

Abstract
Background:
Responding to the disparities in accessing and obtaining health information and healthcare among immigrant populations, the present study focused on Asian Americans. Using a sample that reflects Asian Americans’ cultural and linguistic diversities, the goal was to explore the typologies of health information source and their predictability to unmet healthcare needs (i.e., the experience of not being able to get needed medical care).
Methods:
Data were drawn from the 2015 Asian American Quality of Life Survey (N = 2,592), conducted using culturally and linguistically sensitive approaches. Latent class analysis on nine sources of health information across interpersonal networks (family members, close friends, acquaintances, and health professionals) and Internet-based communication technologies (mobile apps, email listservs, social networking sites, online communities, and health websites) identified six classes: ‘resource-heavy,’ ‘human-oriented,’ ‘expertise-focused,’ ‘family-dominant,’ ‘resource-scarce,’ and ‘health professional-dominant.’ Results: Compared to the resource-heavy group, the odds of having an unmet healthcare need were 2.94 times greater in the family-dominant group and 4.13 times greater in the resource-scarce group.
Discussion:
Findings provide implications for interventions with respect to subgroups to be prioritized and areas to be targeted in efforts to promote access and acquisition of health information and health services in Asian Americans.
Unmet healthcare needs have been widely used in health services research as an index to explore racial/ethnic disparities in health-care (Smedley, Stith, & Nelson, 2002; U.S. Department of Health and Human Services, 2016). National studies using English as a primary survey/interview language often portray Asian Americans favorably with respect to their access to healthcare (Chevarley, 2010; Shi, Lebrun, & Tsai, 2010; Shi & Stevens, 2005). However, studies using community-based samples of Asian Americans collected through culturally and linguistically sensitive approaches demonstrate a wide range of within group variations and a particular vulnerability of subgroups (Jang et al., 2018). For example, according to the Medical Expenditure Panel Survey (MEPS), Asian Americans have the lowest rate (2.8%) of unmet healthcare needs of all racial/ethnic groups (Chevarley, 2010). However, the rate goes up to 12% when the same question was asked to a sample of Asian Americans surveyed by offering an option of using English or their native language version of the questionnaire (Jang et al., 2018). Along the line, there has been an increasing number of studies exploring the factors that facilitate (e.g., English proficiency, health insurance coverage, and social support) or hinder (e.g., low socioeconomic status and negative cultural beliefs) the access to healthcare (Chevarley, 2010; Jang et al., 2018; Shi et al., 2010; Shi & Stevens, 2005). One area that deserves attention and is focus of the present investigation is the source of health information.
The benefits of health information such as facilitation of positive health behaviors and promotions of physical and mental health have been widely known (Clayman, Manganello, Viswanath, Hesse, & Arora, 2010; Richardson, Allen, Xiao, & Vallone, 2012). However, foreign-born immigrants, compared to their US-born counterparts, have fewer health information-seeking experience, less trust in health information, and less confidence in obtaining health informa-tion (Yoon, 2014; Zhao, 2010). Although the rate of health informa-tion-seeking experiences among foreign-born immigrants has increased from 38% to 70% between 2005 and 2014 (Yoon, Huang, & Kim, 2017), many members of the foreign-born population, including a substantial proportion of Asian Americans, still face persistent disparities in accessing and using health information, which may also contribute to their unmet needs for healthcare.
Although the sources of health information vary by the target group (Islam et al., 2016), Internet has often been reported as a popular source of health information across diverse populations (Yoon et al., 2017). With its easy access, anonymity, and language capacity, online health information brings particular benefits to immigrant populations (Wang & Yu, 2015; Yoon et al., 2017). Studies also demonstrate the importance of social networks, such as family, friends, neighbors, co-workers, and church members. The advantages of the interpersonal sources not only include their approachability but also similarities in understandings, experiences, and beliefs in health and healthcare (Davies & Bath, 2002; Kim, Kreps, & Shin, 2015; Todd & Hoffman-Goetz, 2011). It is not surprising that individuals with language barriers have a high reliance on the Internet and media sources in their native language and social network members sharing the same language and culture (Islam et al., 2016; Wang & Yu, 2015). Another important factor in health information seeking is the credibility of the source (Oh, Jun, Zhao, Kreps, & Lee, 2015; Ruppel & Rains, 2012). In a study with Korean American women (Oh et al., 2015), doctors or other health professionals were found to be more trusted than family, friends or media sources in seeking cancer-related information.
It is notable that the aforementioned studies tend to focus on descriptive characteristics of the source of health information by using a variable-centered method. The present study employed a person-centered approach in order to directly identify groups/clusters of individuals who share a similar profile in the sources of health information. Given the presence of multiple sources, their interrelated natures, and the different weight that each source carries (Chen, Kendall, & Shyu, 2010; Ruppel & Rains, 2012), latent class analysis (LCA) serves as an optimal way of systematically identifying group typologies (Muthén, 2001; Thorpe, Thorpe, Kennelty, & Pandhi, 2011). In the present study, latent profiling was performed on various sources of health information that pertain to interpersonal networks (family members, close friends, acquaintances, and health professionals) and Internet-based communication technologies (mobile apps, email listservs, social networking sites, online communities, and health websites).
