

Abstract
The study aim was to classify youths into homogenous groups based on their symptoms of Alcohol Abuse and Dependence. An NIDA-funded cross-sectional survey was administered to 622 middle and high school students in San Juan, Puerto Rico in 2000. Latent class analysis (LCA) examined the Alcohol Abuse and Dependence symptoms. Three distinct classes of drinkers were found: low (86.0% of sample), moderate (11.7% of sample), and high (2.3% of sample) severity classes which were distinguished by differing estimated pr abilities of symptom reporting. The study has implications for the diagnosis of Alcohol Abuse and Dependence among Puerto Rican youths. Limitations are also noted.
Keywords: DSM, alcohol, abuse, dependence, adolescent, Puerto Rico, latent class analysis
Keywords: Manuel Diagnostique et Statistique des Troubles Mentaux (DSM), Abus, Dépendance, Adolescent, Porto Rico, Analyse de la structure latent
Keywords: Manual Diagnóstico y Estadístico de los Trastornos Mentales (DSM), Alcohol, Abuso, Dependencia, Adolescentes, Puerto Rico, LCA
RÉSUMÉ
La présente étude a pour objectif de classer les jeunes en groupes homogènes en fonction des symptômes d’abus d’alcool et de dépendance à l’alcool qu’ils présentent. Une enquête transversale financée par le NIDA a été menée en 2000 auprès de 622 élèves d’écoles intermédiates et secondaires de San Juan, Porto Rico. L’analyse de structure latente a examiné les symptômes d’abus d’alcool et de dépendance à l’alcool. Trois catégories de consommateurs ont été déterminées. Les catégories de gravité suivantes: limitée (86%), modérée (11,7%) et forte (2,3%) ont été déterminées en s’appuyant sur les estimations de probabilité de signalement des symptômes. La présente étude peut avoir des répercussions sur le diagnostic de l’abus d’alcool et de la dépendance à l’alcool chez les jeunes portoricains. Des limites ont également été signalées.
RESUMEN
El principal objetivo de este estudio es clasificar los jovenes en grupos homogenios de acuerdo a sus sintomas por abuso y dependencia del Alcohol. Este estudio transversal fue financiado por el NIDA y administrado a 622 estudiantes de los niveles primaria i secundaria de la ciudad de San Juan de Puerto Rico en el ano 2000. El estudio utilizado fue análisis de clases latentes (LCA) mediante el cual se examinan los sintomas del Abuso y Dependencia del Alcohol. En este estudio se encontro tres clases de bebedores: Bajos bebedores (86.0%), Moderados bebedores (11.7%), i Altos bebedores (2.3%). Estas clases de diferencias se clasifican en base a los sintomas reportados. Este estudio tiene implicaciones por el diagnostico del Abuso y Dependencia del Alcohol de los jovenes de San Juan de Puerto Rico.
INTRODUCTION
Adolescent alcohol use is a significant public health problem that has been associated with unintended/early pregnancy (Naimi, Lipscomb, Brewer, & Gilbert, 2003), HIV/AIDS infection (Grossman, Kaestner, & Markowitz, 2005), violence (Stafstrom, 2007), and traffic fatalities (Centers for Disease Control and Prevention, 2002; Traffic Safety Commission, 1999). Alcohol use among youths is prevalent in many territories worldwide, including the Commonwealth of Puerto Rico (Moscoso, Colon, Parrilla, & Reyes, 2003; Warner, Canino, & Colon, 2001), which is the focus of this study. This study set out to examine the reporting of alcohol problems among youths from Puerto Rico on the island.
The Commonwealth of Puerto Rico is an unincorporated territory/state governed by the United States (US). Puerto Ricans are citizens of the US, but are not allowed to vote for the president and do not have voting representation in the US House or Senate. Economically, Puerto Rico is poorer than the US with a mean per capita income of less than one third the average for the 50 US states (Malavet, 2004, p. 2). Culturally, Puerto Rico and the mainland US differ. Puerto Rican culture is a mix of Spanish and US culture, but Puerto Rico has its own unique culture, which is distinctly Latin American, and has its own separate national identity (Malavet, 2004, p. 106; Negron-Montaner, 2007, p. 1).
Alcohol use and alcohol laws also differ comparing Puerto Rico and the mainland US. The drinking age is 18 in Puerto Rico as opposed to 21 on the mainland US. Until relatively recently, there was little enforcement of existing alcohol drinking laws in Puerto Rico (Harwood, Bernat, Lenk, Vazquez, & Wagenaar, 2004). Some groups have succeeded in having alcohol ordinances created and enforced, suggesting a trend toward greater enforcement of alcohol-related policies in Puerto Rico (Harwood et al., 2004; Robert Wood Johnson Foundation, 1997). Also, Prohibition, enacted in 1917, was largely a failure in Puerto Rico as authorities were either unable or unwilling to enforce it (Pico, 2007, p. 25). It is also important to note that alcohol advertising is pervasive in Puerto Rico and that the alcohol industry is a large contributor to the Puerto Rican economy, through taxes and several alcohol production plants located there (Harwood et al., 2004; Puerto Rico Chamber of Commerce, 1994). Although US Federal laws and self-regulatory bodies govern alcohol advertising in Puerto Rico as well as in all other US states and territories, much of the regulatory power resides with each state or territory. Therefore, as on the mainland US, youths in Puerto Rico are exposed to alcohol advertisements.
In general, Puerto Rico has a culture that is permissive of alcohol use (Harwood et al, 2004; Robert Wood Johnson Foundation, 1997). It has been reported that Puerto Rican youths on the island have access to alcohol at special events and that adults provide the alcohol (Harwood et al., 2004; Robert Wood Johnson Foundation, 1997). It has also been suggested that social drinking may be more normative for Puerto Ricans of all ages and that because of this drinking it may be less likely to actually cause problems for the drinker compared to the mainland US where drinking is frowned upon for youths (Warner et al., 2001).
Examining the prevalence of alcohol use in Puerto Rico compared to other territories, in general, rates of alcohol use are generally lower on the island of Puerto Rico compared to the mainland US general population (the Centers for Disease Control and Prevention [CDC], 2008; Warner et al., 2001). The Youth Risk Behavior Surveillance System (YRBSS) funded by the CDC reported in 2005 that among youths in grades 9–12 the prevalence of lifetime alcohol use was 67.0% among Puerto Rican youths on the island and 74.3% among youths on the mainland US (CDC, 2008). One study found that compared to mainland US youths, more Puerto Rican youths on the island report symptoms of alcohol dependence without having a diagnosis (36.2% vs. 20.0%) and meeting the criteria for alcohol abuse (16.0% vs. 10.5%) (Warner et al., 2001). In addition, Puerto Rico has a lower alcohol use prevalence than many European nations that have some of the highest prevalences of alcohol use in the world (Grube, 2005). For example, the prevalence of drinking in the past 30 days for youths was 32.9% in Puerto Rico (Moscoso et al., 2003), 35% in the US (Grube, 2005), 82% in Austria (Grube, 2005), and 74% in the UK (Grube, 2005). However, in comparison to some of its neighboring Caribbean territories, the message is less clear. The lifetime prevalence of alcohol use among youths aged 15–19 in Puerto Rico (76.2%) is higher than in the Dominican Republic (66.3%; Jernigan, 2001). However, for 13–14-year olds (looking at this age group for comparability between territories), the lifetime prevalence is lower in Puerto Rico (42.5%–57.9%; Moscoso et al., 2003) compared to Jamaica (71.2%; Jernigan, 2001). This suggests differences between Puerto Rican youths on the island and youths from the mainland US and in other places, in terms of alcohol use and expression of alcohol problems. There are likely many reasons why alcohol use differs across cultures, including economy (a country’s gross domestic product and alcohol use are positively associated), acceptability, and permissiveness of alcohol use in the culture, laws or policies governing the sale of alcohol to youths, and advertising and promotion of alcohol use directed at youths (Jernigan, 2001; Plant et al., 2010).
