

Abstract
Context:
Gliomas are the most common brain tumors. In addition to conventional magnetic resonance imaging (MRI) techniques, a variety of new techniques offers more than the anatomic information. The new MRI techniques include perfusion-weighted imaging (PWI) and diffusion-weighted imaging (DWI).
Aims:
The aim of this study is to assess the sensitivity, specificity, predictive value, and accuracy of diffusion- and perfusion-weighted MRI in the preoperative grading of gliomas.
Setting/Design:
The study was conducted in the Department of Neurosurgery, Pathology, and Radiodiagnosis, Sher-e-Kashmir Institute of Medical Sciences, Kashmir, India, which is the only tertiary care neurosurgical center in the state. It was a prospective study.
Patients and Methods:
Thirty-one consecutive patients with gliomas were included in the study. All the patients were evaluated by a standard conventional contrast-enhanced study on Siemens 1.5 Tesla MRI. In addition to the standard MRI, diffusion- and perfusion-weighted MRI were also performed. The histopathological grading of the tumor was done as per the WHO classification of 2007. The sensitivity, specificity, predictive value, and accuracy of diffusion- and perfusion-weighted MRI in determining tumor grade were calculated. Comparison was done between PWI, DWI findings, and WHO histopathological grading.
Analysis Method:
The statistical analysis was done using the Statistical Package for the Social Sciences, and receiver operating characteristic curves were used to estimate sensitivity, specificity, and accuracy.
Results:
The overall sensitivity of PWI (with regional cerebral blood volume cutoff of 1.7) in the preoperative assessment of high-grade gliomas was 82.6% and specificity was 75%, the positive predictive value (PPV) was 90.48%, and the negative predictive value (NPV) was 60%. The overall accuracy was 80.65%. In case of DWI, the sensitivity was 69.57% and the specificity was 75%, and the PPV and NPVs were 88.8% and 46.15%, respectively. The overall accuracy was 71%.
Conclusion:
Our results clearly show higher accuracy of diffusion- and perfusion-weighted MRI in assessment of glioma grade as compared to conventional MRI. This information can prove very useful for the operating neurosurgeon in preoperative assessment and surgical planning. Postoperatively, the neuropathologist can also benefit from such information.
Keywords: Diffusion-weighted imaging, gliomas, perfusion-weighted imaging
Introduction
Gliomas are the most common brain tumors accounting for 40%–50% of brain tumors. They continue to remain a big challenge for the neurosurgeon in terms of surgical decision-making and planning. Magnetic resonance imaging (MRI) in particular has emerged as the imaging modality most frequently used to evaluate gliomas, and it continues to have an ever-expanding multifaceted role in the diagnosis, characterization, and management of gliomas. The conventional MRI with contrast study continues to be the workhorse in both pre- and post-operative imaging of gliomas.
In addition to conventional MRI techniques, a variety of new techniques have found their place in clinical practice. These new techniques offer more than the anatomic information provided by the conventional MRI sequences. Two of the new MRI techniques include perfusion-weighted imaging (PWI) and diffusion-weighted imaging (DWI). Currently, DWI is used primarily in the diagnosis of intracranial abscesses, infarcts, and epidermoid cysts. PWI is mainly utilized in tumors to find the extent of neovascularization and in infarcts to assess the ischemic zones.[1] There are very few studies which attempt to correlate the histopathological grade of the tumor with the findings of diffusion- and perfusion-weighted MRI. The aim of the current study is to assess the same and find if diffusion- and perfusion-weighted MRI can be used for better assessment of glioma grade.
Patients and Methods
This study was conducted in the Departments of Neurosurgery, Radiodiagnosis, and Pathology, Sher-i-Kashmir Institute of Medical Sciences, Kashmir. It was a prospective study conducted from August 2010 to December 2012. A total of 31 consecutive patients a provisional diagnosis of glioma were included in the study. A written and informed consent was obtained from each patient. All the patients were evaluated by a standard conventional contrast-enhanced study on Siemens 1.5 Tesla MRI. In addition to the standard MRI, diffusion- and perfusion-weighted MRI was also performed. On DWI, the following intensity parameters were used and tumors scored from 1 to 5.[2]
Markedly hypointense (1): Intensity nearly equal to cerebrospinal fluid (CSF)
Hypointense (2): Intensity between CSF and subcortical white matter
Isointense (3): Intensity equal to subcortical white matter
Hyperintense (4): Intensity between cortex and subcortical white matter
Markedly hyperintense (5): Intensity higher than cortex.
