

Abstract
Indium-tin oxide production has increased greatly in the last 20 years subsequent to increased global demand for touch screens and photovoltaics. Previous studies used measurements of indium in blood as an indicator of indium exposure and observed associations with adverse respiratory outcomes. However, correlations between measurements of blood indium and airborne respirable indium are inconsistent, in part because of the long half-life of indium in blood, but also because respirable indium measurements do not incorporate inhalable indium that can contribute to the observed biological burden. Information is lacking on relationships between respirable and inhalable indium exposure, which have implications for biological indicators like blood indium. The dual IOM sampler includes the foam disc insert and can simultaneously collect respirable and inhalable aerosol. Here, the field performance of the dual IOM sampler was evaluated by comparing performance with the respirable cyclone and traditional IOM for respirable and inhalable indium and dust exposure, respectively. Side-by-side area air samples were collected throughout an indium-tin oxide manufacturing facility. Cascade impactors were used to determine particle size distribution. Several statistical methods were used to evaluate the agreement between the pairs of samplers including calculating the concordance correlation coefficient and its accuracy and precision components. One-way ANOVA was used to evaluate the effect of dust concentration on sampler differences. Respirable indium measurements showed better agreement (concordance correlation coefficient: 0.932) compared to respirable dust measurements (concordance correlation coefficient: 0.777) with significant differences observed in respirable dust measurements. The dual IOM measurements had high agreement with the traditional IOM for inhalable indium (concordance correlation coefficient: 0.997) but lower agreement for inhalable dust (concordance correlation coefficient: 0.886 and accuracy: 0.896) with a significantly large mean bias (−146.9 mg/m3). Dust concentration significantly affected sampler measurements of inhalable dust and inhalable indium. Results from this study suggest that the dual IOM is a useful single sampler for simultaneous measurements of occupational exposure to respirable and inhalable indium.
Keywords: Indium-tin oxide, Inhalable, IOM, respirable
Introduction
Indium–tin oxide (ITO) is manufactured by blending, compacting, and sintering indium oxide and tin oxide powders. Because ITO has exceptional optical and electrical properties, it is used as a transparent thin film conductor in consumer electronics such as liquid crystal display (LCD) and touch screens, as well as in coatings for solar cells and architectural glass.[1] Workers exposed to indium compounds including ITO can develop indium lung disease, which is characterized by pulmonary alveolar proteinosis that may progress to fibrosis with or without emphysema.[2] Previous epidemiologic studies have used measurements of indium in blood, i.e., in plasma, serum, or whole blood, as a biological indicator of indium exposure and have observed associations with adverse respiratory health outcomes.[3,4] A recent study observed that plasma indium concentration is correlated with cumulative respirable indium exposures and higher cumulative respirable indium exposures were associated with shortness of breath, lower spirometric parameters, and higher blood levels of biomarkers of lung disease.[5] Further, another recent study reported significant associations between current indium exposure and increased DNA damage and chromosome aberrations in the lymphocytes of exposed workers.[6] However, the correlations between measurements of indium in blood matrices and current respirable indium exposure are inconsistent.[7] Differences between these measurements may be due to differences in chemical forms of indium as well as not accounting for larger, inhalable indium particles that deposit in the upper and conducting airways and contribute to blood indium levels. Additionally, indium in blood reflects current ongoing exposures as well as past exposures that may have occurred in different working conditions. Hoet et al. observed that with a half-life of 65 days in blood, indium may accumulate in the body and contribute to blood indium levels observed in exposed workers after exposure ceases.[7] Previous work by Leach et al. observed a biological half-life for indium oxide, a common form of indium found in ITO manufacturing, of 2.5 months in the lungs and 1.75 months in the tracheobronchial lymph nodes.[8] Because indium lung disease manifests in the alveolar region of the lung,[2,9] sampling for respirable indium is a logical choice for this health endpoint. However, evaluating occupational exposure to both respirable and inhalable indium would help characterize (i) the effects of both size fractions on measurements of indium in blood and (ii) sources of exposure to both respirable and inhalable particle size fractions.
Sampling for multiple aerosol size fractions often requires more than one sampling device and can present an increased burden on workers asked to wear multiple samplers during an exposure assessment survey. A single sampler that can provide both respirable and inhalable exposure measurements is desirable because it minimizes the burden on workers and can thereby enhance study participation.[10] The IOM sampler is often used for sampling inhalable aerosol,[11–13] and multiple studies have used it to measure exposure to inhalable dust in widely varied occupational settings including woodworking, metal refineries, metal foundries, paper mills, textile mills, food processing, and agricultural industries.[14–18] The dual IOM sampler (IOMd) includes the MultiDust Foam Disc (a polyurethane foam) insert and can simultaneously collect respirable and inhalable aerosol with a single sampling device. Previous studies have evaluated the laboratory and field performance of the IOMd in measuring respirable and/or inhalable dust.[10,14,19–21] However, to the authors’ knowledge, only one study to date has evaluated the field performance of the IOMd sampler in measuring both respirable and inhalable exposure to metal dusts in a metal manufacturing facility by comparing its performance to other acceptable samplers.[14]
This study evaluates the field performance of the IOMd sampler by comparing it to the (i) respirable cyclone and (ii) traditional IOM sampler when sampling for respirable and inhalable indium and dust exposure, respectively. Field performance of samplers was assessed by collecting side-by-side area air samples from multiple locations and processes throughout an ITO manufacturing facility. Several statistical methods were used to evaluate the agreement between the pairs of samplers and sources of disagreement to characterize performance of the different samplers. In addition, the effect of humidity, dust size, and inhalable dust concentration were also evaluated to understand the impact of these factors on sampler performance.
Methods
An exposure and health assessment was performed at an ITO manufacturing facility to characterize exposure to indium and indium compounds and their associations with measures of indium lung disease. A comprehensive exposure assessment survey was performed during a visit to the facility in the summer of 2014. A sampler comparison study was conducted as part of the exposure assessment, to evaluate the field performance of the IOMd in measuring the respirable and inhalable indium and dust exposure by comparisons with respirable cyclone and the traditional IOM sampler.