The aims of the present study were (1) to identify the typologies of the source of health information, (2) to contrast the characteristics of the identified groups, and (3) to examine how the identified typologies were associated with the unmet health-care needs. The use of LCA will identify subgroups/patterns of health information-seeking behaviors, which cannot be obtained from variable-centered approaches. Based on the review, it was hypothesized that diverse groups of health information sources would emerge and that the groups would be differentially associated with demographic variables (age, gender, marital status, education, and ethnic origin), immigration-related variables (nativity, time in the USA, and English proficiency), health and access variables (chronic medical condition, self-rated health, and health insurance), and unmet healthcare needs. The identified typologies would also be different in the estimates of the odds of having an unmet healthcare need.
Methods
Sample
Data were drawn from the 2015 Asian American Quality of Life (AAQoL) survey. The survey is part of the City of Austin’s AAQoL initiative which was conducted in response to the rapid growth of the Asian American population in the area. Currently, an estimated 110,000 to 115,000 Asians live in metropolitan Austin, and the size of the Asian community has been doubled every 12 years (City of Austin, 2017). Asian Indian, Chinese, Vietnamese, Korean, and Filipino are identified as the five largest Asian groups in Austin, and these groups comprise about 87% of the total Asian population in the area.
The AAQoL survey was conducted with self-identified Asian Americans aged 18 and older living in the Austin area. In order to reach the broadest possible audience, the survey was conducted with culturally and linguistically sensitive approaches that included: (1) providing both English and Asian language versions of the survey questionnaire, (2) using research person-nel (e.g., recruiters and survey assistants) who shared the lan-guages and cultures of the target populations, and (3) building a strong partnership between the research team and key indivi-duals and organizations within ethnic communities.
The 10-page questionnaire for the AAQoL addresses various topics including immigration and acculturation, health and mental health, service utilization, social and community resources, and information-seeking behaviors. The questionnaire was originally developed in English and then translated into the languages of major Asian groups (e.g., Chinese, Vietnamese, Korean, Hindi, Gujarati, and Tagalog). In the case of Chinese, both traditional and simplified versions were prepared. The initial translations were conducted by 8 professional translators and graduate-level bilingual researchers. For each language, the translated version was reviewed for accuracy by two or more bilingual volunteers. Upon refinement of the questionnaire, each language version was pilot tested with 3–5 community members who were representatives of the target group and spoke the target language.
The surveys were completed using a paper and pencil questionnaire in the participants’ preferred languages. Recognizing that Asian Americans are often difficult to locate using standard recruitment strategies and that reliance on a single source can increase the chances for bias, multiple potential survey sites were contacted. In addition, the project was publicized through media and ethnic com-munity sources, and referrals for individuals, groups, and organizations were actively sought. A total of 76 survey sessions took place at various locations and events across the City of Austin (e.g., churches, temples, grocery stores, small group meetings, and cultural events) from August to December, 2015. While the surveys were self-administered, bilingual research assistants at each survey site provided survey assistance. It took about 20 minutes to complete the 10-page questionnaire, and respondents were each paid US $10 for their participation. The AAQoL project was approved by a university’s Institutional Review Board. Of a total of 2,614 individuals who participated in the AAQoL survey, about half (48.5%) used survey questionnaires in languages other than English. After removing cases with missing information on health information sources, the final sample size was 2,592. More information on the AAQoL survey is available elsewhere (City of Austin, 2017).
Measures
Unmet Healthcare Needs
Adapted from national surveys (Chevarley, 2010; Shi & Stevens, 2005), unmet healthcare needs were assessed with a single item asking respondents whether there was a time in the past 12 months when they needed medical care but could not get it. Responses were coded as “no” (0) or “yes” (1). The item has been widely used in healthcare planning and policies as an index of populations’ access to healthcare (Chevarley, 2010; Shi & Stevens, 2005).
Sources of Health Information
Using a list of nine sources that covers both interpersonal networks (family members, close friends, acquaintances, and health professionals) and Internet-based communication technologies (mobile apps, email listservs, social networking sites, online communities, and health websites), participants were asked to indicate all sources that they get health-related information. For each source, responses were coded as “no use” (0) or “use” (1).
Demographic Variables
Background information included age (0 = 18−39; 1 = 40−59; 2 = 60 and older), gender (0 = male, 1 = female), marital status (0 = married, 1 = not married), education (0 = ≥ high-school graduation, 1 = < high-school graduation), and ethnic origin (0 = Chinese, 1 = Asian Indian, 2 = Korean, 3 = Vietnamese, 4 = Filipino, 5 = Other Asian).
Immigration-Related Variables
As indices of the status of immigration and acculturation, nativity (0 = US-born, 1 = foreign-born), time in the USA (0 = ≥ 10 years, 1 = < 10 years), and English proficiency (0 = English proficient, 1 = limited English proficiency) were used. Dichotomy of the duration of residence was based on the immigration literature suggesting the tenth year as a marker of adaptation (Beiser & Edwards, 1994). English proficiency was assessed with a question about how well the respondent spoke English, using a 4-point response scale ranging from “not at all” to “very well.” Using the US Census criteria (Pandya, McHugh, & Batalova, 2011), those who reported that they spoke English less than “very well” were categorized as a group with limited English proficiency.
Health and Access Variables
Chronic medical condition and self-rated health were used as indicators of health. Total count from the checklist of 10 chronic diseases and conditions (diabetes, cancer, arthritis, heart disease, high blood pressure, stroke, liver disease, kidney problem, asthma, and chronic obstructive pulmonary disease) was recoded into binary categories (0 = none, 1 = one or more). Respondents rated their current health on a 5-point scale. Responses were then dichotomized into “excellent/very good/good” (0) and “fair/poor” (1). As an access variable, health insurance coverage was coded as “insured” (0) or “not insured” (1).
