

Abstract
Background:
Dementia is associated with high health care costs, premature long-term care (LTC) placement, medical complications, reduced quality of life, and caregiver burden. Most health care providers and systems are not yet organized or equipped to provide comprehensive long-term care management for dementia, although a range of effective symptoms and supportive care approaches exist. The Maximizing Independence at Home-Streamlined (MIND-S) is a promising model of home-based dementia care coordination designed to efficiently improve person-centered outcomes, while reducing care costs. This report describes the rationale and design of an NIA-funded randomized controlled trial to test the impact of MIND-S on time to LTC placement, person with dementia outcomes (unmet needs, behavior, quality of life), family caregiver outcomes (unmet needs, burden), and cost offset at 18 (primary end point) and 24 months, compared to an augmented usual care group.
Methods:
This is a 24-month, parallel group, randomized trial evaluating MIND-S in a cohort of 304 community-living persons with dementia and their family caregivers in Maryland. MIND-S dyads receive 18 months of care coordination by an interdisciplinary team comprised of trained non-clinical community workers (e.g. Memory Care Coordinators), a registered nurse, and a geriatric psychiatrist. Intervention components include in-home dementia-related needs assessments; individualized care planning; implementation of standardized evidence-based care strategy protocols; and ongoing monitoring and reassessment. Outcomes are assessed by blinded evaluators at baseline, 4.5, 9, 13.5, 18, and 24 months.
Discussion:
Trial results will provide rigorous data to inform innovations in effective system-level approaches to dementia care.
1. Introduction
Alzheimer’s disease and related forms of dementia cause considerable suffering for many individuals and families. An estimated 46.8 million persons worldwide [1], including > 5.3 million older American [2] are living with dementia. In the context of dramatic demographic shifts and an absence of curative or disease altering treatments, the number of cases is expected to nearly triple to 113 million, and 13 million, respectively, by 2050. Dementia is associated with high health care costs, premature and unwanted long-term care (LTC) placement, general medical (e.g., urinary tract infections, falls) and behavioral complications (e.g. agitation, aggression, depression, anxiety, sleep disturbances), functional disability, and poor quality of life [3–10]. The majority (70–80%) of persons with dementia live at home in the community with unpaid family caregivers providing much of the required care and supervision [2]. These family caregivers are themselves at risk for poor outcomes including physical and emotional strain, mental health conditions, isolation, premature retirement and/or lost wages, and financial burden [11].
Management of dementia, focused on identifying and treating symptoms, addressing disease accelerators, and providing supportive social and non-medical care to both the person affected and their caregiver, can improve outcomes [12]. Effective non-drug symptom and disease management approaches are available [13–20], and medical associations recommend the integration and coordinated use of such evidence-based dementia management approaches to maximize effectiveness on outcomes [12,21–25]. However, for a variety of reasons (e.g., system fragmentation, poor coordination across the long-term care continuum, inadequate financing of social and supportive care services, misalignment of health care system incentives), the adequacy of dementia care that persons with dementia and their families actually receive continues to be “a matter of luck.” [26] As a result, common, yet modifiable, dementia-related care needs such as safety (e.g. home safety, wander risk management, driving), general medical care, management of behavioral symptoms, medication management, access to social and supportive care in daily living (e.g., meaningful activities; ADL assistance) often go unevaluated and unmet [27–31], contributing to excesses in adverse outcomes and higher costs.
Care coordination (e.g., care management, case management, collaborative care) models that take an interdisciplinary team approach, attend to the wide-ranging, multidimensional aspects of dementia management, and facilitate critical service linkages between medical, social and supportive care represent an understudied but potentially important tool to promote better coordination, quality of dementia care, and value. The limited empirical data available suggests that such dementia-oriented care coordination models can be beneficial for both persons with dementia (e.g. improved guideline adherence, quality of life, and reduced neuropsychiatric behavior, risk of institutionalization) and caregivers (e.g. reduced caregiver burden/strain/depression) [32–36]. However, limitations and variations in study design and methodological quality, intervention components and delivery processes, reporting deficiencies, and differences in primary outcomes targeted make it difficult to draw conclusions. Further, data on intervention delivery costs, cost savings or cost effectiveness needed to develop value propositions or estimate potential for return on investments is also lacking, which stifles efforts to translate these programs into practice.
The Maximizing Independence (MIND) at Home dementia care coordination program [37,38], one of several promising emergent models [39–42], is a comprehensive, home-based care coordination intervention for people with Alzheimer’s disease or related dementias who live in the community and for their family caregivers. MIND at Home is designed to improve person-centered outcomes such as the ability for a person to remain in one’s own home for as long as appropriate, maximizing quality of life, and reduce caregiver burden, while simultaneously lowering health care and other related costs. In a previous randomized pilot trial, MIND at Home was found to be feasible to deliver, acceptable to pesons with dementia and their family caregivers, and led to significant delays in time to transition from home, fewer dementia-related unmet needs, improved quality of life (QOL), and reduced caregiver objective burden (e.g. time savings) from baseline to 18 months compared to augmented usual care [31,43–45]. However, the trial was not specifically designed to assess impact on delaying time to LTC, or to estimate intervention delivery costs or cost impacts on direct and indirect costs of care, both of which are critical to dissemination adoption and uptake by health care systems and insurers. Further, the intervention did not significantly impact important outcomes like reduction in neuropsychiatric behaviors and subjective caregiver burden.
2. Study design
2.1. Overview of study design and procedures
This is a 24-month, prospective, single-blind, parallel group randomized Phase III trial testing the MIND at Home-Streamlined (MIND-S) care coordination intervention versus augmented usual care in a cohort of 304 community-living persons with dementia and their informal caregivers (dyads) in the greater Baltimore and Maryland suburban District of Columbia (DC) region (clinicaltrials.gov; NCT02396082). The study design and participant flow is in Fig. 1.
Fig. 1.
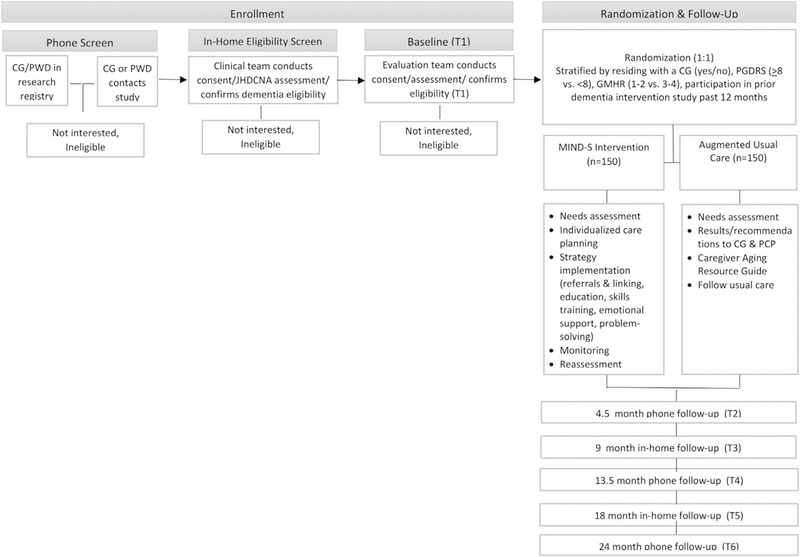
Study design and participant flow.
MIND-S is a new iteration of the original MIND at Home model designed to be more efficient, streamlined, and effective based on the results and experience in the original pilot study (as described below). This study has been reviewed and approved by the Johns Hopkins Medicine Institutional Review Board and is overseen by a three-member Data Safety and Monitoring Board, per NIH guidelines. Oral consent is obtained from participants (i.e., persons with dementia and/or informal caregivers) during a telephone screen. Written consent is obtained from the participants and their identified informal caregiver at the initial in-home assessment. For participants too impaired to provide consent, proxy consent is obtained from a legally authorized representative using the Maryland Health Care Decisions Act as a guide, with assent obtained from the participant.
2.2. Research aims
The main objective of this Phase III clinical efficacy trial is to evaluate whether MIND-S improves the ability of persons with dementia (PWD) to remain at home longer, while simultaneously improving secondary outcomes such as maximizing quality of life, reducing health care and indirect costs, and reducing subjective and objective caregiver burden compared to augmented usual care. Specific aims are below:
2.2.1. Aim 1
To determine the efficacy of MIND-S on time to long-term care (LTC) placement or death at 18 and 24 months (6 months post treatment). Hypothesis: PWD who receive MIND-S will have a significant delay on time to LTC placement or death compared to controls at 18 months (primary end point) and 24 months.