The ITO manufacturing facility processes indium oxide and tin oxide into ITO ceramic tiles used by customers for sputtering applications. The major steps in the production of ITO ceramic tiles and reclamation of indium starts in the refinery, where indium oxide is produced from solid indium metal[22] and have been described previously.[23,24] In the ITO area, indium oxide and tin oxide are mixed together. The resulting mixture is formed into planar or cylindrical tiles in the casting areas or spray dried followed by cold isostatic pressing. These tiles undergo limited cutting and sanding, and are then fired to sinter the ITO. After firing, the sintered tiles are ground and cut to customers’ specifications in the grinding areas. Once cut, a backing material is applied to the tiles in the bonding area, after which the tiles are packaged and shipped. In the reclaim area, spent tiles and waste materials from all production areas are converted to indium metal. Molten metal is then cast into ingots and finally into shot to be used in the refinery. Other production-related processes include quality control (QC) and research and development (R&D).
Air sampling for physical and chemical characterization of aerosols
Cascade impactors were used to collect air samples to characterize the aerosol size distribution during the exposure assessment survey. Eight-stage Marple Cascade Impactors (Marple series 290, MSP Corporation, Shoreview, MN) were used to collect 26 area air samples from production and production support locations and included the planar bond shop, rotary bond shop, planar grinding, ITO, forming, reclaim, refinery, rotary grinding, forming, QA and QC lab, and shipping and receiving areas. Area air samples were collected for 4.5–5.4 hr duration. Marple Cascade Impactors were operated at a flow rate of 2 Lpm and equipped with pre-greased 34 mm PVC filters. Samples were analyzed gravimetrically and for mass of indium. Chemical composition of the aerosol was assessed with three-piece 37-mm open-faced cassette samplers (SKC, Inc., Eighty Four, PA) loaded with polytetrafluoroethylene (PTFE) filters. The open-faced cassette samplers were used to ensure an even distribution of the aerosol across the filter face. Open-faced cassette samples were collected from production and production support locations and were co-located with cascade impactors. Open faced cassette samples were collected for 6.1–38.8 hr and operated at a flow rate of 2 Lpm and analyzed for elemental composition. A minimum of one field blank and one media blank was used for every 10 samples of each cascade impactor or open-face cassette.
Air sampling for sampler comparison
Side-by-side sets of area air samples were collected during the 2014 exposure survey using the respirable cyclone GK2.69 (BGI Inc., Waltham, MA) and the IOMd (IOM with polyurethane foam insert) and traditional IOM (SKC Inc., Eighty Four, PA). Sets of IOMd, traditional IOMs, and respirable cyclones were placed in baskets located in 18 fixed locations in the production areas, which included the planar and rotary bond shops, ITO areas, planar and rotary grinding areas, reclaim, refinery, and research and development (R&D). Full-shift and composite samples were collected for 6.1–16.4 hr duration. The cyclones were operated at a flow rate of 4.2 liters per minute (Lpm) and equipped with a two-piece, 37-mm cassette with a 5-mm pore size polyvinyl chloride (PVC) filter. The IOM samplers were operated at 2 Lpm and used 5-mm pore size PVC filters. The IOMd and traditional IOM samplers were made of conductive plastic. A minimum of one field blank and one media blank were used for every ten samples of each sample type. All samples were analyzed gravimetrically and quantified for the mass of indium (described below). Relative humidity and temperature (Ambient Weather, Chandler, AZ) were recorded at multiple intervals during the day.
Analytical methods
Samples were analyzed by a contract laboratory for respirable and inhalable dusts in accordance with NIOSH Methods 0500 or 0600 and subsequently digested and analyzed for indium by inductively coupled plasma (ICP) atomic emission spectrometry analyses using NIOSH Method 7303.[25] For gravimetric analyses, the IOM cassette assemblies were allowed to equilibrate for a minimum of 2 hr before weighing. Each IOM assembly was passed over a static neutralizer before weighing on a Mettler balance, model number MT5. Inhalable particulate was measured by weighing the entire IOM assembly with the cassette, polyurethane foam insert, and PVC filter. Respirable particulate was measured by weighing the bottom plastic support and PVC filter. The limits of detection (LODs) for IOM cassette assemblies were 50 micrograms (mg) per respirable assembly and 100 mg per inhalable assembly. For cascade impactor samples analyzed using NIOSH Method 0500, the LODs were 20 mg per sample for slotted filters and 40 mg per sample for whole filters. For respirable cyclone samples analyzed gravimetrically using NIOSH Method 0600, the LOD was 50 mg per sample.
Each IOM cassette was wiped with a PVC filter wetted with deionized water. The PVC filter was placed with the corresponding sample and digested and analyzed according to NIOSH Method 7303. For IOMd samples, the polyurethane foam insert was separately digested and analyzed according to NIOSH Method 7303. Laboratory control spike pairs (LCS) and blind spikes were prepared on the PVC and foam media. All PVC samples were recovery corrected with the average of 103.2%, 102.2%, and 111.7% of the LCS pairs for the cascade impactor, respirable cyclone, and IOM samples, respectively. For the IOMd samples, all samples were recovery corrected with the average of the LCS pairs of 106% for the foam insert and 103.6% for the PVC filter. Indium was recovered within the statistical limits on all blind spikes. The LODs for samples analyzed for indium content were 0.375 mg per respirable cyclone sample, 0.4 mg per IOM filter sample, 0.3 mg per IOMd foam sample, and 0.4 mg per cascade impactor filter sample. Open-faced cassette samples were analyzed for 48 elements using proton induced x-ray emission (PIXE) analysis (Elemental Analysis, Inc., Lexington, KY) with detection limits that ranged from 0.02–0.15 mg per cm2.
