

Abstract
Objective
Dietary questionnaires for assessing dietary intakes among populations of individuals aged 80 years or older (the very old) are very limited. We examined the relative validity of forty-three nutrients and twenty-seven food groups estimated by a brief-type self-administered diet history questionnaire (BDHQ) targeting very old Japanese, using semi-weighed dietary records (DR) as a reference.
Design
Between June and August 2012 and between June 2015 and February 2016, a three-day non-consecutive DR (at two-week intervals) and a BDHQ were completed.
Setting
Tokyo, the capital prefecture of Japan.
Subjects
Eighty very old Japanese (thirty-six men and forty-four women) aged 82–94 years.
Results
The median intakes of 40–70 % of the crude and energy-adjusted nutrients estimated by the BDHQ were significantly different from those estimated by the DR. The median Spearman’s correlation coefficient of nutrient intakes between the BDHQ and the DR was 0·39–0·46. About half (48–56 %) of the food groups were significantly different in terms of the median intakes estimated by the BDHQ and the DR in crude and energy-adjusted values. The median Spearman’s correlation coefficient between the BDHQ and the DR was 0·45–0·48.
Conclusions
Acceptable Spearman’s correlations (≥0·3) were obtained for many dietary intakes among the very old Japanese population. The BDHQ is a good candidate for epidemiological studies among very old Japanese, although, for some nutrients and food groups, the difficulty of estimating accurate median intakes is one of the limitations for the tool. Further efforts to enhance the validity of the BDHQ for very old populations are needed.
Keywords: Diet history questionnaire, Dietary intake, Relative validity, Very old Japanese
Populations are ageing throughout the world and this is accompanied by the rapid increase of very old populations aged 85 years or older( 1 ). Because of the vulnerability to age-related chronic diseases and disabilities among very old populations, the use of medical-care services by adults rises with age and per capita costs of health care are relatively high among older age groups. These costs are placing upward pressure on overall health-care spending. Preventing chronic and non-communicable diseases as well as the functional deterioration of very old populations is a major public health objective aimed at slowing the growing financial burden on societies( 1 ). Diet is one of the modifiable factors related to health. Understanding dietary habits and the relationship between diet and health conditions among very old populations is essential for providing dietary strategies focused on maintaining the health and independence of these individuals. However, information about dietary habits among very old populations throughout the world is still limited( 2 – 8 ).
Japan has one of the highest percentages of older populations and is one of the most rapidly ageing countries in the world( 9 ). The size of the very old population (aged 85 years or older) in Japan was estimated to be 5·5 million (4·3 %) in 2017 and this is expected to continue increasing for some time in the future( 10 ). Clarifying dietary habits contributing to successful ageing for very old Japanese can potentially provide effective dietary strategies to health-care providers in other countries, which also face the challenges associated with an ageing population. However, few studies have examined the dietary habits of the very old population in Japan( 11 , 12 ).
Dietary questionnaires can assess long-term dietary habits and are convenient for dietary surveys( 13 , 14 ). The brief-type self-administered diet history questionnaire (BDHQ) was developed to evaluate the dietary habits of Japanese adults( 15 , 16 ). The validity of the intakes of forty-two selected nutrients and twenty-nine food groups estimated by the BDHQ has been examined only among adult Japanese aged 31–76 years( 15 , 16 ). Meanwhile, the dietary assessment using questionnaires for very old populations poses many challenges because of magnified reporting error( 17 ) possibly caused by both a decrease in cognitive function and systematic errors of calculation resulting from a lack of available data on portion sizes in this age group( 5 ). Therefore, the validity of the BDHQ for very old populations needs to be investigated. However, only one study has examined the validity of the BDHQ among very old Japanese, but only for two nutrients (i.e. EPA and DHA) using erythrocyte membrane phospholipid as a reference. That previous study showed a satisfactory correlation between the BDHQ and the biomarker for EPA (Spearman’s correlation coefficient=0·58 in men and 0·44 in women) and DHA (0·55 in men and 0·29 in women)( 11 ). The validity of other nutrient and food intakes estimated by the BDHQ has yet to be examined among very old populations.
In Japan, the Tokyo Oldest Old Survey on Total Health (TOOTH) study( 18 ) and the Septuagenarians, Octogenarians, Nonagenarians Investigation with Centenarians (SONIC) study( 19 ) are being conducted to demonstrate important perspectives on the health and well-being for old Japanese aged 80 years or older (the very old in the present study). These studies use the BDHQ to assess the dietary habits of the participants. Conducting a validation study for the intakes of comprehensive nutrients and foods estimated by the BDHQ among very old Japanese may advance TOOTH and SONIC studies and further epidemiological studies among very old populations in clarifying the relationship between diet and geriatric conditions such as frailty, osteoporosis and cognitive impairment. In the present study, we investigated the relative validity of nutrient and food group intakes assessed by the BDHQ among healthy very old Japanese compared with those assessed by a three-day, semi-weighed dietary record (DR).
Methods
Study population
The participants of the present study represented a portion of the participants aged 85 years or older from the TOOTH study( 18 ) and the participants in their 80s or 90s from the SONIC study( 19 ). A detailed description of the study design and survey procedure of each original cohort study has been published elsewhere( 18 , 19 ). For the present study, we recruited apparently healthy and community-dwelling TOOTH and SONIC participants living in Tokyo, which is the capital prefecture in Japan that includes urban and rural areas, at the 3- or 6-year follow-up survey for TOOTH (2012 or 2015) or at the 3-year follow-up survey for SONIC (2014). We asked the participants to conduct a three-day, non-consecutive semi-weighed dietary record, a one-time diet history questionnaire, and five to fourteen consecutive days of accelerometer wearing (Fig. 1). Although about half of the recruited participants declined to participate, a total of eighty participants (thirty-six men and forty-four women; forty-two from TOOTH and thirty-eight from SONIC) aged 82–94 years participated in the present study. For these participants, the mean score at baseline (3 or 6 years before the present study) of the Barthel index (BI) was 99·4 (sd 2·5), that of the Mini-Mental State Examination (MMSE) was 27·7 (sd 2·5) (n 42 from TOOTH; Y Arai, unpublished results, 2017) and that of the Japanese version of the Montreal Cognitive Assessment (MoCA-J) was 23·1 (sd 3·1) (n 38 from SONIC; Y Masui, unpublished results, 2017).
Fig. 1.

