

Abstract
Purpose
This study was performed to compare outcomes of the Trochanteric Fixation Nail (TFN®) with a helical blade versus TFN® with a femoral neck screw for the treatment of intertrochanteric femoral fractures.
Materials and Methods
A single center, retrospective cohort study. Patients (>18 years of age) with an intertrochanteric femoral fracture, who were operated on between January 1, 2012 and December 31, 2016 were included. Primary and secondary outcome measures were cut-out rate and intervention variables, respectively. Data from X-ray examinations and patient medical files were collected and analyzed. The chi-square test or Student's t-test were used for statistical analysis.
Results
A total of 631 patients were surgically treated for an intertrochanteric femoral fracture. Of this group, 239 patients (37.9%) were treated with a TFN® with helical blade and 392 patients (62.1%) with a TFN® with femoral neck screw. There were no statistically significant differences between the baseline characteristics of both groups. A total of 17 (2.7%) cut-outs were recorded, with no statistically significant difference between the two groups (P=0.19). Additionally, there were no statistically significant differences in the secondary outcome measures between the two groups.
Conclusion
There are no statistically significant differences in primary and secondary outcomes following treatment of intertrochanteric femur fracture with the TFN® helical blade or TFN® femoral neck screw. These findings suggest that the choice of collum implant for the surgical treatment of intertrochanteric femur fractures cannot be made based on the surgical outcomes of the two implants evaluated here.
Keywords: Hip fractures, Trochanteric fixation nail, Helical blade, Femoral neck screw, Cut-out
INTRODUCTION
With an aging population, the number of intertrochanteric femoral fractures treated each year continues to rise. In 2014, 16,000 people in the Netherlands were registered with a hip fracture1,2). Of these, roughly 14,000 were caused by a fall and three quarters of the patients were older than 80 years. The distribution between men and women was 1:3. Twenty-five percent of patients with a hip fracture are left permanently disabled and 25% die within the first year. Approximately 50% of the patients with a hip fracture can return to their own home environment after hospitalization1,3). The total annual costs of all hip fractures in the Netherlands are estimated to be €300 million1,3,4).
Operative treatment of a hip fracture remains the best option as it helps create an anatomical reduction of the fracture, stable fixation, and maintenance of blood supply, thereby providing an opportunity for early and full weight bearing with mobilization. As a result, the postoperative risks from immobilization—e.g., deep vein thrombosis and airway problems-sharply decrease1,5).
The helical blade received regulatory approval in 2005 and was designed to provide stronger fixation through impaction of the cancellous bone which should increase resistance to cut-out6,7). However, several randomized controlled trials comparing helical blade with the lag screw in intramedullary fixations have demonstrated greatly different outcomes compared with published data and theoretical concepts7,8,9,10,11,12).
The choice of implant used for surgical treatment of intertrochanteric femoral fractures depends on the surgeons' preference, not on empirical data or indication. Within the Department of Trauma Surgery, no consensus exists regarding the type of collum implant to be used in when surgically treating patients with an intertrochanteric femoral fracture.
This study aimed to assess if there were any differences in outcomes (i.e., cut-out and/or interventional variables) between a the Trochanteric Fixation Nail (TFN®; Synthes, Raynham, MA, USA) with helical blade and a TFN® with femoral neck screw when applied to surgical treatment of intertrochanteric femoral fractures.
MATERIALS AND METHODS
1. Inclusion/Exclusion Criteria
Within the Trauma Department at our institution, it was decided that surgeons would use TFN® for osteosyntheses of intertrochanteric femoral fractures. The surgeon could choose between a helical blade and femoral neck screw (“lag screw”) for the collum implant. Patients were included if they: i) were older than eighteen years of age, ii) had pre- and postoperative X-ray diagnostics available, and iii) were treated by/under direct supervision of a trauma surgeon. Candidates were excluded if they had a pathologic fracture, prior hip surgery on the ipsilateral side, additional fractures or an incorrectly registered operation code.
The cohort included those identified using the operation code 38535 (femur # intertrochanteric, TFN) from the digital registration system. The study group was comprised of 685 patients with an intertrochanteric femoral fracture treated with a TFN® with helical blade or a TFN® with femoral neck screw between January 1,2012 and December 31, 2016. A total of 631 patients where included in the study; 54 were excluded on the basis of a wrongly registered operation code after reassessment of the preoperative X-ray images (Fig. 1).
