

Summary
The aim of the present study was to evaluate the relationship between social deprivation indexes and anti-influenza vaccination coverage in the elderly population (over 65 years old) in Sardinia.
This relationship was first observed in a regional context. An already-known deprivation index was used, and its trivial relationship with anti-influenza vaccination coverage was evaluated. Secondly, the same relationship was assessed in the homogeneous area of the Municipality of Sassari. This required the adoption of an ad hoc deprivation index, which allowed us to stratify the population into deprivation groups and to correlate vaccination coverage with socio-economic variables.
The results showed that regional anti-influenza vaccination coverage increased linearly as deprivation decreased. This trend was confirmed in the Municipality of Sassari. Pearson’s analysis highlighted factors that significantly correlate with vaccination coverage.
In Sardinia, the relationship between anti-influenza vaccination coverage and socio-economic status is consistent with the international panorama, and highlights the necessity to implement interventions to promote vaccination coverage among the elderly.
Key words: Vaccines, Influenza, Social Deprivation Indexes, Elderly, Italy
Introduction
Socio-economic status and social deprivation influence adherence to health prevention programs, particularly those regarding vaccination [1-7].
The Italian Region of Sardinia participated in a project financed by the Italian Ministry of Health – (National Center for Disease Control and Prevention – CCM 2015: “Indici di deprivazione socioeconomica sanitaria e coperture vaccinali antinfluenzali negli anziani”, as stated by Article 4, paragraph 7 of the collaboration agreement), with the aim of assessing the relationship between socio-economic inequalities and low anti-influenza vaccination coverage among subjects aged over 65 years. To this end, characteristics of socio-economic status were examined in order to study their relationship with vaccination coverage and thus enable vaccination promotion strategies to be implemented on the basis of real needs [7-10].
The present study, which focused on the 2015 and 2016 seasonal influenza periods, was conducted in different phases: firstly, the trivial relationship between social deprivation and anti-influenza vaccination coverage in adults aged over 65 years was observed at the regional level among macro areas by means of an already known social index (IDMS) [8]. Secondly, the same relationship was evaluated by means of an ad hoc social index (SEHDI) for the homogeneous area of the Municipality of Sassari, in order to check for possible biases which could affect the trivial analysis.
Methods
RELATIONSHIP BETWEEN IDMS INDEX AND ANTI-INFLUENZA VACCINATION COVERAGE IN ADULTS AGED OVER 65 YEARS IN SARDINIA
According to the distribution of the population (1,658,138 inhabitants in 2016 in Sardinia), the regional territory is organized into 8 homogeneous areas (AO): 2 metropolitan areas, 5 aggregated communities, and 1 small geographically-isolated community. Each AO includes a Local Social-Health Area (ASSL), which is part of the Territorial Health Protection Agency (ATS), as stated by Regional Law [10]. The organization of the healthcare network is related to various territorial features, such as insularity, conformation, progressive depopulation of rural areas, and population and road distribution [11, 12]. On account of these features, Sardinia has already proved to be an excellent model for epidemiological studies [13].
In order to evaluate the coverage of anti-influenza vaccination offered to over-65s by the 8 ASSLs, data provided by the Regional Health Department referring to two influenza seasons (2015-2016) were analyzed [14].Furthermore, the relationship between the percentage of vaccination coverage and the Index of Sardinian Multiple Deprivation (IDMS) index [8], an index already available at the macro-area level, was evaluated by applying a simple linear regression model.
RELATIONSHIP BETWEEN SEHDI AND ANTI-INFLUENZA VACCINATION COVERAGE IN OVER-65S IN SASSARI
The homogeneous area of Sassari includes its municipal territory, which covers an area of 547.03 km² and has a density of 233.1 inhabitants per km². The municipal territory is divided into 998 census areas, based on common economic, social and/or environmental characteristics.
The relationship between social deprivation status and anti-influenza vaccination coverage in the over-65s was studied with regard to the specific urban and peri-urban area of the Municipality of Sassari. To this end, an ad hoc Socio-Economic Health Deprivation Index (SEHDI), developed by Lillini and Vercelli, was used. This enabled the population to be stratified into groups of deprivation. The methods used to develop the SEHDI and to define different deprivation groups were taken from the previous studies by Lillini and Vercelli on the development of local socio-economic deprivation indexes aimed at identifying health inequalities in the population on the basis of socio-economic stratification [15, 16].