The rationale for conducting the current study centers around two ideas. First, despite the breadth of the problem, there has been little research on Alcohol Abuse and Dependence among Puerto Rican youth on the island. Second, there is heterogeneity and variations in the reporting of Alcohol Abuse and Dependence symptoms, which may affect the diagnosis, treatment, and prognosis of Puerto Rican youths with alcohol problems.
First, there has been relatively little research focusing on alcohol consumption-related problems in Puerto Rican youths on the island. The Consulta Juvenil, a prominent population-based probability survey of Puerto Rican youths that has collected data on adolescent substance use for many years (Moscoso, Parrilla, Robles, Colon, & Garcia, 1998; Robles, Moscoso, Colon, Garcia, & Parrilla, 1995; Robles, Moscoso, Colon, Garcia, & Rebollo, 1991; Robles et al., 1994), recently found that the prevalence of lifetime alcohol use ranged from 30.4% for 12-year olds to 81.7% for 17-year olds (Moscoso et al., 2003). Although some studies exist (Colon, Robles, Canino, & Sahai, 2001; Robles, Martinez, & Moscoso, 1979; Warner et al., 2001), there have been relatively few recent studies examining alcohol consumption-related problems among Puerto Rican adolescents (Colon et al., 2001; Jackson-Moya, 2000; Warner et al., 2001). The Consulta Juvenil and the CDC’s YRBSS do not report symptoms or disorders related to alcohol use in youths. One study (Warner et al., 2001) estimated that 6.4% of Puerto Rican youths between 15 and 18 years old met a diagnosis of Alcohol Abuse or Dependence in their lifetime, as defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) (American Psychiatric Association, 2000). Another study by Jackson-Moya (2000) found that among 15–21-year olds, 10.2% had Alcohol Abuse or Dependence in their lifetimes and 6.7% manifested Alcohol Abuse or Dependence in the past year. Although estimates of Alcohol Abuse and Dependence among Puerto Rican youths differ depending on the study, studies consistently show that a sizable number of Puerto Rican youths exhibit problems with their alcohol use.
Second, there is heterogeneity and variations in the reporting of Alcohol Abuse and Dependence symptoms, which may affect the diagnosis, treatment, and prognosis of youths with alcohol consumption-related problems. Extant studies have also reported variations in Alcohol Abuse and Dependence symptom reporting. Warner and colleagues (Warner et al., 2001) found that several Dependence symptoms were highly prevalent among alcohol using Puerto Rican youths (tolerance [35%], desire or efforts to cut down on drinking [33%], and used more than intended [20.3%], while some abuse symptoms had a very low prevalence, legal problems [0.4%]). Furthermore, more Puerto Rican youths on the island reported symptoms of Alcohol Dependence without having a diagnosis (36.2%) compared to youths on the US mainland (20.0%) (Warner et al., 2001). This underscores the significant heterogeneity in alcohol consumption-related symptom reporting among youths.
In addition, Kuo, Aggen, Prescott, Kendler and Neale (2008) suggest that those meeting the criteria for a diagnosis of Alcohol Abuse or Dependence may be quite heterogenous. This is because in order to meet the DSM criteria for a diagnosis, one must report any one of four Abuse symptoms or any three of seven Dependence symptoms. Those reporting different combinations of these symptoms could be quite different. Indeed, studies have found that youths with Alcohol Abuse are heterogenous (Martin & Winters, 1998). Furthermore, this heterogeneity and variation within categories may be problematic for treatment and prevention efforts and in predicting prognosis (Kuo et al., 2008). Therefore, defining more homogenous groups of youths with alcohol consumption-related problems is an important research goal (Kuo et al., 2008).
Latent class analysis (LCA) is a type of cluster analysis that allows for the empirical classification of individuals with similar symptom profiles (McCutcheon, 1987). LCA assumes that there are distinct subgroups or classes of individuals in the population that are characterized by their pattern of symptoms. LCA has been applied to the examination of patterns of alcohol consumption-related symptom reporting in several studies (Bucholz, Heath, Reich, & Hesselbrock, 1996; Chung & Martin, 2001; Kuo et al., 2008; Moss, Chen, & Yi, 2008). One of these studies found three classes of alcohol consumption-related problems (asymptomatic, mild, and severe) in a clinical sample of adolescents from the US (Chung & Martin, 2001). Another LCA of drinking behaviors and alcohol consumption-related problems found three classes of underage US drinkers (nonproblem drinkers, risky problem drinkers, and regular problem drinkers). These studies and others highlight one hallmark benefit of LCA, which is empirically classifying individuals into more homogenous groups. Furthermore, classifying youths into more homogenous groups based on their alcohol consumption-related problems may lead to a more accurate diagnosis, a more precise determination of their prognosis, and ultimately, to a better, more targeted treatment.
The study aims were to: (1) empirically examine the profile of reported Alcohol Abuse and Dependence symptoms among Puerto Rican adolescents and classify them into distinct groups accordingly, (2) examine the classes with respect to demographic characteristics, such as gender and age, and (3) examine the validity of the classes with respect to a set of criterion variables. The criterion variables were chosen for a number of reasons: (1) they were closely associated with alcohol consumption-related problems, for example alcohol use and DSM-IV-TR-defined Alcohol Use Disorders, (2) they were associated with problem behavior theory (Jessor, 1987; Jessor & Jessor, 1977), which states that youths who use alcohol are more likely to engage in other problem behaviors, such as problem drinking, illicit drug use, sexual behavior, and antisocial behavior, or (3) they were associated with risky behaviors that have been shown to predict poor outcomes, such as driving while intoxicated, riding with drivers who drink, and lack of condom use.
METHODS
Participants and Procedure
The International Longitudinal Survey of Adolescent Health (Latimer, Floyd et al., 2004; Latimer, O’Brien et al., 2004; Latimer et al., 2006) was administered to students attending one middle school (grades seven through nine) and one high school (grades 10 through 12) in a community in San luan, Puerto Rico in the spring of 2000. This confidential survey was designed to assess risk and protective factors1 associated with drug use, sexual behavior, psychiatric problems, and school achievement. All students registered for school were invited to participate, less than 1% of the parents or the students refused to participate, and 11% were absent on the day of the survey. The survey was completed by 989 students with a survey response rate of 88%. Of those who completed the survey, 5.6% (N = 55) were excluded from the analyses because they reported use of a fictitious drug item or had an inconsistent pattern of responses throughout the survey. For the present analysis, those who reported no alcohol use in their lifetime (N = 312, 31.5%) were excluded. The analysis was conducted on the remaining 622 lifetime alcohol users.
For more detail on the development of the survey using forward and backward translation into Spanish, survey administration, and the selection of schools, see the papers by Latimer, O’Brien and colleagues (2004) and Latimer and colleagues (2006). Briefly, one city was randomly selected from among the five largest cities in Puerto Rico and one school system was randomly selected from among the five largest school systems in that selected city. In addition, the survey procedures were adapted from Monitoring the Future Study (O’Malley, Johnston, Bachman, & Schulenberg, 2000), a large school-based confidential survey conducted in the US. All participating students signed study assent forms. Parents provided passive consent for their child’s participation in the study. Parents were sent two letters describing the study and the study procedures and were given multiple methods for withdrawing their child from the study. The University of Minnesota Review Board reviewed and approved the survey and methods, along with the Superintendent of the school system and an ad hoc review board (including the principal, teachers, and parents) formed at each school.
Measures
The items used in this survey were derived mainly from the Adolescent Diagnostic Interview (ADI) (Winters & Henly, 1993) and the Personal Experience Inventory (PEI) (Winters & Henly, 1989). The ADI has also shown moderate to high reliability and validity and has been extensively used in the US (Winters & Henly, 1993; Winters et al., 1999). The PEI has shown good psychometric properties and has been widely used in school and clinic settings in the US (Winters & Henly, 1989; Winters et al., 1999). The survey was originally developed in English but was forward and backward translated into Spanish (Latimer, O’Brien et al., 2004; Latimer et al., 2006).