Fig. 1. Flowchart inclusion/exclusion. TFN®: Trochanteric Fixation Nail (Synthes, Raynham, MA, USA).

The study was approved by the local ethics committee of the Albert Schweitzer Hospital. Signed informed consent forms allowing use of medical records for research purposes were obtained from all patients.
2. Outcome Measures
Mechanical complications (e.g., axial migration, axial cutout, lateral cut-out, non-union, periprothestic fracture, unacceptable position, mechanical complications with a tip-apex distance [TAD] <15 mm or >25 mm)4,13) were obtained from available post-operative X-ray examinations. Axial migration was considered a normal phenomenon due to collapsing of the fracture until sufficient stability was achieved4,13,14). Intervention variables (i.e., TAD, surgery time, position of the collum implant [according to the Cleveland index as shown in Fig. 2]15), weight bearing prescriptions, length of stay, discharge destination after the hospital, postsurgical complications), were obtained from the medical records of electronic patient files. The TAD was calculated (Fig. 3) on the first post-operative X-ray for each patient as described by Baumgaertner et al.14). All measurements were performed by a single investigator, and 10% of his findings were double-checked by a trauma surgeon.
Fig. 2. Cleveland index.
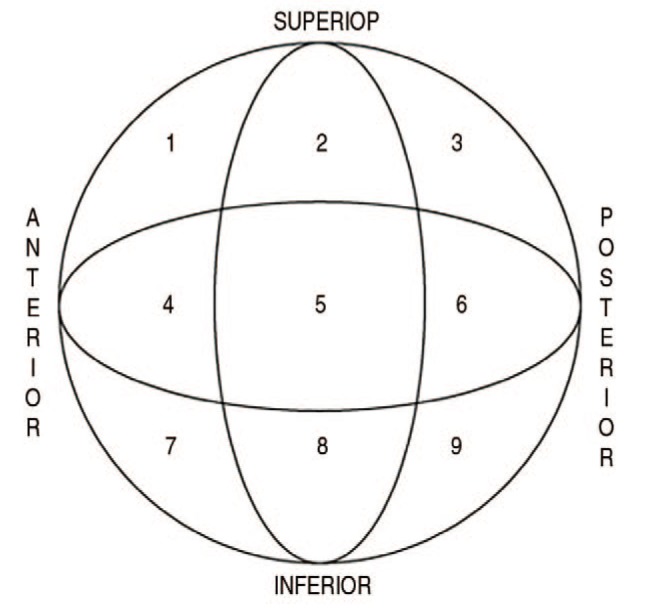
Fig. 3. Calculation of the tip-apex distance (TAD).

AP: anteroposterior; Lat, lateral.
Fractures were classified using the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification and classified as stable (31-A1) or unstable (31-A2) (Appendix 1)16).
4. Statistical Analysis
Statistical analysis was performed using Statistic Package for Social Sciences (SPSS) version 24.0 (IBM Corp., Armonk, NY, USA). Differences were considered to be statistically signiflcant when P<0.05. The chi-square test was used to compare differences between the two groups for each variable, and the Student's t-test was used for quantitative variables.
RESULTS
In total, 631 patients were treated surgically for an intertrochanteric femoral fracture. Of these, 239 (37.9%) were treated with a TFN® with helical blade and 392 (62.1%) with a TFN® with femoral neck screw (Fig. 1). The baseline characteristics demonstrated no statistically significant differences between the groups (Table 1); patients had a mean follow up of one year. The average age in each group was 81 years old and 76.1% were female. According to the AO/OTA classification 56.4% were classified as unstable fractures. There was no statistically significant difference (P=0.98) in the proportion of fractures that were unstable between the helical blade and femoral neck screw, helical blade 135 (56.5%), femoral neck screw 221 (56.4%), respectively.
