

Summary:
Cutaneous myxoma is a rare neoplasm typically occurring as an asymptomatic nodule on the head, neck, and chest regions of adults. However, multiple cutaneous myxoma of the subungual space is even rarer. Here, we report a case of multiple cutaneous myxoma of the subungual space in which the tumor was removed by creating a mid-radial incision while preserving the nail matrix. The excisional biopsy samples were dispatched for histopathological examination and confirmed to be cutaneous myxoma. To the best of our knowledge, this is the first report on multiple cutaneous myxoma of the subungual space.
CASE REPORT
A 41-year-old man presented with complaints of continuous radiating pain in the right ring finger for the past year. The fingertip was excessively sensitive to touch and demonstrated localized tenderness. The patient could not recall any apparent trauma to the finger that could have contributed to the pain. Physical examination revealed a purple spot at the center of the nail plate and a lesion (0.3 cm in diameter) that was extremely painful when touched. X-ray examination showed a pale cystic lesion but no bony lesions. Magnetic resonance imaging of the right ring finger revealed a round 8.0 × 3.0 × 3.0 mm T1-hypointense and T2-hyperintense soft-tissue lesion (Fig. 1). The patient was conservatively treated with nonsteroidal anti-inflammatory drugs, but no response was achieved even after 1 month. Hence, we performed excisional biopsy of the lesion to make a definitive diagnosis and relieve the patient’s pain.
Fig. 1.
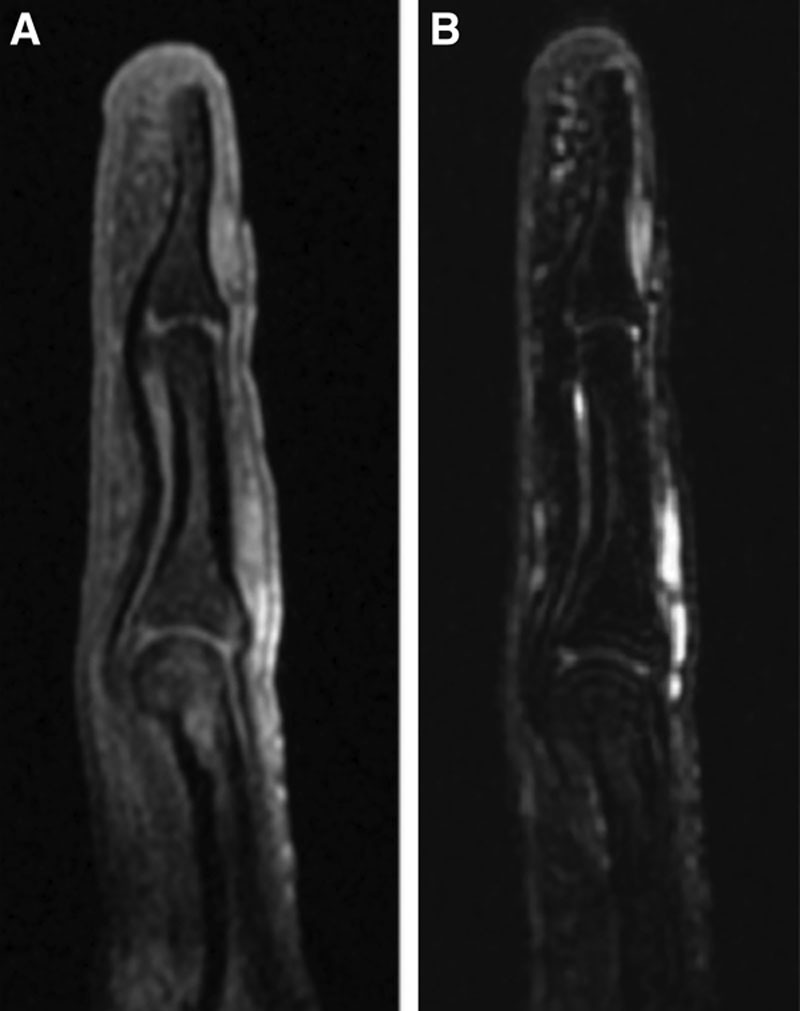
Preoperative magnetic resonance image showing the lesion at the subungual region of the right ring finger. A, T1-weighted image. B, T2-weighted image.
The surgery consisted of excision of the lesion with a modified transthecal digital block. The excision was performed via a mid-radial incision. The nail plate was carefully elevated with a mosquito hemostat to preserve the nail matrix. The dissection was straight rather than dorsal to avoid puncturing the matrix at the nail fold. Intraoperatively, removal of the nail plate exposed an elastic soft tissue (4 mm in diameter) tumor, which was then subjected to resection and biopsy at 3 points. We performed partial resection because total resection of the lesion was difficult. The nail bed was approximated with 6-0 PDS sutures, and the nail plate was repositioned using 5-0 nylon sutures.
Histopathological examination confirmed that the 3 excisional biopsies demonstrated cutaneous myxoma described as well-circumscribed dermal tumors composed of stellate and dendritic cells embedded in a mucinous stroma (Fig. 2). The excisional biopsy samples were dispatched for histopathological examination and confirmed to be cutaneous myxoma.
Fig. 2.
