

Abstract
Background Esophageal stricture following endoscopic submucosal dissection (ESD) for superficial esophageal squamous cell cancer (SESCC) has been associated with wide mucosal defects greater than three-quarters of the luminal circumference. Some patients developed dysphagia and required repeated endoscopic balloon dilation even after steroid therapy. As iodine staining clearly visualized the margin of SESCC, we made a longitudinal mucosal incision close to the margin of the lesion to avoid a mucosal defect involving over three-quarters of the luminal circumference for large lesions. This retrospective study aimed to clarify the clinical feasibility of ESD with minimum lateral margin of SESCC.
Patients and methods Between 2005 and 2013, 94 patients with 94 initial SESCCs had lesions greater than half of the luminal circumference. Of those, 70 patients with 70 SESCCs had achieved endoscopic clearance for the initial SESCC. In this study, endoscopic clearance was defined as en bloc resection of SESCC histologically confined to the mucosa without lymphovascular invasion and with a free deep margin regardless of the lateral margin. This study evaluated the short- and long-term outcomes in patients undergoing endoscopic clearance.
Results In total, 61.4 % (43/70) of the patients had mucosal defects involving over three-quarters of the luminal circumference and 38.5 % (27/70) had a positive or indeterminate lateral margin. However, there was no local or nodal recurrence during the median follow-up period of 3.8 years; the 3-year overall survival rate was 98.5 % and the 3-year disease-free survival rate was 100 %.
Conclusion Using our institutions’ strategy, ESD for SESCCs with minimum lateral margins was oncologically acceptable; this approach could reduce the known risk factor of post-ESD stricture.
Introduction
Endoscopic resection (ER) is accepted as an effective, minimally invasive treatment for early superficial esophageal squamous cell cancer (SESCC) 1 2 3 4 . Although extensive ER has become more common as endoscopic techniques by piecemeal endoscopic mucosal resection (EMR) have developed, piecemeal resection is a significant risk factor for local recurrence after ER 5 6 . Endoscopic submucosal dissection (ESD) has advanced for en bloc resection regardless of tumor size or tumor location 7 . Furthermore, ESD for SESCC yields favorable long-term outcomes 8 9 .
However, when resecting large lesions, the frequency of esophageal strictures after ESD has increased 10 11 . Esophageal strictures following ER are associated with wide mucosal defects greater than three-quarters of the luminal circumference 12 . When the mucosal defect exceeds three-quarters of the luminal circumference, stricture occurrence is prevalent in 68 – 100 % cases 10 11 12 13 . Although oral prednisolone or locoregional steroid injections have shown promising results for the prevention of esophageal strictures following ESD 14 15 16 , some patients may still develop dysphagia and require repeated endoscopic balloon dilation even after steroid therapy 17 .
Markings for ESD are generally made 5 mm away from the borders of the lesion 18 . However, iodine staining enables clear visualization of the SESCC margins 19 , so we applied markings with energy devices just on the border and commenced the incision just outside the applied marks so as to minimize luminal defects for large SESCC cases involving over three-quarters of the luminal circumference. This retrospective study aims to clarify the clinical feasibility of ESD with minimum lateral margin of SESCC.
Methods
Patients
A total of 268 patients with 289 esophageal lesions consecutively underwent ESD of SESCC at our institution between 2005 and 2013. Endoscopic resection was indicated for histologically proven squamous cell carcinoma on biopsy and was not performed in patients with apparent massive submucosal invasion or nodal metastasis. The depth of invasion was estimated by white-light endoscopy, and magnified narrow-band imaging and chromoendoscopy with iodine staining. Endoscopic ultrasonography was also performed to determine the depth of invasion as necessary. Mizuta et al. 10 reported that a lesion more than half of the luminal circumference was closely associated with an ESD-induced mucosal defect involving over three-quarters of the luminal circumference and was considered to be an independent risk factor for esophageal stricture. Thus, amongst those patients, we investigated those who had a lesion more than half of the luminal circumference and met endoscopic clearance for SESCC and who were followed up without any additional treatment. In this study, endoscopic clearance was defined as en bloc resection of SESCC histologically confined to the mucosa without lymphovascular invasion and with a free deep margin, regardless of the lateral margin. In reference to the Guidelines for Diagnosis and Treatment of Carcinoma of the Esophagus edited by the Japan Esophageal Society, those lesions confined to the epithelium (EP) and lamina propria mucosae (LPM) have almost no risk of metastasis; lesions limited to the muscularis mucosae (MM) without lymphovascular invasion also have a very low risk of metastasis 20 . At our institution during the study period, a SESCC involving the whole circumference was mainly treated with chemoradiotherapy rather than ESD.