Table 1. Baseline Characteristics and Demographic Data.
| Variable | Total (n=631) | Blade (n=239) | Screw (n=392) | P-value |
|---|---|---|---|---|
| Collum implant | 631 (100) | 239 (37.9) | 392 (62.1) | |
| Sex | 0.73 | |||
| Female | 480 (76.1) | 180 (75.3) | 300 (76.5) | |
| Male | 151 (23.9) | 59 (24.7) | 92 (23.5) | |
| Age (yr) | 81.83±11.47 | 82.53±10.29 | 81.40±12.13 | 0.67 |
| Body mass index (kg/m2) | 24.37±4.69 | 24.61±4.99 | 24.23±4.51 | 0.89 |
| Affected side | 0.14 | |||
| Left | 328 (52.0) | 115 (48.1) | 213 (54.3) | |
| Right | 303 (48.0) | 124 (51.9) | 179 (45.7) | |
| Fracture | 0.98 | |||
| Stable (31-A1) | 275 (43.6) | 104 (43.5) | 171 (43.6) | |
| Unstable (31-A2) | 356 (56.4) | 135 (56.5) | 221 (56.4) | |
| ASA classification* (n) | 533 | 205 | 328 | 0.46 |
| ASA 1 | 27 (5.1) | 10 (4.9) | 17 (5.2) | |
| ASA 2 | 196 (36.8) | 71 (34.6) | 125 (38.1) | |
| ASA 3 | 295 (55.3) | 121 (59.0) | 174 (53.0) | |
| ASA 4 | 15 (2.8) | 3 (1.5) | 12 (3.7) |
Values are presented as number (%), mean±stadard deviation, or number only.
ASA: American Society of Anesthesiologists.
*Refer to Appendix 2.
An assessment of the primary outcome measure (i.e., cut-out) revealed that a total of 42 (6.7%) mechanical complications were recorded (axial cut-out, lateral cutout, non-union, periprothestic fracture or unacceptable position). A total of 17 (2.7%) cut-outs were recorded in both groups combined (helical blade 9 cut-outs, 3.8%; femoral neck screw 8 cut-outs, 2.0%; P=0.19) (Table 2). There was no statistically significant difference between the two groups when assessing the primary outcome (P=0.19). Also, no statistically significant difference existed in TAD (<15 mm or >25 mm) related to mechanical complications (helical blade 8, 3.3%; femoral neck screw 8, 2.0%; P=0.454). A total of 221 patients (35.0%) experienced axial migration of their collum implant (helical blade 78, 32.6%; femoral neck screw, 143; 36.5%; P=0.296).
Table 2. Mechanical Complications.
| Variable | Total (n=631) | Blade (n=239) | Screw (n=392) | P-value |
|---|---|---|---|---|
| Total mechanical complications | 264 (41.8) | 97 (40.6) | 167 (42.6) | |
| Axial migration | 222 (35.2) | 78 (32.6) | 143 (36.5) | 0.30 |
| Axial cut-out | 8 (1.3) | 5 (2.1) | 3 (0.8) | 0.16 |
| Lateral cut-out | 9 (1.4) | 4 (1.7) | 5 (1.3) | 0.74 |
| Non-union | 10 (1.6) | 5 (2.1) | 5 (1.3) | 0.52 |
| Periprothestic fracture | 7 (1.1) | 1 (0.4) | 6 (1.5) | 0.26 |
| Avascular head necrosis | 2 (0.3) | 1 (0.4) | 1 (0.3) | 1 |
| Unacceptable position of the fracture/osteosyntheses | 1 (0.2) | 1 (0.4) | 0 (0) | 0.38 |
| Other | 5 (0.8) | 2 (0.8) | 3 (0.8) | 1 |
| TAD < 15 mm with mechanical complications | 4 (0.6) | 1 (0.4) | 3 (0.8) | 0.45 |
| TAD > 25 mm with mechanical complications | 12 (1.9) | 7 (2.9) | 5 (1.3) |
Values are presented as number (%).
TAD: tip-apex distance.
There were also no statistically significant differences among the secondary outcome measures between the two groups (Table 3, 4). The positions of the collum implant within the femoral head were evenly divided between the helical blade and screw groups; as shown in Fig. 4, 74.5% were placed in the optimal position (i.e., central in the femoral head, corresponding with position 5 in the Cleveland index) in each group. Post-operative complications were experienced by 605 out of 631 patients. The three most common postoperative complications were low hemoglobin for which transfusion was required (169/605 patients, 27.9%), delirium (129/605 patients, 21.3%) and urinary tract infection (72/605 patients, 11.9%).