Schedule for the present validation study (BDHQ, brief-type self-administered diet history questionnaire; DR, semi-weighed dietary record)
Three-day semi-weighed dietary record
Between June and August 2012 or between June 2015 and February 2016, the participants completed a non-consecutive, three-day DR at two-week intervals (Fig. 1). All of the recording days were weekdays. On the day prior to the first recording day, the research staff, including registered dietitians or nutritionists, visited each participant’s home to provide instruction on the whole survey protocol and dietary record. The research staff supplied the participants with recording sheets and a sample of a completed record and provided face-to-face verbal and written instructions on how to record the diet. Each participant was given a digital scale (model KD-812; Tanita, Tokyo, Japan; ±2 g precision for 0–500 g and ±3 g precision for 501–2000 g), taught how to assign weights to all foods and drinks consumed on the recording day, and asked to record them. If the participants did not cook for themselves, they were advised to request assistance from the person who usually prepared their meals consumed in their home (e.g. their spouse, adult child or helper). When assigning weights was difficult (e.g. when eating out), they were instructed to record the size and quantity of the food eaten using household approximations in as much detail as possible. On the day following each recording day, the research staff revisited the participant’s home to check the dietary record (Fig. 1). The staff reviewed the record and asked the participant to add to or modify the record if necessary.
All collected records were further checked by the research staff at the data centre. If necessary, the staff asked the participant to clarify unclear records by telephone or through an in-home visit. The keeping of records and the conversion of other measurements of quantities into grams were performed by trained dietitians at the survey centre in accordance with uniform procedures. A total of 969 food and beverage items appeared in the whole data of the dietary record.
Brief-type self-administered diet history questionnaire
All participants answered the BDHQ on the day prior to the first DR recording day after receiving instructions on the dietary record procedures (Fig. 1). The staff read through the BDHQ and wrote down the verbal responses obtained from each participant.
The BDHQ is a four-page, fixed-portion questionnaire that asks about the consumption frequency of selected foods, but not about portion size, to estimate the dietary intake of fifty-eight food and beverage items during the preceding month. To facilitate reading and completion for the elderly, we used a large-print version, which increased the size to ten pages but that contained no other changes to structure or content. Details of the BDHQ’s structure, method of calculating dietary intake, and validity for food group and nutrient intakes among the adult population (31–76 years) have been described elsewhere( 15 , 16 ). Briefly, the BDHQ consists of the following five sections: (i) intake frequency of food and non-alcoholic beverage items; (ii) daily intake of rice and miso soup; (iii) frequency of drinking and amount per drink for alcoholic beverages; (iv) usual cooking methods; and (v) general dietary behaviour. Food and beverage items contained in the BDHQ were selected from foods commonly consumed in Japan, mainly from a food list used in the National Health and Nutrition Survey of Japan( 20 ), while standard portion sizes were derived from several recipe books for Japanese dishes( 15 , 21 ). Information on dietary supplements was obtained only for total frequency of use, without specific names or types and quantity of the supplements. Estimates of the intake for fifty-eight food and beverage items were calculated using an ad hoc computer algorithm for the BDHQ( 15 ).
Other variables
When the research staff visited the participants’ homes to provide instruction for the DR, in-home interviews were conducted during which the staff asked the participants about their living arrangements (living alone or living with others). Once the interviews were complete, the staff took in-home body weight measurements of the participants wearing light clothing and no shoes. The participants provided information about their date of birth, alcohol intake and dietary supplement use in the BDHQ. The participants had also been wearing a triaxial accelerometer (model Active style Pro HJA-350IT; Omron Healthcare, Kyoto, Japan) on the waist for five to fourteen consecutive days between the second and third DR (Fig. 1). The number of daily steps (steps/d) was summed over valid days and a mean value was calculated using the data from the accelerometer. Data for participants with at least three valid wear-days and at least eight hours of wear-time per day were included in the analysis. The individual body height measured at the previous follow-up survey, the proportion of past or current smoking status (yes or no) at baseline and the proportion of history of chronic disease (e.g. hypertension, diabetes mellitus, hyperlipidaemia, fragility fracture, cancer other than skin, stroke, heart diseases and renal diseases (yes or no)) at baseline were obtained from the original study (Y Arai, unpublished results, 2017). BMI was calculated as body weight divided by the square of body height (kg/m2).
Statistical analysis
All statistical analyses were conducted using the SAS statistical software package version 9·4.
Intake values of energy and selected nutrients were estimated based on the intakes of food items obtained from the DR or the BDHQ and the corresponding food composition list in the Standard Tables of Food Composition in Japan ( 22 ). In both the DR and the BDHQ, nutrients derived from dietary supplements were not included in the present study. For foods, we categorized the food groups according to the previous study( 15 ).
In consideration of reporting errors, energy-adjusted intakes, as well as crude values, were also calculated by the residual and density methods. The Shapiro–Wilk test for normality showed that almost all crude and energy-adjusted intakes of nutrients and food groups estimated by the DR and the BDHQ had non-normal distribution (about 72 % for nutrients and 94 % for food groups). Therefore, we used the non-parametric test in evaluating the validity for the BDHQ. We evaluated the relative validity of the BDHQ in terms of two abilities. One of the abilities is to estimate median values of a population, using the Wilcoxon signed-rank test. The median and interquartile range (IQR) were shown for dietary intakes estimated by the DR and the BDHQ. The result of P<0·05 for the test was considered to indicate a significant difference between the intakes estimated by the BDHQ and those by the DR. The other is the ability to rank the individuals in a population according to dietary intakes, using Spearman’s correlation coefficients between the intakes estimated by the DR and the BDHQ. Further, we evaluated the agreement for energy and macronutrient intakes between the DR and the BDHQ at the individual level as reference using Bland–Altman plots( 23 ).
Results
The mean age of the eighty participants, including thirty-six men (45 %) and forty-four women (55 %), was 87·2 (sd 3·5) years and their mean BMI was 22·4 (sd 3·4) kg/m2 (Table 1). A total of thirty-nine participants (49 %) lived alone (19 % for men and 73 % for women). The percentages of past or current smoker, alcohol drinker and dietary supplement user were all 40 %. Daily energy intake ranges were 4·24–13·6 MJ for the DR and 4·00–16·1 MJ for the BDHQ (data not shown). We included all eighty participants in the following analyses. We also describe the baseline characteristics of the original cohort of TOOTH (n 542) and SONIC (n 965) in Table 1 by referring to previous studies( 18 , 19 , 24 ) and unpublished results. Similar values were observed for BMI (mean of 21·4 kg/m2 for TOOTH and 22·4 kg/m2 for SONIC), past or current smoker (38 % for TOOTH and 40 % for SONIC) and alcohol drinker (34 % for TOOTH and 31 % for SONIC) between the present participants and the original cohort. The mean percentage of the history of eight chronic diseases for the participants was 21 %, while the respective value was 25 % for TOOTH. The mean scores of BI, MMSE and MoCA-J among the original cohort in the previous publications were 97·1, 26·2 and 21·8, respectively.
Table 1.