ESD procedure
The ESD procedure was performed by expert endoscopists skilled in ESD or trainees with support from expert endoscopists. Trainees were defined as those who had limited experience in performing esophageal ESD procedures (30 cases or less), and expert endoscopists had experienced performing more than 30 esophageal ESD procedures 21 .
A dual knife (KD-650; Olympus, Tokyo) was used to make markings close to the margins of the lesion. The dual knife and an insulation-tipped (IT) knife nano (KD-612; Olympus) were used for mucosal incision and submucosal dissection. Intraoperative bleeding was treated using a hemostatic forceps (Coagrasper, FD-411 QR; Olympus). ESD was performed with the patient under deep sedation using a combination of midazolam or propofol with pentazocine. The ESD strategy for esophageal lesions with minimum lateral margins comprised these three steps: 1) chromoendoscopy with iodine staining to clearly visualize the margin of SESCC; 2) circumferential marking close to the margins of the lesion, and 3) mucosal incision close to the marking, or on the marking in some cases ( Fig. 1 ). This strategy was applied to lesions more than half of the circumference that were closely associated with a mucosal defect involving over three-quarters of the luminal circumference.
Fig. 1.
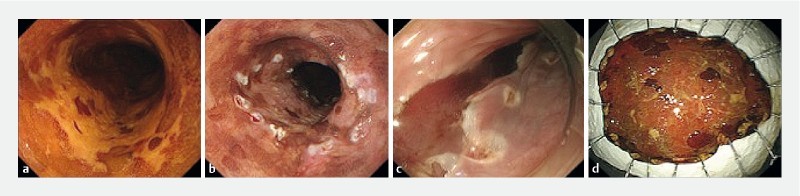
Endoscopic submucosal dissection (ESD) strategy for esophageal lesions with minimum lateral margins. a Chromoendoscopy with iodine staining clearly visualized a superficial esophageal squamous cell carcinoma (SESCC). b Markings close to the margins. c Mucosal incision close to the marking. d Minimize the luminal circumference for large SESCC to avoid stenosis from excessive resection.
Stricture prevention
In this study, until 2010, prophylactic endoscopic balloon dilation (EBD) was performed to avoid esophageal stricture following widespread endoscopic resection 22 . Oral prednisolone and/or locoregional triamcinolone injection were introduced in 2011 based on the discretion of the endoscopist.
Histology
After fixing in 10 % formalin and serial sectioning at 2-mm intervals, the resected specimens were assessed using histological mapping. Expert pathologists were engaged to assess the macroscopic appearance, tumor size, depth of invasion, lymphatic and vascular involvement, and lateral and vertical margins, with reference to the Japanese Classification of Esophageal Carcinoma 23 24 . Lymphovascular involvement was first determined using hematoxylin and eosin (HE)-stained sections; when the diagnosis of lymphovascular involvement was inconclusive using HE-stained sections, immunohistochemistry was also performed with the monoclonal antibody D2-40 and/or Victoria blue or Elastica van Gieson staining.
Follow-up after endoscopic clearance
All patients who achieved endoscopic clearance generally underwent esophagogastroduodenoscopy (EGD) surveillance on an annual or biannual basis. In addition, a computed tomography (CT) scan was performed every 6 months or 1 year to identify lymph node and distant metastases in patients with muscularis mucosa invasion. A local recurrence was defined as an iodine-unstained area detected adjacent to an ESD scar and cancer cells were verified histologically in a biopsy specimen. Metachronous esophageal squamous cell cancer (ESCC) was defined as ESCC other than local recurrence detected in surveillance EGD.
Assessment
This study evaluated short- and long-term outcomes in cases with a lesion more than half of the circumference undergoing endoscopic clearance.
In this study, we investigated alcohol consumption, smoking habits, and grade of Lugol-voiding lesion (LVL) as patient background. LVL was graded according to the number of LVLs per endoscopic view (A, no lesions; B, 1 – 9 lesions; C, ≥ 10 lesions) 25 .