Impactor data analysis
Results for indium and dust mass collected on the cascade impactors were corrected according to the manufacturer’s reported collection efficiency for each stage (Thermo Fisher Scientific, Franklin, MA). Particle mass median aerodynamic diameter (MMAD) and geometric standard deviation (GSD) for unimodal or bimodal size distributions of indium and dust were calculated using the method previously described by Hewett and McCawley.[26] The method fits a smooth curve to particle size data and generates estimates of the parameters for each mode to include the geometric mean size, GSD, and the percentage that each underlying mode contributes to the overall distribution. The estimates of the underlying distribution can be modified until a satisfactory fit is obtained.[26] A satisfactory fit was defined as a value for the squared difference of less than 10 for the percent of total area under the curve and the percent total mass per stage, as previously described by Hewett and McCawley.[26]
Statistical analysis
All statistical analyses were performed using PC-SAS version 9.2 and JMP version 11.0 (SAS Institute, Cary, NC) and all plots were prepared in SigmaPlot (Version 9.01, Systat Software Inc., San Jose, CA). Measurements below the LOD were also randomly simulated from 0 to the corresponding LODs using the beta substitution method, that is shown to generate estimates of the GM and GSD that closely match those from the maximum likelihood method (MLE), the standard for handling LOD data.[27] The distributions of all the measurements were evaluated graphically using probability plots and summary statistics were calculated. Dust concentration was dichotomized as: low (≤50th percentile) or high (>50th percentile) for dust concentrations measured by the IOM.
Mean difference (bias), mean percent difference, standard deviation of the difference, ratio and paired t-test between the sampler types for respirable and inhalable indium, and dust were calculated to assess agreement. Agreement was also assessed by calculating the concordance correlation coefficient (CCC), which is based on the mean of the squared difference between two measurement methods, transformed into a correlation coefficient.[28–30] The CCC has two components: (1) accuracy defined as the deviation of the fitted line from the concordance line, where the concordance line is the line of theoretical perfect agreement; and (2) precision—the deviation of each pair of observations from the fitted line. The CCC, its precision, and accuracy components were calculated in SAS using a macro provided by Lin et al.[28] Singlefactor ANOVA models were fit with percent difference as the outcome variable and dust concentration as the predictor variable to evaluate the dust concentration effect on percent difference between paired sampler types. Because of the disproportionately greater fraction of dust measurements below the LOD for the IOMd sampler compared to the IOM or cyclone, statistical analyses of sampler comparisons were performed twice, once excluding the LOD measurements and once using all the data (reported in the online supplementary).
Simple ordinary least square (OLS) regression models were developed using the natural logarithm of cyclone or the traditional IOM concentrations as the dependent variables with the natural logarithm of the IOMd concentrations as the predictor variable. However, because both the dependent and the predictor variables have measurement error, OLS regression can provide biased estimates for the intercept (which may be biased high) and the slope (which may be biased low). Hence, the same models were also run using an error-in-variables model (Orthogonal regression) in JMP with the assumption that the error variance was equal for the pairs of samplers.
Results
Indium and dust aerosol size distribution and chemical composition
Indium and dust aerosol size distributions varied by department and location (Table 1). Of the 26 Marple Cascade Impactor samples, seven samples for indium and 10 dust samples were not included in size distribution calculations because more than five of the 8 stages had filters with measurements below the LOD.
Table 1.
Physical and chemical characteristics of workplace aerosol in ITO production and reclamation jobs.
| Department | Location | Indium MMADA (μm) |
Indium GSD | Dust MMADA (μm) |
Dust GSD | Chemical compositionA |
|---|---|---|---|---|---|---|
| Refinery | Centrifuge | 2.1 and 20.1A | 1.3 and 4.3A | 0.2 | 1.2 | In |
| Dross processing area | 12 | 2.3 | – | – | * | |
| ITO | Furnace | 11.6 | 2.3 | 5.9 | 5 | In |
| Blending Area | 15.9 | 1.9 | – | – | In, Si | |
| Cutting and Sanding | 2.7 and 8.7A | 1.4 and 4.4A | 2.7 and 17A | 1.4 and 4.4A | In, Fe | |
| Spray Dryer | 18.5 | 1.5 | 24 | 1.5 | In | |
| Casting | 8.4 | 2.8 | – | – | In, S | |
| Planar Bond | Bond Shop | 10.3 | 3.6 | – | – | Al, Ca, In, Fe, Si, S, Cu |
| Planar Grind | Grinding | 7.8 | 2.7 | 7.8 | 2.7 | Cl, In |
| Rotary Bond | Sawing | 8.3 | 3 | – | – | * |
| Bond Shop | 1.2 and 12.7A | 1.8 and 2.2A | – | – | In | |
| Wetting Room | 7.8 | 3.4 | 0.2 | 1.5 | In, Si | |
| Rotary Grind | Grinding | 4.7 | 3.4 | 3.2 | 1.6 | Cl, In |
| Reclaim | Furnace | 11.6 | 2.3 | 17 | 1.8 | Al, Cl, In, Fe, Si, S, Zn |
| Milling | 0.9 | 1.6 | 0.5 | 1.6 | Al, Cl, In, Fe, Si, Sn, Zn | |
| Mixing | 7.3 | 3.1 | 10.5 | 3.1 | Al, Ca, Cl, In, Fe, Si, Sn | |
| Forming | Forming Shop | – | – | 5 | 2.2 | Al, Ca, K, Si, S |
| QA and QC | Inspection | 7.4 | 2.7 | – | – | In |
| Shipping and Receiving | Deck | 11.1 | 2.2 | – | – | * |
MMAD measurements in mm and GSD calculations for bimodal size distributions.
Chemicals are abbreviated by their elemental symbol. ─ indicates samples that were below the limit of detection.
indicates no samples were collected in this area for PIXE analysis.
MMAD measurements for indium aerosol and GSDs ranged from 0.9–20.1 mm and 1.3–4.4, respectively (Table 1). Of the 17 locations with cascade impactor measurements, only the reclaim milling area and the refinery centrifuge area had size distribution data that indicated the indium aerosol was predominantly in the respirable size range (MMAD <4 μm and respirable fraction >0.5). Bimodal size distributions for indium aerosol were observed in the refinery centrifuge area, rotary bond shop, and the ITO cutting and sanding area (Table 1). Of the areas where bimodal size distributions were observed, the indium aerosol in the refinery centrifuge area was predominantly in the respirable size range (MMAD <4 μm and respirable fraction >0.5). All other sampled areas with unimodal or bimodal MMADs had indium aerosol predominantly in the thoracic (MMAD >4 μm and <10 μm) and inhalable size ranges (MMAD >10 μm).