Alcohol Abuse and Dependence Symptoms
Twenty-one items asked participants about the frequency of problems related to alcohol use that they experienced in the past year. The response choices were “never,” “one time,” or “two or more times.” The items were dichotomized into “never” versus “one or more times” for this analysis. There were 11 items that addressed DSM-IV Alcohol Abuse symptoms and 10 items that addressed DSM-IV Alcohol Dependence symptoms (American Psychiatric Association, 2000). These items were derived from the ADI (Winters & Henly, 1993). An example of one of the items addressing Abuse is: “During the past 12 months, have you skipped school because of alcohol use?” The 11 Abuse items were collapsed into four variables corresponding to the four DSM-IV-TR Alcohol Abuse criteria, while the 10 Dependence items were collapsed into six variables corresponding to six (out of the seven) DSM-IV-TR Alcohol Dependence criteria. There was no item corresponding to tolerance, a Dependence criterion.
Criterion Variables for Class Validation
Several criterion variables were chosen in order to examine the validity of the classes. We tried to address multiple forms of validity of the classes. DSM-IV-TR Alcohol Abuse and Dependence was chosen to represent the gold standard of diagnosis and thus aid in determining criterion-related validity. Alcohol use and regular alcohol use were chosen to represent measures with which the alcohol problem classes should correlate and thus get at convergent construct validity. Additional variables were selected to get at the external nomological validity of the classes, variables that should be externally related to the classes. These included variables relating to problem behavior theory (Jessor, 1987; Jessor & Jessor, 1977), such as marijuana use, sexual intercourse, fighting, being sent to the principal, having been arrested/had law trouble and risky behavior variables, such as condom use, drinking and driving, and riding with a driver who had been drinking. All items were adapted from the PEI (Winters & Henly, 1989), except for the Abuse and Dependence and fighting items which were derived from the ADI (Winters & Henly, 1993).
DSM-IV-TR Alcohol Abuse and Dependence.
Alcohol Abuse and Dependence diagnoses were created following the DSM-IV-TR using items derived from the ADI (which has been previously described) (Winters & Henly, 1993). Specifically, the DSM-IV-TR defines Alcohol Dependence as a maladaptive pattern of alcohol use, leading to clinically significant impairment, as manifested by three (or more) of seven criteria in the same 12-month period: tolerance, withdrawal, using larger amounts or over a longer period than intended, desire to or unsuccessful efforts to cut down on use, a great deal of time is spent trying to obtain, use, or recover from the effects of alcohol, important social, occupational, or recreational activities are given up or reduced because of use, and use is continued despite having a physical or psychological problem caused by or exacerbated by alcohol use (American Psychiatric Association, 2000). If one does not meet criteria for Alcohol Dependence, a diagnosis of Abuse is then possible. Alcohol Abuse is defined as a maladaptive pattern of recurrent alcohol use leading to clinically significant impairment, as manifested by one (or more) of four criteria in the same 12-month period: a failure to fulhll major role obligations at work, school, or home, recurrent use in physically hazardous situations, recurrent alcohol-related legal problems, and continued use despite having social or interpersonal problems caused or exacerbated by use.
Alcohol Use Frequency.
Three items inquired about the participant’s frequency of alcohol use. Two items asked how many times the respondent used alcohol in the past 12 months and the past three months by selecting from seven response choices, ranging from never to 40 or more times. For this analysis, past 12-month alcohol use was trichotomized into never, one to nine times, and 10 or more times. Past three-month alcohol use was dichotomized into never versus one or more times. A third item asked participants if they had ever used alcohol regularly for at least one month (yes vs. no).
Lifetime Marijuana Use.
One item asked participants to report how many times they used marijuana or hashish in their lifetime. This item was recoded from never to 40 or more times into never versus one or more times.
Ever Had Sex.
Another item asked participants if they had ever had sexual intercourse in their lifetime (yes or no).
Started Fights.
One item asked participants how many times in the past 12 months they had started physical fights with other kids (never, one, two, or more times). This item was dichotomized into never versus one or more times for this analysis. This item was derived from the Conduct Disorder scale of the ADI (Winters & Henly, 1993).
Sent to the Principal.
One item asked participants if they had been sent to the principal in the past 12 months (yes or no).
Arrested/Law Trouble.
One item asked respondents if they had been arrested or had trouble with the law in the past 12 months (yes or no).
Risky Behaviors.
Three items assessed participants’ risky behaviors. One item asked participants if they used a condom the last time they had sex (haven’t had sex, yes or no). Another item asked participants, would you feel it was okay for you to drive after one, two, three, or more drinks, or I wouldn’t drive after drinking any alcohol. This item was dichotomized into, would feel it was okay to drive after (any) drinking versus would not feel it was okay to drive after (any) drinking. Another item inquired about how often a participant rides with a driver who had been drinking alcohol or taking drugs. This item was recoded into rarely/never versus often/sometimes.
Statistical Analysis
LCA was used to examine the underlying structure of Alcohol Abuse and Dependence symptom reporting among Puerto Rican youths. LCA is a statistical method used with binary (yes/no) items for the purpose of identifying a small number of subgroups or classes of persons who report similar patterns of responses. LCA captures the heterogeneity associated with unobserved (or latent) subpopulations by classifying individuals based on their pattern of responses (McCutcheon, 1987; Whitesell et al, 2006). The main assumption of LCA is that the underlying class structure accounts for the co-occurrence of symptom reporting (Reboussin, Song, Shrestha, Lohman, & Wolfson, 2006). In a statistical sense, the symptom variables (indicators) are independent conditional on the class (Lazarsfeld & Henry, 1968; McCutcheon, 1987; Reboussin et al., 2006). In a practical sense, any association between the reported symptoms is explained by the class membership. The assumption that results allows for homogenous and distinct classes such that within each class the symptom reporting patterns differ only by random error (McCutcheon, 1987; Reboussin et al., 2006).
A series of LCA models were fit to the data. LCA was applied to the 10 Abuse and Dependence criteria variables beginning with a one-class model and increasing the number of classes to determine the best-fitting model with the most parsimony. Mplus version five was used for the LCA modeling (Muthén & Muthén, 2007). To determine the best-fitting model with the most parsimony, multiple fit statistics were used, such as the Bayesian Information Criteria (BIC) (Schwartz, 1978), the sample size-adjusted BIC (ABIC) (Sclove, 1987), the Akaike Information Criteria (AIC) (Akaike, 1987), the parametric bootstrap likelihood ratio test (BLRT) (McLachlan & Peel, 2000) and the Lo–Mendell–Rubin adjusted likelihood ratio test (LMR) (Lo, Mendell, & Rubin, 2001). Although there is no consensus in the statistics community as to which fit statistic should be valued most over another to decide on the number of classes, a simulation study by Nylund, Asparouhov and Muthén (2007) suggests that the BIC and ABIC accurately determine the number of classes in LCA. In addition, the meaningfulness of the solution in terms of the clinical or theoretical interpretation was also considered, as is standard in many LCA studies.
After determining the appropriate number of classes that best fit the data, we sought to examine the validity of the classes by examining the association between class membership and criterion variables. Because latent class regression was not appropriate due to the low cell sizes, most likely resulting from a low sample size in the high-severity class, another method was used to examine the association between class membership and the criterion variables. The AUXILIARY (e) option in Mplus was used to examine these relationships. This method allows for the testing of the equality of the means of the criterion variables across latent classes. This method uses posterior probability-based multiple imputations that account for the error in the latent class membership (Muthén & Muthén, 2007). The result is a chi-square statistic with the p-value determining whether two classes differ in terms of the mean of the criterion variable of interest. Strictly for the purposes of displaying the associations, the assigned most likely latent classes were exported and tabulated against the criterion variables.