Technical results, adverse events, and histopathological results were assessed to determine short-term outcomes. Long-term outcomes included local recurrence, lymph node metastasis, distant metastases, 3-year cumulative incidence of metachronous ESCC, 3-year overall survival (OS), and 3-year disease-free survival (DFS) after endoscopic clearance.
Statistical analysis
All statistical analyses were performed with EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria) 26 . Continuous variables were compared using the Mann-Whitney U test and categorical variables were compared using the χ 2 test or Fisher’s exact test as appropriate. OS and DFS survival rates were calculated by Kaplan-Meier analysis. OS was measured from the date of ESD to the date of death or the date of the latest confirmation of survival. DFS was measured from the date of ESD to the date of death from ESSC.
Results
Amongst 268 consecutive patients with 289 SESCCs, 94 patients with 94 initial SESCCs had lesions more than half of the circumference. Of those, 24 patients with 24 SESCCs were excluded as 13 patients had pathological submucosal invasion, seven patients had mucosal cancer with lymphovascular invasion, and four patients underwent additional chemoradiotherapy for muscularis mucosae lesions. The remaining 70 patients with 70 SESCCs had achieved endoscopic clearance for initial SESCC and were followed up without any additional treatment ( Fig. 2 ).
Fig. 2.
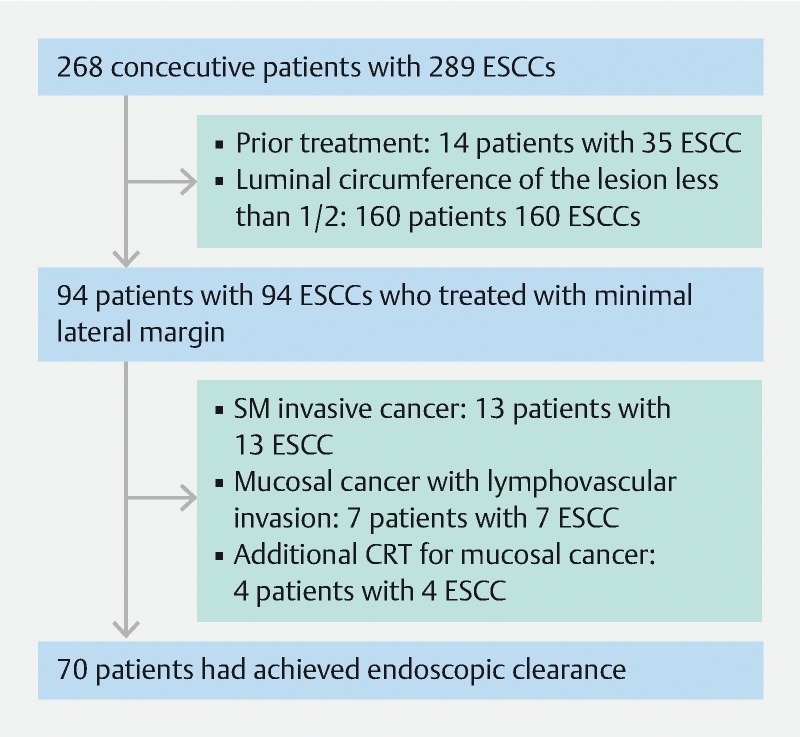
In total, 94 patients with 94 superficial esophageal squamous cell carcinoma (SESCCs) had lesions more than half of the circumference. Of those, we investigated 70 patients who met endoscopic clearance for initial SESCC and who were followed up without any additional treatment.
The male/female ratio was 6.8:1 (61 men/9 women), and median age was 69 years (range, 50 – 86 years); 78.6 % of patients had a current or previous habit of alcohol consumption and 68.6 % of patients were smokers; 88.6 % of patients had multiple dysplastic lesions. More than half of the lesions (57.1 %) were located in the middle esophagus. The median tumor size was 35 mm (range, 20 – 85). With regard to depth of invasion, 4.3 % were EP, 77.1 % were LPM, and 18.6 % of lesions had invaded to the depth of the MM ( Table 1 ). All lesions had achieved en bloc resection. Complete curative resection with a negative lateral margin was achieved in 61.4 % (43/70) of patients and with a positive lateral margin in 38.6 % (27/70) of patients. The median procedure time was 120 minutes (range, 50 – 570). The stricture rate was 35.7 % (25/70). Twelve cases were orally administered prednisolone and five patients underwent locoregional triamcinolone injection; 57.1 % (40/70) of patients had a mucosal defect involving over three-quarters of the luminal circumference. Of those, stenosis was seen in 16 of 25 cases (64 %) in the group who underwent preemptive EBD and in 5 of 15 cases (33 %) in the group who underwent steroid treatment ( Table 2 ). In terms of lateral margin, tumor size was significantly larger in the positive lateral margin group than in the negative lateral margin group. However, there was no statistically significant difference between the two groups in the rate of cases with a circumferential mucosal defect greater than three-quarters of the circumference ( Table 3 ).