The anti-influenza vaccination coverage rates among over-65s within the various deprivation groups were compared by means of the ANOVA with F-test and linearity test. Vaccination coverage data provided by General Practitioners (GPs) working in local clinics/polyclinics were obtained from the Municipal Social-Health District database.
Finally, the relationship between coverage and the SEHDI was elaborated by applying a linear regression model.
All of the data collected were processed by means of Excel (Microsoft Corp.) and STATA (STATA Corp). The datasets are available from the corresponding author on reasonable request.
Results
In recent years (2013-2016), a very low average anti-influenza vaccination coverage (around 40%) was recorded among over-65s in Sardinia, with high variability between areas and municipalities. In the 2015-2016 season, analysis per AO showed an inversely proportional relationship between anti-influenza coverage and the IDMS deprivation index (y = - 12.36x + 50.74; R^2 = 0.15), with the highest coverage observed in Ogliastra (Lanusei) (58%) and the lowest in Cagliari (28%) (Fig. 1).
Fig. 1.
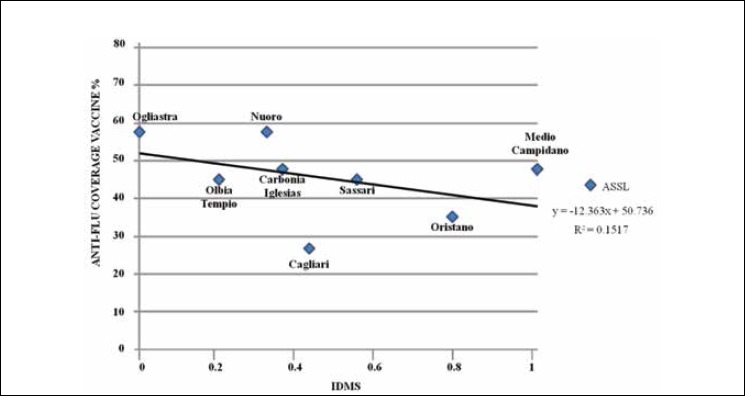
Relationship between the IDMS social index and anti-influenza vaccination coverage among subjects aged over 65 years observed in the 8 Sardinian Local Social-Health Areas (ASSL) during the period 2015-2016.
The survey of the urban and peri-urban areas of the Municipality of Sassari involved the local populations of 998 census areas, which amounted to 127,525 of the 334,103 residents of all ASSLs (74,349 adults over 65) during the survey period [12]. Of these, 111,437 were registered at 119 clinics, served by 96 GPs. Adults aged over 65 years numbered 27,496, of whom 23,943 constituted the sample under study.
On the basis of the SEHDI, the population was divided into 5 groups of deprivation: High Deprivation (7%), Medium-High Deprivation (13%), Medium Deprivation (61%), Medium-low Deprivation (11%) and Low Deprivation (8%).
The study area and the distribution of the SEHDI are depicted in Figure 2; as shown, it is not possible to identify a homogeneous territorial trend.
Fig. 2.
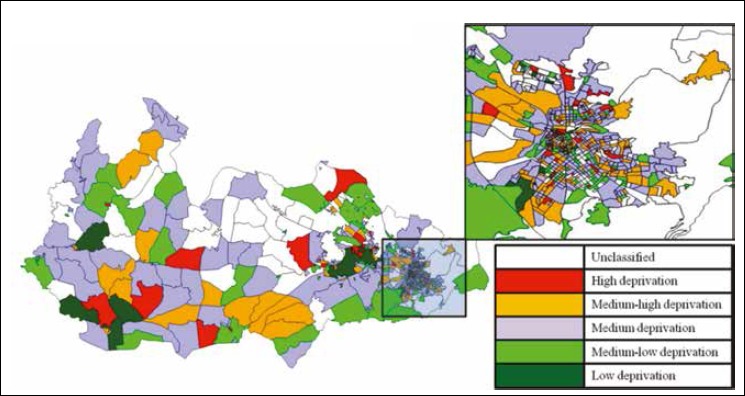
Graphic representation of census areas of the Municipality of Sassari.