Table 3. Secondary Outcome Measures.
| Variable | Total (n=631) | Blade (n=239) | Screw (n=392) | P-value |
|---|---|---|---|---|
| Tip-apex distance (n=558)* | 22.84±9.91 | 23.39±7.96 | 21.71±7.21 | 0.45 |
| Surgery time (min) | 99±29.73 | 94±30.82 | 92±29.04 | 0.27 |
| Cleveland position | 0.70 | |||
| 5 position | 470 (74.5) | 176 (73.6) | 294 (75.0) | |
| Other positions | 161 (25.5) | 063 (26.4) | 98 (25.0) | |
| Weight bearing | 0.19 | |||
| Full | 585 (92.7) | 226 (94.6) | 359 (91.6) | |
| Partial | 25 (4.0) | 5 (2.1) | 20 (5.1) | |
| Non | 6 (1.0) | 1 (0.4) | 5 (1.3) | |
| Unknown | 2 (0.3) | 1 (0.4) | 1 (0.3) | |
| Length of stay (day), (n=604)* | 8.1±5.58 | 7.5±4.45 | 8.5±6.63 | 0.52 |
| Discharge facility | 0.29 | |||
| Return to home | 193 (30.6) | 73 (30.5) | 120 (30.6) | |
| Temporary rehabilitation | 407 (64.5) | 153 (64.0) | 254 (64.8) | |
| Permanent nursing home | 5 (0.8) | 2 (0.8) | 3 (0.8) | |
| Unknown discharge facility | 5 (0.8) | 4 (1.7) | 1 (0.3) |
Values are presented as number (%) or mean±stadard deviation.
*Due to incomplete patient data.
Table 4. Postoperative Complications.
| Complication | Total (n=605) | Blade (n=228) | Screw (n=377) | P-value |
|---|---|---|---|---|
| Delirium | 129 (21.3) | 53 (23.2) | 76 (20.2) | 0.42 |
| Urinary tract infection | 72 (11.9) | 31 (13.6) | 41 (10.9) | 0.37 |
| Thrombosis leg | 1 (0.2) | 0 (0) | 1 (0.3) | 1 |
| Postoperative fall | 3 (0.5) | 1 (0.4) | 2 (0.5) | 1 |
| Vascular event | 0.79 | |||
| TIA | 5 (0.8) | 1 (0.4) | 4 (1.1) | |
| CVA | 4 (0.7) | 1 (0.4) | 3 (0.8) | |
| MI | 7 (1.2) | 3 (1.3) | 4 (1.1) | |
| Atrial fibrillation | 20 (3.3) | 7 (3.1) | 13 (3.4) | 1 |
| Wound infection | 3 (0.5) | 0 (0) | 3 (0.8) | 0.29 |
| Postoperative bleeding | 8 (1.3) | 5 (2.2) | 3 (0.8) | 0.16 |
| Pneumonia | 34 (5.6) | 14 (6.1) | 20 (5.3) | 0.72 |
| Ileus | 2 (0.3) | 1 (0.4) | 1 (0.3) | 1 |
| Death | 24 (4.0) | 8 (3.5) | 16 (4.2) | 0.83 |
| Low Hb for which transfusion | 169 (27.9) | 63 (27.6) | 106 (28.1) | 0.85 |
Values are presented as number (%).
TIA: transient ischemic attack, CVA: cerebral vascular accident; MI: myocardial infarction, Hb: hemoglobin.
Fig. 4. Collum implant position according to the Cleveland index.

DISCUSSION
1. Mechanical Complications
When comparing outcomes associated with the use of helical blades and femoral neck screws for the surgical treatment of intertrochanteric femoral fractures, we observed no statistically significant differences in the frequency of cut-out or other mechanical complications. Axial migration may be an early symptom of cut-out, and in this study, the high number of axial migration events was considered a functional phenomenon as part of the physiological collapse of the fracture to obtain (sufficient) stability and a prerequisite for optimal bone healing. All figures from this study were in accordance with the figures found in recent literature7,13,17,18,19). In our study, the total percentage of mechanical complications (i.e., 6.7%) was lower than what is reported (i.e., 16–23%) in different studies20). One reason for this could be the differentiation within the surgical department. The trauma surgeons operate on greater than 75.3% of the intertrochanteric femoral fractures, thus developing a high level of competence in this type of operation.
2. Intervention Variables
For all intervention variables tested, we observed no statistically significant differences among the two treatment groups. An increased risk of mechanical complications according to the literature occurs at a TAD of <15 mm or >25 mm4,13). The disadvantage of TAD measurements is that they are made using the first postoperative X-ray images. In patients with a TAD of <15 mm or >25 mm, an expectative policy will be maintained with regard to re-operation of the patient and the clinical condition of the patient will lead treatment decisions. The increased risk of mechanical complications described in the literature with a TAD of <15 mm or >25 mm was not observed in this study1,14,21). For the time being, the value of the TAD used in research and how these values are reflective of clinical outcomes remain open for discussion.