Table 1. Patients (n = 70) and tumor characteristics.
| Age, median (range), years | 69 (50 – 86) |
| Sex | |
|
61 |
|
9 |
| Alcohol consumption status | |
|
15 |
|
55 |
| Cigarette smoking status | |
|
22 |
|
48 |
| Location | |
|
6 |
|
40 |
|
24 |
| Tumor depth | |
|
3 |
|
54 |
|
13 |
| LVL grade | |
|
8 |
|
33 |
|
29 |
| Tumor size, median (range), mm | 35 (20 – 85) |
EP, epithelium; LPM, lamina propria mucosae; MM, muscularis mucosae; LVL, Lugol-voiding lesion.
Table 2. Short-term outcomes for patients in this study (n = 70).
| En bloc resection, % | 100 |
| Lateral margin | |
|
43 |
|
27 |
| Procedure time, median (range), min | 120 (50 – 570) |
| Endoscopist | |
|
55 |
|
15 |
| Mucosal defect greater than 3/4 of luminal circumference, % | 57.1 (40/70) |
| Resection size, median (range), mm | 45 (22 – 110) |
| Steroid treatment | |
|
53 |
|
12 |
|
5 |
| Stricture, % | 35.7 (25/70) |
| Perforation, % | 2.9 (2/70) |
Table 3. Comparison of cases with a negative lateral margin vs positive or indeterminate lateral margin.
| Negative lateral margin | Positive or indeterminate lateral margin | P value | |
| Rate of cases with a mucosal defect greater than 3/4 of the luminal circumference, % | 51.2 (21/41) | 65.5 (19/29) | 0.3 |
| Tumor size, median (range), mm | 35 (20 – 55) | 50 (20 – 85) | < 0.01 |
During a median follow-up period of 3.8 years, there was no local or nodal recurrence in the 70 patients. The cumulative incidence of metachronous ESCC at 3 years was 11.8 % ( Fig. 3 ). LVL grade was associated with progressive increases in the 3-year cumulative incidence of metachronous ESCCs (0.0 %, 6.6 %, and 23.4 %, respectively) ( Fig. 4 ). The 3-year OS rate was 98.5 % ( Fig. 5 ) and the 3-year DFS rate was 100 %, respectively.
Fig. 3.
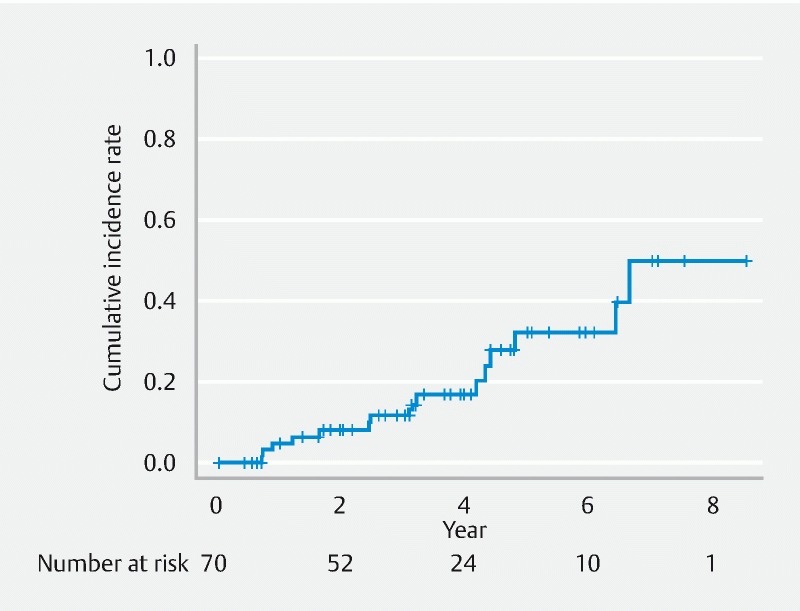
Cumulative incidence of metachronous esophageal squamous cell carcinoma (ESSC) in all patients.