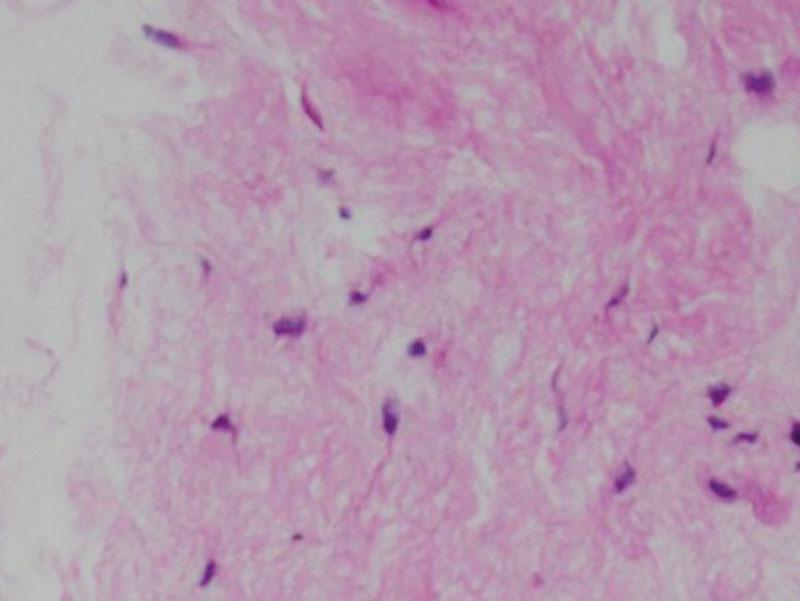
Hypercellular and myxoid areas of spindle and stellate cells (hematoxylin and eosin stain: magnification 40×).
The patient’s symptoms improved on tumor removal, and he healed without any complication. His last follow-up examination at 6 months revealed no evidence of recurrence (Fig. 3).
Fig. 3.

Image of the right ring finger at 6-month follow-up examination.
DISCUSSION
In general, subungual glomus tumors are a rare occurrence.1 Moreover, cutaneous myxoma of the subungual space is an even more uncommon entity. Only 4 cases of myxoma involving the fingertip and 2 involving the palm have been reported.2 There are no reports on multiple cutaneous myxoma of the subungual space.
Most myxomas are detected in the heart, skeletal muscles of the lower limbs, and jaw bones. Myxomas of the upper limbs are extremely rare. Cutaneous myxoma is classified as a specific neoplasm since its detection in a patient with Carney complex.3 Solitary cutaneous myxomas are not typically associated with Carney complex but present as cutaneous or subcutaneous nodules primarily on the skin of the distal areas of the limbs or head.4
Skin and cutaneous tissue involvement of myxoma in the pulp of the finger has been previously reported.5 In the present case, the tumor was involved the cutaneous tissue of the subungual region of the finger. The myxoma demonstrated no secondary bone, tendon, or neurovascular involvement. Sponsel et al.6 classified the clinical behavior and prognosis of myxoma of the extremities into benign, malignant, and intermediate types. Interestingly, benign myxoma may infiltrate a small area of the adjacent structures; hence, it requires sufficient excision and long-term follow-up to monitor for potential recurrence.
The most serious manifestation of Carney complex is cardiac myxoma, which accounts for approximately one-third of the patient population.7 Therefore, patients presenting with similar symptoms should be screened for cutaneous cardiac lesions. No cardiac lesion was identified on surface echocardiogram in our patient. The key to diagnosis lies in identifying multiple lentigines or cutaneous myxoma on echocardiogram. Carney et al.8 first described patients with the association of myxoma, spotty pigmentation of the skin and mucous membranes, and endocrine hyperactivity. They also noted an association among pigmented lesions, cutaneous myxoma, and underlying cardiac myxomas. Each patient had ≥2 of the following lesions: (1) cardiac myxoma; (2) cutaneous myxoma; (3) mammary myxoid fibroadenoma; (4) spotty mucocutaneous pigmentation; (5) primary pigmented nodular adrenocortical disease; and (5) testicular tumor. However, our patient did not exhibit any evidence of spotty pigmentation, cardiac myxoma, or endocrine abnormality.
To the best of our knowledge, this is the first report on multiple cutaneous myxoma of the subungual space.
Footnotes
Published online 5 February 2019.
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Rettig AC, Strickland JW. Glomus tumor of the digits. J Hand Surg Am. 1977;2:261–265. [DOI] [PubMed] [Google Scholar]
- 2.Fletcher JW, Watson HK, Weinzweig J. Recurrent myxoma of the hand. J Hand Surg Am. 2000;25:772–775. [DOI] [PubMed] [Google Scholar]
- 3.Carney JA, Headington JT, Su WP. Cutaneous myxomas. A major component of the complex of myxomas, spotty pigmentation, and endocrine overactivity. Arch Dermatol. 1986;122:790–798. [DOI] [PubMed] [Google Scholar]
- 4.Alaiti S, Nelson FP, Ryoo JW. Solitary cutaneous myxoma. J Am Acad Dermatol. 2000;43:377–379. [DOI] [PubMed] [Google Scholar]
- 5.Winke BM, Blair WF, Benda JA. Myxomas in the fingertips. Clin Orthop Relat Res. 1988;237:271–274. [PubMed] [Google Scholar]
- 6.Sponsel KH, McDonald JR, Ghormley RK. Myxoma and myxosarcoma of the soft tissues of the extremities. J Bone Joint Surg Am. 1952;34 A:820–826. [PubMed] [Google Scholar]
- 7.Stratakis CA, Carney JA, Lin JP, et al. Carney complex, a familial multiple neoplasia and lentiginosis syndrome. Analysis of 11 kindreds and linkage to the short arm of chromosome 2. J Clin Invest. 1996;97:699–705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carney JA, Gordon H, Carpenter PC, et al. The complex of myxomas, spotty pigmentation, and endocrine overactivity. Medicine (Baltimore). 1985;64:270–283. [DOI] [PubMed] [Google Scholar]