This study revealed no difference in postoperative complications between helical blade and femoral neck screws when used to surgically treat intertrochanteric femoral fractures. The actual number of postoperative complications will most likely be much higher since postoperative complications were only identified using data relating to the clinical admission of the patient. Also, postoperative complications are typically underreported and a subset of patients will develop a postoperative complication (e.g., delirium) after discharge from the hospital. Postoperative complications that were treated and resolved during admission and were no longer topical at discharge were often not mentioned in the discharge letter and therefore not reported.
3. Strengths and Weaknesses of the Research
The strengths of this research were that it evaluated patients treated over a five year time frame; all patients who received surgical treatment for an intertrochanteric femoral fracture using a TFN® with helical blade or femoral neck screw were included.
Weaknesses of this research include: i) underreporting of variables that could not be included in the analyses (e.g., blood loss), ii) underreporting of analyzed data, which led to missing data (especially in the registration of postoperative complications), and iii) surgeries were not all performed by the same trauma surgeon. All operators had the skills to place a TFN® with femoralneck screw, however, only three had the skills to place a TFN® with a helical blade; this factor may have possibly influenced the results.
CONCLUSION
This study demonstrated no statistically significant differences in outcomes between the use of a TFN® with helical blade and a TFN® with femoral neck screw for the surgical treatment of intertrochanteric femur fractures. These findings suggest no outcomes-based rationale for choosing between the two collum implants tested in the surgical treatment of intertrochanteric femur fractures.
To generate empirically sound recommendations for the type of collum implant to use for intertrochanteric femur fractures, further research appears necessary.
Appendix 1
Classification of Intertrochanteric Femoral Fractures according to the AO/OTA Classification

Appendix 2
American Society of Anesthesiologists Classification

Footnotes
CONFLICT OF INTEREST: The authors declare that there is no potential conflict of interest relevant to this article.
References
- 1.Nederlandse Vereniging van Heelkunde; Nederlandse Orthopaedische Vereniging. Proximale femurfracturen [Internet] Utrecht: Nederlandse Vereniging van Heelkunde; 2016. [cited 2018 Nov 1]. Available from: https://richtlijnendatabase.nl/richtlijn/proximale_femurfracturen/proximale_femurfracturen_-_startpagina.html. [Google Scholar]
- 2.Reindl R, Harvey EJ, Berry GK, Rahme E. Intramedullary versus extramedullary fixation for unstable intertrochanteric fractures: a prospective randomized controlled trial. J Bone Joint Surg Am. 2015;97:1905–1912. doi: 10.2106/JBJS.N.01007. [DOI] [PubMed] [Google Scholar]
- 3.Registratie LT. LTR factsheet [Internet] Landelijk Netwerk Acute Zorg; 2015. [2018 Nov 1]. Available from: http://www.nazl.nl/sites/nazl/files/ltr_2012_factsheetheupfracturen_140611.pdf. [Google Scholar]
- 4.van Santen M. Waarom heeft een gebroken heup zulke grote consequenties? Plus Magazine. 2016. [cited 2018 Nov 1]. Available from: https://www.plusonline.nl/versleten-heup/waarom-heeft-een-gebroken-heup-zulkegrote-consequenties.