RESULTS
The sample demographics are presented in Table 1. The youths ranged in age from 11 to 19 years old [mean (standard deviation) = 15.2 (1.6))], were predominately Hispanic (95.3%), and mostly female (58.4%; see Table 1). More than half (N = 387, 62.2%) were in grades 10, 11, or 12, while 235 (37.8%) were in grades 7, 8, or 9. The prevalence of Alcohol Abuse and Dependence symptoms in the sample reporting lifetime alcohol use is presented in Table 2. The most prevalent symptoms were used more than intended (12.5%, a Dependence item) and social problems (10.6%, an Abuse item). The least prevalent symptom was having legal problems caused by alcohol use (1.1%, an Abuse item).
TABLE 1.
Selected characteristics of 622-school-based-youth drinkers in Puerto Rico
| Characteristics | No. (N = 622) | % |
|---|---|---|
| Gender | ||
| Female | 363 | 58.4 |
| Male | 259 | 41.6 |
| Age, mean (SD) | 15.2 (1.6) | |
| 11–14 years | 195 | 31.4 |
| 15–19 years | 427 | 68.7 |
| Ethnicity | ||
| Hispanic | 593 | 95.3 |
| Other | 29 | 4.7 |
| School | ||
| Middle school | 235 | 37.8 |
| High school | 387 | 62.2 |
TABLE 2.
Prevalence of Alcohol Abuse and Dependence symptoms among adolescent drinkers in Puerto Rico
| Total |
|||
|---|---|---|---|
| Symptom description | AUD criteria | N | % |
| Failure to fulfill role | A1 | 28 | 4.5 |
| Use in hazardous situations | A2 | 51 | 8.2 |
| Legal problems | A3 | 7 | 1.1 |
| Social problems | A4 | 66 | 10.6 |
| Withdrawal | D2 | 27 | 4.3 |
| Used more than intended | D3 | 78 | 12.5 |
| Unable to cut down | D4 | 56 | 9.0 |
| A lot of time spent drinking | D5 | 48 | 7.7 |
| Activities given up | D6 | 18 | 2.9 |
| Use despite physical or psychological problems | D7 | 19 | 3.1 |
The fit statistics that were used to help in determining the appropriate number of classes for the LCA are presented in Table 3. The BIC and ABIC suggested a three-class solution. Both the LMR and BLRT suggested that the three-class model was better than the two-class model. The best log-likelihood value was not replicated in the four-, five-, and six-class models suggesting that a local maximum may have been reached and that those solutions may not be trustworthy. Entropy is a measure used to quantify how well the model has classified individuals. It is measured on a scale from 0 to 1.0 with 1.0 being perfect classification. The entropy for the three-class solution was 0.94 suggesting very good classification. In addition, examination of the three-class solution suggested that it was clinically interpretable and a likely solution. A three-class solution was deemed most appropriate for the data.
TABLE 3.
Fit statistics for an LCA of alcohol symptoms among adolescent drinkers in Puerto Ricoa
| Class | LL | AIC | BIC | ABIC | LMR | BLRT |
|---|---|---|---|---|---|---|
| 1 | −1409.103 | 2838.207 | 2882.536 | 2850.788 | NA | NA |
| 2 | −1035.242 | 2112.484 | 2205.576 | 2138.904 | <0.001 | <0.001 |
| 3 | −985.972 | 2035.944 | 2177.798 | 2076.203 | 0.0148 | <0.001 |
| 4 | −970.204 | 2026.409 | 2217.025 | 2080.507 | 0.0367 | – |
| 5 | −953.848 | 2015.696 | 2255.075 | 2083.634 | 0.0225 | – |
| 6 | −943.526 | 2017.052 | 2305.193 | 2098.828 | 0.0229 | – |
LL; Log-likelihood value. AIC; Akaike Information Criteria. BIC; Bayesian Information Criteria. BLRT; parametric bootstrap likelihood ratio test. LMR; Lo–Mendell–Rubin adjusted likelihood ratio test. For the four, five, and six class solutions the best log-likelihood values were not replicated suggesting that those solutions may be untrustworthy and that a local maximum may have been reached. The BLRT p-value for the four, five, and six class solutions were also untrustworthy.
Examination of the three classes showed that these were characterized by the number of symptoms endorsed and the estimated probability of endorsing each symptom in the classes. Figure 1 presents the three-class solution for the LCA, the estimated probabilities of symptom endorsement for each class. The first class, which we will name the low-severity class, was the largest class with an estimated prevalence of 86.0% in the sample (see Table 4). The low-severity class was essentially an asymptomatic class that endorsed very few symptoms. In the low-severity class, an estimated 5.2% reported used more than intended (the highest prevalence symptom reported in that class). Class two, which we name the moderate severity class consisted of 11.7% of the sample. The moderate severity class had moderately high estimated probabilities of reporting several symptoms, including used more than intended (56.7%), use in hazardous situations (50.8%), social problems (47.8%), unable to cut down (47.0%), and a lot of time spent drinking (42.0%, see Figure 1 and Table 4). Class three, which we term the high-severity class, was the lowest prevalence class consisting of 2.3% of the sample. The high-severity class was characterized by high estimated probabilities of almost all symptoms, but only moderately high estimated prevalences of having had legal problems due to alcohol use (45.3%) and used more than intended (48.1%). The moderate and high-severity classes were approximately parallel in the sense that the high-severity class represented those with a higher estimated probability of reporting symptoms compared to the moderate class. However, the moderate and high-severity classes had similar estimated probabilities for used more than intended (56.7% and 48.1%, respectively). Additionally, the moderate severity class had low estimated prevalences for activities given up (6.4%) and use despite physical or psychological problems (10.7%) whereas the high-severity class had high estimated prevalences of these symptoms (91.9% and 80.7%, respectively).
FIGURE 1.
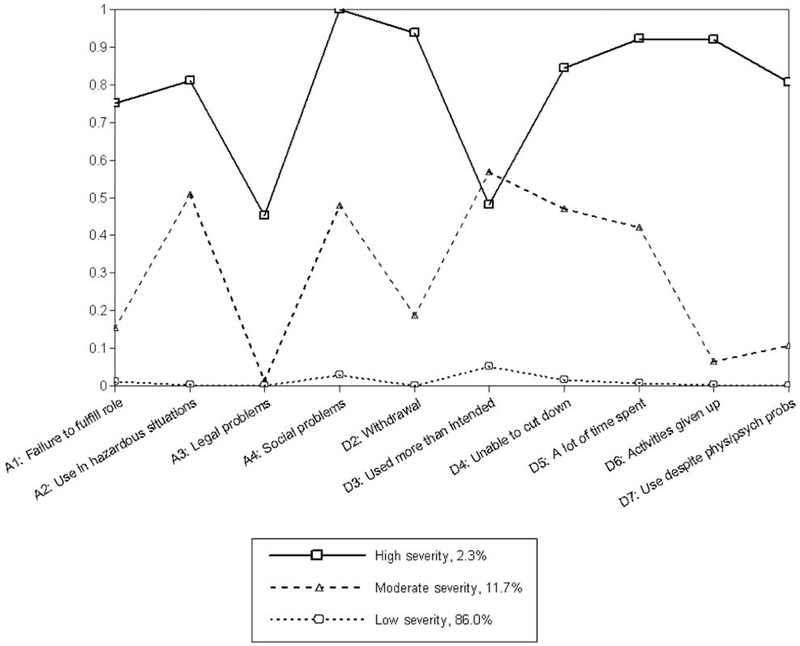
Final three-class solution of an LCA of Alcohol Abuse and Dependence symptoms among adolescent drinkers in Puerto Rico.
TABLE 4.