Selected characteristics of the eighty very old Japanese participants (aged 80 years or older) and comparison with those of the original cohort of the TOOTH and SONIC studies
| Participants of the validation study† | Original cohort at baseline | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total (n 80) | Men (n 36) | Women (n 44) | TOOTH (n 542)‡ | SONIC (n 965)§ | |||||||
| Mean or n | sd or % | Mean or n | sd or % | Mean or n | sd or % | Mean or n | sd or % | Mean or n | sd or % | ||
| Age (years), mean and sd | 87·2 | 3·5 | 87·3 | 3·4 | 87·1 | 3·6 | ≥85 | 79–81 | |||
| Sex, n and % | |||||||||||
| Men | 36 | 45·0 | – | – | 236 | 43·5 | 453 | 46·9 | |||
| Women | 44 | 55·0 | – | – | 306 | 56·5 | 512 | 53·1 | |||
| Body height (cm), mean and sd | 153·0 | 8·6 | 160·3 | 5·5 | 147·0 | 5·5 | – | – | |||
| Body weight (kg), mean and sd | 52·9 | 10·7 | 60·1 | 8·7 | 46·9 | 8·3 | – | – | |||
| BMI (kg/m2), mean and sd | 22·4 | 3·4 | 23·3 | 2·8 | 21·7 | 3·7 | 21·4 | 3·2 | 22·4 | 3·0 | |
| Original cohort, n and % | |||||||||||
| TOOTH | 42 | 52·5 | 21 | 58·3 | 21 | 47·7 | – | – | |||
| SONIC | 38 | 47·5 | 15 | 41·7 | 23 | 52·3 | – | – | |||
| Living arrangements, n and % | |||||||||||
| Living alone | 39 | 48·8 | 7 | 19·4 | 32 | 72·7 | 183 | 34·0 | – | ||
| Living with others | 41 | 51·3 | 29 | 80·6 | 12 | 27·3 | 355 | 66·0 | – | ||
| Past or current smoker, n and % | 32 | 40·0 | 24 | 66·6 | 8 | 18·2 | 205 | 38·2 | 381 | 39·5 | |
| Alcohol drinker, n and % | 32 | 40·0 | 19 | 52·8 | 13 | 30·0 | 185 | 34·1 | 297 | 30·8 | |
| Dietary supplement user, n and % | 32 | 40·0 | 15 | 41·7 | 17 | 38·6 | 152 | 29·6 | – | ||
| Barthel index score (range 0–100), mean and sd | 99·4 | 2·5 | – | – | 97·1 | 8·2 | – | ||||
| Daily steps (steps/d), mean and sd | 4207 | 2762 | 5386 | 2954 | 3302 | 2245 | – | – | |||
| History of chronic disease, n and % | |||||||||||
| Hypertension | 41 | 51·2 | 18 | 50·0 | 23 | 52·3 | 336 | 62·7 | – | ||
| Diabetes mellitus | 10 | 12·5 | 6 | 16·7 | 4 | 9·1 | 100 | 18·7 | 160 | 16·6 | |
| Hyperlipidaemia | 21 | 26·3 | 9 | 25·0 | 12 | 27·3 | 225 | 42·0 | 581 | 60·2 | |
| Fragility fracture | 16 | 20·0 | 3 | 8·3 | 13 | 29·5 | 123 | 23·0 | – | ||
| Cancer other than skin | 16 | 20·0 | 9 | 25·0 | 7 | 15·9 | 100 | 18·9 | – | ||
| Stroke | 5 | 6·3 | 3 | 8·3 | 2 | 4·5 | 92 | 17·2 | – | ||
| Heart disease | 17 | 21·3 | 9 | 25·0 | 8 | 18·2 | 54 | 10·1 | – | ||
| Renal disease | 8 | 10·0 | 4 | 11·1 | 4 | 9·1 | 57 | 10·6 | – | ||
| MMSE score (range 0–30), mean and sd | 27·7 | 2·5 | – | – | 26·2 | 3·9 | – | ||||
| MoCA-J score (range 0–30), mean and sd | 23·1 | 3·1 | – | – | – | 21·8 | 3·8 | ||||
| Daily energy intake (kJ/d), mean and sd | |||||||||||
| DR | 7753 | 1791 | 8176 | 1719 | 7407 | 1793 | – | – | |||
| BDHQ | 7422 | 2211 | 8382 | 2190 | 6637 | 1916 | – | – | |||
TOOTH, Tokyo Oldest Old Survey on Total Health study; SONIC, Septuagenarians, Octogenarians, Nonagenarians Investigation with Centenarians study; MMSE, Mini-Mental State Examination; MoCA-J, Japanese version of the Montreal Cognitive Assessment; DR, three-day semi-weighed dietary record; BDHQ, brief-type self-administered diet history questionnaire.
All values were obtained at the time of the validation study unless otherwise stated; n 76 (thirty-three men and forty-three women) for daily steps. The values of the Barthel index and MMSE (n 42 (twenty-one men and twenty-one women (TOOTH)); Y Arai, unpublished results), MoCA-J (n 38 (fifteen men and twenty-three women (SONIC)); Y Masui, unpublished results) and history of chronic disease (Y Arai, unpublished results) shown were at baseline of the original cohort.
Values of TOOTH presented were from Arai et al.( 18 ) for age, sex, Barthel index and MMSE (n 542) and living arrangements (n 538); from Arai et al.( 24 ) for past or current smoker and history of chronic disease (n 536); and from Y Arai (unpublished results) for BMI, alcohol drinker and dietary supplement user (n 513). Distribution for the age groups was n 496 (91·5 %) for 85–89 years, n 38 (7·0 %) for 90–94 years, n 6 (1·1 %) for 95–99 years and n 2 (0·4 %) for ≥100 years. The value for heart disease presented was from coronary heart disease.
Values of SONIC presented are those for the participants aged 80 years from Ryuno et al.( 19 ). Age range is shown.
Energy intake as determined by the BDHQ was significantly lower than that determined by the DR (Table 2). Spearman’s correlation coefficient for energy intake estimated by the DR and the BDHQ was 0·58. A total of forty-three energy-adjusted nutrient intakes for the DR and the BDHQ using the residual method are also described in Table 2. The intakes of twenty-one (49 %) nutrients differed significantly between the DR and the BDHQ. The median value of Spearman’s correlation coefficient was 0·39 (IQR 0·33–0·47). For retinol and cryptoxanthin, the intakes estimated by the BDHQ were not significantly correlated to those estimated by the DR. For nutrients in the crude and energy-adjusted values as determined by the density method, similar results were obtained (see online supplementary material, Supplemental Table 1). The number of nutrients whose intakes differed significantly between the DR and the BDHQ was seventeen (40 %) for the crude and thirty (70 %) for the density methods. The median value of Spearman’s correlation coefficients for the nutrients was 0·46 (IQR 0·37–0·50) for the crude and 0·39 (IQR 0·34–0·46) for the density methods.