Fig. 4.
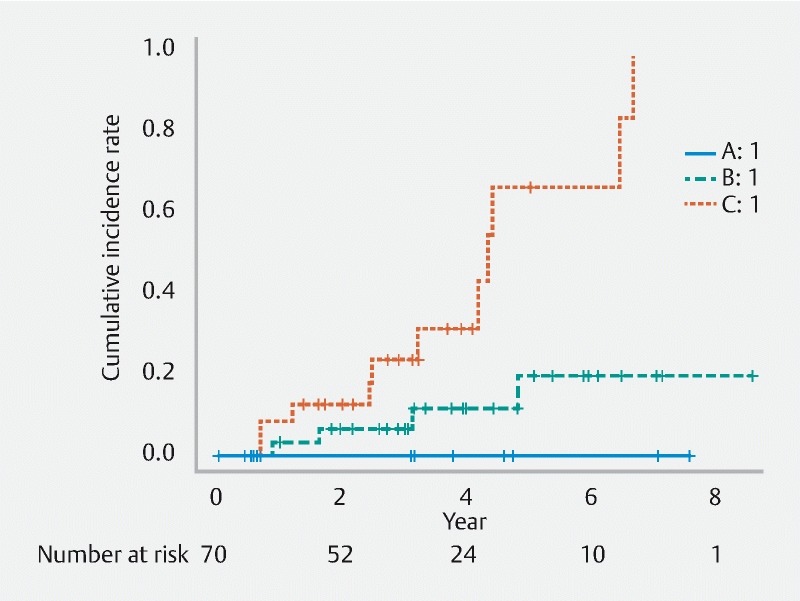
Cumulative incidence of metachronous esophageal squamous cell carcinoma (ESSC) according to Lugol-voiding lesion (LVL) grade. LVL was graded according to the number of LVLs per endoscopic view (A, no lesions; B, 1 – 9 lesions; C, ≥ 10 lesions).
Fig. 5.
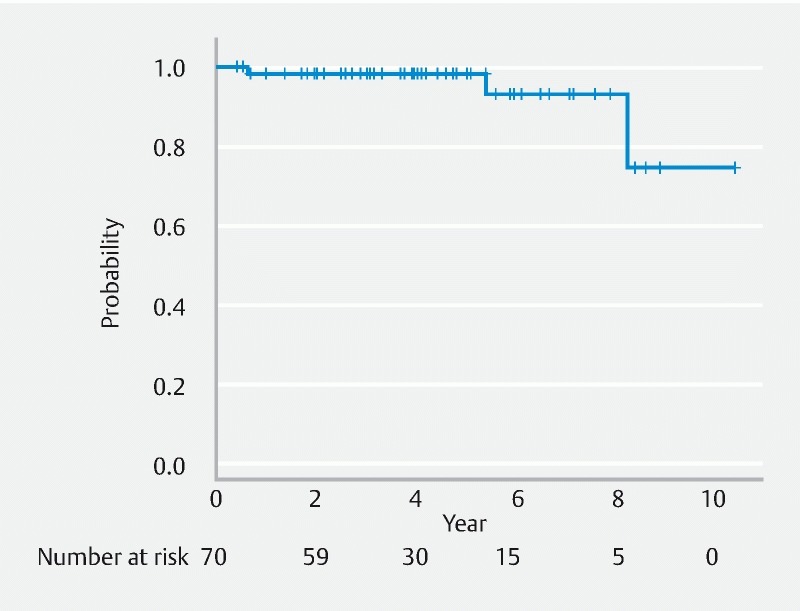
Kaplan-Meier curve of the overall survival rate after endoscopic submucosal dissection (ESD).
Discussion
Chromoendoscopy with iodine staining has been reported to be useful in identifying the margins of SESCC 19 27 . It allows us to make markings close to the margins of the lesion so as to avoid excessive resection. The strength of this study was that no patient developed local recurrence or nodal metastasis in ESD with minimum lateral margins, and this suggested the SESCCs that achieved endoscopic clearance could be clinically and oncologically followed as R0 resections.