Estimated probabilities of Alcohol Abuse and Dependence symptoms by classes and estimated prevalence of three classes of adolescent drinkers in Puerto Ricoa
| Symptom | Class 1 Low (86.0%) | Class 2 Moderate (11.7%) | Class 3 High (2.3%) | |||
|---|---|---|---|---|---|---|
| A1: Failure to fulfill role | 1.2 | (0.2–2.1) | 15.3 | (6.6–24.1) | 75.1 | (34.9–100) |
| A2: Use in hazardous situations | 0.2 | (0.0–0.9) | 50.8 | (36.6–65.1) | 81.0 | (53.8–100) |
| A3: Legal problems | 0.0 | (0.0–0.0) | 1.3 | (0.0–3.8) | 45.3 | (9.9–80.7) |
| A4: Social problems | 3.0 | (1.4–4.5) | 47.8 | (33.7–61.8) | 100.0 | (100.0–100.0) |
| D2: Withdrawal | 0.0 | (0.0–0.0) | 18.8 | (7.9–29.7) | 93.8 | (76.8–100.0) |
| D3: Used more than intended | 5.2 | (3.0–7.4) | 56.7 | (44.3–69.2) | 48.1 | (13.9–82.2) |
| D4: Unable to cut down | 1.6 | (0.2–3.0) | 47.0 | (33.2–60.7) | 84.5 | (62.4–100.0) |
| D5: A lot of time spent drinking | 0.6 | (0.0–1.4) | 42.0 | (27.5–56.6) | 92.1 | (75.9–100.0) |
| D6: Activities given up | 0.2 | (0.0–0.5) | 6.4 | (0.0–14.1) | 91.9 | (75.3–100.0) |
| D7: Use despite physical or psychological problems | 0.0 | (0.0–0.0) | 10.7 | (3.3–18.2) | 80.7 | (46.3–100.0) |
Estimated probabilities and 95% confidence intervals are conditional on most likely class membership; estimated prevalence of most likely latent class in the total sample.
After examining the latent class structure of Puerto Rican adolescent drinkers, we sought to examine the validity of the classes with respect to demographic characteristics and other criterion variables. The bivariate associations of most likely class membership and demographic characteristics and criterion variables are presented in Table 5.
TABLE 5.
Association between latent class membership and characteristics of adolescent drinkers in Puerto Rico
| Class 1 Low severity 535 (86.0) |
Class 2 Moderate severity 73 (11.7) |
Class 3 High severity 14 (2.3) |
|
|---|---|---|---|
| Age, continuous, mean (SD) | 15.1 (1.6)a | 15.7 (1.3)b | 15.4 (1.6)ab |
| Gender | |||
| Male | 214 (40.0) | 38 (52.0) | 7 (50.0) |
| Female | 321 (60.0)a | 35 (48.0)a | 7 (50.0)a |
| DSM-IV alcohol use disorder, past year | |||
| No diagnosis | 473 (88.4) | 0 (0.0) | 0 (0.0) |
| Subthreshold | 40 (7.5) | 15 (20.6) | 0 (0.0) |
| Abuse | 22 (4.1) | 38 (52.0) | 0 (0.0) |
| Dependence | 0 (0.0)a | 20 (27.4)b | 14 (100.0)c |
| Alcohol use, past year | |||
| 0 Times | 136 (25.4) | 0 (0.0) | 0 (0.0) |
| 1–9 Times | 339 (63.4) | 40 (54.8) | 6 (42.9) |
| 10+ Times | 60 (11.2)a | 33 (45.2)b | 8 (57.1)b |
| Alcohol use, past 3 months | |||
| No | 229 (42.8) | 3 (4.1) | 4 (28.6) |
| Yes | 306 (57.2)a | 70 (95.9)b | 10 (71.4)ab |
| Ever used alcohol regularly for at least one month | |||
| No | 417 (84.9) | 41 (59.4) | 4 (28.6) |
| Yes | 74 (15.1)a | 28 (40.6)b | 10 (71.4)c |
| Ever used marijuana/hashish | |||
| No | 466 (87.1) | 45 (61.6) | 1 (7.1) |
| Yes | 69 (12.9)a | 28 (38.4)b | 13 (92.9)c |
| Ever had sex | |||
| No | 345 (71.0) | 24 (40.7) | 2 (14.3) |
| Yes | 141 (29.0)a | 35 (59.3)b | 12 (85.7)c |
| Started fights, past year | |||
| No | 381 (78.4) | 31 (52.5) | 9 (64.3) |
| Yes | 105 (21.6)a | 28 (47.5)b | 5 (35.7)ab |
| Sent to the principal, past year | |||
| No | 410 (82.2) | 49 (71.0) | 7 (53.9) |
| Yes | 89 (17.8)a | 20 (29.0)ab | 6 (46.2)b |
| Arrested/law trouble, past year | |||
| No | 488 (97.6) | 60 (87.0) | 10 (76.9) |
| Yes | 12 (2.4)a | 9 (13.0)b | 3 (23.1)ab |
| Would drive after drinking | |||
| No | 324 (66.7) | 31 (52.5) | 2 (14.3) |
| Yes | 162 (33.3)a | 28 (47.5)b | 12 (85.7)c |
| How often do you ride with a driver who has been drinking? | |||
| Rarely/Never | 421 (86.6) | 42 (71.2) | 5 (35.7) |
| Often/Sometimes | 65 (13.4)a | 17 (28.8)b | 9 (64.3)c |
| Used a condom last time you had sex | |||
| Never Had Sex | 345 (71.1) | 24 (40.7) | 2 (14.3) |
| Used a Condom | 49 (10.1) | 13 (22.0) | 2 (14.3) |
| Did Not Use a Condom | 91 (18.8)a | 22 (37.3)b | 10 (71.4)c |
The equality of means for each variable was examined across latent classes using posterior probability-based multiple imputations. Categories that share superscripts refer to comparisons that are not statistically different, such as 15.1 (1.6)a and 15.7 (1.3)b. Categories that do not share superscripts refer to statistically significant differences at P < 0.05, such as 15.7 (1.3)b and 15.4 (1.6)ab. For all hypothesis tests, the alpha was set at 0.05. For the purposes of display, the assigned most likely latent classes were cross-tabulated against the demographic and criterion variables.
Each of the classes showed distinctiveness from one another on several other variables, as explained below. The low and moderate severity classes were significantly different with respect to all variables (except for gender and having been sent to the principal in the past 12 months), including age, DSM-IV-TR Alcohol Use Disorder, past 12 months and past three months alcohol use, having used alcohol regularly for at least a month, lifetime marijuana use, ever had sex, past 12 months fighting, having been arrested/had law trouble in the past 12 months, would drive after drinking, how often they rode with a driver who had been drinking, and used a condom the last time they had sex (see Table 5). In addition, the low- and high-severity classes were significantly different with respect to all variables except age, gender, past three months alcohol use, past 12 months fighting, and having been arrested/had law trouble in the past 12 months. Finally, the moderate and high classes were significantly different with respect to DSM-IV-TR Alcohol Use Disorder, having used alcohol regularly for at least a month, lifetime marijuana use, ever had sex, would drive after drinking, how often they rode with a driver who had been drinking, and used a condom the last time they had sex.
DISCUSSION
This study examined the patterns of Alcohol Abuse and Dependence symptom reporting among a sample of adolescent drinkers from two schools in Puerto Rico. The study found three classes of drinkers: a low-severity class that reported few symptoms, a moderate severity class that had moderately high probabilities of reporting many symptoms, and a high-severity class that had high probabilities of reporting many symptoms. The classes showed good validity in that they were distinct from one another with respect to several other variables that are associated with alcohol use and alcohol consumption-related problems among youths.
This study is novel in that no studies that we are aware of utilized LCA to classify Puerto Rican youths according to their alcohol consumption-related problems. Therefore, comparison to other studies is difficult. Warner and colleagues (2001) found that the highest prevalence alcohol symptoms endorsed by Puerto Rican youths in the general population were tolerance, desire/efforts to cut down (unable to cut down), and used more than intended. In this study, alcohol users reported high prevalences of used more than intended and social problems due to alcohol use; however, this study reported much lower prevalences compared to the study by Warner. Several methodological differences may account for the differences between these studies.