2.2.2. Aim 2
To estimate MIND-S cost and assess whether it results in net financial benefits by conducting a cost analysis taking the societal perspective at 18 and 24 months (6 months post treatment). Hypothesis: PWD who receive MIND-S will experience net cost savings compared to controls at 18 (primary end point) and 24 months when healthcare, community-based services, and CG productivity impacts are considered.
2.2.3. Aim 3
To determine the efficacy of MIND-S on PWD unmet care needs, neuropsychiatric symptoms (NPS), and quality of life (QOL), and on CG unmet needs and burden at 18 and 24 months (6 months post treatment). Hypothesis 3a: PWD who receive MIND-S will experience a greater reduction in unmet needs, NPS, and better QOL ratings compared to controls at 18 (primary end point) and 24 months; Hypothesis 3b: CGs who receive MIND-S will experience a greater reduction in unmet care needs and burden (perceived and objective) compared to controls at 18 (primary end point) and 24 months.
2.2.4. Exploratory aims
To explore whether the intervention’s effect on time to transition varies as a function of participant cognitive impairment, socioeconomic status, or race (moderators) and whether impact on predicted PWD and CG clinical outcomes mediate the impact of MIND-S on time to transition to LTC or death (mediators).
2.3. Conceptual framework
The relationship of MIND-S and proposed aims is in Fig. 2. We hypothesize the intervention will have a direct impact on time to LTC placement (Aim 1) and will result in net financial benefits (Aim 2), when all financial impacts are considered. MIND-S has been improved over the first iteration of the MIND at Home program [37] by streamlining the Johns Hopkins Dementia Care Needs Assessment (JHDCNA) to be shorter, more targeted and efficient; integrating new evidence-supported strategies (e.g., home safety, personal safety, preventive care, activities, CG chronic stress management, communication, behavior management skills) that we hypothesize will produce improved clinical outcomes for PWD and CGs (Aim 3); refining the MIND-S intervention delivery protocols and greater specification of the minimum core components; streamlining and standardizing the initial and on-going MIND-S team training and mentorship/supervision protocols; and enhancing the clinical tracking software for the care team (Dementia Care Management System [DCMS 2.0] to improve efficiency, fidelity in care delivery, and intervention characterization (e.g., improved user navigation, reporting, care plan generation, storage and access of resource referrals and education materials, embedded tracking of specific care options utilized by unmet need type, duration and intensity of contacts). Given improvements in the intervention, we further hypothesize that benefits will be sustained 6 months post intervention. We will also explore moderating effects of dementia severity, race, and socioeconomic status (SES) on intervention benefits, to provide targeting data for later trials, assess evidence of health disparities in dementia care and outcome [46,47], and assess whether impact on predicted PWD and CG clinical outcomes mediate the impact of MIND-S on time to transition to LTC (mediators)—to inform the next stages of translation and evaluation. MIND-S is informed by Institute of Medicine’s (IOM) Health Care Quality Framework [48] and Wagner’s chronic care model (CCM) [49], with content derived from decades of clinical expertise in clinical dementia care, practice recommendations [12,21–23], prior research, and the pilot.
Fig. 2.
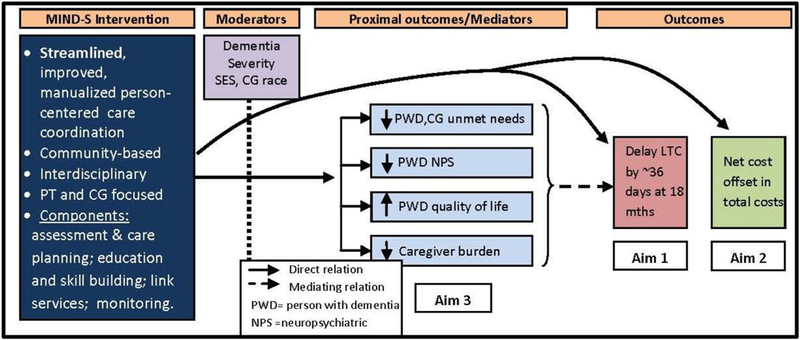
Conceptual model of MIND-S and study aims.
3. Inclusion and exclusion criteria
Study participants include the person with dementia and an informal caregiver (dyad). Both the person with dementia and the informal caregiver must meet the following eligibility criteria:
3.1. Inclusion criteria for PWD
(1) Diagnosed with all-cause dementia using standard assessments and diagnostic criteria [50] applied by a nurse clinician trained and supervised by a neuropsychiatrist (DJ) and with confirmation by neuropsychiatrist [described below]; (2) English speaking; (3) has a reliable informal caregiver (see definition below) available and willing to participate; and (4) living in a private home in the Baltimore area (40 mile radius from Johns Hopkins Bayview Medical Center).
3.2. Exclusion criteria for PWD
(1) That they are deemed to be in a crisis/unsafe situation at baseline (e.g., imminent risk of hospitalization, acute unstable medical conditions, suspected abuse or neglect, active suicidal ideations, extreme environmental hazard such as active bed bug infestation), (2) reported planned transition to another residential or care setting in < 6 months, (3) at end-stage disease (defined as bed-bound and non-communicative, or on hospice at BL), (4) spends longer than 3 months per year in a secondary residence outside of catchment area, or (5) they are currently enrolled in a interventional clinical trial for dementia or associated symptoms.
3.3. Inclusion criteria for CGs
(1) A reliable person who has contact with the PWD on a regular basis and at least once a week (e.g., in-person, by phone, by email), (2) is relied on by the PWD for assistance, (3) provides informal caregiving [not paid for their caregiving or caregiving as a volunteer through a volunteer service organization], (4) English speaking, and (5) 21 years of age or older (male or female).
3.4. Exclusion criteria for CGs
(1) They plan to leave the area within 12 months, (2) they do not expect to continue regular contact with the PWD within 12 months or (3) they are currently involved in another clinical trial of psychosocial or educational interventions. These exclusion criteria are designed to reduce CG attrition.
4. Recruitment and enrollment
Community-living persons with dementia and their informal caregivers are recruited from the Greater Baltimore region (40 mile radius of Johns Hopkins Bayview Medical Center), with a goal of including 30% minorities (the proportion of minority adults ≥65 in the geographic catchment area). Recruitment efforts primarily target CGs and family members since PWD may not have insight into their condition, be reluctant, or be too impaired to initiate enrollment. Participants are recruited through community organizations (e.g. religious organizations, senior housing); health and community service providers (e.g. public and private social service agencies, health professional practices, aging resource agencies, nutritional services); existing Johns Hopkins research registries; and general outreach including community-based events and local media publicity. As we have used previously [51], a three-pronged recruitment approach is taken: [1] collaboration with a diverse set of community organizations, health care providers, local and state Medicaid waiver programs, and health departments to send targeted mailings about the study to individuals on their mailing lists and to receive direct referrals, (2) a strategic community outreach campaign to promote a “background” community awareness through community presentations and publicity, and (3) use of existing dementia research registries at Johns Hopkins, with IRB approval. All recruitment material are IRB approved. We target an average monthly accrual rate of 14 dyads per month.
Enrollment is conducted in three stages. Persons referred to the study first complete a brief phone screen where a study team member explains the study and procedures, determines demographic eligibility, confirms a CG, and screens for cognitive impairment using the Telephone Interview for Cognitive Status (TICS) [52], a brief global cognition test administered to the potential participant, and the Informant Questionnaire for Cognitive Disorders in the Elderly (IQCODE), a 16-item informant rated cognitive screen [53], to the identified CG. Based on previously established cut-off scores, a positive screen is defined as TICS < 31 and IQCODE > 52 [52–54]. Eligible and willing participants then receive an in-home baseline visit (BL; T1) to confirm PWD diagnosis of dementia using NIA all-cause dementia criteria [50] and gather information that directly relates to the Johns Hopkins Dementia Care Needs Assessment (JHDCNA 2.0) tool [31,38]. Dyads who complete baseline are then randomized to the MIND-S intervention or the Augmented Usual Care group (control group). All dyads and their primary care physicians receive written results of the in-home needs assessment, recommendations for meeting needs, and a written standardized Aging and Caregiver Resource Guide developed in the previous MIND trial. Evaluators masked to group allocation reassess all dyads at 4.5 months (T2), 9 months (T3), 13.5 months (T4), 18 months (T5) (the main trial endpoint, testing immediate effects), and 24 months (T6) (6 month after treatment cessation, testing sustained effects) through a combination of phone (T2,T4, T6) and in-home contacts (T1,T3, T5).