The perfusion study was performed using dynamic T1-weighted contrast imaging technique. A single dose of gadolinium (0.1 mmol/kg) was administered at 2 ml/s, and repetitive acquisitions were made through the tumor at longer intervals, typically every 15–26 s. Cerebral blood volume (CBV) was defined as the total volume of blood traversing a given region of the brain, measured in milliliters of blood per 100 g of brain tissue (ml/100 g). Cerebral blood flow was defined as the volume of blood traversing a given region of the brain per unit time, measured in milliliters of blood per 100 g of brain tissue per minute (ml/100 g/min). The tumors were analyzed by perfusion-weighted MRI, and the regional CBV (rCBV) was calculated. The tumors were divided into two groups depending on whether the rCBV was high or low. A cutoff value of 1.7 was used in grading high-grade tumors. The statistical analysis was done using the SPSS version 17 (SPSS Inc., Chicago, USA) and receiver operating characteristic (ROC) curves were used to estimate sensitivity, specificity, and accuracy.
After the MRI and additional work-up, 25 patients were operated for tumor decompression and biopsy, and in 6 patients, stereotactic biopsy was done to achieve histopathological diagnosis. The histopathological grading of the tumor was done as per the WHO classification of 2007.[3] All gliomas of the WHO Grade 1 and 2 were grouped together as low-grade gliomas and gliomas of the WHO Grade 3 and 4 were grouped together as high-grade gliomas. The histopathological examination was done by a single pathologist who was blinded to the MRI findings of the tumors. The sensitivity, specificity, predictive value, and accuracy of diffusion- and perfusion-weighted MRI in determining glioma grade were calculated. Comparison was done between the estimated values on DWI and PWI with that of the WHO histopathological grade of the glioma.
Results
There were 22 male and 9 female. The mean age was 41.7 years (range 22–63 years). There were 23 high-grade gliomas and 8 low-grade gliomas [Table 1]. Twelve of the glioblastomas, 2 anaplastic astrocytomas, and 2 anaplastic oligodendrogliomas were markedly hyperintense on DWI. Four glioblastomas, 2 anaplastic astrocytomas, and 1 anaplastic oligodendroglioma were hyperintense on DWI. None of the high-grade tumors was isointense, hypointense, or markedly hypointense on DWI. One low-grade astrocytoma and 1 oligodendroglioma were markedly hyperintense on DWI. One low-grade astrocytoma, 1 oligodendroglioma and oligoastrocytoma were hyperintense on DWI. One low-grade astrocytoma and pilocytic astrocytoma were isointense on DWI. The dysembryoplastic neuroepithelial tumors were hypointense on DWI. None of the low-grade gliomas were markedly hypointense on DWI [Table 2].
Table 1.
rCBV values obtained in different tumors on Perfusion weighted imaging
| Tumor | Total no. of patients | No. of patients with high rCBV | No. of patients with Low rCBV |
|---|---|---|---|
| Glioblastoma | 16 | 14 | 2 |
| Anaplastic Astrocytoma | 4 | 3 | 1 |
| Anaplastic oligodendroglioma | 3 | 2 | 1 |
| Low Grade Astrocytoma | 3 | 0 | 3 |
| Oligodendroglioma | 2 | 1 | 1 |
| Oligoastrocytoma | 1 | 0 | 1 |
| Pilocytic Astrocytoma | 1 | 1 | 0 |
| DNET | 1 | 0 | 1 |
Table 2.
Values on Diffusion weighted imaging for various tumors
| Tumor | No. of patients | Markedly hyperintense (5) | Hyperintense (4) | Isointense (3) | Hypointense (2) | Markedly hypointense (1) |
|---|---|---|---|---|---|---|
| Glioblastoma | 16 | 12 | 4 | 0 | 0 | 0 |
| Anaplastic astrocytoma | 4 | 2 | 2 | 0 | 0 | 0 |
| Anaplastic oligodendroglioma | 3 | 2 | 1 | 0 | 0 | 0 |
| Low Grade Astrocytoma | 3 | 1 | 1 | 1 | 0 | 0 |
| Oligodendroglioma | 2 | 1 | 1 | 0 | 0 | 0 |
| Oligoastrocytoma | 1 | 0 | 1 | 0 | 0 | 0 |
| Pilocytic Astrocytoma | 1 | 0 | 0 | 1 | 0 | 0 |
| DNET | 1 | 0 | 0 | 0 | 1 | 0 |
Keeping a cutoff score of 5 for high-grade gliomas and using ROC curves [Figure 1] the overall sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for predicting high-grade tumors using DWI were calculated. The sensitivity was 69.57%, the specificity was 75%, and the PPV and NPVs were 88.8% and 46.15%, respectively. The overall accuracy was 71%.