It is interesting to note that in this study no class of youth reported a pattern of behavior consistent with reporting only Abuse symptoms. Although 4.1% of youths in the low-severity class and 52.0% in the moderate severity group met criteria for Alcohol Abuse, no group endorsed solely Abuse items and the moderate severity group endorsed Abuse and Dependence symptoms alike. Importantly, 7.5% of those in the moderate severity group and 20.6% of those in the high-severity group endorsed symptoms but did not meet criteria for Abuse or Dependence. These so-called “diagnostic orphans” are reporting alcohol consumption-related problems but falling through the cracks of the diagnostic system (Pollock & Martin, 1999). This is especially a problem because more Puerto Rican youths compared to US youths on the mainland report Dependence symptoms without meeting the criteria for a Dependence diagnosis (Warner et al, 2001). Other studies in adults suggest that this pattern of reporting is not specific to Puerto Rico and that in the US, Mexico, Argentina, and Poland, Alcohol Abuse and Dependence symptoms form a single unidimensional construct and Abuse and Dependence symptoms generally hang together (Borges et al., 2010). Taken together, this evidence suggests that these results are consistent with the results of other studies on adolescents from Puerto Rico and other places. Also interesting was that 27.4% in the moderate severity class and 100% of the youths in the high-severity class met criteria for Dependence. Although we did not specifically examine those youths reporting only Dependence items, the bivariate results suggest that youths in the moderate severity class were distinct from those in the high-severity class. This may mean that the number of symptoms reported may be more indicative of alcohol problem severity for Puerto Rican adolescents than the type of symptom reported (i.e., whether it is an Abuse or a Dependence item). This is actually consistent with a growing body of research questioning the diagnostic validity of the DSM-defined Substance Use Disorders, especially the Abuse category (Borges et al., 2010; Harrison, Fulkerson, & Beebe, 1998; Hasin et al., 2003).
Study’s Limitations
The present study had some noteworthy limitations. First, this study did not include a measure of tolerance which studies have shown is a highly prevalent symptom of Alcohol Dependence in Puerto Rican and US youths (Martin & Winters, 1998; Warner et al., 2001). The inclusion of this symptom would likely have altered our interpretations. In an effort to understand the degree to which children in the two schools sampled were representative of children throughout Puerto Rico, we examined family income variations throughout the country. Data from the 2005–2009 American Community Survey showed that approximately half of the households in Puerto Rico had annual incomes ranging from <$10,000 to $19,999 (U.S. Census Bureau, 2011) that also encompasses the range of family incomes of most of the children attending the schools we sampled. Thus, while findings from our study sample cannot be generalized to all school-based children in Puerto Rico, the findings do likely pertain to a considerable proportion of the population who are low to middle income. In addition, our sample was school-based and did not include adolescents who dropped out or skipped school, who are at greater risk for Substance Use Disorders and other problem behaviors (Cox, Zhang, Johnson, & Bender, 2007). Further, given the cross-sectional analyses performed, we were not able to examine the stability of class membership over time. Additionally, small sample sizes limited our ability to conduct a more thorough statistical examination of the differences between class membership and other important variables. For example, we were unable to conduct latent class regressions that would allow us to adjust for confounding factors, such as age and gender. Furthermore, as with other studies of this kind, we relied solely on students’ self-report. Still, extant research has supported the validity of adolescent self-report (O’Malley et al., 2000) and the present study incorporated both valid scales and response consistency checks in an effort to eliminate invalid responders. Another limitation of this study is that the data were collected in 2000. However, the scarcity of recent data on Alcohol Abuse and Dependence symptoms in this population justifies using this older dataset. Also, data from the Consulta Juvenil showed that rates of lifetime alcohol use did not appreciably change between 1991–1992 (58.5%) and 2003–2004 (56.9%; the last year data are available). The CDC’s YRBSS showed a similar trend in lifetime alcohol use from 1991 (64.1%) to 2005 (67.0%; the last year data are available). These data suggest that older data may still offer some valid insights into alcohol consumption-related problems in this population.
Study’s Strengths
However, the present study also had many noteworthy and offsetting strengths. The sample was collected from adolescents in Puerto Rico who are rarely studied with respect to their alcohol consumption-related problems. The study applied an empirical method for the classification of youths, rather than applying arbitrary cut points in the data or utilizing the DSM classification system that has been criticized (Chung & Martin, 2001). In addition, the study contributes to the discussion of how DSM-based criteria items function with respect to the diagnosis of adolescents from a different culture, Puerto Rico. This is important because the DSM-V is scheduled to be published in the recent future.
The public health significance of this study is underscored by the fact that an estimated 11.7% of youths were classified into the moderate severity class and 2.3% were classified into the high-severity class, both of which were characterized by having multiple alcohol consumption-related problems. Additionally, this study attempts to classify youths into more homogenous groups that is important for targeting youths to selected and indicated prevention and treatment programs (Winters et al., 1999). Specifically, youths with different patterns of alcohol consumption-related problems (i.e., moderate vs. high-severity groups) would be assigned a different intensity treatment regimen or prevention program. Grouping youths together in this way who are more similar to one another may improve the cost-effectiveness and the outcomes of these programs (Collins, Murphy, & Bierman, 2004).
CONCLUSION
In conclusion, this study found three distinct classes of Puerto Rican youth drinkers with increasing prevalences of Alcohol Abuse and Dependence symptoms. Results showed that the classes were valid in that they were distinct with respect to several other problem and risk behaviors. This study has implications for the diagnosis of Alcohol Abuse and Dependence among Puerto Rican youths and targeting youths to selected and indicated prevention and treatment programs.
Acknowledgments
The authors would like to thank Dr. Sarra Hedden, Dr. Silvia Martins, and Dr. Karen Bandeen-Roche for their invaluable epidemiological and statistical advice. The research and preparation of this article were supported by the US National Institute on Drug Abuse (Grants DA00254 and DA007292).
GLOSSARY
- DSM
Diagnostic and Statistical Manual of Mental Disorders, published by the American Psychiatric Association, a manual used for the diagnosis and classification of psychiatric disorders. The current version is the DSM-IV-TR (fourth edition, text revision).
- LCA
Latent class analysis is a statistical method used with binary (yes/no) items for the purpose of identifying a small number of subgroups or classes of persons who report similar patterns of responses. It is a type of cluster analysis and has been called a categorical analog to factor analysis. Latent class analysis assumes that there are distinct subgroups or classes of individuals in the population that are characterized by their pattern of responses.
- NIDA
National Institute on Drug Abuse, one of the National Institutes of Health, a US government funded research institute whose mission is to study drug abuse and addiction.
- PR
Puerto Rico or Puerto Rican, someone residing on or born on the island of Puerto Rico.
Biographies
THE AUTHORS

Dr. Brent E. Mancha,, Ph.D., M.H.S., is are search associate in the Department of Mental Health at the Johns Hopkins Bloomberg School of Public Health (JHSPH). He is currently assistant director of the Hubert H. Humphrey Fellowship Program at Johns Hopkins. He is a graduate of the PhD program in the Department of Mental Health at JHSPH and an alumnus of the NIDA Drug Dependence Epidemiology Training (DDET) Program. During his first two years of doctoral study, he was a recipient of the NIMH Child Mental Health Services Training Program fellowship. While at Johns Hopkins, he has worked extensively with Dr. William Latimer. Dr. Mancha’s research focuses on the epidemiology of alcohol and drug dependence, with a special interest in alcohol use during adolescence. His dissertation examined patterns of DSM-IV alcohol problems among youths from the US and Puerto Rico and utilized LCA to examine different profiles of adolescent drinkers. Dr. Mancha has experience analyzing multiple datasets, including the National Survey of Drug Use and Health (NSDUH) and several of Dr. Latimer’s datasets, and has experience using multiple statistical techniques.