5. Randomization and follow-up
Randomization (1) is performed after the baseline visit using a custom Excel-VBA software developed by the statistician (JSL). Randomization is at the dyad level. If a caregiver is caring for more than one participant, the randomization is done once, and then the treatment allocation is applied to the second participant. Based on findings in our pilot trial, randomization is stratified by whether the persons with dementia is residing with a CG (yes/no), Psychogeriatric Dependency Rating Scale (PGDRS) [55] total score (≥8 vs. < 8), General Medical Health Rating (GMHR) [56] (1–2 vs. 3–4), and whether the participant took part in a dementia intervention study in the past 12 months. Participants are replaced if for any reason they become ineligible, unavailable, or unwilling to participate up to the date they are randomized. This is an intent to treat analysis (ITT) once randomized.
Participants have follow-up visits at 4.5 months (T2), 9 months (T3), 13.5 months (T4), 18 months (T5) (the main trial endpoint, testing immediate effects), and 24 months (T6). Several strategies are used to retain participants for the full 24 months (use of home and phone visits; remuneration of $20 per person, per in-person study visit; emphasis on staff “customer service”; maintaining several contacts for each participant; prompt rescheduling practices).
Study endpoints include death, a permanent transition to residential long-term care setting (e.g. long-term care nursing home, assisted living), a move to another home outside of the catchment area, loss to follow-up, and withdrawal. Participants moving to other community residences inside the catchment area will be counted as an event failure for analyses evaluating risk and time to all-cause transition from home (secondary aim) but will continue to be assessed at regular follow-up intervals for all other outcomes (e.g. unmet needs, quality of life).
6. Treatment arms
6.1. MIND-S intervention
Participant/caregiver dyads randomized to the MIND-S intervention receive up to 18 months of dementia care coordination with written results of the needs assessment and care plan provided to the caregiver and primary care provider at baseline and 18 months. Participants also receive a Caregiver Resource Binder with general and individualized aging and dementia care information, a copy of the Aging and Caregiver Resource Guide, and a monthly newsletter that contains relevant education information, notices about community events, health tips, seasonal recipes, and entertainment (e.g. word find, crossword puzzles).
MIND-S is a comprehensive, home-based care coordination intervention designed to systematically assess and address unmet needs that may be barriers to persons with dementia remaining in their home, while maintaining their health and wellbeing, and that of their caregiver. The intervention key principles are summarized in Table 1.
Table 1.
Key principles of MIND-S.
| • Home-based care coordination |
| - Assesses and address a broad range of dementia related needs not usually attended to in usual office-based care, taking a wholistic approach to account for personal, environment, and contextual factors. |
| • Person-centered approach |
| - Systematic yet tailored person-centered approach that seeks to account individuals’ unique characteristics, desired outcomes, preferences, and values while creating high efficiency, as compared to a “one-size-fits-all” approach. |
| - Outcomes and goals of care are important to patients and families. |
| • Evidence-based |
| - Derived from decades of clinical expertise in dementia care, practice recommendations, prior research. |
| • Pragmatic |
| - Links medical and community based care services in cost efficient way through implementation by trained non-clinical community workers as the frontline interventionists. |
| - Integrates untapped community-based resources and workforce to support primary care providers and provide greater coordination of services. |
| • Proactive |
| - Proactive focus to address dementia-related needs that may offset crisis situations later. |
| - Empowers CGs with self-management strategies, problem-solving, education and skills designed to have lasting impacts and benefits. |
| • Replicable |
| - Consideration of health system design, workforce, and development and use of standardized training and delivery tools (i.e. Johns Hopkins Dementia Care Needs Assessment 2.0©; MIND at Home Intervention Handbook©; Care planning template; standardized MIND at Home Care team job descriptions and competencies) to promote translation, replication and scalability. |
The MIND-S model (Fig. 3) is delivered by Memory Care Coordinators (MCCs) (non-clinical community worker), working within an interdisciplinary team (Geriatric psychiatrist, Registered Nurse). MCCs are the front line interventionists (i.e. “in the trenches”) and provide PWD and CGs resource referrals, help with long-term care services and supports navigation and coordination, dementia education, behavior management skills training, emotional support, problem-solving strategies—as well as on-going monitoring, assessment and planning for emergent needs. Depending on needs, MCCs may also interact with PWD’s health providers, and other community resource agencies to facilitate the linking, continuity, and coordination of medical, social, and supportive care. MCCs receive initial training and ongoing structured support and mentoring from a geriatric psychiatrist and registered nurse with clinical expertise in dementia care. Facilitated through the MCC, the geriatric psychiatrist and nurse may also directly consult with PWD and CGs on complex issues, those requiring clinical acumen, and for the periodic full needs assessments.
Fig. 3.
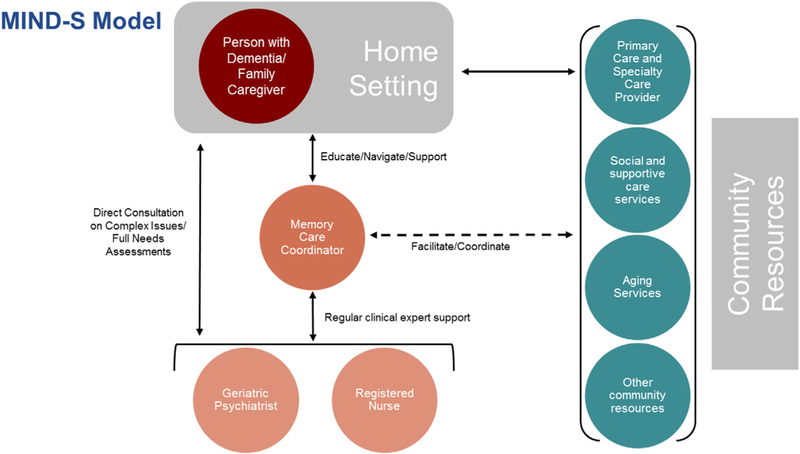
MIND-S model (adapted Figure, used with permission from Samus et al., 2017, International Journal of Care Coordination).
A set of tools supports the implementation and delivery of MIND-S:
Johns Hopkins Dementia Care Needs Assessment 2.0: © Standardized in-home needs assessment tool to capture 13 domains of dementia-related needs for persons with dementia and their family caregivers;
MIND at Home Intervention Handbook©: Manualized best practice and evidence-derived protocols that provides definitions and descriptions for a menu of recommended care strategies, which are linked to each identified unmet JHDCNA 2.0 need;
Dementia Care Management System (DCMS 2.0) ©: Custom cloud-based care management software platform to track intervention delivery progress; log contacts, duration, and care strategies employed; provide reminders for action items; manage, update and link shared referral directories for health providers and community services and supports; manage and update links to educational and information materials; secure sharing of information in real-time across the MIND at Home care team for higher quality care and self-monitoring; and creation of automated reports;
Structured MIND-S care planning template;
Detailed team member job descriptions and competencies;
Initial Certification Course©: 40 h structured didactic and interactive training for all team members that covers dementia and best practice principles, the MIND-S model and use of the tools, community resource identification, caregiver skill building techniques, family engagement and rapport, and use of the DCMS 2.0.;
Structured case-conferencing case presentation template;
Menu of continuing education mini-modules on key topics for continued knowledge and team capacity building over time;
Standard Operating Procedures manual.
The delivery process and minimum core components of the MIND-S model are listed in Table 2. The MCC and nurse jointly conduct the initial in-home dementia-related needs assessment for both the PWD and CG, and then immediately rate the JHDCNA and draft an individualized care plan, with input from the broader team as indicated by complexity. The MCC then reviews the care plan with the PWD and/ or CG and collaborates on prioritization of needs and implementation of strategies to address needs. MCCs monitor the program and revise the care plan as new needs emerge and as needs are met. The intervention intensity is driven by individual cases and needs, however MCCs are required to have a direct encounter with assigned cases at least every 30 days and are required to work with a nurse to complete a full JHDCNA reassessment at 9 months. Each encounter, consultation, or action taken by any care team member in regard to a particular dyad is logged in the DCMS 2.0 using standard procedures to track intervention delivery and fidelity. All intervention participants receive all intervention components for up to 18 months, but each component is tailored to the particular needs of PWD and CG. All recommended resource referrals are typically available in the local community. MIND-S does not provide any direct medical care treatment or services, nor does it provide any hands-on supportive care services.