Esophageal stricture following ESD has been associated with wide mucosal defects greater than three-quarters of the luminal circumference 12 . Mizuta et al. reported that many cases of lesions greater than half of the circumference were the result of a mucosal defect involving over three-quarters of the luminal circumference 10 . Because the minimum lateral margin strategy is a method of reducing the risk of mucosal defects involving over three-quarters of the luminal circumference, we included patients who had a lesion involving more than half of the luminal circumference. This study demonstrated that mucosal defects involving over three-quarters of the luminal circumference were seen in only 57.1 % of cases that had a lesion greater than half of the circumference. The proportion of cases with a mucosal defect involving over three-quarters of the luminal circumference was lower than that in standard esophageal ESD 10 .
Locoregional steroid injection and oral prednisolone could reduce the stenosis rate of lesions with wide mucosal defects greater than three-quarters of the luminal circumference to 10.0 – 62.5 % and 5.3 – 50 %, respectively 14 15 16 28 . Steroid treatments were demonstrated to have a significant effect in preventing stricture. However, locoregional steroid injection can cause delayed perforation, and oral prednisolone can cause systemic adverse effects, including diabetes, peptic ulceration, osteoporosis, and increased susceptibility to infection 29 30 . Furthermore, some patients with wide mucosal defects greater than three-quarters of the luminal circumference failed to avoid esophageal stricture even with steroid treatment, particularly in those with mucosal defects involving the whole circumference 31 . Therefore, it is important to reduce lesions with a mucosal defect involving over three-quarters of the luminal circumference as much as possible using the minimum lateral margin strategy. We believe our strategy could reduce the risk of extensive ESD and thus minimize preventive steroid administration, which was generally unnecessary for lesions which did not have the risk factor of post-ESD stricture.
En bloc curative resection is considered to be the ideal for both EMR and ESD treatment because it provides an accurate histological assessment and reduces the risk of local recurrence 9 . Ishihara et al. evaluated factors associated with local recurrence following endoscopic resection of SESCC and concluded that multiple piecemeal resection (more than five pieces) was a significant risk factor for local recurrence and that there were few recurrences if en bloc resection could be achieved 6 . In terms of lateral margin, a positive lateral margin tended to occur in large lesions. Although the positive lateral margin rate was 38.6 % in this study, there was no local recurrence in those who achieved endoscopic clearance. Nagami et al. also reported that the rate of en bloc resection with tumor-free margins was 90.4 % and no local recurrence was encountered regardless of tumor margins in ESD 32 . The results of previous reports support the concept of endoscopic clearance but did not support piecemeal resection.
Similar conclusions have been reported in our institution for large colorectal tumors 33 . Electrocautery devices might damage the squamous epithelium on the lateral margin of the lesion, and therefore the pathologists might be unable to evaluate whether or not the margins of the lesion were neoplastic. Since squamous cell carcinoma has a clear boundary with iodine staining, the potential for neoplastic tissue to remain within the lumen is believed to be very low. Furthermore, Matsuda et al. reported squamous cell carcinoma invading under the epithelium in only 0.67 % of surgically excised specimens 34 . There were very few cases of squamous cell carcinomas invading under the epithelium and this result also supported our strategy of minimum lateral margins for SESCC.
The cumulative recurrence rate was consistent with previous reports, which showed that multiple dysplastic lesions in the esophagus increase the risk of multiple ESCCs 25 . Surveillance endoscopy should be performed focusing on the early detection of metachronous SESCC rather than local recurrence after endoscopic clearance.
This study had some limitations. First, this was a single center, retrospective study. Second, it is difficult to conclude that the endoscopic clearance strategy reported in this study directly resulted in the prevention of stricture formation. Prophylactic steroid treatment was introduced in 2011 to avoid post-ESD esophageal stricture and it became the current standard of care for wide mucosal defects that were greater than three-quarters of the luminal circumference. The steroid treatment could contribute to stricture prevention in our study. Further prospective study is warranted to investigate the efficacy of ESD with minimum lateral margins.
In conclusion, ESD for SESCCs with minimum lateral margins using our institutions’ strategy was oncologically acceptable and this approach could reduce the known risk factor of post-ESD stricture.
Acknowledgments
The research team would like to thank Mr Saswata Banerjee (Consultant Colorectal Surgeon, Barking, Havering and Redbridge University Hospitals NHS Trust, London, UK) for his kind support for this article. In addition, part of this work was supported by the National Cancer Center Research and Development Fund (25-A-12, 28-K-1, and 29-A-12).