Figure 3 shows the population of over-65s in Sassari, stratified according to the 5 above-mentioned SEHDI categories, in relation to anti-influenza vaccination coverage. A growing trend was observed as wealth increased (y = 1.2223x + 28.662; R^2 = 0.8735). Indeed, vaccination coverage was seen to vary from 30% in high deprivation areas to 34% in low deprivation areas, the difference being statistically significant (ANOVA (F); p < 0.05).
Fig. 3.
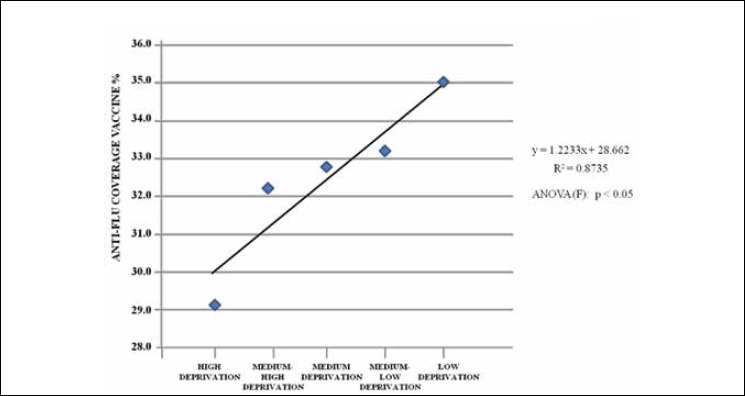
Relationship between SEHDI groups of deprivation and anti-influenza vaccination coverage.
Table I shows the correlation between the percentage of vaccination coverage in the over-65s and the socio-economic variables by census areas.
On the one hand, vaccination coverage increased as the following variables increased: percentage of married people, percentage of home-owners, and average number of people per occupied dwellings; on the other, it decreased as the percentage of foreigners and stateless persons residing in Italy, rented homes and 1-member families increased.
The vaccination coverage observed in the high deprivation group increased as the percentage of 2-member families and the old-age index rose, whereas it decreased as the percentage of those working in temporary jobs increased.
In the medium-high deprivation group, vaccination coverage was higher among graduates, the self-employed, and employees. Furthermore, vaccination coverage in the medium deprivation group increased as the percentage of 4-member families and those with average number of people per occupied dwellings, whereas it decreased as the percentage of tenants and 1-member families increased.
Vaccination coverage in the medium-low deprivation group increased as the percentage of foreigners and stateless residents in Italy rose. Finally, vaccination coverage in the low deprivation group rose as the percentage of single-parent families with children under 15 years old rose.
Discussion
Socio-economic deprivation in urban areas is closely associated with low vaccination coverage among high-risk groups, such as the elderly [3, 4, 17]. Indeed, socio-economic status is considered one of the main social determinants both of individuals’ health and of their adherence to preventive measures [17, 18]. In particular elderly people’s socio-economic status appears to play an important role in their compliance with anti-influenza vaccination [6, 7].
Low socio-economic status is usually correlated with low vaccination coverage, as reported in Spain, France and the United Kingdom [19]. In Italy, however, studies by Damiani and Chiatti [17, 20] seemed to suggest that the opposite was true, in that anti-influenza vaccination was found to be more widespread among elderly subjects belonging to more deprived social classes (65%) than among those from wealthier classes (57%).
The present study was conducted in various AOs throughout the Sardinia Region, though it focused on deprivation in the population of Sassari’s. The aim was to determine the relationship between influenza vaccination coverage and deprivation in an at-risk age-group (over-65s). In the past, urban and peri-urban areas of Sassari have been the focus of various health investigations [21, 25]. To the best of our knowledge, however, this is the first study to focus on the relationship between socio-economic status and vaccination coverage.