Table 2.
MIND-S delivery process and minimum core components.
| 1. A 1.5-hour initial in-home visit with person with dementia and their informal caregiver. Data collected then informs the Johns Hopkins Dementia Care Needs Assessment 2.0 (JHDCNA 2.0) TheJHDCNA2.0 assesses PWD and caregiver needs and serves as the basis for development of the individualized care plan. |
| 2. Individualized need-based care planning and standardized MIND service delivery |
| ○ Written care plan (provided to family and primary care provider), prioritizing needs |
| ○ Implement core care strategies per standardized protocol |
| ▪ Disorder education |
| ▪ Referrals and linking to community based resources |
| ▪ Specific skills training/care strategies/problem solving |
| ▪ Emotional support |
| ▪ Symptom screening/needs assessment |
| ○ Caregiver resource binder |
| ○ Referral to occupational therapist for specialized protocols (Tailored Activities |
| 3. Monitoring and revision of care plan |
| • Memory care coordinator direct encounter every 30 days |
| • Quality reviews every 60 days by clinical supervisor |
| • Weekly care team rounds (addressing challenging/complex cases) |
| • Tracking encounters in Dementia Care Management System |
| 4. Full Johns Hopkins Dementia Care Needs Assessment (JHDCNA) In-Home Reassessment (every 9 months) |
| 5. Critical Events (e.g. hospitalizations, emergency room visits, falls) protocols are conducted in certain situations as described below: |
| • MCC and clinician home visit |
| • As-needed clinician mobile telehealth visits within 1 week of discharge |
| • As-needed clinician mobile telehealth visits to support coordinator in addressing pressing caregiver concerns, e.g., management of behavioral symptoms |
| • Transitions/discharges |
Citation: Samus et al., 2017 MIND at Home PLUS.
Telehealth is used for special circumstances on an as needed-basis for situations that may require clinical input or supervision (such as checking in with a patient a week after discharge from the hospital). If needed, MCCs travel to the PWD’s home and facilitate telehealth visits using iPads with 4G LTE between PWD/CG and a clinician in the office. These visits use the HIPAA compliant Cloud Axis/Polycom infrastructure managed by Johns Hopkins ISVC at Central IT. Telehealth has several purposes: to more fully assess the situation by the study’s clinical team so that the appropriate clinical referrals can be made to the patient’s health provider(s), to provide targeted behavioral management or health education to the caregiver, dementia care education, to help with problem solving, to role model interviewing techniques for MCCs, and to supplement other coordination activities.
6.2. Augmented usual care (control group)
Participant/caregiver dyads randomized to the Augmented Usual Care (control group) and their primary care physicians receive the written results of the in-home dementia care needs assessment following BL and 18 month visits including applicable generic intervention recommendations, as well as a brief Aging and Caregiver Resource Guide, developed in the pilot study that includes program and contact information for several local and national aging service organizations (e.g., Alzheimer’s Association, Administration on Aging, Centers for Medicare and Medicaid). They are able to pursue any intervention, evaluation, or treatment that they or their health providers deem appropriate. This condition likely exceeds the usual level of intervention in primary care settings [39] and likely represents a low-grade intervention.
7. Fidelity and bias
To ensure fidelity in delivery of the MIND-S intervention: (1) interventionists (i.e. MCCs, nurses, physicians) are trained as described above; (2) are observed during their first 3 independent field visits for their initial assigned intervention dyads; (3) the intervention team (MCCs, Nurse, Physician) meets weekly to discuss cases, procedures, troubleshoot problems; (4) the intervention team uses the DCMS 2.0; and (5) every case in the DCMS 2.0 is reviewed for quality assurance by a clinician at least every 60 days. Although MIND at Home interventionist fidelity to the assessment protocol is not measured using a structured tool, the visits are observed and supervised by a trained physician or nurse and all assessment documentation are also reviewed. This supervising clinician ultimately recommends to the Director of the clinical team (DJ) that new interventionist is ready to conduct the protocol independently and the Director then gives approval, or alternatively recommends further training. Also, any new interventionists are required to present their first three assessment cases to the full team during the weekly case presentation meetings to ensure fidelity. The DCMS 2.0 is used to quantify intervention delivery characteristics (care strategies employed by identified need, success rate by need, time spent during each contact, number and type of contacts, contact persons involved and role) and fidelity.
Potential bias is minimized as follows: (1) All study staff (evaluators and Interventionists) are required to take the JHU Research Compliance Training courses and are oriented to basic research principles, actions to take for an unsafe situation, and effective communication. (2) Intervention team and evaluator teams have separate meetings to discuss progress, individual cases, or challenging situations. Full team meetings are necessary to troubleshoot overall challenges such as recruitment; however all study staff are instructed not discuss specific participants or situations; (3) Evaluators are ‘certified’ in data collection (e.g. trained in measure administration, participate in role-play training exercises prior to live data collection visits, observed for the first 3 live data collection visits). The study coordinator performs quality assurance on data collection forms and the evaluation team is routinely asked to provide feedback on data collection, logistics, or if critical pieces of information are not being captured. (4) Evaluators remind participants at every visit not to disclose treatment group assignment.
8. Measures
Table 3 summarizes descriptive, covariate, and secondary outcome measures by data collection interval. Data are collected at initial home visit, baseline, 4.5 months (T2), 9 months (T3), 13.5 months (T4), 18 months (T5) (the main trial endpoint, testing immediate effects), and 24 months (T6) by masked evaluators. Participant characteristics assessed include demographics, living arrangements, use of health care services and home and community-based supports (proxy reported), income, satisfaction with care, care financing, medications (brown-bag review, use and adherence survey), medical history and medical diagnoses (proxy reported), function (Instrumental Activities of Daily Living and Basic Activities of Daily Living), cognition (Mini-Mental State Exam [57]), history of present illness and a brief physical exam (conducted by a clinician), and a home safety walkthrough. Caregiver characteristics assessed include demographics, marital status, employment, informal support networks, medical diagnoses, and use of health care services and home and community-based supports. Main outcome measures are summarized below.
Table 3.
Summary of descriptive and secondary outcome measures by data collection interval.
| Domain | Measure | Description | Respondent | Visit |
|---|---|---|---|---|
| Sociodemographic characteristics (covariate) | Individual items | PWD and CG–Age, sex, race, education, income range. Living with CG | PWD, CG | Screening |
| PWD cognitive status (descriptive, Covariate | Mini-mental state exam (MMSE) Clock drawing Mental alternations | Widely used measures, excellent validity, reliability | PWD | Screening |
| Physical frailty (descriptive, covariate) | Timed up and go | Validated measure of mobility, balance, walking ability, and fall risk in older adults | Nurse Interviewer | Screening |
| Medications (descriptive, secondary outcome) | Medication list (type, dose, frequency, indication) | Examination of PWD and CG medications in home | Interviewer | Screening, T2, T3, T4, T5, T6 |
| Medical diagnoses (covariate) | Self-reported medical diagnoses for PWD and CG | PWD and CG listing of medical diagnoses | PWD, CG | Screening, T3, T5 |
| Quality of life-self report (secondary outcome) | Quality of Life in Alzheimer’s Disease (QOL-AD- self report) | 13 item measure for QOL in dementia, excellent validity and reliability, useful in severe dementia | PWD | T1, T3, T5, T6 |
| Quality of life-proxy report (secondary outcome) | Quality of Life in Alzheimer’s Disease (QOL-AD- informant) | 13 item proxy rated version of QOL-AD | CG | T1, T3, T5, T6 |
| ADL Function (descriptive, covariate) | Psychogeriatric Dependency Rating Scale- (PGDRS) | 16-item scale assess basic activities of daily living (ADL) impairment in PWD | CG | T1, T3, T5, T6 |
| Mental/behavior disturbances (secondary outcome) | Neuropsychiatric Inventory (NPI) | Frequency, severity, distress, 12 domains of disturbances in PWD. | CG | T1, T3, T5, T6 |
| CG Burden (secondary) | Zarit Burden Inventory (Short) | 12-item version of original ZBI | CG | T1,T3, T5, T6 |
| CG Depression (covariate) | Patient Health Questionnaire (PHQ-9) | A 9-item, self-report measure assessing symptoms of depression | CG | T1, T3, T5, T6 |
T1 = Baseline visit, In-person.
