

Abstract
Background:
A mismatch between the prosthesis size and bone may result in a number of complications. Keeping this in view, it is essential to analyze the morphological differences of the knee observed across various ethnic groups to improve the performance of total knee arthroplasty (TKA). The current study was aimed at studying the computed tomography (CT) profile of distal femur in Indian population and evaluates it morphologically.
Materials and Methods:
This descriptive study was conducted on 62 patients presenting to the Department of Orthopedics in a tertiary care center in rural north-west India for features suggestive of osteoarthritis and trauma of knee from September 17, 2015 to September 16, 2016. Helical CT of both knees was done, and the data were analyzed using Statistical Package for Social Sciences Version 17.0 statistical significance was assessed with the help of t-test and the value of P < 0.05 was considered to be statistically significant.
Results:
The mean mediolateral (ML) value in male patients was 72.74 ± 4.45 while the mean ML value in female patients was lower (63.59 ± 2.61). The mean anteroposterior (AP) value in male patients was significantly (statistically) higher (49.62 ± 3.86) in comparison to mean AP value in female patients (45.11 ± 4.4). The mean anterior lateral condylar height (ALCH) value in male patients was higher (17.53 ± 2.72) in comparison to mean ALCH value in female patients (14.63 ± 3.42).
Conclusions:
The current study highlights the need to develop components and implants for use in TKA and fractures of distal femur keeping the age- and sex-specific anatomical features of people of different ethnic origins in view.
Keywords: Helical computed tomography, lower end femur, morphometric, study
Introduction
Manufacturing of the prosthesis for total knee arthroplasty (TKA) requires anthropometric measurements of the femoral as well as tibial components. In the sizing of the femoral component, the anteroposterior (AP) diameter is important in maintaining flexion extension spacing and optimal tension in the quadriceps mechanism, whereas the mediolateral (ML) diameter determines adequate coverage of the resected bone surface.1 Component oversizing in the AP dimension alters the delicate balance in flexion extension spacing resulting in flexion tightness postoperatively.
Implants essentially designed for TKA of the Western population are currently being used without modifications for the Asian population as well.2 However, smaller build and stature of the Asian-Pacific population gives rise to TKA component mismatch.3 A mismatch between the prosthesis size and bone may result in a number of complications such as implant loosening and impingement of the surrounding soft tissues.3 Keeping this in view, it is essential to analyze the morphological differences of the knee observed across various ethnic groups to improve the performance of TKA. The current study aimed at morphologic characterization of the distal femur in Indian population. The study assumes significance in view of the outcome of our previous study on anthropometric characterization of elbow angles in children from our part of India.4
Materials and Methods
This descriptive study was conducted on 62 patients presenting to the Department of Orthopedics at a tertiary care center in rural north-west India for features suggestive of osteoarthritis and trauma of knee between 17th September 2015 and 16th September 2016. All patients of age 18 years and above with osteoarthritis of the knee joint with contralateral normal knee and patients undergoing computed tomography (CT) knee for trauma evaluation with contralateral normal knee were included in the study. All patients with gross osteoarthritis (both knees) whose morphology has been altered, patients with postoperative knee with or without implant in situ, patients with congenital or developmental anomalies of the knee, patients having knee flexion deformities >10° and patients with polyarticular arthritis such as rheumatoid arthritis and ankylosing spondylitis were excluded from the study. In case of trauma knee patient's contralateral normal knee was included and the traumatic knee was excluded from the study. Gross osteoarthritis was defined using Kellgren and Lawrence classification and patients with osteoarthritis Grade 3 and 4 were excluded from the study.5
Written informed consent was obtained from all the patients and attendants included in the study. The patients were given the right to abstain from participation in the study or to withdraw at any time of the study without reprisal. Each patient and his attendants were adequately informed of the aim, methods, the anticipated benefits, potential risks of the study, the discomfort it may entail them and the remedies thereof.
The study subjects were placed in the supine position on the CT table with fully extended knee joint with patella facing the sky for CT examination. Helical CT of both knees was done and the images of the knees were analyzed at an advanced workstation in the Department of Radiodiagnosis. Measurement of the parameters was performed by a team comprising of one member from the Department of Orthopedics and the other from the Department of Radiodiagnosis. The process of measurement was supervised by two consulting orthopedicians and one consulting radiologist. Following parameters of distal femur were noted in each patient.