Dust size distributions varied greatly within and between processes in different departments and locations. MMAD measurements for dust and GSDs ranged from 0.2–24 mm and 1.2–5.0, respectively. Dust MMADs in the respirable size range were observed in the reclaim milling area, refinery centrifuge area, ITO cutting and sanding area, rotary grinding, and rotary bond wetting room (Table 1). Bimodal dust size distributions were observed in the planar grinding area and the ITO cutting and sanding area.
Chemical composition of aerosol particles varied by department and location as well (Table 1). For the majority of the 48 elements analyzed, all samples were below the LOD. Elements quantified in some of the samples included aluminum (Al), calcium (Ca), chloride (Cl), copper (Cu), indium (In), iron (Fe), potassium (K), silicon (Si), sulfur (S), tin (Sn), and zinc (Zn). A majority of samples for these elements (76% for Al, 88% for Ca, 80% for Cl, 96% for Cu, 80% for Fe, 96% for K, 68% for Si, 80% for S, 88% for Sn, and 92% for Zn) were also below the LOD and are thus summarized as present or absent for a particular area.
Temperature and relative humidity measurements
Temperature and relative humidity measurements varied by location. Temperature measurements ranged from 18.9 ○C (planar grinding) to 35–35.6 ○C (ITO and reclaim) (Supplementary Table S1). Relative humidity measurements ranged from 20% (ITO) to 80–82% (forming, planar grinding, and R&D) (Supplementary Table S1).
Respirable indium and dust
Seventeen pairs of IOMd and respirable cyclone samples were available for comparison. Six IOMd and three respirable cyclone measurements for respirable dust were below the LOD and were excluded from analyses presented in Figures 1, 2, S3, and S4, and Tables 2–4. Imputed values for measurements below the LOD were included in results presented in corresponding Figures S1 and S2, and Tables S3 and S4. Respirable indium measurements collected using the IOMd and respirable cyclone ranged from 0.9–294.6 mg/m3 and 0.2–295.8 mg/m3, respectively (Table 2). Respirable dust measurements collected using the IOMd and respirable cyclone ranged from <27.0–430.5 mg/m3 and <13.0–378.0 mg/m3, respectively (Table 2, Table S2). The IOMd measured higher levels of respirable indium (mean bias = 4.39 mg/m3, mean difference 60.7%) and respirable dust (mean bias 31.2 mg/m3, mean difference 82.1%) than the respirable cyclone (Table 3). Paired t-test analyses indicated this difference was statistically significant for respirable dust but not for respirable indium. Respirable indium measurements showed better agreement (CCC: 0.932) compared to respirable dust measurements (CCC: 0.777), with a high degree of accuracy (accuracy coefficient 0.987 vs. 0.885) and with lower precision being the cause of disagreement (precision coefficient 0.945 vs. 0.878), respectively, for respirable indium and respirable dust (Table 3). Analyses using imputed values for the three cyclone and six IOMd respirable dust measurements below the LOD increased the sample size and showed better agreement between the sampler types for respirable dust (CCC: 0.850) with an increased accuracy (accuracy coefficient = 0.959) but lower precision (precision coefficient = 0.887) (Table S3).
Figure 1.
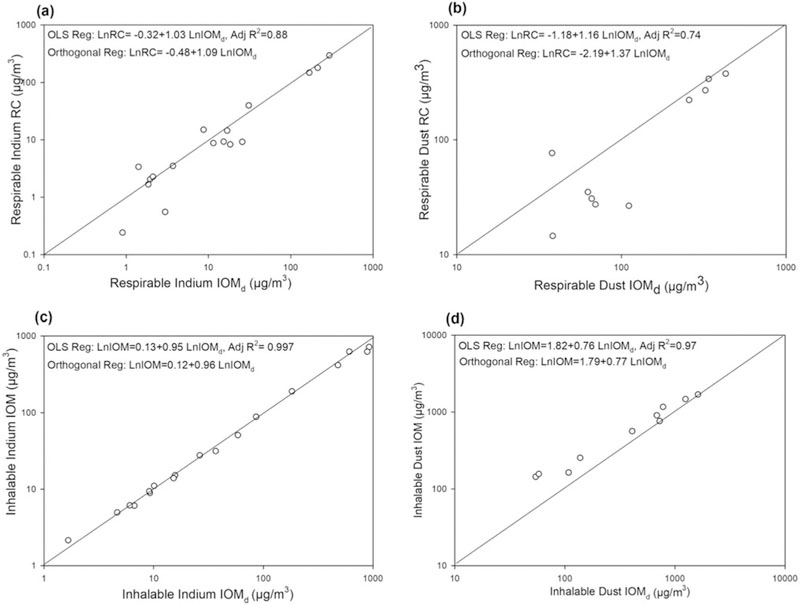
Respirable and inhalable indium and dust measurements. Panels (a) and (b): (a) respirable indium and (b) respirable dust measurements collected using the IOMd compared with respirable cyclone (RC). Panels (c) and (d): (c) inhalable indium (d) and inhalable dust measurements collected using the IOMd compared with the IOM sampler. Dust measurements below the LOD are excluded in panels (b) and (d). All dust measurements including imputed values for measurements below the LOD can be seen in Figure S1.
Figure 2.