Analytic Strategy
After assessing descriptive characteristics of the sample, LCA was conducted using the nine binary variables of the sources of health information as criterion variables. Starting from two class model, LCA analysis increased the number of classes at subsequent analyses and compared the fit between models. The optimal number of classes was assessed based on an evaluation of conceptually meaningful groups and several indices of model fit including Bayesian information criterion (BIC), entropy (index of the classification quality), Lo–Mendell–Rubin likelihood ratio test (LMR-LRT), bootstrap likelihood test (BLRT), and posterior probabilities. Once the optimal model solution was identified, the groups of health information sources were named to capture their distinct characteristics. The groups were compared with respect to the criterion variables, demographic characteristics, immigration-related characteristics, health and access indicators, and unmet healthcare needs. Chi-square tests were used in group comparisons. Finally, logistic regression models of the unmet need for healthcare were estimated. Analyses were performed using Mplus version 8 and SPSS statistical programs version 24.
Results
Descriptive Characteristics of the Sample
Table 1 summarized the descriptive characteristics of the overall sample. The mean age was 42.8 (SD = 17.1), ranging from 18 to About 20% of the participants were 60 and older. More than half (55.1%) were female, and 33.4% were unmarried. About 19% had received less than a high-school education. The sample included Chinese (24.6%), Asian Indian (22%), Korean (18.1%), Vietnamese (19.6%), Filipino (10%), and other Asians (5.6%).
Table 1.
Descriptive characteristics of the overall sample (N = 2,592)
| % | |
|---|---|
| Demographic variable | |
| Age | |
| 18–39 | 48.4 |
| 40–59 | 31.2 |
| 60 and over | 20.4 |
| Gender | |
| Male | 44.9 |
| Female | 55.1 |
| Marital status | |
| Married | 66.6 |
| Not married | 33.4 |
| Education | |
| ≥ High school | 81.5 |
| < High school | 18.5 |
| Ethnicity | |
| Chinese | 24.6 |
| Asian Indian | 22.0 |
| Korean | 18.1 |
| Vietnamese | 19.6 |
| Filipino | 10.0 |
| Other | 5.6 |
| Immigration-related variable | |
| Nativity | |
| US-born | 9.2 |
| Foreign-born | 90.8 |
| Time in the USA | |
| ≥ 10 years | 58.5 |
| < 10 years | 41.5 |
| English proficiency | |
| Proficient | 37.8 |
| Limited | 62.2 |
| Health and access variable | |
| Chronic medical condition | |
| None | 71.7 |
| One or more | 28.3 |
| Self-rated health | |
| Excellent/very good/good | 89.4 |
| Fair/poor | 10.6 |
| Health insurance | |
| Insured | 85.3 |
| Not insured | 14.7 |
| Source of health information | |
| Family members | 51.4 |
| Close friends | 37.6 |
| Acquaintance | 17.7 |
| Health professionals | 48.9 |
| Mobile apps | 9.4 |
| Email listservs | 12.1 |
| Social networking sites | 17.4 |
| Online communities | 15.8 |
| Health websites | 42.8 |
| Unmet healthcare needs | 11.5 |
About 91% of the participants were foreign-born, 42% had stayed in the USA less than 10 years, and more than 62% had limited English proficiency. More than a quarter of the sample (28.3%) had at least one chronic medical condition, and 11% rated their health as either fair or poor. Approximately 15% of the sample had no health insurance coverage.
With regard to the source of health information, family members (51.4%) were most frequently reported, followed by health professionals (48.9%) and health websites (42.8%). Acquaintances, mobile apps, email listservs, social networking sites, and online communities were each endorsed by less than 20% of the sample. About 12% of the participants had an experience of not being able to use the needed medical care in the past 12 months.
Latent Class Analysis
The results of a series of LCA are summarized in Table 2. Based on multiple model-fit criteria and an evaluation of conceptually meaningful groups, the six-class model was identified as most optimal. Generally, lower BIC values and higher entropy values indicate higher model fit and classification quality. The two likelihood ratio tests (LMR-LRT and BLRT) compare two adjacent models: the (c–1)-class model vs. the c-class model, with significant p-values suggesting the current model performs better than the prior model. Another consideration for determining the number of classes was to evaluate posterior probabilities, which contains the matrix of conditional probabilities for cases to be placed in their respective class; diagonal values closer to one indicate higher classification quality.
Table 2.
Model fit statistics for selecting the optimal number of the classes
| Model | BIC | Entropy | LMR-LRT (H0 = k − 1 classes) | BLRT (H0 = k − 1 classes) |
|---|---|---|---|---|
| 2-class | 24051.07 | .76 | p = .13 | p = .00 |
| 3-class | 23759.37 | .59 | p = .00 | p = .00 |
| 4-class | 23660.58 | .65 | p = .16 | p = 1.00 |
| 5-class | 23632.25 | .69 | p = .09 | p = .00 |
| 6-class | 23609.11 | .70 | p = .00 | p = .00 |
| 7-class | 23620.16 | .71 | p = .03 | p = .00 |
Note. BIC = Bayesian information criterion; LMR-LRT = Lo–Mendell–Rubin likelihood ratio test; BLRT = bootstrap likelihood ratio test; The best class solutions can be achieved with low BIC values, high entropy (i.e., an index of the classification quality). Additionally, the LMR-LRT and BLRT compare the current model (c-Class) with prior model (c-1 Class). The significant p-value suggests that the current model performs better than the prior model; Selected model is bolded.