ML dimension
AP dimension
Anterior lateral condylar height (ALCH)
Anterior medial condylar height (AMCH)
Femoral aspect ratio (FAR).
The measurements were taken with the help of digital scale of CT console room monitor. The AP dimension was measured for both medial and lateral femoral condyle. While measuring the AP dimension, we excluded the anterior medial condylar height (AMCH) and ALCH as shown in Figure 1.
Figure 1.
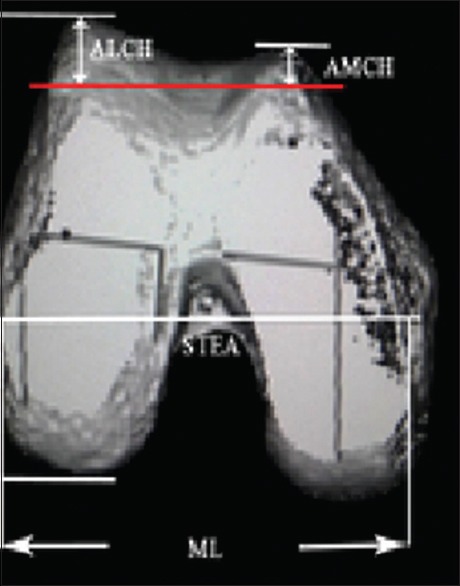
Different distal femoral parameters
Statistical analysis
A database of all registered patients was maintained and entered into MS Excel 2007. The statistical analysis was performed using Statistical Package for Social Sciences Version 17.0 (IBM, Armonk, New York, United States,) and result had been expressed using percentage. Statistical significance was assessed with the help of t-test and the value of P < 0.05 was considered as statistically significant.
Results
Table 1 and Graph 1 show the distribution of morphometric profile in male and female study participants. Out of 62 patients, majority (n = 48/62; 77.4%) of patients were male. The mean ML value in male patients was 72.74 ± 4.45, whereas the mean ML value in female patients was lower (63.59 ± 2.61) with an interquartile range of 4.75 and 2.82, respectively. The difference in ML dimension between male and female was statistically significant (P = 0.00). The mean AP value in male patients was significantly higher (49.62 ± 3.86) in comparison to mean AP value in female patients (45.11 ± 4.4).
Table 1.
Distribution of morphometric profile in males and females
| No of Pt. | Male 48 (77.4%) | Female 14 (22.6%) | t-test | P | Statistical significance | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | IQR | Mean | Median | SD | IQR | ||||
| ML | 72.74 | 73.2 | 4.45 | 4.75 | 63.59 | 64.55 | 2.61 | 2.82 | 5.67 | 0.00 | Sig. |
| AP | 49.62 | 49.05 | 3.86 | 2.67 | 45.11 | 45.45 | 4.4 | 2.37 | 3.72 | 0.00 | Sig. |
| ALCH | 17.53 | 17.55 | 2.72 | 2.35 | 14.63 | 13.5 | 3.42 | 4.05 | 3.526 | 0.00 | Sig |
| AMCH | 9.82 | 9.7 | 1.88 | 1.82 | 8.92 | 8.7 | 2.49 | 0.57 | 1.55 | 0.12 | Non Sig. |
| Aspect Ratio | 1.47 | 1.47 | 0.11 | 0.05 | 1.42 | 1.42 | 0.12 | 0.07 | 1.57 | 0.12 | Non Sig. |
Graph 1.
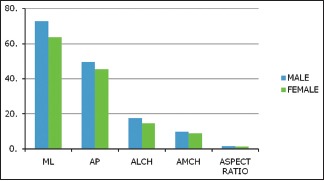
Distribution of morphometric profile in males and females
The mean ALCH value in male patients was higher (17.53 ± 2.72) in comparison to mean ALCH value in female patients (14.63 ± 3.42). The difference in ALCH value between male and female was statistically significant (P = 0.00). The mean AMCH value in male and female patients was 9.82 ± 1.88 and 8.92 ± 2.49, respectively. The femoral aspect ratio in male and female patients was 1.47 with 0.11 and 1.42 with 0.07. The difference in AMCH value and aspect ratio was not significant statistically (P ≥ 0.5).