Data from the entire Sardinian Region, which were obtained by means of the IDMS deprivation index, showed an inverse correlation between vaccination coverage and deprivation. This finding is similar to that observed in the literature, but opposite to that recorded in Italy. Indeed, in Sardinia, influenza vaccination coverage in adults aged 65 years and over appears to decrease as deprivation increases. This difference between Sardinia and the national context could be attributed to two main reasons: 1) the non-homogeneous vaccination offer among the different AOs, which does not depend on the IDMS used, but could be due to a possible different agreement between the ASSLs and the GPs, who strongly influence vaccination uptake among the over-65s; 2) a variable relationship between vaccination coverage and status, which may be attributable, on the one hand, to a linear pattern at low levels of coverage, as in Sardinia, and, on the other, to a non-linear pattern at higher levels of vaccination coverage, such as those found in other territorial contexts [14, 16].
In order to exclude the potential bias due to possible different agreements with GPs, which could occur regardless of socio-economic determinants, our study focused on the AO of Sassari. The SEHDI enabled us to identify and evaluate the relationship between socio-economic inequalities and health outcomes. As suggested by the literature data [26, 27], using a deprivation index is useful in the study of the health characteristics of the population, particularly those of sensitive groups (e.g., populations at risk of late diagnosis and/or undergoing therapy for chronic-degenerative diseases) [27, 31]. We observed that flu vaccination coverage depends on SEHDI at the AO level, too.
Moreover, we observed a direct proportional correlation between vaccination coverage in over-65s and various socio-economic variables (percentage of married people, average number of people per occupied dwellings, rented homes, and 1-member families). Conversely, a statistically significant inverse relationship was seen between coverage and the percentage of foreigners and stateless persons residing in Italy, of those in rented homes and of 1-member families.
On the basis of these results, the present study confirms the role played by occupational and cultural factors in influencing adherence to anti-influenza immunization programs, as previously observed by several authors [6, 32, 33]. The relationship between influenza vaccination coverage and clusters of deprivation shows how cultural level and professional occupation positively influence adherence to flu vaccination among over-65s [6, 34].
Conclusions
In Sardinia, the relationship observed between low vaccination uptake and socio-economic status was consistent with that reported in the literature. The analysis of data on the Municipality of Sassari by means of an ad hoc deprivation index (SEHDI) confirmed the relationship seen at the regional level.
Our results emphasize the need to implement interventions for the promotion of vaccination [30, 35], especially in high- risk groups, such as the elderly, and to hone information on the main cultural and occupational factors observed.
Tab. I.
Correlation between socio-economic variables and vaccination coverage among residents aged over 65 years in the Municipality of Sassari, by deprivation group.
| Population observed | Socioeconomic variables | Pearson correlation | P-value |
|---|---|---|---|
| Over-65s resident in the Municipality of Sassari | % married | 0.120 | 0.032 |
| % foreigners and stateless persons residing in Italy | - 0.115 | 0.039 | |
| % rented homes | - 0.109 | 0.051 | |
| % owned homes | 0.135 | 0.016 | |
| % 1- member families | - 0.185 | 0.001 | |
| Number of components per family | 0.149 | 0.008 | |
| Average number of people per occupied dwelling | 0.129 | 0.019 | |
| Over-65s high deprivation | % 2- member families | 0.405* | 0.040 |
| % temporary job | - 0.389* | 0.050 | |
| Retirement index | 0.446* | 0.043 | |
| Over-65s medium-high deprivation | % degree or other academic qualification | 0.391** | 0.007 |
| % self-employed | 0.402** | 0.005 | |
| Activity rate | 0.293* | 0.046 | |
| Over-65s medium deprivation | % rented homes | - 0.147* | 0.034 |
| % 1- member families | - 0.248** | 0.000 | |
| % 4- member families | 0.219** | 0.001 | |
| Average number of people per occupied dwelling | 0.222** | 0.001 | |
| Average number of persons per family | 0.233** | 0.001 | |
| Over-65s, medium-low deprivation | % foreigners and stateless persons residing in Italy | - 0.594** | 0.009 |
| Over-65s, low deprivation | % single-parent families with children under 15 years | 0.544* | 0.013 |
*: p < 0.05
**: p < 0.01.
Acknowledgements
Project financed with the support of the Ministry of Health – CCM 2015, as in Article 4, paragraph 7 of the collaboration agreement.