The results suggest that the six-class model had the lowest BIC value and about the same level of entropy value (.70) compared to adjacent five-class or seven-class model (.69 vs. .71). Although likelihood tests indicated the six-class model was no better than the five-class model, the former had lower BIC value. The six-class model was comparable to seven-class model, yet the latter had an increase in BIC value and had a class with few cases. In the six-class model, the average latent class probabilities for most likely latent class membership (not shown in the Table) ranged from .71 to .87, demonstrating decent classification quality. Based on statistical and conceptual considerations and model parsimony, we selected the six-class model as the most optimal solution.
Profiles of the Health Information Sources
Table 3 presents the characteristics of the six classes with respect to the nine criterion variables on which the LCA was based. To illustrate the profiles graphically, Figure 1 presents the average conditional probabilities of being in each of six classes. After reviewing the distributions of the sources of health information, the groups were named resource-heavy, human-oriented, expertise-focused, family-dominant, resource-scarce, and health professional-dominant.
Table 3.
Profiles of the sources of health information
| Class 1: resource-heavy (n = 116, 4.9%) | Class 2: human-oriented (n = 665, 24.1%) | Class 3: expertise-focused (n = 860, 35.8%) | Class 4: family-dominant (n = 240, 8.1%) | Class 5: resource-scarce (n = 431, 18.4%) | Class 6: health professional-dominant (n = 280, 8.8%) | |
|---|---|---|---|---|---|---|
| Family members | 87.1 | 97.7 | 33.6 | 100 | 12.3 | 0 |
| Close friends | 89.7 | 95.2 | 9.1 | 0 | 32.3 | 7.5 |
| Acquaintances | 71.6 | 35.6 | 1.9 | 0 | 25.3 | 5.4 |
| Health professionals | 83.6 | 51.7 | 63.5 | 0 | 0 | 100 |
| Mobile apps | 60.3 | 6.8 | 13.4 | 0 | 3.5 | 0 |
| Email listservs | 64.7 | 11.6 | 9.0 | 0 | 19.5 | 0 |
| Social networking sites | 94.0 | 18.3 | 16.6 | 0 | 17.9 | 0 |
| Online communities | 87.9 | 12.6 | 18.5 | 0 | 15.1 | 0 |
| Health websites | 89.7 | 45.3 | 80.0 | 0 | 3.5 | 0 |
Figure 1.
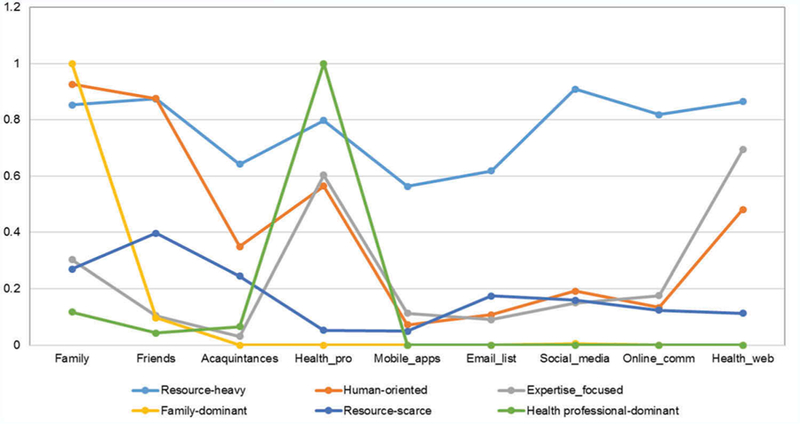
Conditional probabilities of the six groups of health information sources.
The smallest group of all, the resource-heavy group (n = 116) utilized all sources of health information with using social network sites most frequently (94%) and mobile apps least frequently (60.3%). The human-oriented group (n = 665) relied mostly on the sources based on human interactions such as family members (97.7%), close friends (95.2%), health professionals (51.7%), and acquaintances (35.6%). The expertise-focused group was the largest (n = 860) and relied heavily on health professionals (63.5%) and health websites (80%). The family-dominant group (n = 240) presented a full reliance on their family (100%) but no use of other sources. The resource-scarce group (n = 431) had a relatively low engagement across all types of health information sources, the usage rate ranging from 0% (health professionals) to 32.3% (close friends). The health professional-dominant group (n = 280) counted exclusively on health professionals (100%) as their source of health information.
Characteristics of the Six Classes of Health Information Sources
In addition to criterion variables, the six classes were compared with respect to demographic characteristics, immigration-related variables, health and access variables, and unmet healthcare needs. The results are summarized in Table 4. The young, middle, and old age groups were most represented by the human-oriented, health professional-dominant, and family-dominant groups, respectively. The health professional-dominant group had the highest proportion of being married and the family-dominant group had the highest proportion of not being married. A majority of the expertise-focused group had greater than high-school education whereas one third of the familydominant received less than high-school education. In terms of ethnicity distribution, Chinese were more likely to belong to the human-oriented, expertise-focused, and family-oriented groups. Asian Indians were about equally dispersed across classes. Koreans were most likely to belong to resource-scarce group and least likely to belong to resource-heavy group. Vietnamese were more likely to be health professional-dominant and less likely to be human-oriented. Filipinos tended to be resource-heavy and family-dominant; only a small portion belonged to the resource-scarce group. Members of the other Asian group were spread out across classes.