Table 2.
Daily energy and energy-adjusted† nutrient intakes and Spearman’s correlation coefficients estimated by the three-day semi-weighed dietary records (DR) and the brief-type self-administered diet history questionnaire (BHDQ) among the eighty very old Japanese men and women (aged 80 years or older), June–August 2012 and June 2015–February 2016
| Energy/nutrient | Unit | Daily intake | Spearman’s correlation coefficient | |||
|---|---|---|---|---|---|---|
| DR | BDHQ | |||||
| Median | IQR | Median | IQR | |||
| Energy | kJ/d | 7666 | 6516–8815 | 6871* | 5856–8812 | 0·58 |
| Protein | g/d | 72·6 | 66·1–76·8 | 73·0 | 67·5–80·3 | 0·32 |
| Fat | g/d | 57·7 | 51·6–62·3 | 55·7 | 49·1–61·4 | 0·37 |
| SFA | g/d | 16·16 | 12·53–18·94 | 15·15 | 13·40–17·08 | 0·48 |
| MUFA | g/d | 20·02 | 16·46–22·47 | 19·73 | 16·43–21·53 | 0·35 |
| PUFA | g/d | 12·55 | 10·31–14·41 | 12·66 | 11·00–15·10 | 0·43 |
| n-6 PUFA | g/d | 10·12 | 8·11–11·41 | 9·96 | 8·28–11·78 | 0·43 |
| n-3 PUFA | g/d | 2·31 | 1·79–2·95 | 2·82*** | 2·42–3·26 | 0·37 |
| Marine-origin n-3 PUFA‡ | g/d | 0·93 | 0·62–1·36 | 0·98 | 0·81–1·40 | 0·36 |
| EPA acid | g/d | 0·29 | 0·17–0·44 | 0·33* | 0·26–0·49 | 0·34 |
| DHA | g/d | 0·52 | 0·36–0·71 | 0·56 | 0·45–0·78 | 0·36 |
| α-Linolenic acid | g/d | 1·24 | 0·93–1·53 | 1·61*** | 1·18–1·88 | 0·37 |
| Cholesterol | mg/d | 331 | 274–399 | 439*** | 364–517 | 0·36 |
| Carbohydrate | g/d | 250·1 | 237·6–267·4 | 233·6*** | 215·9–256·1 | 0·42 |
| Total dietary fibre | g/d | 15·6 | 12·9–19·0 | 14·2** | 12·3–16·4 | 0·42 |
| Soluble dietary fibre | g/d | 3·6 | 2·8–4·1 | 3·6 | 3·0–4·0 | 0·56 |
| Insoluble dietary fibre | g/d | 11·4 | 9·5–14·0 | 9·9*** | 8·6–11·4 | 0·39 |
| Alcohol | g/d | 2·1 | 0·4–5·0 | 1·2* | 0·2–3·3 | 0·66 |
| Retinol | μg/d | 232 | 132–336 | 366*** | 284–661 | 0·20 |
| Vitamin A (retinol equivalents)§ | μg/d | 573 | 430–792 | 808*** | 598–1112 | 0·46 |
| α-Carotene | μg/d | 351 | 233–653 | 341 | 268–697 | 0·44 |
| β-Carotene | μg/d | 3547 | 2310–5307 | 3664 | 2543–5097 | 0·50 |
| β-Carotene equivalents║ | μg/d | 3856 | 2585–6135 | 3907 | 2995–5826 | 0·51 |
| Cryptoxanthin | μg/d | 90 | 45–336 | 353** | 133–665 | 0·13 |
| Vitamin D | μg/d | 8·5 | 5·1–11·5 | 16·3*** | 12·8–23·4 | 0·28 |
| α-Tocopherol | mg/d | 8·1 | 7·0–9·6 | 8·2 | 7·0–9·9 | 0·42 |
| Vitamin K | μg/d | 207 | 161–338 | 308*** | 248–444 | 0·54 |
| Thiamin | mg/d | 0·99 | 0·84–1·14 | 0·86*** | 0·76–1·00 | 0·22 |
| Riboflavin | mg/d | 1·45 | 1·18–1·67 | 1·50 | 1·34–1·66 | 0·23 |
| Niacin | mg/d | 16·2 | 13·9–19·5 | 16·9 | 14·9–19·7 | 0·53 |
| Vitamin B6 | mg/d | 1·38 | 1·18–1·68 | 1·37 | 1·20–1·58 | 0·64 |
| Vitamin B12 | μg/d | 6·7 | 4·3–11·0 | 9·5*** | 7·2–12·1 | 0·33 |
| Folate | μg/d | 405 | 337–511 | 416 | 367–491 | 0·39 |
| Pantothenic acid | mg/d | 6·21 | 5·52–7·13 | 7·10*** | 6·40–7·67 | 0·46 |
| Vitamin C | mg/d | 134 | 107–171 | 152** | 121–199 | 0·52 |
| Na | mg/d | 3846 | 3162–4381 | 4288*** | 3787–4971 | 0·33 |
| K | mg/d | 2901 | 2473–3410 | 2892 | 2586–3365 | 0·50 |
| Ca | mg/d | 622 | 514–725 | 652* | 550–762 | 0·32 |
| Mg | mg/d | 283 | 242–319 | 272 | 253–315 | 0·40 |
| P | mg/d | 1088 | 1011–1213 | 1153** | 1048–1267 | 0·27 |
| Fe | mg/d | 8·7 | 7·4–10·7 | 8·7 | 8·0–10·1 | 0·38 |
| Zn | mg/d | 7·9 | 7·4–8·5 | 8·2* | 7·5–9·0 | 0·29 |
| Cu | mg/d | 1·25 | 1·07–1·37 | 1·19 | 1·08–1·29 | 0·39 |
| Mn | mg/d | 3·78 | 3·18–4·99 | 3·94 | 3·18–4·26 | 0·48 |
IQR, interquartile range.
Significant differences between the DR and BDHQ: *P<0·05, **P<0·01, ***P<0·001 (Wilcoxon signed-rank test).
Energy adjustment was performed according to the residual method.
Sum of EPA, DPA (docosapentaenoic acid) and DHA.
Sum of retinol, β-carotene/12, α-carotene/24 and cryptoxanthin/24.
Sum of β-carotene and α-carotene/2 and cryptoxanthin/2.