Footnotes
Competing interests None
References
- 1.Shimizu Y, Takahashi M, Yoshida T et al. Endoscopic resection is the criterion standard of treatment for patients with early squamous cell neoplasia of the esophagus. Gastrointest Endosc. 2012;76:464–465. doi: 10.1016/j.gie.2012.02.007. [DOI] [PubMed] [Google Scholar]
- 2.Inoue H, Tani M, Nagai K et al. Treatment of esophageal and gastric tumors. Endoscopy. 1999;31:47–55. doi: 10.1055/s-1999-13647. [DOI] [PubMed] [Google Scholar]
- 3.di Pietro M, Canto M I, Fitzgerald R C. Endoscopic management of early adenocarcinoma and squamous cell carcinoma of the esophagus: Screening, diagnosis, and therapy. Gastroenterology. 2018;154:421–436. doi: 10.1053/j.gastro.2017.07.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Katada C, Muto M, Momma K et al. Clinical outcome after endoscopic mucosal resection for esophageal squamous cell carcinoma invading the muscularis mucosae – a multicenter retrospective cohort study. Endoscopy. 2007;39:779–783. doi: 10.1055/s-2007-966761. [DOI] [PubMed] [Google Scholar]
- 5.Katada C, Muto M, Manabe T et al. Local recurrence of squamous-cell carcinoma of the esophagus after EMR. Gastrointest Endosc. 2005;61:219–225. doi: 10.1016/s0016-5107(04)02756-7. [DOI] [PubMed] [Google Scholar]
- 6.Ishihara R, Iishi H, Takeuchi Y et al. Local recurrence of large squamous-cell carcinoma of the esophagus after endoscopic resection. Gastrointest Endosc. 2007;67:799–804. doi: 10.1016/j.gie.2007.08.018. [DOI] [PubMed] [Google Scholar]
- 7.Ishihara R, Iishi H, Uedo N et al. Comparison of EMR and endoscopic submucosal dissection for en bloc resection of early esophageal cancers in Japan. Gastrointest Endosc. 2008;68:1066–1072. doi: 10.1016/j.gie.2008.03.1114. [DOI] [PubMed] [Google Scholar]
- 8.Ono S, Fujishiro M, Niimi K et al. Long-term outcomes of endoscopic submucosal dissection for superficial esophageal squamous cell neoplasms. Gastrointest Endosc. 2009;70:860–866. doi: 10.1016/j.gie.2009.04.044. [DOI] [PubMed] [Google Scholar]
- 9.Takahashi H, Arimura Y, Masao H et al. Endoscopic submucosal dissection is superior to conventional endoscopic resection as a curative treatment for early squamous cell carcinoma of the esophagus (with video) Gastrointest Endosc. 2010;72:255–264. doi: 10.1016/j.gie.2010.02.040. [DOI] [PubMed] [Google Scholar]
- 10.Mizuta H, Nishimori I, Kuratani Y et al. Predictive factors for esophageal stenosis after endoscopic submucosal dissection for superficial esophageal cancer. Dis Esophagus. 2009;22:626–631. doi: 10.1111/j.1442-2050.2009.00954.x. [DOI] [PubMed] [Google Scholar]
- 11.Ono S, Fujishiro M, Niimi K et al. Predictors of postoperative stricture after esophageal endoscopic submucosal dissection for superficial squamous cell neoplasms. Endoscopy. 2009;41:661–665. doi: 10.1055/s-0029-1214867. [DOI] [PubMed] [Google Scholar]
- 12.Katada C, Muto M, Manabe T et al. Esophageal stenosis after endoscopic mucosal resection of superficial esophageal lesions. Gastrointest Endosc. 2003;57:165–169. doi: 10.1067/mge.2003.73. [DOI] [PubMed] [Google Scholar]
- 13.Shi Q, Ju H, Yao L-Q et al. Risk factors for postoperative stricture after endoscopic submucosal dissection for superficial esophageal carcinoma. Endoscopy. 2014;46:640–644. doi: 10.1055/s-0034-1365648. [DOI] [PubMed] [Google Scholar]
- 14.Yamaguchi N, Isomoto H, Nakayama T et al. Usefulness of oral prednisolone in the treatment of esophageal stricture after endoscopic submucosal dissection for superficial esophageal squamous cell carcinoma. Gastrointest Endosc. 2011;73:1115–1121. doi: 10.1016/j.gie.2011.02.005. [DOI] [PubMed] [Google Scholar]