Table 4.
Characteristics of the six classes
| Class 1: resource-heavy (n = 116) | Class 2: human-oriented (n = 665) | Class 3: expertise-focused (n = 860) | Class 4: family-dominant (n = 240) | Class 5: resource-scarce (n = 431) | Class 6: health professional-dominant (n = 280) | χ2 | |
|---|---|---|---|---|---|---|---|
| Demographic variable | |||||||
| Age | 77.0*** | ||||||
| 18–39 | 44.8 | 56.3 | 51.3 | 42.7 | 44.3 | 33.3 | |
| 40–59 | 35.3 | 25.6 | 31.9 | 24.7 | 35.7 | 39.8 | |
| 60 and over | 19.8 | 18.1 | 16.9 | 32.6 | 20.0 | 26.9 | |
| Gender | |||||||
| Male | 50.0 | 47.9 | 44.4 | 40.9 | 43.2 | 42.9 | 6.24 |
| Female | 50.0 | 52.1 | 55.6 | 59.1 | 56.8 | 57.1 | |
| Marital status | |||||||
| Married | 69.6 | 62.6 | 69.0 | 62.2 | 65.4 | 72.8 | 14.5* |
| Not married | 30.4 | 37.4 | 31.0 | 37.8 | 34.6 | 27.2 | |
| Education | |||||||
| ≥ High school | 81.7 | 84.2 | 88.9 | 66.7 | 76.4 | 72.7 | 90.4*** |
| < High school | 18.3 | 15.8 | 11.1 | 33.3 | 23.6 | 27.3 | |
| Ethnicity | |||||||
| Chinese | 21.6 | 32.5 | 27.0 | 22.5 | 18.8 | 10.7 | 203.6*** |
| Asian Indian | 22.4 | 23.8 | 21.0 | 23.8 | 22.3 | 18.2 | |
| Korean | 7.8 | 18.8 | 17.2 | 13.3 | 26.2 | 15.4 | |
| Vietnamese | 28.4 | 14.1 | 14.8 | 20.0 | 23.7 | 37.5 | |
| Filipino | 16.4 | 6.6 | 12.6 | 15.4 | 3.9 | 12.5 | |
| Other | 3.4 | 4.2 | 7.4 | 5.0 | 5.1 | 5.7 | |
| Immigration-related variable | |||||||
| Nativity | |||||||
| US-born | 8.6 | 12.0 | 10.0 | 10.0 | 4.7 | 6.8 | 19.7** |
| Foreign-born | 91.4 | 88.0 | 90.0 | 90.0 | 95.3 | 93.2 | |
| Time in the USA | |||||||
| ≥ 10 years | 62.9 | 53.9 | 62.3 | 51.5 | 51.2 | 73.9 | 52.2*** |
| < 10 years | 37.1 | 46.1 | 37.7 | 48.5 | 48.8 | 26.1 | |
| English proficiency | |||||||
| Proficient | 40.5 | 37.7 | 47.9 | 29.4 | 23.5 | 34.5 | 82.9*** |
| Limited | 59.5 | 62.3 | 52.1 | 70.6 | 76.5 | 65.5 | |
| Health and access variable | |||||||
| Chronic medical condition | |||||||
| None | 67.2 | 71.4 | 74.1 | 67.5 | 74.0 | 66.3 | 10.6 |
| One or more | 32.8 | 28.6 | 25.9 | 32.5 | 26.0 | 33.7 | |
| Self-rated health | |||||||
| Excellent/very good/good | 94.0 | 89.2 | 91.5 | 84.5 | 85.8 | 91.8 | 20.1** |
| Fair/poor | 6.0 | 10.8 | 8.5 | 15.5 | 14.2 | 8.2 | |
| Health insurance | |||||||
| Insured | 84.5 | 86.3 | 97.7 | 79.0 | 79.5 | 90.4 | |
| Not insured | 15.5 | 13.7 | 12.3 | 21.0 | 20.5 | 9.5 | 29.1*** |
| Unmet healthcare needs | 5.2 | 10.4 | 7.2 | 15.8 | 21.0 | 11.2 | 62.7*** |
p < .05
p < .01
p < .001.
Regarding immigration-related characteristics, the human-oriented class had the highest proportion of those who were born in the USA, whereas the resource-scarce class was made up disproportionately of those who were not born in the USA. The health professional-dominant group constituted of more than three quarters of those who lived more than 10 years, and about half of family-dominant and resource-scarce were made up of those who lived in the USA less than 10 years. The majority of the resource-scarce group and of the family-dominant group had limited English proficiency. Additionally, these two groups were more likely to rate their health as fair or poor, lack health insurance, and have unmet health-care needs.
The Effect of the Typology of Health Information Source on Unmet Healthcare Needs
Table 5 presents the results of logistic regression models of unmet healthcare needs. Prior to multivariate analyses, correlations among variables were assessed. All variables were associated in expected directions, and the highest coefficient was observed between nativity and English proficiency (r = .35, p < .001). When the resource-heavy group was used as a reference, the odds of having unmet healthcare needs were 4.13 times higher in the resource-scarce group (95% CI = 1.69 −10.0, p < .01) and 2.94 times higher in the family-dominant group (95% CI = 1.15−7.49, p < .05).
Table 5.