Figure 1.
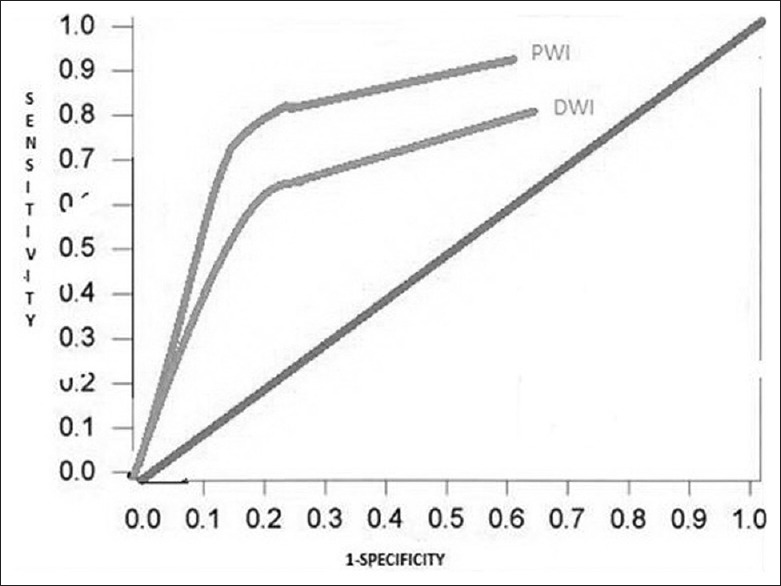
Receiver operating characteristic curves show that perfusion-weighted imaging sequence is more sensitive than that of diffusion weighted as the area under curve is more for perfusion-weighted imaging
The gliomas were analyzed by perfusion-weighted MRI. Among the high-grade gliomas, 14 glioblastomas, 3 anaplastic astrocytomas, and 2 anaplastic oligodendrogliomas showed high rCBV (>1.7). Among the low-grade gliomas, high rCBV values were seen in 1 oligodendroglioma and in the only case of pilocytic astrocytoma. Rest of the low-grade gliomas showed low rCBV values [Table 1].
Based on the above results, the sensitivity, specificity, PPV, and the NPV of perfusion-weighted MRI in grading gliomas into high and low grade were calculated by ROC curves [Figure 1]. The overall sensitivity of PWI was 82.6%, specificity was 75%, the PPV was 90.48%, and the NPV was 60%. The overall accuracy was 80.65%.
Discussion
The predominance of glial tumors has been well documented in most series on brain tumors. In the series by Weber et al.,[4] glioblastomas constituted 44.7% of all patients. Anaplastic astrocytomas accounted for 13.92% and low-grade astrocytomas for 11.39% patients, respectively. These results are similar to those in our series. Glial tumors of astrocytic lineage were most common in the series by Chishty et al.[5] Glioblastomas constituted 30% of the cases in the study by Stadnik et al.,[6] making it the most common tumor in their series as well.
The overall sensitivity of PWI, with a rCBV threshold of 1.7, in our study, was 82.6%, specificity was 75%, the PPV was 90.48%, and the NPV was 60%. The overall accuracy was 80.65%. Comparing our study with the results of several previous studies suggests that rCBV measurements predict the glioma histopathological grade better. Law et al.,[7] in their study, found that the sensitivity, specificity, PPV, and NPV for determination of a high-grade glioma with conventional MRI were 72.5%, 65.0%, 86.1%, and 44.1%, respectively.