Twenty-seven food group intakes estimated by the DR and the BDHQ using the residual method are shown in Table 3. For a total of fifteen (56 %) food groups, the intakes estimated by the BDHQ differed significantly from those estimated by the DR. The median Spearman’s correlation coefficient between the intakes estimated by the DR and the BDHQ was 0·48 (IQR 0·39–0·55), as estimated by the residual method. Only the intakes of sugar estimated by the DR and the BDHQ were not significantly correlated. Similar results were obtained from crude values and energy-adjusted values as estimated by the density method (see online supplementary material, Supplemental Table 2). A total of fourteen (52 %) food group intakes in crude values and thirteen (48 %) food group intakes in energy-adjusted values using the density method differed significantly between the DR and the BDHQ. For Spearman’s correlation coefficient between the DR and the BDHQ, the median value was 0·47 (IQR 0·38–0·56) for the crude and 0·45 (IQR 0·36–0·54) for the density methods. We also examined the validity of the BDHQ among thirty-six men and forty-four women, separately (data not shown). The number of nutrients for which intakes differed significantly between the DR and the BDHQ was more in men than in women. The number of foods in men was almost the same as that in women. For the Spearman’s correlation coefficient, the median values of men tended to be higher than those of women for both nutrient and food intakes.
Table 3.
Daily energy-adjusted† food group intakes and Spearman’s correlation coefficients estimated by the three-day semi-weighed dietary records (DR) and the brief-type self-administered diet history questionnaire (BHDQ) among the eighty very old Japanese men and women (aged 80 years or older), June–August 2012 and June 2015–February 2016
| Food group | Daily intake (g/d) | Spearman’s correlation coefficient | |||
|---|---|---|---|---|---|
| DR | BDHQ | ||||
| Median | IQR | Median | IQR | ||
| Cereals | 336·7 | 277·1–393·3 | 312·9* | 273·3–361·1 | 0·40 |
| Rice | 196·8 | 146·0–254·4 | 153·0* | 115·4–247·8 | 0·54 |
| Noodles | 59·9 | 2·8–130·7 | 68·1 | 33·3–113·3 | 0·58 |
| Bread | 38·5 | 17·5–57·7 | 56·9*** | 29·7–68·4 | 0·59 |
| Pulses | 50·8 | 26·4–95·2 | 61·3* | 42·1–91·5 | 0·40 |
| Potatoes | 24·6 | 9·8–57·4 | 58·5*** | 33·3–87·2 | 0·29 |
| Sugar and confectioneries | 56·9 | 28·7–103·6 | 75·0 | 42·9–94·9 | 0·48 |
| Sugar | 11·2 | 5·9–17·9 | 3·5*** | 1·5–6·8 | 0·05 |
| Confectioneries | 46·3 | 18·0–91·3 | 70·4* | 39·2–90·8 | 0·48 |
| Oil | 11·5 | 7·4–19·2 | 16·8* | 9·4–23·0 | 0·36 |
| Fruits | 149·8 | 80·8–282·5 | 124·9** | 63·5–185·4 | 0·48 |
| Total vegetables | 304·9 | 247·2–440·2 | 318·8 | 245·8–420·2 | 0·43 |
| Green and yellow vegetables | 128·9 | 76·9–185·8 | 119·6 | 83·1–181·2 | 0·50 |
| Other vegetables | 151·5 | 110·7–204·6 | 139·1 | 104·9–186·7 | 0·32 |
| Pickled vegetables | 18·4 | 9·0–32·8 | 19·1 | 7·3–27·7 | 0·40 |
| Mushrooms | 4·1 | 0·1–9·9 | 10·3** | 3·8–19·7 | 0·21 |
| Seaweeds | 9·5 | 3·1–19·7 | 14·4*** | 8·8–30·5 | 0·51 |
| Alcoholic beverages | 25·3 | −7·3–85·1 | 14·8 | 2·4–38·8 | 0·64 |
| Fruit and vegetable juice | 1·4 | −2·5–8·1 | 10·1*** | −0·8–118·0 | 0·57 |
| Green tea | 408·0 | 204·0–690·9 | 460·5 | 253·3–625·5 | 0·48 |
| Black and oolong tea | 77·8 | 1·8–328·3 | 29·0* | 3·0–134·2 | 0·65 |
| Coffee | 39·2 | 0·0–180·9 | 65·1** | 16·1–163·3 | 0·67 |
| Soft drinks | 8·4 | −2·7–61·8 | 5·3 | −2·5–13·2 | 0·44 |
| Fish and shellfish | 81·1 | 59·0–104·9 | 85·9 | 68·2–115·1 | 0·38 |
| Meats | 60·3 | 40·2–78·9 | 60·5 | 44·6–75·5 | 0·22 |
| Eggs | 34·8 | 15·9–52·8 | 44·5*** | 25·3–65·5 | 0·47 |
| Dairy products | 173·3 | 76·0–233·6 | 154·6 | 101·3–208·3 | 0·55 |
IQR, interquartile range.
Significant differences between the DR and BDHQ: *P<0·05, **P<0·01, ***P<0·001 (Wilcoxon signed-rank test).
Energy adjustment was performed according to the residual method.
The Bland–Altman plots for energy and macronutrients are shown in Fig. 2 and the online supplementary material, Supplemental Fig. 1. Poor agreement was observed for the intakes of energy and each nutrient at the individual level.
Fig. 2.
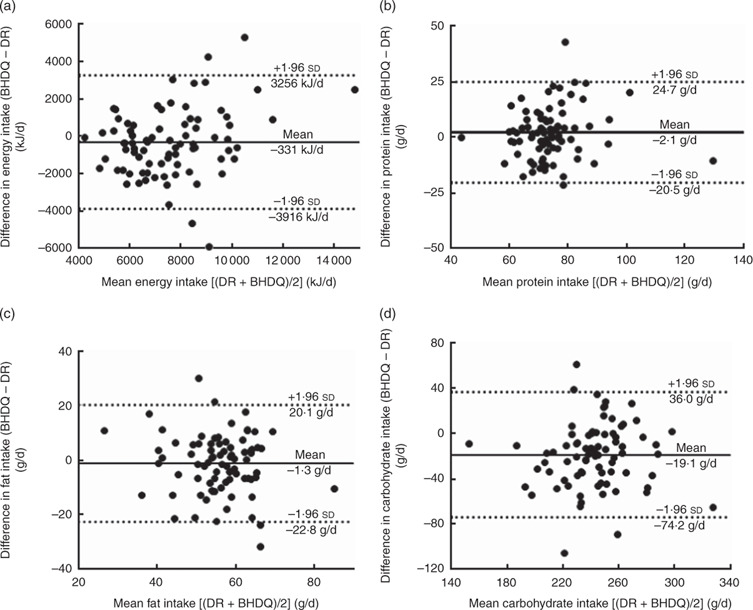
Bland–Altman plots for agreement between energy and energy-adjusted macronutrient intakes estimated using the three-day semi-weighed dietary records (DR) and the brief-type self-administered diet history questionnaire (BDHQ) among eighty very old Japanese men and women (aged 80 years or older), June–August 2012 and June 2015–February 2016. The difference in intake between the two methods is plotted v. the mean intake from the two methods for: (a) energy; (b) protein; (c) fat; (d) carbohydrate. —— represents the mean difference (bias) and · · · represent the limits of agreement. Energy adjustment was performed according to the residual method
Discussion
The present study examined the relative validity among very old Japanese of the intakes of energy, forty-three nutrients and twenty-seven food groups as estimated by the BDHQ by comparing these values with the three-day DR as a reference. Relatively acceptable correlations were obtained for both nutrient and food group intakes between the DR and the BDHQ. The BDHQ may have the potential to rank individuals regarding dietary intakes among very old populations. Meanwhile, the intakes of approximately half (40–70 %) of the nutrients and food groups estimated by the BDHQ were significantly different from those estimated by the DR. For some nutrients and food groups, it may be difficult to use the BDHQ to accurately estimate representative intakes among very old Japanese populations as well as among adults aged 31–76 years( 15 , 16 ).