Dr. Alicia Hulbert, M.S., M.D. is a physician scientist. Her current research focus is on the etiology, prevention, diagnosis, and treatment of HIV-infected lung cancer patients across racial and ethnic groups both domestically and internationally. In addition, Dr. Hulbert was a recipient of the NIDA T32 fellowship in Drug Dependence Epidemiology at the Johns Hopkins Bloomberg School of Public Health where she focused on the epidemiology, prevention, and treatment of infectious disease and drug dependence.

Dr. William W. Latimer, Ph.D., M.P.H. is the Elizabeth Faulk professor and chair of the Department of Clinical and Health Psychology in the College of Public Health and Health Professions at the University of Florida. Dr. Latimer’s research has been NIDA-funded since 1995 and focuses on the epidemiology, prevention, and treatment of infectious disease and drug dependence, with a special focus on neurobehavioral risk factors of disease, treatment engagement, and outcome. His epidemiologic research focuses on neuropsychological and social-behavioral risk factors of HIV and other infectious diseases among drug using populations in the US, South Africa, and Russia. Dr. Latimer’s HIV and drug prevention research focuses on evaluation of efficacy and effectiveness of interventions that coordinate cognitive-behavioral and family systems approaches. Dr. Latimer’s drug treatment research also focuses on evaluating neurobehavioral and process factors influencing the efficacy and effectiveness of cognitive-behavioral, family systems, and 12-Step approaches for adolescent and adult drug abuse. Since 2001, Dr. Latimer has conducted five R01 studies in Baltimore City, including randomized trial studies to test IFCBT efficacy to reduce HIV risk behavior and foster drug abstinence among adults with drug dependence and epidemiologic studies of HIV risk behavior among adult heroin and cocaine addicts.
Footnotes
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.
The reader is reminded that these two posited processes concepts are often noted in the literature, without adequately describing and understanding their dimensions (linear, nonlinear), their “demands”, the critical necessary conditions (endogenously as well as exogenously; from a micro to a macro level) that are necessary for either of them to operate (begin, continue, become anchored, and integrate, change as de facto realities change, cease, etc.) or not to and whether their underpinnings are theory-driven, empirically-based, individual, and/or systemic stake holder-bound, based upon “principles of faith”, historical observation, precedents and traditions that accumulate over time, perceptual and judgmental constraints, “transient public opinion” or what. This is necessary to clarify and to consider if these terms are not to remain as yet additional shibboleths in a field of many stereotypes.
REFERENCES
- Akaike H (1987). Factor analysis and AIC. Psychometrika, 52, 317–332. [Google Scholar]
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, 4th ed., text revision: DSM-IV-TR. Washington, DC: American Psychiatric Association. [Google Scholar]
- Borges G, Ye Y, Bond J, Cherpitel CJ, Cremonte M, Moskalewicz J, et al. (2010). The dimensionality of alcohol use disorders and alcohol consumption in a cross-national perspective. Addiction, 105(2), 240–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bucholz KK, Heath AC, Reich T, & Hesselbrock VM (1996). Can we subtype alcoholism? A latent class analysis of data from relatives of alcoholics in a multicenter family study of alcoholism. Alcoholism: Clinical and Experimental Research, 20(8), 1462–1471. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2002). Involvement by young drivers in fatal alcohol-related motor-vehicle crashes–United States, 1982–2001. MMWR. Morbidity and Mortality Weekly Report, 51(48), 1089–1091. Retrieved January 10, 2009, from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5148a1082.htm [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2008). Youth risk behavior surveillance system (YRBSS), Youth Online: Comprehensive Results [Internet Site]. Retrieved January 9, 2008, from http://apps.nccd.cdc.gov/yrbss/
- Chung T, & Martin CS (2001). Classification and course of alcohol problems among adolescents in addictions treatment programs. Alcoholism: Clinical and Experimental Research, 25(12), 1734–1742. [PubMed] [Google Scholar]
- Collins LM, Murphy SA, & Bierman KL (2004). A conceptual framework for adaptive preventive interventions. Prevention Science, 5(3), 185–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colon HM, Robles RR, Canino G, & Sahai H (2001). Prevalence and correlates of DSM-IV substance use disorders in Puerto Rico. Boletin de la Asociacion Medica de Puerto Rico, 93(1–12), 12. [PubMed] [Google Scholar]
- Cox RG, Zhang L, Johnson WD, & Bender DR (2007). Academic performance and substance use: Findings from a state survey of public high school students. The Journal of School Health, 77(3), 109. [DOI] [PubMed] [Google Scholar]
- Grossman M, Kaestner R, & Markowitz S (2005). An investigation of the effects of alcohol policies on youth STDs. Advances in Health Economics and Health Services Research, 16, 229. [PubMed] [Google Scholar]
- Grube JW (2005). Youth drinking rates and problems: a comparison of European countries and the United States. Calverton, MD: Pacific Institute for Research and Evaluation, Office of Juvenile Justice Enforcing the Underage Drinking Laws Program; Retrieved February 11, 2011, from http://www.udetc.org/documents/CompareDrinkRate.pdf [Google Scholar]
- Harrison PA, Fulkerson JA, & Beebe TJ (1998). DSM-IV substance use disorder criteria for adolescents: A critical examination based on a statewide school survey. The American Journal of Psychiatry, 155(4), 486–492. [DOI] [PubMed] [Google Scholar]
- Harwood EM, Bernat DH, Lenk KM, Vazquez MJ, & Wagenaar AC (2004). Public opinion in Puerto Rico on alcohol control policies. Hispanic Journal of Behavioral Sciences, 26(4), 426–445. [Google Scholar]
- Hasin DS, Schuckit MA, Martin CS, Grant BF, Bucholz KK, & Helzer JE (2003). The validity of DSM-IV alcohol dependence: What do we know and what do we need to know? Alcoholism: Clinical and Experimental Research, 27(2), 244–252. [DOI] [PubMed] [Google Scholar]
- Jackson-Moya I (2000). Co-occurrence of psychiatric syndromes and substance use disorders among Puerto Rican adolescents. Unpublished Dissertation/Thesis, Columbia University, New York. [Google Scholar]
- Jernigan DH (2001). Global status report: Alcohol and Young People. Geneva: World Health Organization; Retrieved February 11, 2011, from http://www.who.int/substance_abuse/publications/alcohol/en/index.html [Google Scholar]
- Jessor R (1987). Problem-behavior theory, psychosocial development, and adolescent problem drinking. British Journal of Addiction, 82(4), 331–342. [DOI] [PubMed] [Google Scholar]
- Jessor R, & Jessor SL (1977). Problem behavior and psychosocial development: a longitudinal study of youth. New York: Academic Press. [Google Scholar]
- Kuo PH, Aggen SH, Prescott CA, Kendler KS, & Neale MC (2008). Using a factor mixture modeling approach in alcohol dependence in a general population sample. Drug and Alcohol Dependence, 98(1–2), 105–114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Latimer WW, Floyd LJ, Vasquez M, O’Brien M, Arzola A, & Rivera N (2004). Substance use among school-based youths in Puerto Rico: differences between gender and grade levels. Addictive Behaviors, 29(8), 1659–1664. [DOI] [PubMed] [Google Scholar]
- Latimer WW, O’Brien MS, McDouall J, Toussova O, Floyd LJ, & Vazquez M (2004). Screening for “substance abuse” among school-based youth in Mexico using the Problem Oriented Screening Instrument (POSIT) for Teenagers. Substance Use & Misuse, 39(2), 307–329. [DOI] [PubMed] [Google Scholar]