Logistic regression model of the unmet healthcare needs
| Odds ratio (95% confidence interval) | |
|---|---|
| Typology of health information | |
| source | |
| Resource-heavy | 1.0 [reference] |
| Human-oriented | 2.24 (.92, 5.47) |
| Expertise-focused | 1.63 (.66, 3.97) |
| Family-dominant | 2.94 (1.15, 7.49)* |
| Resource-scarce | 4.13 (1.69, 10.0)** |
| Health professional-dominant | 2.17 (.85, 5.56) |
| Demographic variable | |
| Age | |
| 18−39 | 1.0 [reference] |
| 40−59 | .76 (.52, 1.12) |
| 60 and older | .74 (.47, 1.17) |
| Gender | |
| Male | 1.0 [reference] |
| Female | 1.05 (.80, 1.39) |
| Marital status | |
| Married | 1.0 [reference] |
| Not married | 1.19 (.87, 1.62) |
| Education | |
| ≥ High school | 1.0 [reference] |
| < High school | 1.28 (.92, 1.77) |
| Ethnic origin | |
| Chinese | 1.0 [reference] |
| Asian Indian | .54 (.33, .90)* |
| Korean | 1.35 (.91, 2.00) |
| Vietnamese | 1.81 (1.21, 2.69)** |
| Filipino | 1.13 (.64, 1.99) |
| Other Asian | .73 (.35, 1.50) |
| Immigration-related variable | |
| Nativity | |
| US born | 1.0 [reference] |
| Foreign-born | .97 (.54, 1.73) |
| Time in the USA | |
| ≥ 10 years | 1.0 [reference] |
| < 10 years | 1.06 (.75, 1.49) |
| English proficiency | |
| Proficient | 1.0 [reference] |
| Limited | 1.70 (1.14, 2.52)** |
| Health and access variable | |
| Chronic medical condition | |
| None | 1.0 [reference] |
| One or more | 1.81 (1.31, 2.49)*** |
| Self-rated health | |
| Excellent/very good/good | 1.0 [reference] |
| Fair/poor | 1.85 (1.26, 2.72)** |
| Health insurance | |
| Insured | 1.0 [reference] |
| Not insured | 2.47 (1.79, 3.40)*** |
p < .05
p < .01
p < .001.
Among the covariates, significance was observed in ethnic origin, English proficiency, chronic medical conditions, self-rated health, and health insurance. Compared to Chinese, Asian Indians had the reduced odds of having unmet healthcare needs by 46% (95% CI = .33−.90, p < .05) whereas Vietnamese presented an increased odds by 81% (95% CI = 1.21−2.69, p < .01). Having limited English proficiency, one or more chronic medical conditions, fair or poor ratings of health, and no health insurance contributed to increasing the odds of unmet need for healthcare by 1.70−2.47 times.
Discussion
Building upon previous studies on disparities in accessing and obtaining health information and health services among immigrant populations (Islam et al., 2016; Jang et al., 2018; Yoon et al., 2017), the present study explored the typologies of health information source and their predictability to unmet healthcare needs in a sample of Asian Americans. The AAQoL survey, which employed multiple strategies to capture cultural and linguistic diversities of Asian Americans (e.g., use of Asian language versions of the questionnaire, bilingual and bicultural research personnel, and community partnerships), offered an optimal opportunity to explore health information seeking and health service utilization in a sample that reflect the target population’s linguistic and cultural diversities. About half of the AAQoL survey participants responded in their native language versions of the questionnaire, and their rate of unmet healthcare needs (11.5%) was high.
The present sample sought health information from multiple sources across interpersonal networks and Internet-based communication technologies. Family members (51.4%), health professionals (48.9%), and health websites (42.8%) were among the most frequently used sources. These three types have been identified as main sources of health information among immigrants, although preferences were different depending on the target population. According to the study by Yoon and colleagues (2017), which analyzed the first health information source among foreign-born populations, the Internet was the most dominant source of health information (57%), followed by health care providers (22%), and the use of friends and family was minimal (2%−5%). The preferences of family, friends, and social networks as sources of health information were reported from Korean American adults (Kim et al., 2015) and older Chinese immigrant women in Canada (Todd & Hoffman-Goetz, 2011). In addition to these Asian populations, studies with Somali women living in the U.K. (Davies & Bath, 2002) and newly immigrated Latinos in the USA (Courtright, 2005) also reported the importance of interpersonal sources for health information. It seems that interpersonal sources were preferred among those who shared understandings, experiences, cultural norms, and languages (Kim et al., 2015; Todd & Hoffman-Goetz, 2011). The preference of health professionals was observed in a study with Korean American women on cancer-related information seeking behaviors (Oh et al., 2015) where health professionals were found to be the most important, trust-worthy, and credible sources of health information.
As hypothesized, hidden groups varying in their use of health information sources emerged in latent class analyses. The six classes identified included: resource-heavy, human-oriented, expertise-focused, family-dominant, resource-scarce, and health professional-dominant. These identified classes were also uniquely associated with their characteristics in demographic, immigration-related, health and access, and service use variables.
The resource-heavy group demonstrated favorable characteristics in general, being represented by individuals with a higher level of education, English proficiency, and positive ratings of health. Their rate of unmet healthcare needs (5.2%) was the lowest among all groups. The expertise-focused group also presented advantageous characteristics in terms of education and English proficiency. A vast majority (98%) of its members had health insurance, which allowed them to use health professionals as a dominant source of health information.