List of abbreviations
- CCM
National Centre for Disease Control and Prevention
- AO
Homogeneous Area
- ASSL
Local Social-Health Area
- ATS
Territorial Health Protection Agency
- IDMS
Index of Sardinian Multiple Deprivation
- SEHDI
Socio-Economic Health Deprivation Index
Footnotes
Conflict of interest statement
None declared.
Authors’ contributions
PC conceived the study; MDM, ED and AAz collected the data; PC and AAr analyzed and interpreted the data; PC, MD and AAr wrote the paper; ED revised the manuscript. All authors have read and approved the final manuscript.
References
- [1].Peretti-Watel P, Raude J, Sagaon-Teyssier L, Constant A, Verger P, Beck F. Attitudes toward vaccination and the H1N1 vaccine: poor people’s unfounded fears or legitimate concerns of the elite? Soc Sci Med 2014;109:10-8. 10.1016/j.socscimed.2014.02.035 [DOI] [PubMed] [Google Scholar]
- [2].Cabrera-Barona P, Murphy T, Kienberger S, Blaschke T. A multi-criteria spatial deprivation index to support health inequality analyses. Int J Health Geogr 2015;14:1-14. 10.1186/s12942-015-0004-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Topuzoglu A, Ozaydin GAN, Cali S, Cebeci D, Kalaca S, Harmanci H. Assessment of sociodemographic factors and socio-economic status affecting the coverage of compulsory and private immunization services in Istanbul, Turkey. Public Health 2005;119:862-9. 10.1016/j.puhe.2005.01.015 [DOI] [PubMed] [Google Scholar]
- [4].Lopez de Andres A, Carrasco P, Hernández-Barrera V, Vázquez-Fernández S, Gil A, Jiménez-García R. Influenza vaccination among the elderly Spanish population: trend from 1993 to 2003 and vaccination-related factors. Eur J Public Health 2006;17:272-7. [DOI] [PubMed] [Google Scholar]
- [5].Lebel A, Pampalon R, Villeneuve PY. A multi-perspective approach for defining neighbourhood units in the context of a study on health inequalities in the Quebec City region. Int J Health Geogr 2007;6 10.1186/1476-072X-6-27 [DOI] [PMC free article] [PubMed]
- [6].Nagata JM, Hernández-Ramos I, Kurup AS, Albrecht D, Vivas-Torrealba C, Franco-Paredes C. Social determinants of health and seasonal influenza vaccination in adults ≥ 65 years: a systematic review of qualitative and quantitative data. BMC Public Health 2013;25;13:388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Istat. Percorsi evolutivi dei territori italiani. 60 anni di storia socio-demografica attraverso i dati censuari. [Google Scholar]
- [8].Serci A, De Arca A, Podda A, Perra S, Cabras S, Renoldi S. Indice di deprivazione multipla della Sardegna 2013. www.sardegnaprogrammazione.it/documenti/35_84_20140213123944.pdf. Accessed on 02 August 2018.
- [9].Bona L, Mundula L. Sviluppo socio-economico della Sardegna: federalismo, libertà repubblicana e reddito minimo garantito. 2012: pp. 13-5. [Google Scholar]
- [10].Legge Regionale 27 luglio 2016, n. 17 “Istituzione dell’Azienda per la tutela della salute (ATS) e disposizioni di adeguamento dell’assetto istituzionale e organizzativo del servizio sanitario regionale. Modifiche alla legge regionale 28 luglio 2006, n. 10 (Tutela della salute e riordino del servizio sanitario della Sardegna. Abrogazione della legge regionale 26 gennaio 1995, n. 5) e alla legge regionale 17 novembre 2014, n. 23 (Norme urgenti per la riforma del sistema sanitario regionale)”. Regione Autonoma della Sardegna. [Google Scholar]
- [11].Regione Autonoma della Sardena. Sardegna in cifre 2017. www.regione.sardegna.it/documenti/1_46_20170802113800.pdf. [Accessed on 06 November 2018].
- [12].Demo.Istat. http://demo.istat.it/pop2016/index.html. [Accessed on 02 August 2018].