Table 2a and b and Graph 2 show the distribution of morphometric profile in patients of different age groups. The mean ML value in the age group of 18–30, 31–45, 46–60 and >60 were 72.82 ± 4.81, 70.74 ± 5.07, 68.39 ± 6.41, and 69.24 ± 5.66 with an interquartile range of 1, 3, 5.8, and 9. The mean ML value in the age group of 18–30 and 31–45 was higher (72.82 ± 4.81 and 70.74 ± 5.07) in comparison to mean ML value in the age group of 46–60 and >60 (68.39 ± 6.41 and 69.24 ± 5.66). The difference in mean ML value between different age group was statistically significant (P = 0.01). The mean AP value in the age group of 18–30, 31–45, 46–60, and >60 were 51.6 ± 4.17, 47.2 ± 3.66, 46.5 ± 3.95, and 47.7 ± 2.35 with an interquartile range of 3.42, 1.9, 1.2, and 2.1. The mean AP value in the age group of 18–30 and 31–45 was higher (51.6 ± 4.17 and 47.2 ± 3.66) in comparison to mean AP value in the age group of 46–60 and >60 (46.5 ± 3.95 and 47.7 ± 2.35). The difference in mean AP value between different age group was statistically significant (P = 0.00). The lowest value of ML dimension was observed in the age group of 46–60 years and lowest value of AP dimension were observed in the age group of >60 years. This table also shows that there is no significant (P > 0.05) difference in ALCH, AMCH, and ASPECT RATIO values with increasing age.
Table 2a.
The distribution of morphometric profile with age
| Age group | No. of PT (%) | ML dimension | AP dimension | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | SD | IQR | Mean | Median | SD | IQR | ||
| 18-30 | 22 (35) | 72.82 | 74.33 | 4.81 | 1 | 51.6 | 50.7 | 4.17 | 3.42 |
| 31-45 | 18 (29) | 70.74 | 71.4 | 5.07 | 3 | 47.2 | 47.4 | 3.66 | 1.9 |
| 46-60 | 17 (27) | 68.39 | 66.1 | 6.41 | 5.8 | 46.5 | 46.9 | 3.95 | 1.2 |
| >60 | 5 (8) | 69.24 | 65.9 | 5.66 | 9 | 47.7 | 47.7 | 2.35 | 2.1 |
| t test | 3.64 | 6.74 | |||||||
| P value | 0.01 | 0.00 | |||||||
| Statistical Significance | Significant | Significant | |||||||
Table 2b.
The distribution of morphometric profile with age
| Age group | No of PT(%) | ALCH | AMCH | Aspect ratio | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Med | SD | IQR | Mean | Med | SD | IQR | Mean | Med | SD | IQR | ||
| 18-30 | 22 (35%) | 17.28 | 17.6 | 3.35 | 2.55 | 10.1 | 10.6 | 1.97 | 1.4 | 1.41 | 1.44 | 0.1 | 0.04 |
| 31-45 | 18 (29%) | 16.62 | 16.9 | 2.85 | 1.6 | 9.41 | 9.2 | 2.42 | 2.7 | 1.5 | 1.48 | 0.09 | 0.08 |
| 46-60 | 17 (27%) | 16.22 | 16.7 | 3.3 | 1.62 | 8.86 | 8.7 | 1.16 | 0.8 | 1.47 | 1.45 | 0.14 | 0.11 |
| >60 | 5 (8%) | 18.28 | 18.7 | 2.03 | 0.4 | 10.9 | 9.4 | 2.87 | 3.3 | 1.45 | 1.45 | 0.1 | 0.05 |
| t test | 0.74 | 1.95 | 2.20 | ||||||||||
| P value | 0.53 | 0.13 | 0.09 | ||||||||||
| Statistical Significance | non significant | non significant | non significant | ||||||||||
Graph 2.