The median values of Spearman’s correlation coefficient were 0·39–0·46 for nutrients and 0·45–0·48 for food groups. Regarding the food groups, a previous study showed that the median values of Spearman’s correlation coefficient for adults were 0·48 for men and 0·44 for women( 15 ). The present study among the very old population showed median correlation values comparable to those of middle-aged adults. There are several reasons why the correlation between the BDHQ and the DR for very old populations was comparable to that for middle-aged adult populations. First, all our participants may be very healthy and active according to daily steps( 25 ). The food portion sizes consumed by our participants, as derived from the DR, might have little variety. Second, our participants might be sufficiently able to recall their diet during the preceding month. Although the MMSE or MoCA-J values for our participants were 3 or 6 years old, the values were relatively higher than those obtained from other studies among community-dwelling, very old Japanese( 26 , 27 ). Our participants might answer the BDHQ and conduct the DR with an appropriate level of consistency. Third, our participants answered the BDHQ verbally. This prevented the participants from becoming either tired or bored when answering the BDHQ. Further, verbal and courtesy questions from the staff may have helped the participants answer the BDHQ accurately. Meanwhile, for nutrient intakes, the median values of Spearman’s correlation coefficient among our participants (0·39–0·46) might be slightly lower than the medians of Pearson’s correlation coefficient in the previous validation study of adults (0·34–0·51 for men and 0·40–0·49 for women)( 16 ). These results may imply that different kinds of food items may be consumed by middle-aged Japanese and very old Japanese even if the same food groups were consumed. Unfortunately, these different correlation coefficients (i.e. Spearman’s and Pearson’s) could not be simply compared.
We compared the present results with those of previous validation studies that targeted very old populations. However, these studies included not only participants aged 80 years or older but also those aged 60–80 years( 28 – 35 ). One review study, where most of the participants were aged 65 years or older, defined the mean correlation coefficient values for micronutrients of 0·30–0·50, 0·51–0·70 and >0·7 as acceptable, good and very good correlation, respectively( 35 ). In applying the same definition, our present study showed that almost all macronutrients had acceptable (82–88 %) or good (12–18 %) correlation. Many of the micronutrients (54–77 %) achieved acceptable correlation and 15–19 % nutrients achieved good correlation. Most of the food groups showed acceptable (48–52 %), good (33–41 %) or very good (0–4 %) correlation. These results may indicate that the BDHQ is useful for ranking in terms of most of the dietary variables. However, the correlation coefficients of some micronutrients, such as retinol, vitamin D, cryptoxanthin and thiamin, were low. We should treat the intakes of these nutrients estimated from the BDHQ carefully in an epidemiological study.
For food group intakes in the present study, the intakes of bread, potatoes and confectioneries estimated from the BDHQ were significantly higher and those of rice and sugar were significantly lower compared with the DR. Meanwhile, energy and carbohydrate intakes estimated from the BDHQ were lower than the DR estimates, although bread, potatoes and confectioneries were assumed to be high-energy-density foods. Since rice is the first contributor of energy (35 % for men and 29 % for women) and carbohydrate (55 and 43 %) among the Japanese population( 36 ), the low estimation of rice from the BDHQ may affect the low estimation for energy and carbohydrate from the BDHQ. Further, the BDHQ estimated fruit and vegetable intakes to be reasonably consistent with those from the DR. However, many of the micronutrients did not estimate well from the BDHQ. To estimate dietary intakes among very old Japanese by the BDHQ more accurately in the future, determining the portion size of rice and reconsidering the food code assigned to food items in the BDHQ might be the most immediate priorities.
The strength of the present study was that we conducted multiple semi-weighed DR with a very old population aged 80 years or older. To collect dietary information from the participants as accurately as possible, the research staff visited each participant’s home on the day following each recording day, reviewed the record and asked for clarification on unclear points face-to-face.
Several limitations of the present study warrant mention. First, our participants might be extremely healthy. Daily steps and the cognitive function of our participants may be relatively high compared with other very old, community-dwelling Japanese( 25 – 27 ). Further, the participants may have high health consciousness, given that all of them completed this time-consuming survey. Therefore, the results obtained from the present study cannot be readily extrapolated to the general very old Japanese population. However, the scores of the BI, MMSE and MoCA-J, and the prevalence of the history of chronic diseases did not differ significantly from those of the original cohort of TOOTH and SONIC, although our participants may be slightly healthier than the participants of the original cohort. These results may indicate that the BDHQ can be used not only for the present participants but also for those in the original TOOTH and SONIC studies. Second, we mainly conducted analysis using the combined data of men and women, not by sex, because the number of participants was not large enough( 37 ). However, we examined the validity of the BDHQ for energy-adjusted intakes as well as crude intakes. Although men had higher energy intakes than women, the effect of the different energy intake by sex was attenuated by using energy-adjusted values in the present study. Further, many other validation studies for dietary questionnaires among elderly populations used combined data of men and women and examined a similar number of subjects( 30 – 32 , 34 , 35 ). These results may provide support for our methods of analysis as acceptable and valid. Although we also examined the validity of the BDHQ by sex as reference, we thought that more participants were needed to conclude the sex-specific result. Third, in the present study, our participants answered the BDHQ verbally. This method may help our participants answer the BDHQ easily and in a more focused manner. If the participants wrote down the answers to the questionnaire by themselves, the validity of the BDHQ may be lower. Fourth, we used the DR as a reference and assumed that dietary intakes derived from the DR were accurate. Although the relative validity in the present study relied on the extent to which the DR is accurate, a DR is susceptible to measurement error because of erroneous recording and potential changes in eating behaviour. However, errors in the DR are thought to have lower correlation with errors in the BDHQ compared with other dietary assessment methods that rely on memory( 13 ). Further, family’s or helper’s support to record the DR (about thirty participants) and our face-to-face checking of records on the day following each recording day may have been helpful in obtaining accurate dietary information of our participants. Meanwhile, biomarkers are a better standard for some nutrients and any errors in such markers are independent of errors in the questionnaires. A validation study for some nutrients using 24 h urine collection as a reference among very old Japanese is also needed in the future. Fifth, we did not consider the supplement intakes in calculating nutrient intakes from the DR and the BDHQ. Although the BDHQ asks about the use of dietary supplements, the types and the quantity of the supplements were not queried. Even if the BDHQ asks about supplement intake, we cannot consider the intake of supplements in the calculation because of a lack of a reliable food composition table for dietary supplements in Japan. A previous study showed that the omission of dietary supplements might alter the estimation of nutrient intakes among elderly populations( 38 ). The intakes of some nutrients described in the present study might therefore be underestimated. Also, the validity of the BDHQ for some nutrients might have been altered if nutrient intakes derived from dietary supplements were added to the DR. Sixth, because of no reliable data on the food portion size among very old populations, the BDHQ calculated dietary intakes using general adult portions. This may make it more difficult to estimate accurate dietary intakes among very old populations than among other age groups of adults. Finally, we conducted the DR for only three days. A previous study showed that estimating usual intakes among adults with 95 % CI with a deviation within 20 % required measurements for more than three days for almost all nutrients( 37 ). A long-term DR is therefore more appropriate for reference. However, a three-day DR was thought to be more feasible because of the considerable burden placed on very old participants for recording such information. Meanwhile, seasonality on the validity of the BDHQ was not considered in the present study. However, the seasonality of the validity of a comprehensive diet history questionnaire (DHQ), from which the BDHQ was developed, showed that to rank individuals by nutrient intake is acceptable for epidemiological studies regardless of season, even though the estimated nutrient intakes in one season should not be interpreted as yearly average intakes( 39 ). That previous study might be helpful for interpreting the seasonality of the BDHQ.