- [13].Dettori M, Arru B, Azara A, Piana A, Mariotti G, Camerada MV, Stefanelli P, Rezza G, Castiglia P. In the digital era, is community outrage a feasible proxy indicator of emotional epidemiology? The case of meningococcal disease in Sardinia, Italy. Int J Environ Res Public Health 2018;15:1-8. 10.3390/ijerph15071512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Ministero della Salute. Prevenzione e controllo dell’influenza: raccomandazioni per la stagione 2015-2016. www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=0&codLeg=52703&parte=1%20&serie. [Accessed on 06 November 2018].
- [15].Lillini R, Quaglia A, Vercelli M, Registro mortalità Regione Liguria Building of a local deprivation index to measure the health status in the Liguria Region. Epidemiol Prev 2012;36:180-7. [PubMed] [Google Scholar]
- [16].Quaglia A, Lillini R, Casella C, Giachero G, Izzotti A, Vercelli M, Liguria Region Tumour Registry The combined effect of age and socio-economic status on breast cancer survival. Crit Rev Oncol Hematol 2011;77:210-20. [DOI] [PubMed] [Google Scholar]
- [17].Damiani G, Federico B, Visca M, Agostini F, Ricciardi W. The impact of socioeconomic level on influenza vaccination among Italian adults and elderly: a cross-sectional study. Preventive Medicine 2007;45:373-9. [DOI] [PubMed] [Google Scholar]
- [18].D’Alessandro D, Arletti S, Azara A, Buffoli M, Capasso L, Cappuccitti A, Casuccio A, Cecchini A, Costa G, De Martino AM, Dettori M, Di Rosa E, Fara GM, Ferrante M, Giammanco G, Lauria A, Melis G, Moscato U, Oberti I, Patrizio C, Petronio MG, Rebecchi A, Romano Spica V, Settimo G, Signorelli C, Capolongo S, and the attendees of the 50th Course “Urban Health. Instruments for promoting health and for assessing the hygienic and sanitary conditions in urban areas”. Strategies for disease prevention and health promotion in urban areas: the Erice 50 Charter. Ann Ig 2017;29:481-93. 10.7416/ai.2017.2179. [DOI] [PubMed] [Google Scholar]
- [19].Guillaume E, Pornet C, Dejardin O, Launay L, Lillini R, Vercelli M, Marí-Dell'Olmo M, Fernández Fontelo A, Borrell C, Ribeiro AI, de Pina MF, Mayer A, Delpierre C, Rachet B, Launoy G. Development of a cross-cultural deprivation index In five European countries. J. Epidemiol Community Health 2015. doi:10.1136/jech-2015-205729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Chiatti C, Di Rosa M, Barbadoro P, Lamura G, Di Stanislao F, Prospero E. Socioeconomic determinants of influenza vaccination among older adults in Italy. Prev Med 2010;51:332-3. [DOI] [PubMed] [Google Scholar]
- [21].Firenze A, Calamusa G, Amodio E, Morici M, Di Paquale M, Mazzucco W, Azara A, Muresu E, Dettori M, Maida G, Gelsomino V, Vitale F. Evaluation of radon levels in indoor gymnasia of Palermo (Sicily) and Sassari (Sardinia). Ital J Public Health 2009;6:316-22. [Google Scholar]
- [22].Dettori M, Piana A, Castiglia P, Loria E, Azara A. Qualitative and quantitative aspects of drinking water supply in Sardinia, Italy. A descriptive analysis of the ordinances and public notices issued during the years 2010-2015. Ann Ig 2016;28:296-303. [DOI] [PubMed] [Google Scholar]
- [23].Azara A, Muresu E, Dettori M, Ciappeddu P, Deidda A, Maida A. First results on the use of chloramines to reduce disinfection by products in drinking water. Ig Sanita Pubbl 2010;66:583-600. [PubMed] [Google Scholar]
- [24].Azara A, Castiglia P, Piana A, Masia MD, Palmieri A, Arru B, Maida G, Dettori M. Derogation from drinking water quality standards in Italy according to the European Directive 98/83/EC and the Legislative Decree 31/2001 - a look at the recent past. Ann Ig 2018;30:517-26. doi:10.7416/ai.2018.2252. [DOI] [PubMed] [Google Scholar]