On the other hand, the resource-scarce group was most dis-advantaged, being represented by those who were less educated and foreign-born and had less years of residence in the USA, limited English proficiency, negative ratings of health, and no health insurance coverage. At 21%, their rate of unmet health-care needs was highest. The family-dominant group shared many of the unfavorable characteristics with the resource-scarce group, but they were disproportionately represented by older adults (≥ 60). Family members may be able to share personal experiences and provide emotional support, but they typically cannot serve as one’s main source of credible medical information (Davies & Bath, 2002; Kim et al., 2015; Todd & Hoffman-Goetz, 2011). Furthermore, it is concerning that members of both resource-scarce and family-dominant groups rarely used reliable information sources such as health professionals (0%) and health websites (0%−3.5%). Findings call attention not only to their limited access to health information but also to the quality and credibility of the obtained information.
In general, personal resources based on education, acculturation, and health and access seem to enable individuals to have a broad range of the sources and be actively engaged in information-seeking behaviors. With regard to ethnicity, the vulnerability of Koreans was evident with their notably high proportion in the resource-scarce group (26.2%) and low proportion in the resource-heavy group (7.8%). Vietnamese were also highly represented in the resource-scarce group (23.7%). These findings are in line with previous studies reporting that Koreans and Vietnamese have high levels of limited English proficiency and barriers to healthcare (Islam et al., 2016; Jang et al., 2018; Pandya et al., 2011). It is interesting to note that Vietnamese were also highly represented in the resource-heavy group (28.4%) and the health-professional dominant group (37.5%). The finding suggests within-group variations and calls attention to the health service environment in ethnic communities.
The results from multivariate models further supported the hypothesis that the groups identified would be different in the estimates of the odds of having an unmet healthcare need. The heightened vulnerabilities of the resource-scarce group and the family-dominant group were confirmed. The groups presented 2.94−4.13 times greater odds of having an unmet healthcare need compared to the resource-heavy group. Findings demonstrate the important contributions of the sources of health information to health service use. Findings also provide practical implications by prioritizing the groups at particular risk in health-related information seeking and utilization of healthcare and suggest ways to approach them.
In efforts to close a gap in healthcare disparities, more attention needs to be paid to health information sources. As a way to meet individuals’ needs for healthcare, enhancing one’s access to diverse and credible sources of health information is recommended. An exposure to various sources and active engagement with health information-seeking behaviors would enable individuals to have a healthy life style, proper knowledge and use of health services, and satisfaction with the services used (Clayman et al., 2010; Richardson et al., 2012). Given the vulnerability of the resource-scarce and family-oriented groups, their member-ship characteristics shed light on whom to be prioritized in intervention efforts. Attention is needed for individuals who lack personal resources in terms of education, acculturation, and health insurance. Efforts may include offering health education programs tailored to education and acculturation levels. It is recommended to use simple content that is understandable by persons with low literacy, evaluate cultural relevance of the materials, and translate the information into the several Asian languages. Promotion of the access and utilization of online health information would be another strategy. With the advancement of communication technologies, online sources are anticipated to serve as an important means of obtaining health information, and such resource and benefit should be shared across diverse populations.
Several limitations to the present study should be noted. Given the non-representative and regionally-defined nature of the sample, caution should be exercised in generalizing the findings to the larger population of Asian Americans. Future studies should revisit the topic with a representative sample on a national level and consider geographic differences in the sources of health information and health services. For example, the size of ethnic communities and availability of healthcare providers who offer culturally and linguistically appropriate services (CLAS) in the area may play a critical role in determining ethnic minorities’ access to and use of health information and health services (Jang et al., 2018). It should also be noted that the measure of health information source in the present study only asked the participants to report whether they had used each of the sources in the list on a yes/no format. Future endeavors should include exploring other aspects of health information sources such as the frequency of use, qualitative assessment of the source (e.g., perceived credibility and satisfaction), and language concordance with the source.
Despite these limitations, our findings provide implications for interventions with respect to subgroups to be prioritized and areas to be targeted in efforts to promote access and acquisition of health information and health services in Asian Americans. Considering that the most vulnerable groups have limited access to the most reliable sources such as health professionals, efforts should be made to connect those individuals with credible sources of health information.
Acknowledgments
Funding
This work was supported by the City of Austin’s Asian American Quality of Life Initiative [grant number 26-8275-39 to PI: Yuri Jang] and the Oak Ridge Associated Universities (ORAU) Travel Grant [grant number 201703479-001 to PI: Yuri Jang].
Footnotes
Color versions of one or more of the figures in the article can be found online at www.tandfonline.com/uhcm.
Disclosure
The authors have reported no conflicts of interest.