In our study, the addition of perfusion-weighted MRI to the imaging protocol improved both the sensitivity (from 72.5% to 82.6%) and the specificity (from 65% to 75%). In the study by Law et al.,[7] a threshold value of 1.75 for rCBV in PWI provided sensitivity, specificity, PPV, and NPV of 95.0%, 57.5%, 87.0%, and 79.3%, respectively, which is comparable to our study. On the other hand, a threshold value of 2.97 in the same study[7] for rCBV provided sensitivity, specificity, PPV, and NPV of 72.5%, 87.5%, 94.6%, and 51.5%, respectively. In this case, the specificity has increased (87.5% as compared to our 75%) as higher threshold values of rCBV have been used as cutoff. Using a higher cutoff value (2.97) decreases the sensitivity of the study as compared to our study (72.5% as compared to our 82.6%). A threshold value of 2.97 provided the same sensitivity as that of conventional MRI but higher specificity and PPV.[7] A threshold value of 2.18 provided the same specificity as that of conventional MRI but higher sensitivity, PPV, and NPV.[7] Lev et al.[8] used an rCBV threshold value of 1.5 in discriminating among 32 consecutive patients with glioma. All the 13 astrocytomas were correctly categorized as high-grade gliomas. Three of these did not enhance after administration of contrast material. Of the nine low-grade astrocytomas, seven were correctly classified. The sensitivity and specificity with the use of an rCBV of 1.5 as a threshold value were 100% and 69%, respectively. It compares well with our study, but our specificity was higher because of using a slightly higher rCBV cutoff (1.7 as compared to 1.5). Bulakbasi et al.[9] used rCBV value of 3.9 to classify tumors and attained a high sensitivity (95.46%), specificity (91.67%), and accuracy (93.10%), than conventional MRI parameters. Our results are comparable with the findings in terms of sensitivity (95.46% compared to ours of 82.6%). Their findings are also comparable to those of Law et al.[7] in which they found a cutoff value of 1.75 for rCBV yielding a sensitivity and specificity of 95% and 57.5% and those of Lev et al.[8] in which they found 100% sensitivity and 69% specificity using a cutoff value of 1.5 for rCBV. Although the sensitivity was similar, the specificity in this study by Bulakbasi et al.[9] was higher than that in ours and other aforementioned studies. This is because they picked up a higher rCBV cutoff value of 3.9 than others, to eliminate false positives. Shin et al.[10] used a cutoff value of 2.9 for rCBV to detect high-grade tumors and achieved 91% sensitivity and 83% specificity. Again, the specificity is higher than with our study and with studies of Law et al.[7] and Lev et al.[8] However, the sensitivity is comparable with other studies. In studies by Liu et al.,[11] the sensitivity and specificity, based on an rCBV cutoff of 1.75, were 60% and 58.6%, respectively. The study has used similar rCBV cutoff values as our study and that of Law et al.[7] However, the sensitivity values in our study are higher than in this study (82.6% as compared to 60%). Similarly, the specificity values in our study are higher (75% as compared to 58.6%). Using similar rCBV cutoff, Law et al.[7] also obtained higher sensitivity (95%) values. However, the specificities are similar.
Keeping a cutoff of score 5 for high-grade tumors, the overall sensitivity, specificity, PPV, and NPVs for predicting high-grade tumors using DWI were calculated. In our study, the sensitivity was 69.57%, the specificity was 75%, and the PPV and NPVs were 88.8% and 46.15%, respectively. The overall accuracy was 70%. In the study by Seo et al.,[2] similar five-point scale for grading tumors by diffusion-weighted MRI was used. The mean score of all high-grade gliomas was significantly higher than that of low-grade gliomas. The sensitivity and specificity of diffusion-weighted MRI in preoperative-grade assessment of brain tumors were 70% and 76.9%, respectively. This is similar to the sensitivity and specificity obtained in our study (69.57% and 75%, respectively). The PPV and NPV in their study were 94.4% and 40%, respectively. In our study, the PPV was 88.8% and the NPV was 46.15%. These values compare favorably with our study. In the study by Stadnik et al.,[6] all the cases of lymphomas showed marked hyperintensity on DWI. In our study, 4(80%) of the lymphomas were markedly hyperintense with a score of 5 on the assessment scale. This may be useful in differentiating from metastasis which did not show such marked hyperintensity on DWI.
Fan et al.[12] found that on DWI, the signal intensity in the solid portion of the tumor was hyperintense with respect to the white matter. In our study, the mean signal intensity on DWI was 4.7 + 0.5 for high-grade tumors and 3.7 + 1.0 for low-grade tumors. Castillo et al.[13] found that DWI was helpful in distinguishing between tumor, edema, and nontumorous tissue. Tien et al.[14] showed that diffusion-weighted echo planar MRI can be used to distinguish nonenhancing tumor from peritumoral edema when these abnormalities are located in white matter in the direction of diffusion-weighted gradient and differentiate various components of tumor.