- [25].Castiglia P, Solinas G, Sotgiu G, Palmieri A, Maida A, Dettori M. Epidemiology of hydatidosis in the province of Sassari, Italy. Parassitologia 2004;46(4). [PubMed] [Google Scholar]
- [26].Caranci N, Costa G. Un indice di deprivazione a livello aggregato da utilizzare su scala nazionale: giustificazioni e composizione dell’indice. Costa G, Cislaghi C, Caranci N. (eds.). Disuguaglianze sociali di salute. Problemi di definizione e di misura. Salute e Società; 2009;7:1. [Google Scholar]
- [27].Woods LM, Rachet B, Coleman MP. Choice of geographic unit influences socioeconomic inequalities in breast cancer survival. Br J Cancer 2005;92:1279-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Domínguez-Berjón F, Borrell C, Rodríguez-Sanz M, Pastor V. The usefulness of area-based socioeconomic measures to monitor social inequalities in health in Southern Europe. Eur J Public Health 2006;16:54-61. [DOI] [PubMed] [Google Scholar]
- [29].Puigpinòs R, Borrell C, Antunes JLF, Azlor E, Pasarín MI, Serral G, Pons-Vigués M, Rodríguez-Sanz M, Fernández E. Trends in socioeconomic inequalities in cancer mortality in Barcelona: 1992-2003. BMC Public Health 2009;9:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].De Andres AL, Garrido PC, Hernández-Barrera V, Del Pozo SVF, De Miguel ÁG, Jiménez-García R. Influenza vaccination among the elderly Spanish population: trend from 1993 to 2003 and vaccination-related factors. Eur J Public Health 2007:17:272-7. 10.1093/eurpub/ckl242 [DOI] [PubMed] [Google Scholar]
- [31].Newton JN, Briggs AD, Murray CJ, Dicker D, Foreman KJ, Wang H, Naghavi M, Forouzanfar MH, Ohno SL, Barber RM, Vos T, Stanaway JD, Schmidt JC, Hughes AJ, Fay DF, Ecob R, Gresser C, McKee M, Rutter H, Abubakar I, Ali R, Anderson HR, Banerjee A, Bennett DA, Bernabé E, Bhui KS, Biryukov SM, Bourne RR, Brayne CE, Bruce NG, Brugha TS, Burch M, Capewell S, Casey D, Chowdhury R, Coates MM, Cooper C, Critchley JA, Dargan PI, Dherani MK, Elliott P, Ezzati M, Fenton KA, Fraser MS, Fürst T, Greaves F, Green MA, Gunnell DJ, Hannigan BM, Hay RJ, Hay SI, Hemingway H, Larson HJ, Looker KJ, Lunevicius R, Lyons RA, Marcenes W, Mason-Jones AJ, Matthews FE, Moller H, Murdoch ME, Newton CR, Pearce N, Piel FB, Pope D, Rahimi K, Rodriguez A, Scarborough P, Schumacher AE, Shiue I, Smeeth L, Tedstone A, Valabhji J, Williams HC, Wolfe CD, Woolf AD, Davis AC. Changes in health in England, with analysis by English regions and areas of deprivation, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;386:2257-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Khan SR, Hall AG, Tanner RJ, Marlow NM. Association between race/ethnicity and disability status and receipt of vaccines among older adults in Florida. Disabil Health J 2018;11:339-44. [DOI] [PubMed] [Google Scholar]
- [33].Evans MR, Watson PA. Why do older people not get immunised against influenza? A community survey. Vaccine 2003;21:2421-7. [DOI] [PubMed] [Google Scholar]
- [34].Schensul J, Radda K, Coman E, Vazquez E. Multi-level intervention to prevent influenza infections in older low income and minority adults. Am J Comm Psychol 2009;43:313-29. [DOI] [PubMed] [Google Scholar]
- [35].Vukovic V, Gasparini R, Amicizia D, Arata L, Boccalini S, Fortunato F, Lillini R, Panatto D, Stefanati A, de Waure C. Identifying elderly with low vaccine uptake using social deprivation indices: a systematic review. Eur J Public Health 2017;27(3). 10.1093/eurpub/ckx187.381 [DOI] [Google Scholar]