- 5.Müller ME, Allgöwer M, Schneide R, Willenegger H. Manual of internal fixation: techniques recommended by the AO-ASIF group. 3rd ed. Berlin: Springer-Verlag; 1991. [Google Scholar]
- 6.Sandifer PA, Hulick RM, Graves ML, et al. Extent and morbidity of lateralization of a trochanteric fixation nail blade. Orthopedics. 2017;40:e886–e891. doi: 10.3928/01477447-20170810-05. [DOI] [PubMed] [Google Scholar]
- 7.Stern R, Lübbeke A, Suva D, Miozzari H, Hoffmeyer P. Prospective randomised study comparing screw versus helical blade in the treatment of low-energy trochanteric fractures. Int Orthop. 2011;35:1855–1861. doi: 10.1007/s00264-011-1232-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Li C, Xie B, Chen S, Lin G, Yang G, Zhang L. The effect of local bone density on mechanical failure after internal fixation of pertrochanteric fractures. Arch Orthop Trauma Surg. 2016;136:223–232. doi: 10.1007/s00402-015-2369-5. [DOI] [PubMed] [Google Scholar]
- 9.Fang C, Lau TW, Wong TM, Lee HL, Leung F. Sliding hip screw versus sliding helical blade for intertrochanteric fractures: a propensity score-matched case control study. Bone Joint J. 2015;97-B:398–404. doi: 10.1302/0301-620X.97B3.34791. [DOI] [PubMed] [Google Scholar]
- 10.Goffin JM, Pankaj P, Simpson AH, Seil R, Gerich TG. Does bone compaction around the helical blade of a proximal femoral nail anti-rotation (PFNA) decrease the risk of cut-out?: A subject-specific computational study. Bone Joint Res. 2013;2:79–83. doi: 10.1302/2046-3758.25.2000150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Huang X, Leung F, Liu M, Chen L, Xu Z, Xiang Z. Is helical blade superior to screw design in terms of cut-out rate for elderly trochanteric fractures? A meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol. 2014;24:1461–1468. doi: 10.1007/s00590-014-1429-9. [DOI] [PubMed] [Google Scholar]
- 12.Li S, Chang SM, Niu WX, Ma H. Comparison of tip apex distance and cut-out complications between helical blades and lag screws in intertrochanteric fractures among the elderly: a meta-analysis. J Orthop Sci. 2015;20:1062–1069. doi: 10.1007/s00776-015-0770-0. [DOI] [PubMed] [Google Scholar]
- 13.Caruso G, Bonomo M, Valpiani G, et al. A six-year retrospective analysis of cut-out risk predictors in cephalomedullary nailing for pertrochanteric fractures: Can the tip-apex distance (TAD) still be considered the best parameter? Bone Joint Res. 2017;6:481–488. doi: 10.1302/2046-3758.68.BJR-2016-0299.R1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Baumgaertner MR, Curtin SL, Lindskog DM, Keggi JM. The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip. J Bone Joint Surg Am. 1995;77:1058–1064. doi: 10.2106/00004623-199507000-00012. [DOI] [PubMed] [Google Scholar]
- 15.Cleveland M, Bosworth DM, Thompson FR, Wilson HJ, Jr, Ishizuka T. A ten-year analysis of intertrochanteric fractures of the femur. J Bone Joint Surg Am. 1959;41-A:1399–1408. [PubMed] [Google Scholar]
- 16.AO Foundation. AO Surgery References [Internet] Davos: AO Foundation; 2016. [cited 2018 Nov 1]. Available from: http://www2.aofoundation.org/wps/portal/surgery?showPage=diagnosis&bone=Femur&segment=Proximal. [Google Scholar]
- 17.Liu W, Zhou D, Liu F, Weaver MJ, Vrahas MS. Mechanical complications of intertrochanteric hip fractures treated with trochanteric femoral nails. J Trauma Acute Care Surg. 2013;75:304–310. doi: 10.1097/TA.0b013e31829a2c43. [DOI] [PubMed] [Google Scholar]
- 18.Depuy Synthes. TFN - titanium trochanteric fixation nail system [Internet] Raynham: Depuy Synthes; 2016. [cited 2018 Nov 1]. Available from: http://synthes.vo.llnwd.net/o16/LLNWMB8/INT%20Mobile/Synthes%20International/Product%20Support%20Material/legacy_Synthes_PDF/DSEM-TRM-0714-0116-3_LR.pdf. [Google Scholar]
- 19.Zehir S, Zehir R, Zehir S, Azboy İ, Haykir N. Proximal femoral nail antirotation against dynamic hip screw for unstable trochanteric fractures; a prospective randomized comparison. Eur J Trauma Emerg Surg. 2015;41:393–400. doi: 10.1007/s00068-014-0463-y. [DOI] [PubMed] [Google Scholar]
- 20.Kerremans MS, van Langelaan EJ, Apachitei I. Vermoeidheidsfractuur van de helical blade van een Proximal Femoral Nail Antirotation. Ned Tijdschr Orthop. 2010;17:117–121. [Google Scholar]
- 21.Flores SA, Woolridge A, Caroom C, Jenkins M. The utility of the tip-apex distance in predicting axial migration and cutout with the trochanteric fixation nail system helical blade. J Orthop Trauma. 2016;30:e207–e211. doi: 10.1097/BOT.0000000000000505. [DOI] [PubMed] [Google Scholar]