

Abstract
Usual sites of the spread of the squamous cell carcinoma (SCC) larynx is regional–cervical lymphadenopathy. The lung is the most frequent site of distant metastasis, accounting for 66% of distant metastasis. Other metastatic sites include bone (22%), liver (10%), skin, mediastinum, and bone marrow. Occurrence of distant metastasis adversely affects the survival and alters the treatment planning completely, more towards palliative intent. Here, we present a case with very rare presentation of malignant ascites in a case of SCC larynx.
Keywords: SCC larynx, Malignant ascites
Case Report
A 70-year-old male patient, chronic alcoholic and chronic smoker, presented with hoarseness of voice. No significant family history or any medical or surgical history was present. General examination was normal except for grade 2 clubbing. The oral cavity was normal on examination. Neck examination revealed bilateral level 2 and 3 cervical lymphadenopathy. Hopkin’s examination revealed ulcerative growth involving the entire glottis and extending to the subglottic region. Supraglottic structures were normal. Respiratory, cardiovascular, central nervous system, and per abdominal examination did not reveal any significant abnormality.
CECT Neck showed enhancing mass lesion involving the right vocal cord, anterior commissure, and anterior part of the left vocal cord with subglottic extension and effacement of adjacent air column suggestive of malignant lesion of the larynx. Bilateral level 2 and 3 cervical lymphadenopathy was also seen.
CT Thorax revealed diffuse panacinar emphysema with thin-walled bullae in bilateral upper lobes with dense pericardial calcification. No evidence of lung metastasis or pleural effusion was present.
CBC and coagulation profile were normal. USG abdomen was also normal.
Direct laryngoscopy under anaesthesia showed ulcero-infiltrative growth involving the whole of the glottis and anterior commissure and extending to subglottis. Punch biopsy was taken which was suggestive of well-differentiated SCC (Figs. 1 and 2).
Fig. 1.
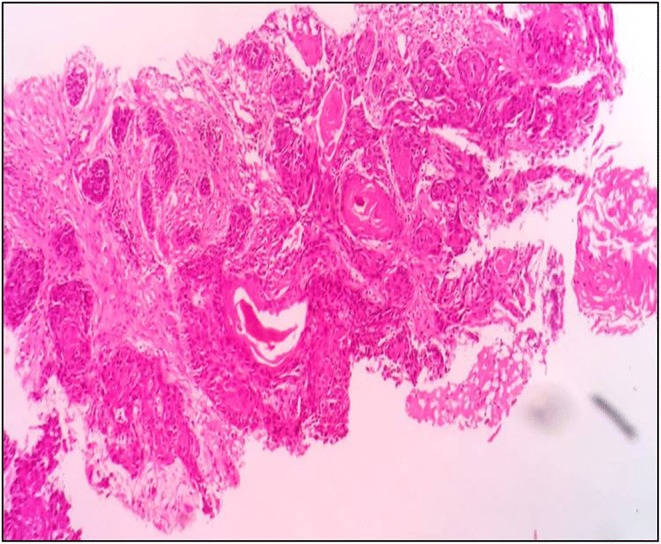
Punch biopsy of the glottic growth suggestive of well differentiated SCC
Fig. 2.

Magnified view suggestive of well differentiated SCC
The patient was lost to follow-up for 4 weeks and later on presented with stridor and gross abdominal distension. Emergency tracheostomy done. On examination, tense ascites was present with fluid thrill. Bilateral pedal oedema was also present. USG abdomen revealed moderate ascites. Two thousand milliliters of ascitic fluid was drained by aseptic tapping and sent for cytology examination. USG did not reveal any evidence of liver metastasis.
Cytology revealed cellular component showing presence of inflammatory cells, RBCs, and mesothelial cells. In addition, a small number of atypical cells were also seen (Figs. 3 and 4). Cell block was made and on immunohistochemical (IHC) markers study, diagnosis of metastatic squamous cell carcinoma was given(CK5/6—positive, P40—positive, CD 56—positive in histiocytes, calretinin—negative, WT—negative).