Conclusion
In conclusion, the present study showed that the BDHQ provided acceptable Spearman’s correlation coefficients for the intakes of nutrients and food groups examined, using a three-day DR as a reference, among the very old participants who participated in the TOOTH and SONIC studies. The present results indicated that the BDHQ is a good candidate for dietary assessment in epidemiological studies among very old Japanese. Meanwhile, accurate median dietary intakes among the population could not be estimated for some nutrients and food groups, which is one of the present limitations for usefulness of the BDHQ. Reconsidering food portion size to calculate dietary intakes in the BDHQ is necessary when estimating dietary intakes accurately among the general very old population. Further efforts to enhance the validity of the BDHQ for very old populations are needed.
Acknowledgements
Acknowledgements: The authors would like to thank all the participants for their participation in this time-consuming research. They would also like to express their appreciation for the support of the dietitians on the research staff: Chisa Katsuragi, Nana Kimoto, Nanako Koe, Kazuyo Shozawa, Yuko Sunami and Tomono Yahata. Financial support: This study was supported by a grant from the medical–welfare–food–agriculture collaborating consortium project from the Japan Ministry of Agriculture, Forestry, and Fisheries, and a grant from the Foundation for Total Health Promotion. The funding agencies had no role in the design, analysis or writing of this article. Conflict of interest: Y.Ar. received research grant funding from Daiichi-Sankyo Company, Limited, a pharmaceutical company. The funder did not provide the grant to this article and had no role in the design, analysis or writing of this article. The remaining authors declare that they have no financial disclosures. Authorship: S.S. designed and directed the study. Y.O., T.H., M.T., Y.Ar., Y.M. and T.I. contributed to the coordination of the fieldwork and recruitment for the study. S.K. and Y.O. arranged the fieldwork. S.K., Y.O., T.H., M.T. and Y.Ar. conducted fieldwork and data collection. S.K. and X.Y. performed the statistical analyses. Y.Ab., Y.Ar. and Y.M. supported data analyses. S.K. drafted the manuscript. All authors provided input into the final draft of the manuscript. Ethics of human subject participation: The protocol of this study was approved by the Ethics Committee of the Keio University School of Medicine (approval number 2011276; approved on 26 December 2011), the University of Tokyo Faculty of Medicine (approval number 10828; approved on 12 June 2015) and the Tokyo Metropolitan Geriatric Hospital and Institute of Gerontology (approval number H27-18; approved on 9 July 2015). Written informed consent was obtained from all participants.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980018002331.
click here to view supplementary material
References
- 1. National Institute on Aging, National Institutes of Health, US Department of Health and Human Services & World Health Organization (2011) Global health and ageing. http://www.who.int/ageing/publications/global_health/en/ (accessed October 2017).
- 2. Mendonca N, Hill TR, Granic A et al. (2016) Macronutrient intake and food sources in the very old: analysis of the Newcastle 85+ Study. Br J Nutr 115, 2170–2180. [DOI] [PubMed] [Google Scholar]
- 3. Mendonca N, Hill TR, Granic A et al. (2016) Micronutrient intake and food sources in the very old: analysis of the Newcastle 85+ Study. Br J Nutr 116, 751–761. [DOI] [PubMed] [Google Scholar]
- 4. Wham C, Teh R, Moyes SA et al. (2016) Macronutrient intake in advanced age: Te Puawaitanga o Nga Tapuwae Kia ora Tonu, Life and Living in Advanced Age: A Cohort Study in New Zealand (LiLACS NZ). Br J Nutr 116, 1103–1115. [DOI] [PubMed] [Google Scholar]
- 5. Adamson AJ, Collerton J, Davies K et al. (2009) Nutrition in advanced age: dietary assessment in the Newcastle 85+ study. Eur J Clin Nutr 63, Suppl. 1, S6–S18. [DOI] [PubMed] [Google Scholar]
- 6. Volkert D, Kreuel K, Heseker H et al. (2004) Energy and nutrient intake of young-old, old-old and very-old elderly in Germany. Eur J Clin Nutr 58, 1190–1200. [DOI] [PubMed] [Google Scholar]
- 7. Ferry M, Hininger-Favier I, Sidobre B et al. (2001) Food and fluid intake of the SENECA population residing in Romans, France. J Nutr Health Aging 5, 235–237. [PubMed] [Google Scholar]
- 8. Bates CJ, Prentice A & Finch S (1999) Gender differences in food and nutrient intakes and status indices from the National Diet and Nutrition Survey of people aged 65 years and over. Eur J Clin Nutr 53, 694–699. [DOI] [PubMed] [Google Scholar]
- 9. Cabinet Office, Government of Japan ( 2017) White paper on aging society, 2017 (in Japanese). http://www.8.cao.go.jp/kourei/whitepaper/w-2017/zenbun/29pdf_index.html (accessed October 2017).
- 10. Ministry of Internal Affairs and Communication (2017) Japanese elderly populations from the statistics, 2017 (in Japanese). http://www.stat.go.jp/data/topics/topi1030.htm (accessed October 2017).