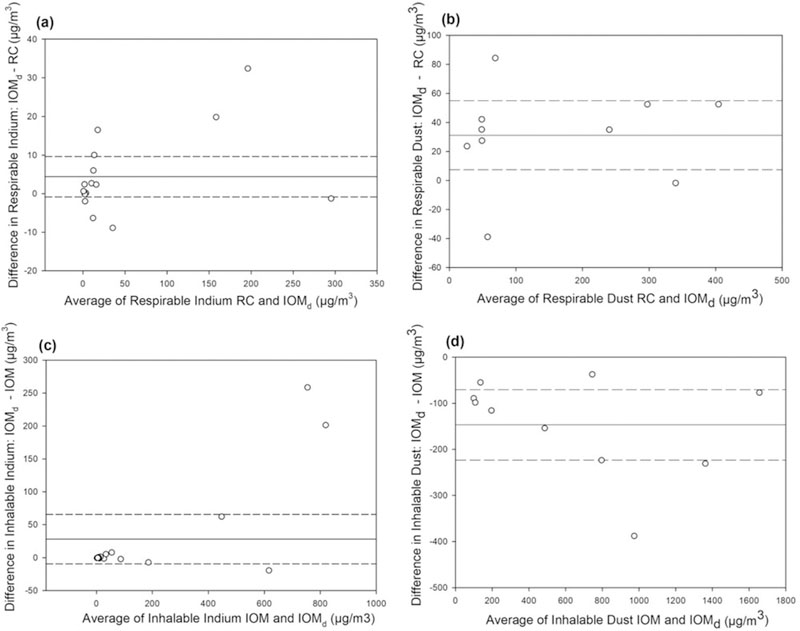
Respirable and inhalable sampler bias across different aerosol concentrations. Panels (a) and (b): (a) respirable indium and (b) respirable dust measurements collected using the IOMd compared with respirable cyclone (RC). Panels (c) and (d): (c) inhalable indium (d) and inhalable dust measurements collected using the IOMd compared with the IOM sampler. Dust measurements below the LOD are excluded in panels (b) and (d). Sampler bias calculated using imputed values for dust measurements below the LOD can be seen in Figure S2.
Table 2.
Respirable indium and dust and inhalable indium and dust measurements by sampler type.
| Respirable indium (μg/m3) |
Respirable dustC (μg/m3) |
Inhalable indium (μg/m3) |
Inhalable dustC (μg/m3) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sampler | N | GMA | Min-MaxB | N | GMA | Min-MaxB | N | GMA | Min-MaxB | N | GMA | Min-MaxB |
| IOMd | 17 | 10.9 | 0.9‒294.6 | 10 | 118.8 | 37.9‒430.5 | 18 | 36.5 | 1.7‒920.1 | 10 | 329.1 | 54.2‒1617.7 |
| Respirable Cyclone | 17 | 8.4 | 0.2‒295.8 | 10 | 76.6 | 14.6‒378.0 | – | – | – | – | – | – |
| IOM | – | – | – | – | – | – | 18 | 35.1 | 2.1‒718.9 | 10 | 503.9 | 143.3‒1694.4 |
Geometric mean of mass concentrations measurements.
Minimum and maximum values for mass concentration measurements.
indicates respirable dust and inhalable dust measurements with samples < LOD excluded from analyses. All dust measurements including samples below the LOD can be seen in Supplementary Table S2.
indicates no samples collected.
Table 4.
One-way analysis of variance of percent differences in measurements of respirable and inhalable indium and dust, by dust concentration.
| Sampler comparison | Mean percent difference (95% CI), by dust concentration (µg/m3) |
|
|---|---|---|
| LowA (≤ 663) | HighA (> 663) | |
| IOMd : Respirable Cyclone Respirable Indium (n=17) | 10.1 (–5.6–25.9) (n=12) | 5.3 (–19.1–29.7) (n=5) |
| IOMd : Respirable Cyclone Respirable Dust (n=10) | 126.4 (3.0–249.7) (n=4) | 34.0 (–48.1–153.4) (n=6) |
| IOMd : IOM Inhalable Indium (n=18) | 0.53B (–7.4–8.5) (n=13) | 15.8B (3.0–28.5) (n=5) |
| IOMd : IOM Inhalable Dust (n=10) | –46.4B(–61.3‒ –31.5) (n=5) | –16.6B( –31.5–1.7) (n=5) |
50th percentile of all IOM dust concentration measurements =663 μg/m3.
Indicates ANOVA results with p < 0.05.
Table 3.
Comparisons between respirable indium and dust and inhalable indium and dust measurements.
| Sampler Comparison | Mean ratio (range) |
Mean difference or bias in mg/m3 (95% CI) |
Mean % difference (range) |
Std. of difference |
CCC | Accuracy coefficient |
Precision coefficient |
|---|---|---|---|---|---|---|---|
| IOMd : Respirable Cyclone Respirable Indium (n = 17) | 1.61 (0.42–5.38) | 4.39 (−0.87–9.63) | 60.7 (−58.4–437.8) | 10.22 | 0.932 | 0.987 | 0.945 |
| IOMd : Respirable Cyclone Respirable DustB (n = 10) | 1.82 (0.49–4.16) | 31.2A (7.41–55.0) | 82.1A (−50.7–315.8) | 33.2 | 0.777 | 0.885 | 0.878 |
| IOMd : IOM Inhalable Indium (n = 18) | 1.05 (0.77–1.41) | 28.1 (−9.58–65.8) | 4.8 (−22.9–41.4) | 75.77 | 0.997 | 0.999 | 0.998 |
| IOMd : IOM Inhalable DustB (n = 10) | 0.69 (0.37–0.95) | 146.9A (−223.5–−70.3) | 31.5A (−62.9–−4.5) | 107.1 | 0.886 | 0.896 | 0.989 |
Mean differences that were significant on paired t-test, with p < 0.05.
indicates respirable dust and inhalable dust measurements with samples < LOD excluded from analyses. Sampler comparisons using imputed values for dust measurements below the LOD can be seen in Supplementary Table S3.
Scatterplots of respirable cyclone by IOMd measurements for respirable indium and respirable dust show the spread of the data around the unity line (Figures 1a and 1b). The unity line indicates perfect agreement between the two sampler’s measurements. The OLS and orthogonal regression were very similar for respirable indium but not respirable dust. Scatterplots of the respirable sampler types with measurements displayed by department did not indicate a pattern of deviation from the unity line by department. However, the small number of measurements by department limit certainty of this observation (Supplementary Figures S3a and S3b). The Bland-Altman difference plots show a positive bias for respirable indium and dust measured with IOMd, and the patterns suggest a possible concentration effect (Figures 2a, 2b, S2a, and S2b). However, results of the one-way ANOVA models did not indicate a significant effect of dust concentration on differences in sampler types for respirable indium or dust (Tables 4 and S4).