- Latimer WW, O’Brien MS, Vasquez MA, Medina-Mora E, Rios-Bedoya CF, & Floyd LJ (2006). Adolescent substance abuse in Mexico, Puerto Rico and the United States: Effect of anonymous versus confidential survey formats. Journal of Child and Adolescent Substance Abuse, 16(1), 69–89. [Google Scholar]
- Lazarsfeld P, & Henry N (1968). Latent structure analysis. New York: Houghton Mifflin. [Google Scholar]
- Lo Y, Mendell N, & Rubin D (2001). Testing the number of components in a normal mixture. Biometrika, 88, 767–778. [Google Scholar]
- Malavet PA (2004). America’s colony: The political and cultural conflict between the United States and Puerto Rico. New York: New York University Press. [Google Scholar]
- Martin CS, & Winters KC (1998). Diagnosis and assessment of alcohol use disorders among adolescents. Alcohol Health and Research World, 22(2), 95–105. [PMC free article] [PubMed] [Google Scholar]
- McCutcheon AL (1987). Latent class analysis. Newbury Park, CA: Sage. [Google Scholar]
- McLachlan G, & Peel D (2000). Finite mixture models. New York: John Wiley. [Google Scholar]
- Moscoso MR, Colon HM, Parrilla I, & Reyes JC (2003). El uso de substancias en los escolares Puertorriquenos: Consulta Juvenil V, 2000–2002. Bayamon, PR: Administracion de Servicios de Salud Mental y Contra la Adiccion. Departamento de Medicina de Familia y Salud Comunal, Universidad Central del Caribe. [Google Scholar]
- Moscoso MR, Parrilla I, Robles R, Colon HM, & Garcia M (1998). En uso de substancias en los escolares Puertorriquenos Consulta Juvenil IV, 1997–98. Hato Rey: Instituto de Investigaciones, Administracion de Servicios de Salud Mental y Contra la Adiccion, Departamento de Medicina de Familia y Salud Comunal, Universidad Central del Caribe. [Google Scholar]
- Moss HB, Chen CM, & Yi HY (2008). DSM-IV crite-ria endorsement patterns in alcohol dependence: Relationship to severity. Alcoholism: Clinical and Experimental Research, 32(2), 306–313. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2007). Mplus user’s guide (5th ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Naimi TS, Lipscomb LE, Brewer RD, & Gilbert BC (2003). Binge drinking in the preconception period and the risk of unintended pregnancy: Implications for women and their children. Pediatrics, 111(5 Part 2), 1136–1141. [PubMed] [Google Scholar]
- Negron-Montaner F (2007). Introduction In Negron-Muntaner F (Ed.), None of the above: Puerto ricans in the global era (pp. 1–17). New York: Palgrave Macmillan. [Google Scholar]
- Nylund KL, Asparouhov T, & Muthén BO (2007). Deciding on the number of classes in latent class analysis and growth mixture modeling: A monte carlo simulation study. Structural Equation Modeling, 14, 535–569. Retrieved March 5, 2008, from http://www.statmodel.com/download/LCA_tech2011_nylund_v2083.pdf [Google Scholar]
- O’Malley PM, Johnston LD, Bachman JG, & Schulenberg JE (2000). A comparison of confidential versus anonymous survey procedures: Effects on reporting of drug use and related attitudes and beliefs in a national study of students. Journal of Drug Issues, 30(1), 35–54. [Google Scholar]
- Pico F (2007). The absent state In Negron-Muntaner F (Ed.), None of the above: Puerto ricans in the global era (pp. 21–28). New York: Palgrave Macmillan. [Google Scholar]
- Plant M, Miller P, Plant M, Gmel G, Kuntsche S, Bergmark WK, et al. (2010). The social consequences of binge drinking among 24- to 32-year-olds in six European countries. Substance Use and Misuse, 45(4), 528–542. [DOI] [PubMed] [Google Scholar]
- Pollock NK, & Martin CS (1999). Diagnostic orphans: Adolescents with alcohol symptoms who do not qualify for DSM-IV abuse or dependence diagnoses. The American Journal of Psychiatry, 156(6), 897–901. [DOI] [PubMed] [Google Scholar]
- Puerto Rico Chamber of Commerce. (1994). Self-regulation of the alcoholic beverage and beer industries. San Juan, PR: Industrial Committee for Alcoholic Beverages and Beer. [Google Scholar]
- Reboussin BA, Song EY, Shrestha A, Lohman KK, & Wolfson M (2006). A latent class analysis of underage problem drinking: Evidence from a community sample of 16–20 year olds. Drug and Alcohol Dependence, 83(3), 199–209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robert Wood Johnson Foundation. (1997). Puerto Rico Coalition funded by the Robert Wood Johnson Foundation National Program to Reduce Underage Drinking Through Coalitions. Retrieved April 11, 2009, from http://www.rwjf.org/reports/grr/041116.htm
- Robles R, Martinez R, & Moscoso M (1979). Drug use among public and private secondary school students in Puerto Rico. The International Journal of the Addictions, 14(2), 243. [DOI] [PubMed] [Google Scholar]
- Robles R, Moscoso MR, Colon HM, Garcia M, & Parrilla I (1995). En uso de substancias en los escolares Puertorriquenos Consulta Juvenil III, 1994–95. Hato Rey: Instituto de Investigaciones, Administracion de Servicios de Salud Mental y Contra la Adiccion, Departamento de Medicina de Familia y Salud Comunal, Universidad Central del Caribe. [Google Scholar]
- Robles R, Moscoso M, Colon H, Garcia M, & Rebollo J (1991). En uso de substancias en los escolares Puertorriquenos. Hato Rey: Instituto de Investigaciones, Administracion de Servicios de Salud Mental y Contra la Adiccion, Departamento de Medicina de Familia y Salud Comunal, Universidad Central del Caribe. [Google Scholar]
- Robles R, Moscoso MR, Colon HM, Garcia M, Rebollo J, & Parrilla I (1994). En uso de substancias en los escolares Puertorriquenos Consulta Juvenil II, 1992–93. Hato Rey: Instituto de Investigaciones, Administracion de Servicios de Salud Mental y Contra la Adiccion, Departamento de Medicina de Familia y Salud Comunal, Universidad Central del Caribe. [Google Scholar]
- Schwartz G (1978). Estimating the dimension of a model. The Annals of Statistics, 6, 461–464. [Google Scholar]
- Sclove L (1987). Application of model-selection criteria to some problems in multivariate analysis. Psychometrika, 52, 333–343. [Google Scholar]
- Stafstrom M (2007). Kick back and destroy the ride: Alcohol-related violence and associations with drinking patterns and delinquency in adolescence. Substance Abuse Treatment, Prevention, and Policy, 2, 18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Traffic Safety Commission. (1999). El problema del alcohol y su relacion con los choques de transito en Puerto Rico. Santurce, PR: Traffic Safety Commission of Puerto Rico. [Google Scholar]
- U.S. Census Bureau. (2011). 2005–2009 American Community Survey 5-year estimates. Retrieved May 13, 2011, from http://factfinder2.census.gov
- Warner LA, Canino G, & Colon HM (2001). Prevalence and correlates of substance use disorders among older adolescents in Puerto Rico and the United States: A cross-cultural comparison. Drug and Alcohol Dependence, 63(3), 229–243. [DOI] [PubMed] [Google Scholar]
- Whitesell NR, Beals J, Mitchell CM, Novins DK, Spicer P, Manson SM, et al. (2006). Latent class analysis of substance use: Comparison of two American Indian reservation populations and a national sample. Journal of Studies on Alcohol, 67(1), 32. [DOI] [PubMed] [Google Scholar]
- Winters KC, & Henly GA (1989). Personal Experience Inventory and manual. Los Angeles, CA: Western Psychological Services. [Google Scholar]
- Winters KC, & Henly GA (1993). Adolescent Diagnostic Interview and manual. Los Angeles, CA: Western Psychological Services. [Google Scholar]
- Winters KC, Latimer WW, Stinchfield RD, Ott PJ, Tarter RE, & Ammerman RT (1999). Adolescent treatment In Ott PJ, Tarter RE, & Ammerman RT (Eds.), Source book on substance abuse: Etiology, epidemiology, assessment, and treatment (pp. 350–361). New York: Allyn and Bacon. [Google Scholar]