- 11. Takayama M, Arai Y, Sasaki S et al. (2012) Association of marine-origin n-3 polyunsaturated fatty acids consumption and functional mobility in the community-dwelling oldest old. J Nutr Health Aging 17, 82–89. [DOI] [PubMed] [Google Scholar]
- 12. Osawa Y, Arai Y, Takayama M et al. (2017) Identification of dietary patterns and their relationships with general and oral health in the very old. Asia Pac J Clin Nutr 26, 262–270. [DOI] [PubMed] [Google Scholar]
- 13. Willett W (2013. ) Nutritional Epidemiology , 3rd ed. New York: Oxford University Press. [Google Scholar]
- 14. Cade JE, Burley VJ, Warm DL et al. (2004) Food-frequency questionnaires: a review of their design, validation and utilisation. Nutr Res Rev 17, 5–22. [DOI] [PubMed] [Google Scholar]
- 15. Kobayashi S, Murakami K, Sasaki S et al. (2011) Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16d dietary records in Japanese adults. Public Health Nutr 14, 1200–1211. [DOI] [PubMed] [Google Scholar]
- 16. Kobayashi S, Honda S, Murakami K et al. (2012) Both comprehensive and brief self-administered diet history questionnaires satisfactorily rank nutrient intakes in Japanese adults. J Epidemiol 22, 151–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Tooze JA, Vitolins MZ, Smith SL et al. (2007) High levels of low energy reporting on 24-hour recalls and three questionnaires in an elderly low-socioeconomic status population. J Nutr 137, 1286–1293. [DOI] [PubMed] [Google Scholar]
- 18. Arai Y, Iinuma T, Takayama M et al. (2010) The Tokyo Oldest Old survey on Total Health (TOOTH): a longitudinal cohort study of multidimensional components of health and well-being. BMC Geriatr 10, 35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ryuno H, Kamide K, Gondo Y et al. (2016) Differences in the association between high blood pressure and cognitive functioning among the general Japanese population aged 70 and 80 years: the SONIC study. Hypertens Res 39, 557–563. [DOI] [PubMed] [Google Scholar]
- 20. Ministry of Health, Labour, and Welfare (2017) The National Health and Nutrition Survey in Japan, 2015. Tokyo: Ministry of Health, Labour, and Welfare (in Japanese). [Google Scholar]
- 21. Sasaki S, Yanagibori R & Amano K (1998) Self-administered diet history questionnaire developed for health education: a relative validation of the test-version by comparison with 3-day diet record in women. J Epidemiol 8, 203–215. [DOI] [PubMed] [Google Scholar]
- 22. Science and Technology Agency (2010) Standard Tables of Food Composition in Japan, 2010. Tokyo: Ministry of Education, Culture, Sports, Science and Technology; (in Japanese). [Google Scholar]
- 23. Bland JM & Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1, 307–310. [PubMed] [Google Scholar]
- 24. Arai Y, Martin-Ruiz CM, Takayama M et al. (2015) Inflammation, but not telomere length, predicts successful ageing at extreme old age: a longitudinal study of semi-supercentenarians. EBioMedicine 2, 1549–1558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Tudor-Locke C, Craig CL, Aoyagi Y et al. (2011) How many steps/day are enough? For older adults and special populations. Int J Behav Nutr Phys Act 8, 80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Narazaki K, Nofuji Y, Honda T et al. (2013) Normative data for the Montreal cognitive assessment in a Japanese community-dwelling older population. Neuroepidemiology 40, 23–29. [DOI] [PubMed] [Google Scholar]
- 27. Sakuma N, Ura C, Miyamae F et al. (2017) Distribution of Mini-Mental State Examination scores among urban community-dwelling older adults in Japan. Int J Geriatr Psychiatry 32, 718–725. [DOI] [PubMed] [Google Scholar]
- 28. Rosilene WV, Cumming R, Travison T et al. (2015) Relative validity of a diet history questionnaire against a four-day weighed food record among older men in Australia: the Concord Health and Ageing in Men Project (CHAMP). J Nutr Health Aging 19, 603–610. [DOI] [PubMed] [Google Scholar]
- 29. Talegawkar SA, Tanaka T, Maras JE et al. (2015) Validation of nutrient intake estimates derived using a semi-quantitative FFQ against 3 day diet records in the Baltimore Longitudinal Study of Aging. J Nutr Health Aging 19, 994–1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Shatenstein B & Payette H (2015) Evaluation of the relative validity of the short diet questionnaire for assessing usual consumption frequencies of selected nutrients and foods. Nutrients 7, 6362–6374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Eysteinsdottir T, Thorsdottir I, Gunnarsdottir I et al. (2012) Assessing validity of a short food frequency questionnaire on present dietary intake of elderly Icelanders. Nutr J 11, 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Mitchell DC, Tucker KL, Maras J et al. (2012) Relative validity of the Geisinger Rural Aging Study food frequency questionnaire. J Nutr Health Aging 16, 667–672. [DOI] [PubMed] [Google Scholar]
- 33. Huang YC, Lee MS, Pan WH et al. (2011) Validation of a simplified food frequency questionnaire as used in the Nutrition and Health Survey in Taiwan (NAHSIT) for the elderly. Asia Pac J Clin Nutr 20, 134–140. [PubMed] [Google Scholar]
- 34. Henn RL, Fuchs SC, Moreira LB et al. (2010) Development and validation of a food frequency questionnaire (FFQ-Porto Alegre) for adolescent, adult and elderly populations from Southern Brazil. Cad Saude Publica 26, 2068–2079. [DOI] [PubMed] [Google Scholar]
- 35. Ortiz-Andrellucchi A, Sanchez-Villegas A, Doreste-Alonso J et al. (2009) Dietary assessment methods for micronutrient intake in elderly people: a systematic review. Br J Nutr 102, Suppl. 1, S118–S149. [DOI] [PubMed] [Google Scholar]
- 36. Sasaki S, Takahashi T, Iitoi Y et al. (2003) Food and nutrient intakes assessed with dietary records for the validation study of a self-administered food frequency questionnaire in JPHC Study Cohort I. J Epidemiol 13, 1 Suppl ., S23–S50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Fukumoto A, Asakura K, Murakami K et al. (2013) Within- and between-individual variation in energy and nutrient intake in Japanese adults: effect of age and sex differences on group size and number of records required for adequate dietary assessment. J Epidemiol 23, 178–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Fabian E, Bogner M, Kickinger A et al. (2012) Vitamin status in elderly people in relation to the use of nutritional supplements. J Nutr Health Aging 16, 206–212. [DOI] [PubMed] [Google Scholar]
- 39. Suga H, Asakura K, Sasaki S et al. (2014) Effect of seasonality on the estimated mean value of nutrients and ranking ability of a self-administered diet history questionnaire. Nutr J 13, 51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980018002331.
click here to view supplementary material