Inhalable indium and dust
Eighteen pairs of IOMd and traditional IOM samples were available for comparison, and eight IOMd measurements for inhalable dust were below the LOD were excluded from analyses presented in Figures 1, 2, S3, S4, and Tables 2–4. Imputed values for measurements below the LOD were included in results presented in corresponding Figures S1 and S2, and Tables S3 and S4. Inhalable indium measurements collected using the IOMd and IOM ranged from 1.7–920.1 μg/m3 and 2.1–718.9 μg/m3, respectively (Table 2). Inhalable dust measurements collected using the IOMd and IOM ranged from <50.4–1617.7 μg/m3 and 110.0–1694.4 μg/m3, respectively (Tables 2, S2). The IOMd measured similar levels of inhalable indium (mean bias 28.1 μg/m3, mean difference 4.8%) but lower levels of inhalable dust (mean bias −146.9 μg/m3, mean difference −31.5%) than the traditional IOM (Table 3). Paired t-test showed that this difference was statistically significant for inhalable dust. The IOMd showed a high degree of agreement with the traditional IOM for inhalable indium (CCC: 0.997, accuracy: 0.999, and precision: 0.998), but less agreement for inhalable dust (CCC: 0.886, accuracy: 0.896, and precision: 0.989) (Table 2). Analyses using imputed values for the eight IOMd respirable dust measurements below the LOD increased the sample size but showed even lower agreement between the sampler types for inhalable dust (CCC: 0.661, accuracy: 0.689, and precision: 0.959) (Table S3).
Scatterplots of the traditional IOM vs. IOMd illustrate strong agreement for inhalable indium with measurements close to the unity line (R2 = 0.997), but poor agreement for inhalable dust with measurements clustered above the unity line (Figures 1c and 1d). The OLS and orthogonal regression were very similar for both inhalable indium and dust. Scatterplots of the inhalable sampler types distinguishing measurements by department did not indicate a pattern of deviation by department due to paucity of data by department (Supplementary Figures S1c and S1d). The Bland-Altman difference plots show a slight positive bias for inhalable indium and a large negative bias for inhalable dust measured with IOMd, and the pattern suggests a possible concentration effect at higher concentrations (Figures 2c and 2d). Results of the one-way ANOVA models indicate significant effect of dust concentration on differences in sampler types for inhalable indium and inhalable dust (Tables 4 and S4).
Discussion
Physical and chemical characteristics of aerosols sampled in this ITO facility varied by department and location. Indium and dust size distributions were not always similar within departments and locations. Of the areas sampled, only the reclaim milling area and the refinery centrifuge had an indium MMAD in the respirable size range and a predominantly (>0.5) respirable mass fraction. All other areas sampled had indium MMADs in the thoracic and inhalable size fractions. Bimodal size distributions for indium aerosol were observed in areas where multiple processes were present, or where processes present included size separation of indium, such as in the centrifuge area of the refinery. Size distribution of dust measurements also varied greatly by department and location. GSDs for dust measurements ranged from 1.2–5, which suggested a large range in measured dust sizes. Some of the variability observed between indium and dust size distribution data may be due to the higher LOD for dust using gravimetric measurements compared to the LOD for indium using NIOSH method 7303. This difference in LOD for dust and indium (50–100-fold difference) would disproportionately affect dust measurements on stages that collect smaller particles, where larger numbers of particles are required to achieve the mass-based LOD. Additionally, discrepancies between indium and dust size distribution measurements may reflect different material types and mechanical processes present at each location and step of ITO production. Indium was present in all locations sampled except for forming where indium was not used. However, tin was quantified in only two locations in the reclaim area, likely due to its low proportion in the alloy (0.1–3.3%)[23] and a higher LOD.
The IOMd and the respirable cyclone showed good agreement for respirable indium and moderate agreement for respirable dust across a range of dust concentrations. Previous work by Kenny et al. suggested that the IOMd may be a valid alternative method to respirable cyclones for measuring respirable aerosol exposures.[10,15] However, Kenny et al. also cautioned that the IOMd performance should be verified in the occupational setting of interest to account for any sampling error due to dust loadings and different particle types.[10,15] Two previous studies of IOMd and respirable cyclone measurements of dust exposures in brick manufacturing or mining industries also observed differences between the IOMd and respirable cyclone performance.[19,20] However, unlike the results presented here, De Vocht et al. and Belle et al. reported that the IOMd collected less respirable dust mass than the respirable cyclone.[19,20] De Vocht et al. suggested that surface characteristics of the clay particulates sampled in a brick manufacturing setting may affect the IOMd foam filtering efficiency and may capture smaller particles in the foam resulting in lower respirable dust measurements with the IOMd.[19] Specifically, De Vocht et al. observed that the clay particulates consisted of weakly bonded, stacked layers that allow water or other polar molecules to enter between these layers.[19] De Vocht et al. hypothesized that the clay particulates might expand or form particles with increased aerodynamic diameters that will be captured by the foam insert.[19] Surface characteristics of the respirable dust aerosol may explain differences observed between the two respirable samplers;[19] however, the surface characteristics of the respirable dust at this facility were not evaluated. The indium aerosol and indium feedstock at this facility were previously analyzed by Badding et al. who characterized indium particles collected in eight locations, to include locations in the refinery, ITO, and reclaim.[23] Characterization results indicated a lack of porosity in the indium particulates, with crystalline structures observed for samples from ITO and reclaim.[23] The overall morphology of the indium aerosol and feedstock observed at this facility suggest that respirable indium particulates at this facility are less likely to expand or form particles with increased aerodynamic diameters that will be captured by the foam insert than the clay particulates analyzed in the study by De Vocht et al., and may help explain why the IOMd performed as well as the respirable cyclone when sampling respirable indium. Another study by Linnainmaa et al. reported that samples exceeding 4 mg of dust loading may underestimate the respirable fraction due to increased filter loading and filtering efficiency of the foam.[14] In the study presented here, no samples exceeded the suggested 4 mg sample loading limit. With the exception of one IOMd sample that had a total of 3.8 mg dust, all other samples were below 1.8 mg total dust loading. Smaller sample loading may explain why overall, the IOMd did not underestimate respirable exposures when compared to measurements using the respirable cyclone in the study presented here.