T2 = 4.5 month visit, phone.
T3 = 9 month visit, in-person.
T4 = 13.5 month visit, phone.
T5 = 18 month visit, in-person.
T6 = 24 month visit, phone.
8.1. Time to LTC
The primary outcome for persons with dementia, time to LTC placement or death, is assessed by masked evaluators at T2, T3, T4, T5, and T6. At each data collection interval, evaluators determine if the PWD is still residing in his/her original residence by caregiver report. In cases of permanent transfer from home, the date, destination, and primary reason for transfer is recorded. For temporary transfers (e.g., in-patient hospital, rehabilitation facility), the location is recorded and evaluators follow-up at the next scheduled interval to determine the participant’s location. For death of the participant, the date, location of death, and cause of death are recorded. If death occurred outside of the home, evaluators record the date the participant left the home, the destination(s) and duration of stay in each destination prior to death. Time is expressed in days as time from baseline to time of permanent transfer/death, or censor. All available study data are used to resolve any discrepancies in date of permanent transition from home.
8.2. Cost measures
Proxy-reported health services utilization is assessed by masked evaluators at T2, T3, T4, T5, and T6 using an adapted measure that combines the Resource Utilization in Dementia (RUD) [58], and Services Utilization and Resources Survey (SURF) [59]. This adapted measure is administered to the CG and collects type and duration of service use for PWD’s healthcare service use (inpatient, outpatient, emergency visits, medications), home and community-based service use (e.g., Meals on Wheels, social worker visits, adult day care, formal homemaker/housecleaning services, formal caregiver/home aides), and long-term care use (e.g. admission or respite stays in nursing home, rehabilitation, assisted living, group homes) over a specified lookback period (e.g. year prior to baseline, between baseline visit and 4.5 month visit, between 4.5 month and 9 month visit). CG healthcare service use is also collected. PWD medications are recorded by a structured in-home brown bag review at baseline, T3, and T5. Healthcare service and medication use will be monetized using procedures described here. All direct medical costs will be estimated using published sources of Medicare reimbursement rates for inpatient and outpatient medical services (obtained from the U.S. Agency for Healthcare Resource and Quality Health Care Utilization Project National Inpatient Sample; Ingenix National Fee Analyzer) [60,61]. We will apply Medicare Part D average sales prices (ASP), inflated to the study year using the Consumer Price Index for healthcare services to estimate medication costs. If these data are not available, costs estimates will be based on Average Wholesale Price (AWP) for medications. Since AWP is considered to be an inflated measure of drug cost, we will apply an appropriate discount rate in sensitivity analyses (e.g., AWP minus 5–10%). Community-based services and long-term care costs (nursing home, assisted living, hosice facility) will come from publically available administrative data sets as done in previous AD trials [62]. Health utility is captured by CG proxy using Health Utilities Index [63].
MIND-S intervention costs are estimated using a template previously developed by the economic investigators [64]. The interventionists (i.e., MCC, nurse, geriatric psychiatrist) log time spent in preparation, documentation and implementation of MIND-S in each participant’s “action log” in the DCMS 2.0. Travel mileage and intervention materials are also captured in expenditure reports. Total intervention costs of MIND-S will be the sum of five direct cost categories: interventionist time for home and telephone sessions, training, intervention materials, interventionist travel, and supervision/adherence. Interventionist time will be calculated as the present value of earnings: (number of hours spent delivering MIND-S) × (interventionist reported wage rates + fringe benefits).
Indirect CG costs in the form of out of pocket spending, time spent caregiving, and productivity losses are estimated from caregiver administered items at baseline, 9, and 18 months. Time spent caring for the PWD will be calculated as: (number of hours spent caregiving) × (published regional hourly wage for a home health aide). Productivity losses will be calculated as: (number of hours of lost work time) × (published regional hourly wage for the stated occupation).
8.3. Dementia care needs
The JHDCNA 2.0, a streamlined version of the original assessment developed earlier (JHDCNA 1.0) [31], is used to record dementia related needs for PWD and their CGs at screening and T5 (unmasked). A trained study clinician documents unmet needs in 13 domains (e.g. Cognitive Symptoms, Behavioral, Home and Personal Safety, Medical Care, Activities and Daily Living, Legal and Advanced Care Planning, Care Financing, Caregiver Dementia Education, Caregiver skills training, Caregiver Medical Care, Caregiver Mental Health Care, Caregiver Informal supports, Caregiver Legal Issues), with 61 individual items. Ratings are based on a range of data (medical, physical, psychosocial, functional, behavioral, services use, environmental assessments) collected during the in-home visit. Need items have standardized descriptions and definitions, and each item is documented as being needed or not. If needed, the assessor determines whether the need is “fully met”, “partially met”, or “unmet”. A “fully met” need is one that is being addressed and potential benefits of available interventions have been achieved to the extent possible for the individual. A need is considered “partially met” if it has been or is being addressed but potential benefits of available interventions have not yet been achieved and “unmet” if it has not been addressed and potentially beneficial interventions are available. The JHDCNA was developed by a multidisciplinary group of clinical dementia care experts and is based on best practices in dementia care [12,21–25], suggesting content validity. While its psychometric properties have not been formally tested, prior studies demonstrate concurrent validity with QOL and caregiver burden measures [65,66]. Total percent unmet care needs will equal (# of unmet need items)/ (# need items assessed) ∗ 100.
9. Data analysis and power
Standard descriptive analyses will be used to check for outliers, missing data, and to ensure that distributional and other assumptions of the planned analyses are met. If not, transformations and/or non-parametric methods will be used. Primary outcomes will be analyzed using the intention-to-treat (ITT) approach. All primary analyses will control for whether the person with dementia is residing with a CG (yes/no), PGDRS total score (≥8 vs. < 8), GMHR (1–2 vs. 3–4), and whether the participant took part in a dementia intervention study in the past 12 months (randomization stratification variables). To investigate sensitivity to missing values, those with and without missing values will be compared by background covariates. Tests will be two-sided with α = 0.05. Multiple test corrections will be applied as appropriate.
To determine the efficacy of MIND-S on time to long-term care (LTC) placement or death at 18 and 24 months (Aim 1), we will fit Cox proportional hazards models [67] for each time period with group assignment as the covariate of interest and adjustment for the randomization variables. Model assumptions will be checked via Kaplan-Meier plots and Schoenfeld residuals [68]. In secondary analyses we will explore the efficacy of MIND-S on time to all-cause transition from home, the competing risks of death and care placement [69,70], as well as the effects of additional covariates, including baseline cognition, socioeconomic status, race, ADL disability, and caregiver factors.
We will conduct a cost-offset analysis to estimate MIND-S cost and assess whether it results in net financial benefits at 18 and 24 months (Aim2). Defined as the net financial benefit, in dollars, of the program considering a broad catchment of direct (healthcare service, HCBS) and productivity costs [71], the main cost measure will be the cost-offset of MIND-S calculated as the difference in the sum of all costs between MIND-S group and the sum of all costs in the augmented usual care from T1-T5 (baseline-18 months). An analysis will also be done to determine whether there would be sufficient cost offsets without considering productivity costs. Where necessary, healthcare costs will be inflated to the year of study using the Medical Care Consumer Price Index in the study year. In accordance with best practices in health economic analyses, sensitivity analyses will be conducted in order to determine the robustness of the cost analysis [72]. Univariate sensitivity analysis will be performed, whereby one variable is changed at a time and impact on net benefit is determined. Sensitivity analyses will include those variables where we anticipate “real world” uncertainty and will include, at a minimum, modification of key cost variables, e.g., inpatient and outpatient medical costs, based on 25th and 75th percentiles of Medicare reimbursement.
To determine the efficacy of MIND-S on PWD unmet care needs, NPS, and QOL, and on CG unmet needs and burden at 18 and 24 months (Aims 3), we will fit longitudinal mixed-effects linear regression models [73]. These models will include a random intercept, a random slope (if necessary), and terms for treatment group, time, and group x time interaction. This last term (the treatment effect) represents the difference in change over time between the two groups. We will also control for the four randomization variables. We will only include data on secondary outcomes for participants up to the time they transitioned from the home or died.
