibit leukocyte-endothelial interactions through activation of PPAR alpha. Blood. 2002;100(4):1340–1346. doi: 10.1182/blood-2002-01-0316. [DOI] [PubMed] [Google Scholar]
- 64.Calder PC. Long chain fatty acids and gene expression in inflammation and immunity. Curr Opin Clin Nutr Metab Care. 2013;16(4):425–433. doi: 10.1097/MCO.0b013e3283620616. [DOI] [PubMed] [Google Scholar]
- 65.Serhan CN, Chiang N, Van Dyke TE. Resolving inflammation: dual anti-inflammatory and pro-resolution lipid mediators. Nat Rev Immunol. 2008;8(5):349–361. doi: 10.1038/nri2294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Serhan CN. Pro-resolving lipid mediators are leads for resolution physiology. Nature. 2014;510(7503):92–101. doi: 10.1038/nature13479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Oh DY, et al. GPR120 is an omega-3 fatty acid receptor mediating potent anti-inflammatory and insulin-sensitizing effects. Cell. 2010;142(5):687–698. doi: 10.1016/j.cell.2010.07.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Endo J, Arita M. Cardioprotective mechanism of omega-3 polyunsaturated fatty acids. J Cardiol. 2016;67(1):22–27. doi: 10.1016/j.jjcc.2015.08.002. [DOI] [PubMed] [Google Scholar]
- 69.Jordao L, et al. Effects of omega-3 and -6 fatty acids on Mycobacterium tuberculosis in macrophages and in mice. Microbes Infect. 2008;10(12-13):1379–1386. doi: 10.1016/j.micinf.2008.08.004. [DOI] [PubMed] [Google Scholar]
- 70.Yan Y, et al. Omega-3 fatty acids prevent inflammation and metabolic disorder through inhibition of NLRP3 inflammasome activation. Immunity. 2013;38(6):1154–1163. doi: 10.1016/j.immuni.2013.05.015. [DOI] [PubMed] [Google Scholar]
- 71.Lin C, et al. Omega-3 fatty acids regulate NLRP3 inflammasome activation and prevent behavior deficits after traumatic brain injury. Exp Neurol. 2017;290:115–122. doi: 10.1016/j.expneurol.2017.01.005. [DOI] [PubMed] [Google Scholar]
- 72.Andrieu S, et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017;16(5):377–389. doi: 10.1016/S1474-4422(17)30040-6. [DOI] [PubMed] [Google Scholar]
- 73.Gapinski JP, VanRuiswyk JV, Heudebert GR, Schectman GS. Preventing restenosis with fish oils following coronary angioplasty. A meta-analysis. Arch Intern Med. 1993;153(13):1595–1601. [PubMed] [Google Scholar]
- 74.Morris MC, Sacks F, Rosner B. Does fish oil lower blood pressure? A meta-analysis of controlled trials. Circulation. 1993;88(2):523–533. doi: 10.1161/01.CIR.88.2.523. [DOI] [PubMed] [Google Scholar]
- 75.Nestel P, Shige H, Pomeroy S, Cehun M, Abbey M, Raederstorff D. The n-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid increase systemic arterial compliance in humans. Am J Clin Nutr. 2002;76(2):326–330. doi: 10.1093/ajcn/76.2.326. [DOI] [PubMed] [Google Scholar]
- 76.Glueck CJ, Khan N, Riaz M, Padda J, Khan Z, Wang P. Titrating lovaza from 4 to 8 to 12 grams/day in patients with primary hypertriglyceridemia who had triglyceride levels >500 mg/dl despite conventional triglyceride lowering therapy. Lipids Health Dis. 2012;11:143. doi: 10.1186/1476-511X-11-143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Vors C, et al. Inflammatory gene expression in whole blood cells after EPA vs. DHA supplementation: Results from the ComparED study. Atherosclerosis. 2017;257:116–122. doi: 10.1016/j.atherosclerosis.2017.01.025. [DOI] [PubMed] [Google Scholar]
- 78.Marsh PD. Are dental diseases examples of ecological catastrophes? Microbiology (Reading, Engl) 2003;149(Pt 2):279–294. doi: 10.1099/mic.0.26082-0. [DOI] [PubMed] [Google Scholar]
- 79.Han YW, et al. Interactions between periodontal bacteria and human oral epithelial cells: Fusobacterium nucleatum adheres to and invades epithelial cells. Infect Immun. 2000;68(6):3140–3146. doi: 10.1128/IAI.68.6.3140-3146.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Bui FQ, et al. Fusobacterium nucleatum infection of gingival epithelial cells leads to NLRP3 inflammasome-dependent secretion of IL-1β and the danger signals ASC and HMGB1. Cell Microbiol. 2016;18(7):970–981. doi: 10.1111/cmi.12560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Mendes RT, et al. Endothelial cell response to Fusobacterium nucleatum. Infect Immun. 2016;84(7):2141–2148. doi: 10.1128/IAI.01305-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Bashir A, Miskeen AY, Hazari YM, Asrafuzzaman S, Fazili KM. Fusobacterium nucleatum, inflammation, and immunity: the fire within human gut. Tumour Biol. 2016;37(3):2805–2810. doi: 10.1007/s13277-015-4724-0. [DOI] [PubMed] [Google Scholar]
- 83.Bourre JM. Dietary omega-3 fatty acids for women. Biomed Pharmacother. 2007;61(2-3):105–112. doi: 10.1016/j.biopha.2006.09.015. [DOI] [PubMed] [Google Scholar]
- 84.Gould JF, Smithers LG, Makrides M. The effect of maternal omega-3 (n-3) LCPUFA supplementation during pregnancy on early childhood cognitive and visual development: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. 2013;97(3):531–544. doi: 10.3945/ajcn.112.045781. [DOI] [PubMed] [Google Scholar]
- 85.Best KP, Gold M, Kennedy D, Martin J, Makrides M. Omega-3 long-chain PUFA intake during pregnancy and allergic disease outcomes in the offspring: a systematic review and meta-analysis of observational studies and randomized controlled trials. Am J Clin Nutr. 2016;103(1):128–143. doi: 10.3945/ajcn.115.111104. [DOI] [PubMed] [Google Scholar]
- 86.Han YW, Ikegami A, Bissada NF, Herbst M, Redline RW, Ashmead GG. Transmission of an uncultivated Bergeyella strain from the oral cavity to amniotic fluid in a case of preterm birth. J Clin Microbiol. 2006;44(4):1475–1483. doi: 10.1128/JCM.44.4.1475-1483.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Han YW. Laboratory maintenance of fusobacteria. Curr Protoc Microbiol. 2006;Chapter 13:Unit 13A.1. doi: 10.1002/9780471729259.mc13a01s00. [DOI] [PubMed] [Google Scholar]
- 88.Poltorak A, et al. Defective LPS signaling in C3H/HeJ and C57BL/10ScCr mice: mutations in Tlr4 gene. Science. 1998;282(5396):2085–2088. doi: 10.1126/science.282.5396.2085. [DOI] [PubMed] [Google Scholar]
- 89.Sodhi CP, et al. Intestinal epithelial Toll-like receptor 4 regulates goblet cell development and is required for necrotizing enterocolitis in mice. Gastroenterology. 2012;143(3):708–718.e5. doi: 10.1053/j.gastro.2012.05.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Jaffe EA, Nachman RL, Becker CG, Minick CR. Culture of human endothelial cells derived from umbilical veins. Identification by morphologic and immunologic criteria. J Clin Invest. 1973;52(11):2745–2756. doi: 10.1172/JCI107470. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.