Conclusion
Our results clearly show the improved accuracy of diffusion- and perfusion-weighted MRI in assessment of tumor grade as compared to conventional MRI. Hence, we recommend the integration of these imaging techniques in the routine protocol of MRI imaging of brain tumors for better assessment of tumor grade.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Young GS. Advanced MRI of adult brain tumors. Neurol Clin. 2007;25:947–73. doi: 10.1016/j.ncl.2007.07.010. viii. [DOI] [PubMed] [Google Scholar]
- 2.Seo HS, Chang KH, Na DG, Kwon BJ, Lee DH. High b-value diffusion (b = 3000 s/mm2) MR imaging in cerebral gliomas at 3T: Visual and quantitative comparisons with b = 1000 s/mm2. AJNR Am J Neuroradiol. 2008;29:458–63. doi: 10.3174/ajnr.A0842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol. 2007;114:97–109. doi: 10.1007/s00401-007-0243-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Weber MA, Zoubaa S, Schlieter M, Jüttler E, Huttner HB, Geletneky K, et al. Diagnostic performance of spectroscopic and perfusion MRI for distinction of brain tumors. Neurology. 2006;66:1899–906. doi: 10.1212/01.wnl.0000219767.49705.9c. [DOI] [PubMed] [Google Scholar]
- 5.Chishty IA, Rafique MZ, Hussain M, Akhtar W, Ahmad MN, Sajjad Z, et al. MRI characterization and histopathological correlation of primary intra-axial brain glioma. J Liaquat Univ Med Health Sci. 2010;9:64–9. [Google Scholar]
- 6.Stadnik TW, Chaskis C, Michotte A, Shabana WM, van Rompaey K, Luypaert R, et al. Diffusion-weighted MR imaging of intracerebral masses: Comparison with conventional MR imaging and histologic findings. AJNR Am J Neuroradiol. 2001;22:969–76. [PMC free article] [PubMed] [Google Scholar]
- 7.Law M, Yang S, Wang H, Babb JS, Johnson G, Cha S, et al. Glioma grading: Sensitivity, specificity, and predictive values of perfusion MR imaging and proton MR spectroscopic imaging compared with conventional MR imaging. AJNR Am J Neuroradiol. 2003;24:1989–98. [PMC free article] [PubMed] [Google Scholar]
- 8.Lev MH, Ozsunar Y, Henson JW, Rasheed AA, Barest GD, Harsh GR, 4th, et al. Glial tumor grading and outcome prediction using dynamic spin-echo MR susceptibility mapping compared with conventional contrast-enhanced MR: Confounding effect of elevated rCBV of oligodendrogliomas. AJNR Am J Neuroradiol. 2004;25:214–21. [PMC free article] [PubMed] [Google Scholar]
- 9.Bulakbasi N, Kocaoglu M, Farzaliyev A, Tayfun C, Ucoz T, Somuncu I. Assessment of diagnostic accuracy of perfusion MR imaging in primary and metastatic solitary malignant brain tumors. AJNR Am J Neuroradiol. 2005;26:2187–99. [PMC free article] [PubMed] [Google Scholar]
- 10.Shin JH, Lee HK, Kwun BD, Kim JS, Kang W, Choi CG, et al. Using relative cerebral blood flow and volume to evaluate the histopathologic grade of cerebral gliomas: Preliminary results. AJR Am J Roentgenol. 2002;179:783–9. doi: 10.2214/ajr.179.3.1790783. [DOI] [PubMed] [Google Scholar]
- 11.Liu X, Tian W, Kolar B, Yeaney GA, Qiu X, Johnson MD, et al. MR diffusion tensor and perfusion-weighted imaging in preoperative grading of supratentorial nonenhancing gliomas. Neuro Oncol. 2011;13:447–55. doi: 10.1093/neuonc/noq197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fan GG, Deng QL, Wu ZH, Guo QY. Usefulness of diffusion/perfusion-weighted MRI in patients with non-enhancing supratentorial brain gliomas: A valuable tool to predict tumour grading? Br J Radiol. 2006;79:652–8. doi: 10.1259/bjr/25349497. [DOI] [PubMed] [Google Scholar]
- 13.Castillo M, Smith JK, Kwock L, Wilber K. Apparent diffusion coefficients in the evaluation of high-grade cerebral gliomas. AJNR Am J Neuroradiol. 2001;22:60–4. [PMC free article] [PubMed] [Google Scholar]
- 14.Tien RD, Felsberg GJ, Friedman H, Brown M, MacFall J. MR imaging of high-grade cerebral gliomas: Value of diffusion-weighted echoplanar pulse sequences. AJR Am J Roentgenol. 1994;162:671–7. doi: 10.2214/ajr.162.3.8109520. [DOI] [PubMed] [Google Scholar]