Differences between the two respirable samplers did not vary by department and were not concentration-dependent for respirable indium and respirable dust concentrations. However, our analyses by department were limited by small sample sizes. Because department may be a surrogate for dust concentration, sampler differences were also analyzed accounting for areas with low and high dust concentrations. No significant differences in sampler measurements for respirable indium or respirable dust were observed when stratified by dust concentrations.
The IOMd and the IOM sampler were in good overall agreement for measurements of inhalable indium (% difference = 4.8%) but differed significantly for inhalable dust (% difference = −31.5%). Differences between the two inhalable samplers did not vary by department for inhalable indium and dust. However, our analyses by department were limited by small sample sizes. Dust concentration had a significant effect on the percent differences between sampler types for both inhalable indium and for inhalable dust. Differences between the inhalable sampler types for inhalable dust were significantly larger at lower dust concentrations and may be due to increased variability in gravimetric analyses at lower dust loadings. Results from our study are similar to results from previous laboratory studies that reported difficulty with gravimetric analyses of inhalable dust measurements using the plastic IOM sampler.[31,32] Due to the variability in gravimetric analyses at lower masses of dust loading, Stacey et al. suggested that the plastic IOM sampler should only be used when several mg of dust loading are expected.[31] Additionally, Lid´en and Bergman suggest that plastic IOM samplers should be stored in the weighing room for at least 1 week after sampling to allow sampling cassettes a chance to equilibrate to and approach a stable weight.[33] The shorter time used to allow the plastic IOM samplers to equilibrate prior to the gravimetric analyses presented here also may have contributed to variability observed between the two inhalable sampler types. Further, Smith et al. observed that stainless steel cassettes are more stable than the plastic IOMs used in our study, and may be preferable for gravimetric analyses.[34] However, moisture absorption by the plastic foam insert may also affect measurements of inhalable dust concentrations regardless of the plastic or steel cassette housing.[14] Results from our field study are also similar to results from the field investigation of the IOM and IOMd by Linnainmaa et al. who also observed that the IOMd was not stable for inhalable dust measurements.[14]
A limitation of this study is that only field measurements were collected. Unlike environmental chamber tests, aerosol size distribution and concentration could not be directly controlled in this field investigation. A small sample size and inability to directly control aerosol size distribution and concentration limited the ability to quantify the effect of these factors on sampler performance. Additionally, air velocity, temperature, and relative humidity could not to directly controlled either, to quantify their effects on sampler performance. Another limitation is that NIOSH Method 7303 has not been validated for analysis of metals in the IOMd foam insert. However, LCS and blind spikes of the foam media had indium recovery well within statistical limits and all foam samples were recovery corrected with the average recovery.
Despite these limitations, the IOMd showed good agreement with the respirable cyclone for respirable and inhalable indium across a range of temperatures (range: 18.9–35.6 ○F), relative humidity (range: 20–82%), indium aerosol sizes (MMAD range: 0.9–20.1 mm), and concentrations (respirable indium range: < 0.14–296 mg/m3; inhalable indium range: 1.7–920.1 mg/m3). Results from this study suggest that the IOMd is a useful single sampler for simultaneous measurements of respirable and inhalable indium and may be applicable in other occupational settings where simultaneous measurements of respirable and inhalable elemental metal exposures are needed. However, it would be prudent to verify its performance in the workplace setting of interest to account for variability and any errors.
Conclusion
Results from this field investigation suggest that the IOMd sampler is a useful single sampler that can provide measurements of respirable and inhalable indium exposures. In ITO manufacturing settings, measurement of respirable indium is of interest for understanding risk of indium lung disease whereas inhalable indium would account for larger, thoracic and inhalable, indium particles that deposit in the upper and conducting airways and contribute to indium body burden. Inhalable indium exposure measurements may help explain the inconsistent correlations previously observed between indium blood levels and respirable indium exposure. The IOMd could be used to understand (i) sources of exposure to both respirable and inhalable indium aerosol and (ii) the effects of exposure to both respirable and inhalable size fractions on biological indicators associated with adverse respiratory outcomes such as measurements of indium in blood.
Supplementary Material
Acknowledgments
We would like to thank the following NIOSH staff for their help in data collection and analysis: Michael Beaty, Randy Boylstein, Matt Duling, Nicole Edwards, Deborah Hirst, Robert B. Lawrence, Stephen B. Martin, Ju-Hyeong Park, Chris Piacitelli, and Rena Saito.
Disclaimer
This work was supported by intramural funding from the National Institute for Occupational Safety and Health. The authors declare no conflicts of interest. The findings and conclusions in this report are those of the author(s) and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH), Centers for Disease Control and Prevention (CDC).