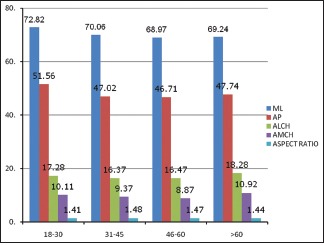
Distribution of morphometric profile with age
Discussion
The present study was conducted with the aim of evaluating the morphometric profile of lower end femur using helical CT in patients of age 18 years and above with trauma or osteoarthritis of the knee to the Department of Orthopedics of a tertiary care centre in north-west India. Extensive PubMed search revealed the paucity of data on morphometry of lower end femur in the Indian context.
It has been observed in our study that there is an incremental reduction in AP and ML dimension of lower end femur. Importantly, this reduction with an increase in age was found to significant statistically. The study findings are in line with the argument that human height has steadily increased over the past two centuries across the globe and India is no exception to this global trend. This is due to the general improvements in health and nutritional status across populations reflecting in younger populations on average being taller than older populations.6 Humans are significantly taller today than in mid-19 century which is reflected in the relatively smaller bone size in the older population in our study.
The study points to a difference in femoral ML and femoral AP dimensions between male and female participants with males reporting higher values as compared to female participants. Previous studies in this regard have reported with variable results. However, a majority of studies conducted across the globe report that values for ML and AP dimension are more in males in comparison to females,7,8,9,10,11,12 which is similar to the findings from the study. Detail on the comparison of the morphological record of different populations is as under Table 3.
Table 3.
Comparison of the morphological data with those reported in literature
| Asian | Caucasian | ||||
|---|---|---|---|---|---|
| Authors | ML | AP | Authors | ML | AP |
| Vaidya et al., 200013 (Indian) | 61.09 (male) | Lonner et al., 200810 (American) | 76.9 (male) | 62.27 (male) | |
| 55.58 (female) | 67.49 (female) | 56.32 (female) | |||
| Cheng et al., 200914 (Chinese) | 74.4±2.9 (male) | 66.6±2.4 (male) | Yue et al., 20117 (American) | 74.6±3.9 (male) | 59.6±3.2 (male) |
| 66.8±3.11 (female) | 61.0±24.6 (female) | 65.4±1.4 (female) | 55.4±2.8 (female) | ||
| Ha and Na, 201215 (Korean) | 74.8 (male) | 66.3 (male) | |||
| 68.2 (female) | 60.8 (female) | ||||
| Yue et al., 20117 (Chinese) | 72.7±3.8 (male) | 56.5±2.5 (male) | |||
| 64.4±2.6 (female) | 52.8±2.6 (female) | ||||
| Our study | 72.74±4.45 (male) | 49.62±3.86 (male) | |||
| 63.592.61 (female) | 45.11±4.4 (female) | ||||
ML=Mediolateral, AP=Anteroposterior
An analysis of this data reveals that the ML and AP diameter in our study population is almost similar to the diameters reported on Chinese population in a study conducted in 2014, although the diameters reported for the females are different in two studies. However, the diameters are much smaller than the one reported in an earlier study on Chinese population conducted in the year 2009. A comparison of the data obtained from our study with the studies conducted on Korean population reveals that the diameters for our population are much smaller than the ones reported for Korean population. The differences are all the more important when a comparison is established with data obtained from studies on the American population. In India, people reach adult height in the early twenties, much later than the United States and societies with better nutritional status and eventually tend to be much smaller in height, a possible reasons for the difference in diameters.16
Significantly, however, Vaidya et al. from Mumbai report mean femoral AP dimension in males and females 61.09 and 55.58 mm, respectively, which is about 10 mm higher than our findings.13 This despite the fact that in most Indian states (Including Maharashtra and Himachal Pradesh), both men and women states have grown taller over time with men growing more than women. Therefore the probable reason for this difference in two Indian population groups may be because of noninclusion of the height of anterior condyle of the femur in AP dimension in case our study [Figure 1].
Limitations
A small sample size could limit the extrapolation of the study findings to a large population base. Nevertheless the study does provide some insight regarding morphometry of Indian Lower End Femur.