In exploratory analyses, we will determine whether the effect of the intervention on time to transition varies as a function of cognitive impairment, socioeconomic status or race by fitting additional hazards models with interactions between treatment group and these potential moderators. We will also do mediation analysis and test whether patient and caregiver clinical outcomes (including NPS, needs, burden) mediate the effect of the intervention on time to transition using the process outlined by Roth & MacKinnon [70].
Sample size estimates are based on data from PWD in the pilot MIND study. For our primary outcome (Aim 1), based on the formulae of Schoenfeld [74] with a sample of 300, 1:1 randomization, and an 18-month study period, we will have 80% power to detect a hazard ratio (HR) of 0.59 comparing risk of long-term care placement or death for treated relative to controls. For the 24-month analysis we would have 80% power to detect an HR of 0.63 or less. These calculations are conservative in that it is known that adjustment for baseline covariates (as planned) will substantially increase power. These effects are similar in magnitude to what was observed in our preliminary data, and would be clinically and financially significant. For cost-offset analysis (Aim 2), there were no comparable data to draw from prior studies to estimate net benefit group differences or variances. Using post-hoc estimates from our pilot study on intervention cost and the mean expected LTC placement delay (assuming costs in other categories are not significantly different between groups but allowing for large variability in mean total cost), we will have 80% power to detect a total cost difference of $3654 (SD $10,000) between the groups over 18 months. This assumes a 36 day delay in LTC placement in the MIND-S group (as observed in dementia participants in the pilot study), average cost per day of LTC at $164/day (an equal proportion of participants enter NH at $214/day and assisted living facilities at $114/day), and an 18 month cost of MIND-S of $2250 ($1500 estimated MIND-S per year ∗ 1.5 years) [i.e., 36 day mean LTC delay ∗ $164/day − $2250 of MIND-S = $3654 net cost offset savings per patient]. This would yield a nontrivial expected return on investment of 162% per MIND-S participant. Power for our mixed effects models (Aim 3) was calculated via simulation with 1000 repetitions, using data from PWD in the MIND pilot study, assuming an 18-month intervention, and attrition of 20% at 18 months. For the QOL-AD self-rated scale, we will have 80% power to detect a between-group difference in slope of 0.1, which would correspond to between-group differences in improvement on each measure of approximately 2 points over the course of the 18-month intervention. For the Zarit Burden Inventory (ZBI), we would have 80% power to detect a between-group difference in slope of 0.12, which will correspond to a between-group difference in improvement over 18 months of approximately 2 points. These are consistent with the pilot data, but more importantly, we would have power to detect clinically meaningful changes (≥0.5 SD on the QOL-AD and ZBI).
10. Discussion
Development and refinement of efficacious dementia management models aimed at improving persons with dementia (PWD) and caregiver (CG) outcomes, reducing costs, and linking health and community long-term services and supports must be a public health priority to care for those affected now and in the future. This 24-month, prospective, single-blind, parallel RCT will evaluate the efficacy and cost-offset of the MIND-S care coordination intervention for dementia as a comprehensive, community-level care delivery model for community-living PWD and their informal CGs (dyads) living in the Greater Baltimore area. We hypothesize that the MIND intervention will delay transition from the home. It may also improve care quality, quality of life for PWD and reduce health care costs, and burden in CGs and family members in the long-term. This project will provide information critical for health care decision-makers, at a time when both quality and cost containment in health care are necessary. If proven efficacious and cost efficient, the MIND-S model has the potential to change how dementia care services are provided and coordinated at the community level and serve as a national model. It is responsive to the National Alzheimer’s Project Act (Public Law 111–375) calling for development and testing of new comprehensive models of dementia care.
Acknowledgement
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Grant Number R01AG046274 from the National Institute on Aging, National Institutes of Health (US).
References
- [1].Prince M, Wimo A, Guerchet M, Gemma-Claire A, Wu Y-T, Prina M, World Alzheimer Report, The global impact of dementia - an analysis of prevalence, incidence, cost and trends, Alzheimer’s Dis. Int 2015 (2015) 84, 10.1111/j.0963-7214.2004.00293.x. [DOI] [Google Scholar]
- [2].Alzheimer’s Association, 2017 Alzheimer’s disease facts and figures, Alzheimers Dement 13 (2017) 325–373 http://www.alz.org/documents_custom/2017-facts-and-figures.pdf, Accessed date: 10 May 2017. [Google Scholar]
- [3].Gaugler JE, Yu F, Krichbaum K, Wyman JF, Predictors of nursing home admission for persons with dementia, Med. Care 47 (2) (2009) 191–198, 10.1097/MLR.0b013e31818457ce. [DOI] [PubMed] [Google Scholar]
- [4].Black BS, Rabins PV, German PS, Predictors of nursing home placement among elderly public housing residents, Gerontologist 39 (5) (1999) 559–568, 10.1093/geront/39.5.559. [DOI] [PubMed] [Google Scholar]
- [5].Yaffe K, Fox P, Newcomer R, et al. , Patient and caregiver characteristics and nursing home placement in patients with dementia, JAMA 287 (16) (2002) 2090–2097, 10.1001/jama.287.16.2090. [DOI] [PubMed] [Google Scholar]
- [6].Miller EA, Weissert WG, Predicting elderly people’s risk for nursing home placement, hospitalization, functional impairment, and mortality: a synthesis, Med. Care Res. Rev 57 (3) (2000) 259–297, 10.1177/107755870005700301. [DOI] [PubMed] [Google Scholar]
- [7].Hébert R, Dubois MF, Wolfson C, Chambers L, Cohen C, Factors associated with long-term institutionalization of older people with dementia: data from the Canadian Study of Health and Aging, J. Gerontol. A Biol. Sci. Med. Sci 56 (11) (2001) M693–M699 http://biomedgerontology.oxfordjournals.org/content/56/11/M693.full.pdf+html. [DOI] [PubMed] [Google Scholar]
- [8].Cooper C, Bebbington P, Katona C, Livingston G, Successful aging in health adversity: results from the National Psychiatric Morbidity Survey, Int. Psychogeriatr 21 (5) (2009) 861–868, 10.1017/S104161020900920X. [DOI] [PubMed] [Google Scholar]
- [9].Miller EA, Schneider LS, Rosenheck RA, Predictors of nursing home admission among Alzheimer’s disease patients with psychosis and/or agitation, Int. Psychogeriatr 23 (1) (2011) 44–53, 10.1017/S1041610210000244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Hurd MD, Martorell P, Delavande A, Mullen KJ, Langa KM, Monetary costs of dementia in the United States, N. Engl. J. Med 14368 (4) (2013) 1326–1334, 10.1056/NEJMsa1204629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Connell CM, Janevic MR, Gallant MP, The costs of caring: impact of dementia on family caregivers, J. Geriatr. Psychiatry Neurol 14 (4) (2001) 179–187, 10.1177/089198870101400403. [DOI] [PubMed] [Google Scholar]
- [12].Rabins PV, Lyketsos CG, Steele C, Practical Dementia Care, 3rd edn, Oxford University Press, New York, 2016. [Google Scholar]
- [13].Gitlin LN, Kales HC, Lyketsos CG, Nonpharmacologic management of behavioral symptoms in dementia, JAMA 308 (19) (2012) 2020–2029, 10.1001/jama.2012.36918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Brodaty H, Arasaratnam C, Meta-analysis of nonpharmacological interventions for neuropsychiatric symptoms of dementia, Am. J. Psychiatry 169 (9) (2012) 946–953, 10.1176/appi.ajp.2012.11101529. [DOI] [PubMed] [Google Scholar]