References
- Beiser M, & Edwards RG (1994). Mental health of immigrants and refugees. New Directions for Mental Health Services, 61, 73–86. doi: 10.1002/yd.23319946110 [DOI] [PubMed] [Google Scholar]
- Chen CJ, Kendall J, & Shyu YIL (2010). Grabbing the rice straw: Health information seeking in Chinese immigrants in the United States. Clinical Nursing Research, 19(4), 335–353. doi: 10.1177/1054773810372542 [DOI] [PubMed] [Google Scholar]
- Chevarley FM (2010). Percentage of persons unable to get or delayed in getting needed medical care, dental care, or prescription medicines: United States, 2007 (Medical Expenditure Panel Survey statistical brief No. 282) Rockville, MD: Agency for Healthcare Research and Quality; Retrieved from http://meps.ahrq.gov/mepsweb/data_files/publications/st282/stat282.pdf [Google Scholar]
- City of Austin. (2017). Asian American quality of life Retrieved from http://austintexas.gov/department/documents-3
- Clayman ML, Manganello JA, Viswanath K, Hesse BW, & Arora NK (2010). Providing health messages to Hispanics/Latinos: Understanding the importance of language, trust in health information sources, and media use. Journal of Health Communication, 15(sup3), 252–263. doi: 10.1080/10810730.2010.522697 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtright C (2004). Health information-seeking among Latino newcomers: An exploratory study. Information Research, 10(2), 224 Retrieved from http://InformationR.net/ir/10-2/paper224.html [Google Scholar]
- Davies MM, & Bath PA (2002). Interpersonal sources of health and maternity information for Somali women living in the UK: Information seeking and evaluation. Journal of Documentation, 58(3), 302–318. doi: 10.1108/00220410210425629 [DOI] [Google Scholar]
- Islam NS, Patel S, Wyatt LC, Sim SC, Mukherjee-Ratnam R, Chun K, … Kwon SC (2016). Sources of health information among select Asian American immigrant groups in New York City. Health Communication, 31(2), 207–216. doi: 10.1080/10410236.2014.944332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang Y, Park NS, Yoon H, Huang Y, Rhee M, Chiriboga DA, & Kim MT (2018). The risk typology of healthcare access and its association with unmet healthcare needs in Asian Americans. Health and Social Care in the Community, 26(1), 72–79. doi: 10.1111/hsc.12463 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim W, Kreps GL, & Shin CN (2015). The role of social support and social networks in health information–Seeking behavior among Korean Americans: A qualitative study. International Journal for Equity in Health, 14(1), 40. doi: 10.1186/s12939-015-0169-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén BO (2001). Latent variable mixture modeling. In Marcoulides GA & Schumacker RE (Eds.), New developments and techniques in structural equation modeling (2nd ed., pp. 1–33). Mahwah, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Oh KM, Jun J, Zhao X, Kreps GL, & Lee EE (2015). Cancer information seeking behaviors of Korean American women: A mixed-methods study using surveys and focus group interviews. Journal of Health Communication, 20(10), 1143–1154. doi: 10.1080/10810730.2015.1018578 [DOI] [PubMed] [Google Scholar]
- Pandya C, McHugh M, & Batalova J (2011). Limited English proficient individuals in the United States: Number, share, growth, and linguistic diversity Washington, DC: Migration Policy Institute. [Google Scholar]
- Richardson A, Allen JA, Xiao H, & Vallone D (2012). Effects of race/ethnicity and socioeconomic status on health information-seeking, confidence, and trust. Journal of Health Care for the Poor and Underserved, 23(4), 1477–1493. doi: 10.1353/hpu.2012.0181 [DOI] [PubMed] [Google Scholar]
- Ruppel EK, & Rains SA (2012). Information sources and the health information-seeking process: An application and extension of channel complementarity theory. Communication Monographs, 79(3), 385–405. doi: 10.1080/03637751.2012.697627 [DOI] [Google Scholar]
- Shi L, Lebrun LA, & Tsai J (2010). Assessing the impact of the health center growth initiative on health center patients. Public Health Reports, 125(2), 258–266. doi: 10.1177/003335491012500514 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shi L, & Stevens GD (2005). Vulnerability and unmet health care needs: The influence of multiple risk factors. Journal of General Internal Medicine, 20(2), 148–154. doi: 10.1111/j.1525-1497.2005.40136.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smedley BD, Stith AY, & Nelson AR (Eds.). (2002). Unequal treatment: Confronting racial and ethnic disparities in health care Washington, DC: National Academies Press. [PubMed] [Google Scholar]
- Thorpe JM, Thorpe CT, Kennelty KA, & Pandhi N (2011). Patterns of perceived barriers to medical care in older adults: A latent class analysis. BMC Health Services Research, 11, 181. doi: 10.1186/1472-6963-11-181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Todd L, & Hoffman-Goetz L (2011). A qualitative study of cancer information seeking among English-as-a-second-Language older Chinese immigrant women to Canada: Sources, barriers, and strategies. Journal of Cancer Education, 26(2), 333–340. doi: 10.1007/s13187-010-0174-y [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. (2016). A nation free of disparities in health and health care Retrieved from http://minority-health.hhs.gov/npa/files/plans/hhs/hhs_plan_complete.pdf
- Wang W, & Yu N (2015). Coping with a new health culture: Acculturation and online health information seeking among Chinese immigrants in the United States. Journal of Immigrant and Minority Health, 17(5), 1427–1435. doi: 10.1007/s10903-014-0106-8 [DOI] [PubMed] [Google Scholar]
- Yoon J (2014). Health information seeking of foreign-born population in U.S. Ewha Journal of Social Sciences, 30(2), Available at SSRN https://ssrn.com/abstract=2577607 [Google Scholar]
- Yoon J, Huang H, & Kim S (2017). Trends in health information-seeking behaviour in the U.S. foreign-born population based on the Health Information National Trends Survey, 2005–2014. Information Research, 22(3), paper 760. Retrieved from http://InformationR.net/ir/22-3/paper760.html Retrieved from [Google Scholar]
- Zhao X (2010). Cancer information disparities between US-and foreign-born populations. Journal of Health Communication, 15(sup3), 5–21. doi: 10.1080/10810730.2010.522688 [DOI] [PubMed] [Google Scholar]