Conclusions
The current study highlights the need to develop components and implants for use in TKA and fractures of distal femur keeping the age- and sex-specific anatomical features of people of India in view.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jain JP. Knee prosthesis sizes in Indian patients undergoing total knee replacement. Int Surg J. 2015;2:348–51. [Google Scholar]
- 2.Uehara K, Kadoya Y, Kobayashi A, Ohashi H, Yamano Y. Anthropometry of the proximal tibia to design a total knee prosthesis for the Japanese population. J Arthroplasty. 2002;17:1028–32. doi: 10.1054/arth.2002.35790. [DOI] [PubMed] [Google Scholar]
- 3.Hussain F, Abdul Kadir MR, Zulkifly AH, Sa’at A, Aziz AA, Hossain G, et al. Anthropometric measurements of the human distal femur: A study of the adult Malay population. Biomed Res Int. 2013;2013:175056. doi: 10.1155/2013/175056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Awasthi B, Raina SK, Chauhan N, Sehgal M, Sharma V, Thakur L. Anthropometric characterisation of elbow angles and lines among Indian children. Adv Hum Biol. 2017;7:71–4. [Google Scholar]
- 5.Schiphof D, Boers M, Bierma-Zeinstra SM. Differences in descriptions of Kellgren and Lawrence grades of knee osteoarthritis. Ann Rheum Dis. 2008;67:1034–6. doi: 10.1136/ard.2007.079020. [DOI] [PubMed] [Google Scholar]
- 6.Roser M. Human Height. [Last accessed on 2017 Jul 14]. Available from: https://www.ourworldindata.org/human-height .
- 7.Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li G, et al. Differences of knee anthropometry between Chinese and white men and women. J Arthroplasty. 2011;26:124–30. doi: 10.1016/j.arth.2009.11.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hitt K, Shurman JR, 2nd, Greene K, McCarthy J, Moskal J, Hoeman T, et al. Anthropometric measurements of the human knee: Correlation to the sizing of current knee arthroplasty systems. J Bone Joint Surg Am. 2003;85-A(Suppl 4):115–22. [PubMed] [Google Scholar]
- 9.Clarke HD, Hentz JG. Restoration of femoral anatomy in TKA with unisex and gender-specific components. Clin Orthop Relat Res. 2008;466:2711–6. doi: 10.1007/s11999-008-0454-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lonner JH, Jasko JG, Thomas BS. Anthropomorphic differences between the distal femora of men and women. Clin Orthop Relat Res. 2008;466:2724–9. doi: 10.1007/s11999-008-0415-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chin PL, Tey TT, Ibrahim MY, Chia SL, Yeo SJ, Lo NN, et al. Intraoperative morphometric study of gender differences in Asian femurs. J Arthroplasty. 2011;26:984–8. doi: 10.1016/j.arth.2010.11.012. [DOI] [PubMed] [Google Scholar]
- 12.Ho WP, Cheng CK, Liau JJ. Morphometric measurements of resected surface of femurs in Chinese knees: Correlation to the sizing of current femoral implants. Knee. 2006;13:12–4. doi: 10.1016/j.knee.2005.05.002. [DOI] [PubMed] [Google Scholar]
- 13.Vaidya SV, Ranawat CS, Aroojis A, Laud NS. Anthropometric measurements to design total knee prostheses for the Indian population. J Arthroplasty. 2000;15:79–85. doi: 10.1016/s0883-5403(00)91285-3. [DOI] [PubMed] [Google Scholar]
- 14.Cheng FB, Ji XF, Lai Y, Feng JC, Zheng WX, Sun YF, et al. Three dimensional morphometry of the knee to design the total knee arthroplasty for Chinese population. Knee. 2009;16:341–7. doi: 10.1016/j.knee.2008.12.019. [DOI] [PubMed] [Google Scholar]
- 15.Ha CW, Na SE. The correctness of fit of current total knee prostheses compared with intra-operative anthropometric measurements in Korean knees. J Bone Joint Surg Br. 2012;94:638–41. doi: 10.1302/0301-620X.94B5.28824. [DOI] [PubMed] [Google Scholar]
- 16.Deaton A. Height, health, and inequality: The distribution of adult heights in India. Am Econ Rev. 2008;98:468–74. doi: 10.1257/aer.98.2.468. [DOI] [PMC free article] [PubMed] [Google Scholar]