References
- [1].Hines CJ, Roberts JL, Andrews RN, Jackson MV, and Deddens JA: Use of and occupational exposure to indium in the United States. J. Occup. Environ. Hyg 10(12):723–733 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Cummings KJ, Nakano M, Omae K, et al. : Indium lung disease. Chest 141(6):1512–1521 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Nakano M, Omae K, Tanaka A, et al. : Causal relationship between indium compound inhalation and effects on the lungs. J. Occup. Health 51(6):513–521 (2009). [DOI] [PubMed] [Google Scholar]
- [4].Cummings KJ, Virji MA, Trapnell BC, Carey B, Healey T, and Kreiss K: Early changes in clinical, functional, and laboratory biomarkers in workers at risk of indium lung disease. Ann. Amer. Thorac. Soc 11(9):1395–1403 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Cummings KJ, Virji MA, Park JY, et al. : Respirable indium exposures, plasma indium, and respiratory health among indium-tin oxide (ITO) workers. Am. J. Ind. Med 59(7):522–531 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Liu N, Guan Y, Xue L, et al. : Assessment of DNA/chromosome damage in the peripheral blood lymphocytes of workers exposed to indium compounds. Toxicol. Sci 157(1):41–49 (2017). [DOI] [PubMed] [Google Scholar]
- [7].Hoet P, De Graef E, Swennen B, et al. : Occupational exposure to indium: What does biomonitoring tell us? Toxicol. Lett 213(1):122–128 (2012). [DOI] [PubMed] [Google Scholar]
- [8].Leach LJ, Scott JK, Armstrong RD, Steadman LT, and Maynard EA: The inhalation toxicity of indium sesquioxide in the rat. ORINS [reports]. U.S. Atomic Energy Commission UR-590:1–30 (1961). [DOI] [PubMed] [Google Scholar]
- [9].Cummings KJ, Donat WE, Ettensohn DB, Roggli VL, Ingram P, and Kreiss K: Pulmonary alveolar proteinosis in workers at an indium processing facility. Am. J. Respir. Crit. Care Med 181(5):458–464 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Kenny L, Chung K, Dilworth M, et al. : Applications of low-cost, dual-fraction dust samplers. Ann. Occup. Hyg 45(1):35–42 (2001). [PubMed] [Google Scholar]
- [11].Woehkenberg ML, and Bartley DL: Inhalable aerosol samplers. Appl. Ocup. Environ. Hyg 13(5):274–278 (1998). [Google Scholar]
- [12].Kenny LC, Aitken R, Chalmers C, et al. : A collaborative european study of personal inhalable aerosol sampler performance. Ann. Occup. Hyg 41(2):135–153 (1997). [DOI] [PubMed] [Google Scholar]
- [13].L’Orange C, Anderson K, Sleeth D, Anthony TR, and Volckens J: A simple and disposable sampler for inhalable aerosol. Ann. Occup. Hyg 60(2):150–160 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Linnainmaa M, Laitinen J, Leskinen A, Sippula O, and Kalliokoski P: Laboratory and field testing of sampling methods for inhalable and respirable dust. J. Occup. Environ. Hyg 5(1):28–35 (2007). [DOI] [PubMed] [Google Scholar]
- [15].Kenny L, Chung K, Dilworth M, et al. : Applications of low-cost, dual-fraction dust samplers. Ann. Occup. Hyg 45(1):35–42 (2001). [PubMed] [Google Scholar]
- [16].Demange M, Go€rner P, Elcabache J-M, and Wrobel R: Field comparison of 37-mm closed-face cassettes and IOM samplers. Appl. Occup. Environ. Hyg 17(3):200–208 (2002). [DOI] [PubMed] [Google Scholar]
- [17].Predicala BZ, and Maghirang RG: Field comparison of inhalable and total dust samplers for assessing airborne dust in swine confinement barns. Appl. Occup. Environ. Hyg 18(9):694–701 (2003). [DOI] [PubMed] [Google Scholar]
- [18].Martin JR, and Zalk DM: Comparison of total dust/inhalable dust sampling methods for the evaluation of airborne wood dust. Appl. Occup. Environ. Hyg 13(3):177–182 (1998). [Google Scholar]
- [19].De Vocht F, Hirst A, and Gardner A: Application of PUF foam inserts for respirable dust measurements in the brick-manufacturing industry. Ann. Occup. Hyg 53(1):19–25 (2009). [DOI] [PubMed] [Google Scholar]
- [20].Belle B: Experiences of the institute of occupational medicine foam respirable sampler use in mines (2012).
- [21].Teikari M, Linnainmaa M, Laitinen J, et al. : Laboratory and field testing of particle size-selective sampling methods for mineral dusts. AIHA J 64(3):312–318 (2003). [DOI] [PubMed] [Google Scholar]
- [22].Medvedovski E, Alvarez N, Yankov O, and Olsson MK: Advanced indium-tin oxide ceramics for sputtering targets. Ceram. Int 34(5): 1173–1182 (2008). [Google Scholar]
- [23].Badding MA, Stefaniak AB, Fix NR, Cummings KJ, and Leonard SS: Cytotoxicity and characterization of particles collected from an indium-tin oxide production facility. J. Toxicol. Environ. Heath Part A 77(20):1193–1209 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Cummings KJ, Suarthana E, Edwards N, et al. : Serial evaluations at an indium-tin oxide production facility. Am. J. Ind. Med 56(3):300–307 (2013). [DOI] [PubMed] [Google Scholar]
- [25].NIOSH: “NIOSH manual of analytical methods (NMAM®)” Cincinnati, OH, 2003. [Google Scholar]
- [26].Hewett P, and McCawley MA: A microcomputer spreadsheet technique for analyzing multimodal particle size distributions. Appl. Occup. Environ. Hyg 6(10):865–873 (1991). [Google Scholar]
- [27].Ganser GH, and Hewett P: An accurate substitution method for analyzing censored data. Appl. Occup. Environ. Hyg 7(4):233–244 (2010). [DOI] [PubMed] [Google Scholar]
- [28].Lin L, Hedayat AS, Sinha B, and Yang M: Statistical methods in assessing agreement. J. Am. Statist. Assoc 97(457):257–270 (2002). [Google Scholar]
- [29].Lin LI: A concordance correlation coefficient to evaluate reproducibility. Biometrics 45(1):255–268 (1989). [PubMed] [Google Scholar]
- [30].Lin LIK: Total deviation index for measuring individual agreement with applications in laboratory performance and bioequivalence. Stastist. Med 19(2):255–270 (2000). [DOI] [PubMed] [Google Scholar]
- [31].Stacey P, Revell G, and Tylee B: Accuracy and repeatability of weighing for occupational hygiene measurements: Results from an inter-laboratory comparison. Ann. Occup. Hyg 46(8):693–699 (2002). [DOI] [PubMed] [Google Scholar]
- [32].Smith JP, Bartley DL, and Kennedy ER: Laboratory investigation of the mass stability of sampling cassettes from inhalable aerosol samplers. Am. Industr. Hyg. Assoc. J 59(8):582–585 (1998). [DOI] [PubMed] [Google Scholar]
- [33].Lid´en G, and Bergman G: Weighing imprecision and handleability of the sampling cassettes of the IOM sampler for inhalable dust. Ann. Occup. Hyg 45(3):241–252 (2001). [DOI] [PubMed] [Google Scholar]
- [34].Smith AM, and Bernstein DI: Management of work-related asthma. J. Allerg. Clin. Immunol 123(3):551–557 (2009). [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.