- [15].Cooper C, Mukadam N, Katona C, et al. , Systematic review of the effectiveness of non-pharmacological interventions to improve quality of life of people with dementia, Int. Psychogeriatr 24 (6) (2012) 856–870, 10.1017/S1041610211002614. [DOI] [PubMed] [Google Scholar]
- [16].Health Quality O, Behavioural Interventions for Urinary Incontinence in Community-Dwelling Seniors: An Evidence-based Analysis, vol. 8, (2008) http://www.ncbi.nlm.nih.gov/pubmed/23074508%5Cnhttp://www.ncbi.nlm.nih.gov/pmc/articles/PMC3377527/pdf/ohtas-08-52.pdf. [PMC free article] [PubMed] [Google Scholar]
- [17].Livingston G, Johnston K, Katona C, Paton J, Lyketsos CG, Systematic review of psychological approaches to the management of neuropsychiatric symptoms of dementia, Am. J. Psychiatry 162 (11) (2005) 1996–2021, 10.1176/appi.ajp.162.11.1996. [DOI] [PubMed] [Google Scholar]
- [18].Dw O, Ames D, Gardner B, et al. , Psychosocial treatments of psychological symptoms in dementia: a systematic review of reports meeting quality standards, Int. Psychogeriatr 21 (2) (2009) 241–251, 10.1017/S1041610208008223. [DOI] [PubMed] [Google Scholar]
- [19].O’Neil ME, Freeman M, Christensen V, Telerant R, Addleman A, Kansagara D, A Systematic Evidence Review of Non-pharmacological Interventions for Behavioral Symptoms of Dementia, Department of Veterans Affairs (US), 2011, http://www.ncbi.nlm.nih.gov/pubmed/21634073 , Accessed date: 10 May 2017. [PubMed] [Google Scholar]
- [20].Bond M, Rogers G, Peters J, et al. , The effectiveness and cost-effectiveness of donepezil, galantamine, rivastigmine and memantine for the treatment of Alzheimer’s disease (review of Technology Appraisal No. 111): a systematic review and economic model, Health Technol. Assess 16 (21) (2012) 1–470, 10.3310/hta16210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Committee AGSCP, Guidelines abstracted from the American Academy of Neurology’s Dementia Guidelines for Early Detection, Diagnosis, and Management of Dementia, J. Am. Geriatr. Soc 51 (6) (2003) 869–873, 10.1046/j.1365-2389.2003.51272.x. [DOI] [PubMed] [Google Scholar]
- [22].Lyketsos CG, Colenda CC, Beck C, et al. , Position statement of the American Association for Geriatric Psychiatry regarding principles of care for patients with dementia resulting from Alzheimer disease, Am. J. Geriatr. Psychiatry 14 (7) (2006) 561–572, 10.1097/01.JGP.0000221334.65330.55. [DOI] [PubMed] [Google Scholar]
- [23].Gould N, Guidelines across the health and social care divides: the example of the NICE-SCIE dementia guideline, Int. Rev. Psychiatry 23 (4) (2011) 365–370, 10.3109/09540261.2011.606537. [DOI] [PubMed] [Google Scholar]
- [24].Sorbi S, Hort J, Erkinjuntti T, et al. , EFNS-ENS guidelines on the diagnosis and management of disorders associated with dementia, Eur. J. Neurol 19 (9) (2012) 1159–1179, 10.1111/j.1468-1331.2012.03784.x. [DOI] [PubMed] [Google Scholar]
- [25].Waldemar G, Dubois B, Emre M, et al. , Recommendations for the diagnosis and management of Alzheimer’s disease and other disorders associated with dementia: EFNS guideline, Eur J Neurol 14 (1) (2007), 10.1111/j.1468-1331.2006.01605.x. [DOI] [PubMed] [Google Scholar]
- [26].Borson S, Chodosh J, Developing Dementia-capable Health Care Systems: A 12- Step Program, (2014), 10.1016/j.cger.2014.05.001. [DOI] [PubMed] [Google Scholar]
- [27].Callahan CM, Hendrie HC, Documentation and evaluation of cognitive impairment in elderly primary care patients, Ann. Intern. Med 122 (6) (1995) 422, 10.7326/0003-4819-122-6-199503150-00004. [DOI] [PubMed] [Google Scholar]
- [28].Boustani M, Callahan CM, Unverzagt FW, et al. , Implementing a screening and diagnosis program for dementia in primary care, J. Gen. Intern. Med 20 (7) (2005) 572–577, 10.1111/j.1525-1497.2005.0126.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Gaugler JE, Kane RL, Kane RA, Newcomer R, Unmet care needs and key outcomes in dementia, J. Am. Geriatr. Soc 53 (12) (2005) 2098–2105, 10.1111/j.1532-5415.2005.00495.x. [DOI] [PubMed] [Google Scholar]
- [30].Miranda-Castillo C, Woods B, Orrell M, The needs of people with dementia living at home from user, caregiver and professional perspectives: a cross-sectional survey, BMC Health Serv. Res 13 (1) (2013) 43, 10.1186/1472-6963-13-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Black BS, Johnston D, Rabins PV, Morrison A, Lyketsos C, Samus QM, Unmet needs of community-residing persons with dementia and their informal caregivers: findings from the maximizing independence at home study, J. Am. Geriatr. Soc 61 (12) (2013) 2087–2095, 10.1111/jgs.12549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Pimouguet C, Lavaud T, Dartigues JF, Helmer C, Dementia case management effectiveness on health care costs and resource utilization: a systematic review of randomized controlled trials, J. Nutr. Health Aging 14 (8) (2010) 669–676, 10.1007/s12603-010-0314-4. [DOI] [PubMed] [Google Scholar]
- [33].Somme D, Trouve H, Dramé M, Gagnon D, Couturier Y, Saint-Jean O, Analysis of case management programs for patients with dementia: {A} systematic review, Alzheimers Dement 8 (5) (2012) 426–436, 10.1016/j.jalz.2011.06.004. [DOI] [PubMed] [Google Scholar]
- [34].Hickam DH, Weiss JW, Guise JM, et al. , Outpatient case management for adults with medical illness and complex care needs, Compar. Effect. Rev 99 (2013), http://effectivehealthcare.ahrq.gov/index.cfm/search-for-guides-reviews-and-reports/?pageaction=displayproduct&productid=1369. [PubMed] [Google Scholar]
- [35].Tam-Tham H, Cepoiu-Martin M, Ronksley PE, Maxwell CJ, Hemmelgarn BR, Dementia case management and risk of long-term care placement: a systematic review and meta-analysis, Int. J. Geriatr. Psychiatry 28 (9) (2013) 889–902, 10.1002/Gps.3906. [DOI] [PubMed] [Google Scholar]
- [36].Reilly S, Miranda-Castillo C, Malouf R, et al. , Case management approaches to home support for people with dementia, in: Reilly S (Ed.), Cochrane Database of Systematic Reviews, 1 John Wiley & Sons, Ltd, Chichester, UK, 2015CD008345, , , 10.1002/14651858.CD008345.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Samus QM, Johnston D, Black BS, et al. , A multidimensional home-based care coordination intervention for elders with memory disorders: the maximizing independence at home (MIND) pilot randomized trial, Am. J. Geriatr. Psychiatry 22 (4) (2014) 398–414, 10.1016/j.jagp.2013.12.175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Samus QM, Davis K, Willink A, et al. , Comprehensive home-based care coordination for vulnerable elders with dementia: maximizing independence at home plus—study protocol, Int. J. Care Coord 20 (4) (2017), 10.1177/2053434517744071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Callahan CM, Boustani MA, Unverzagt FW, et al. , Effectiveness of collaborative care for older adults with Alzheimer disease in primary care: a randomized controlled trial, JAMA 295 (18) (2006) 2148–2157, 10.1001/jama.295.18.2148. [DOI] [PubMed] [Google Scholar]
- [40].Vickrey BG, Mittman BS, Connor KI, et al. , The effect of a disease management intervention on quality and outcomes of dementia care: a randomized, controlled trial, Ann. Intern. Med 145 (2006) 713 http://search.ebscohost.com/login.aspx?direct=true&db=jlh&AN=2009348647&site=ehost-live. [DOI] [PubMed] [Google Scholar]
- [41].Menne HL, Bass DM, Johnson JD, Kearney KR, Bollin S, Teri L, Program components and outcomes of individuals with dementia: results from the replication of an evidence-based program, J. Appl. Gerontol 36 (5) (2017) 537–552, 10.1177/0733464815591212. [DOI] [PubMed] [Google Scholar]