Fig. 3.
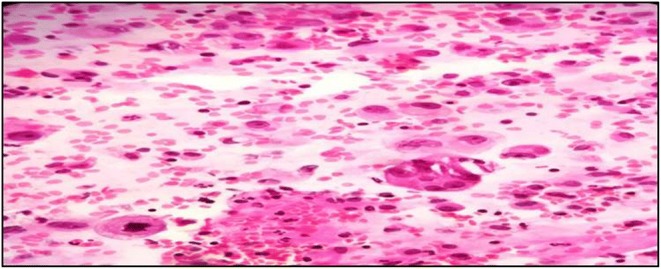
A small number of atypical cells
Fig. 4.
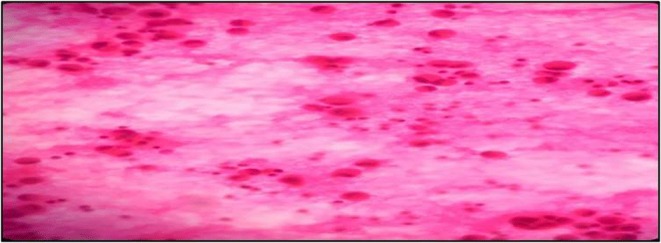
Another set of atypical cells
Discussion
Laryngeal SCC commonly spreads to cervical lymph nodes. Distant metastasis usually involves the lung. However, a few cases of unusual sites of distant metastasis have been reported in literature, e.g. peritoneum [1]. Some other case reports have also shown SCC larynx metastasizing to the ileum and appendix [2], peritoneal and pleural fluids [3].
The question of whether “recurrent” laryngeal carcinoma is truly a new tumour with a clonal origin that differs from that of the primary tumour. The clonality of the tumour can be checked for LOH (loss of heterozygosity). Patients without LOH usually have the longer time to recurrence.
Of importance is also the pattern of allelic loss, whether the same or different alleles for primary and recurrent tumour.
Having the same clonal origin for both primary and recurrent tumour implies that one has failed to clear the disease radically or there were micrometastases from the time of first detection of the disease which went undiagnosed by the routine diagnostic tools.
Regarding management of this patient, it is to be explained to the patient that the disease biology is aggressive and carries a very poor prognosis. The only suitable management option for this patient is to undergo palliative chemotherapy and Best Supportive Care.
Conclusion
We, herein, report a very rare case of SCC larynx who presented with malignant ascites as a sole mode of distant metastasis without any liver or lung metastasis. Genetic studies including LOH and p53 mutation testing can be considered in these kinds of atypical presentations. Although rare, malignant origin should be considered in any patient presenting with ascites during or after treatment of SCC larynx or any other head and neck primary site.
Peritoneal metastasis in a case of primary SCC of the larynx is a rare occurrence and it carries a poor prognosis compared to usual sites [1]. Immunohistochemical and biomarker studies may reveal a mutation in p53 gene in these types of cases which is indicative of unfavourable prognosis [4].
References
- 1.Stebbing J, Crane J, Greenstein AS, Ezra DG Atypical metastases from squamous cell cancers. Grand Rounds J 2:43–45
- 2.Glicksman JT, Bottoni D, Shepherd J, Parry N, Franklin JH. CASE REPORT Open Access Carcinoma of the larynx, metastatic to ileum, presents as ruptured appendicitis: case report and literature review. [DOI] [PMC free article] [PubMed]
- 3.Smith-Purslow MJ, Kini SR, Naylor B. Cells of squamous cell carcinoma in pleural, peritoneal and pericardial fluids. Acta Cytol. 2006;50:603–607. doi: 10.1159/000326027. [DOI] [PubMed] [Google Scholar]
- 4.Chen HY, Hsu CT, Lin WC, Tsai HD, Chang WC. Prognostic value of p53 expression in stage 1B1 cervical carcinoma. Gynecol Obstet Investig. 2000;49:266–271. doi: 10.1159/000010257. [DOI] [PubMed] [Google Scholar]