- [42].Possin KL, Merrilees J, Bonasera SJ, et al. , Development of an adaptive, personalized, and scalable dementia care program: early findings from the Care Ecosystem, PLoS Med 14 (3) (2017) e1002260, , 10.1371/journal.pmed.1002260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Johnston D, Samus QM, Morrison A, et al. , Identification of community-residing individuals with dementia and their unmet needs for care, Int. J. Geriatr. Psychiatry 26 (3) (2011) 292–298, 10.1002/gps.2527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Samus QM, Johnston D, Black BS, et al. , A multidimensional home-based care coordination intervention for elders with memory disorders: the maximizing independence at home (MIND) pilot randomized trial, Am. J. Geriatr. Psychiatry 22 (4) (2014) 398–414, 10.1016/j.jagp.2013.12.175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Tanner JA, Black BS, Johnston D, et al. , A randomized controlled trial of a community-based dementia care coordination intervention: effects of MIND at home on caregiver outcomes, Am. J. Geriatr. Psychiatry 23 (4) (2015) 391–402, 10.1016/j.jagp.2014.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [46].Chin AL, Negash S, Hamilton R, Diversity and disparity in dementia: the impact of ethnoracial differences in Alzheimer disease, Alzheimer Dis. Assoc. Disord 25 (3) (2011) 187–195, 10.1097/WAD.0b013e318211c6c9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Russ TC, Stamatakis E, Hamer M, Starr JM, Kivimäki M, Batty GD, Socioeconomic status as a risk factor for dementia death: individual participant meta-analysis of 86 508 men and women from the UK, Br. J. Psychiatry 203 (1) (2013) 10–17, 10.1192/bjp.bp.112.119479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [48].Adams K, Greiner AC, Corrigan JM, Crossing the quality chasm: next steps toward a new health care system, US Inst. Med 1 (2004) 19–23 http://www.ncbi.nlm.nih.gov/books/NBK215516/. [Google Scholar]
- [49].E. W. Care of Older People with Chronic Illness, New Ways to Care for Older People: Building Systems Based on Evidence, Springer, New York, 1999, pp. 39–64. [Google Scholar]
- [50].McKhann G, Knopman D, The diagnosis of dementia due to alzheimer’s disease: recommendations from the national institute on aging-alzheimer’s association workgroups on, Alzheimer’s 7 (3) (2011) 263–269, 10.1016/j.jalz.2011.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Samus QM, Amjad H, Johnston D, Black BS, Bartels SJ, Lyketsos CG, A multipronged, adaptive approach for the recruitment of diverse community-residing elders with memory impairment: the MIND at home experience, Am. J. Geriatr. Psychiatry 23 (7) (2015) 698–708, 10.1016/j.jagp.2015.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Brandt J, Spencer M, Folstein M, The telephone interview for cognitive status, Neuropsychiatry Neuropsychol. Behav. Neurol 1 (2) (1988) 111–117. [Google Scholar]
- [53].Jorm AF, Jacomb PA, The informant questionnaire on cognitive decline in the elderly (IQCODE): socio-demographic correlates, reliability, validity and some norms, Psychol. Med 19 (4) (1989) 1015–1022, 10.1017/S0033291700005742. [DOI] [PubMed] [Google Scholar]
- [54].Jorm AF, Broe GA, Creasey H, et al. , Further data on the validity of the informant questionnaire on cognitive decline in the elderly (IQCODE), Int. J. Geriatr. Psychiatry 11 (2) (1996) 131–139, 10.1002/(SICI)1099-1166(199602)11:2<131::AID-GPS294>3.0.CO;2-5. [DOI] [Google Scholar]
- [55].Wilkinson IM, Graham-White J, Psychogeriatric dependency rating scales (PGDRS). A method of assessment for use by nurses, Br. J. Psychiatry 137 (6) (1980) 558–565, 10.1192/bjp.137.6.558. [DOI] [PubMed] [Google Scholar]
- [56].Lyketsos CG, Galik E, Steele C, et al. , The general medical health rating: a bedside global rating of medical comorbidity in patients with dementia, J. Am. Geriatr. Soc 47 (4) (1999) 487–491 http://www.ncbi.nlm.nih.gov/pubmed/10203127 , Accessed date: 27 March 2018. [DOI] [PubMed] [Google Scholar]
- [57].Folstein MF, Folstein SE, McHugh PR, "Mini-mental state". A practical method for grading the cognitive state of patients for the clinician, J. Psychiatr. Res 12 (3) (1975) 189–198 http://www.ncbi.nlm.nih.gov/pubmed/1202204 , Accessed date: 22 May 2017. [DOI] [PubMed] [Google Scholar]
- [58].Wimo A, Wetterholm AL, Mastey V, Winblad B, Evaluation of the resource utilization and caregiver time in anti-dementia drug trials—a quantitative battery, Health Econ. Dement (1998) 465–499. [Google Scholar]
- [59].Schneider LS, Ismail MS, Dagerman K, et al. , Clinical antipsychotic trials of intervention effectiveness (CATIE): Alzheimer’s disease trial, Schizophr. Bull 29 (1) (2003) 57–72 http://www.ncbi.nlm.nih.gov/pubmed/12908661 , Accessed date: 29 March 2018. [DOI] [PubMed] [Google Scholar]
- [60]. National Fee Analyzer, Charge Data for Evaluating Fees Nationally, (2011).
- [61].Agency for Healthcare Research and Quality. HCUPNet www.hcupnet.arhq.gov. Published 2012. Accessed January 21, 2013. [Google Scholar]
- [62].Rosenheck RA, Leslie DL, Sindelar JL, et al. , Cost-benefit analysis of second-generation antipsychotics and placebo in a randomized trial of the treatment of psychosis and aggression in alzheimer disease, Arch. Gen. Psychiatry 64 (11) (2007) 1259–1268, 10.1001/archpsyc.64.11.1259. [DOI] [PubMed] [Google Scholar]
- [63].Horsman J, Furlong W, Feeny D, Torrance G, The Health Utilities Index (HUI): concepts, measurement properties and applications, Heal Qual. Life Outcomes 1 (2003) 54, 10.1186/1477-7525-1-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [64].Gitlin LN, Harris LF, McCoy M, Chernett NL, Jutkowitz E, Pizzi LT, A community-integrated home based depression intervention for older African Americans: [corrected] description of the beat the blues randomized trial and intervention costs, BMC Geriatr 12 (2012) 4, 10.1186/1471-2318-12-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Black BS, Johnston D, Morrison A, Rabins PV, Lyketsos CG, Samus QM, Quality of life of community-residing persons with dementia based on self-rated and caregiver-rated measures, Qual. Life Res 21 (8) (2012) 1379–1389, 10.1007/s11136-011-0044-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [66].Hughes TB, Black BS, Albert M, et al. , Correlates of objective and subjective measures of caregiver burden among dementia caregivers: Influence of unmet patient and caregiver dementia-related care needs, Int. Psychogeriatrics 26 (11) (2014), 10.1017/S1041610214001240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [67].Cox DR, Regression models and life tables, J. R. Stat. Soc. Ser. B 34 (2) (1972) 187–220. [Google Scholar]
- [68].Schoenfeld D, Partial residuals for the Proportionnal hazards regression model, Biometrika 69 (1) (1982) 239–241 http://www.jstor.org/stable/2335876. [Google Scholar]
- [69].Szychowski JM, Roth DL, Clay OJ, Mittelman MS, Patient death as a censoring event or competing risk event in models of nursing home placement, Stat. Med 29 (3) (2010) 371–381, 10.1002/sim.3797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Roth DL, MacKinnon DP, Mediation analysis with longitudinal data, Longitudinal Data Analysis: A Practical Guide for Researchers in Aging, Health, and Social Sciences, vol. 18, 2012, pp. 181–216 https://login.pallas2.tcl.sc.edu/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=2011-16366-006&site=ehost-live. [Google Scholar]
- [71].Drummond M, Stoddard GL, Torrance GW, Methods for the Economic Evaluation of Health Care Programmes, (2015). [Google Scholar]
- [72].Gold MR, Siegel JE, Russell LB, Weinstein MC, Cost-Effectiveness in Health and Medicine, vol. 2, (1996), 10.1002/(SICI)1099-176X(199906)2:2<91::AID-MHP46>3.0.CO;2-I. [DOI] [PubMed] [Google Scholar]
- [73].Laird NM, Ware JH, Random-effects models for longitudinal data, Biometrics 38 (4) (1982) 963–974, 10.1111/j.1541-0420.2005.00440.x. [DOI] [PubMed] [Google Scholar]
- [74].Schoenfeld DA, Sample-size formula for the proportional-hazards regression model, Biometrics 39 (2) (1983) 499–503, 10.2307/2531021. [DOI] [PubMed] [Google Scholar]