- 15.Hashimoto S, Kobayashi M, Takeuchi M et al. The efficacy of endoscopic triamcinolone injection for the prevention of esophageal stricture after endoscopic submucosal dissection. Gastrointest Endosc. 2011;74:1389–1393. doi: 10.1016/j.gie.2011.07.070. [DOI] [PubMed] [Google Scholar]
- 16.Hanaoka N, Ishihara R, Takeuchi Y et al. Intralesional steroid injection to prevent stricture after endoscopic submucosal dissection for esophageal cancer: a controlled prospective study. Endoscopy. 2012;44:1007–1011. doi: 10.1055/s-0032-1310107. [DOI] [PubMed] [Google Scholar]
- 17.Hanaoka N, Ishihara R, Uedo N et al. Refractory strictures despite steroid injection after esophageal endoscopic resection. Endosc Int Open. 2016;4:E354–359. doi: 10.1055/s-0042-100903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bhatt A, Abe S, Kumaravel A et al. Indications and techniques for endoscopic submucosal dissection. Am J Gastroenterol. 2015;110:784–791. doi: 10.1038/ajg.2014.425. [DOI] [PubMed] [Google Scholar]
- 19.Shiozaki H, Tahara H, Kobayashi K et al. Endoscopic screening of early esophageal cancer with the Lugol dye method in patients with head and neck cancers. Cancer. 1990;66:2068–2071. doi: 10.1002/1097-0142(19901115)66:10<2068::aid-cncr2820661005>3.0.co;2-w. [DOI] [PubMed] [Google Scholar]
- 20.Kuwano H, Nishimura Y, Oyama T et al. Guidelines for Diagnosis and Treatment of Carcinoma of the Esophagus April 2012 edited by the Japan Esophageal Society. Esophagus. 2015;12:1–30. doi: 10.1007/s10388-014-0465-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ohata K, Fu K, Sakai E et al. Esophageal endoscopic submucosal dissection assisted by an overtube with a traction forceps: An animal study. Gastroenterol Res Pract. 2016;2016:3.186168E6. doi: 10.1155/2016/3186168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ezoe Y, Muto M, Horimatsu T et al. Efficacy of preventive endoscopic balloon dilation for esophageal stricture after endoscopic resection. J Clin Gastroenterol. 2011;45:222–227. doi: 10.1097/MCG.0b013e3181f39f4e. [DOI] [PubMed] [Google Scholar]
- 23.Japan Esophageal Society . Japanese Classification of Esophageal Cancer, 11th Edition: part I. Esophagus. 2017;14:1–36. doi: 10.1007/s10388-016-0551-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Japan Esophageal Society . Japanese Classification of Esophageal Cancer, 11th Edition: part II and III. Esophagus. 2017;14:37–65. doi: 10.1007/s10388-016-0556-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Katada C, Yokoyama T, Yano T et al. Alcohol consumption and multiple dysplastic lesions increase risk of squamous cell carcinoma in the esophagus, head, and neck. Gastroenterology. 2016;151:860–867. doi: 10.1053/j.gastro.2016.07.040. [DOI] [PubMed] [Google Scholar]
- 26.Kanda Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013;48:452–458. doi: 10.1038/bmt.2012.244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ban S, Toyonaga A, Harada H et al. Iodine staining for early endoscopic detection of esophageal cancer in alcoholics. Endoscopy. 1998;30:253–257. doi: 10.1055/s-2007-1001251. [DOI] [PubMed] [Google Scholar]
- 28.Abe S, Iyer P G, Oda I et al. Approaches for stricture prevention after esophageal endoscopic resection. Gastrointest Endosc. 2017;86:779–791. doi: 10.1016/j.gie.2017.06.025. [DOI] [PubMed] [Google Scholar]
- 29.Matsuda Y, Kataoka N, Yamaguchi T et al. Delayed esophageal perforation occurring with endoscopic submucosal dissection: A report of two cases. World J Gastrointest Surg. 2015;7:123–127. doi: 10.4240/wjgs.v7.i7.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ishida T, Morita Y, Hoshi N et al. Disseminated nocardiosis during systemic steroid therapy for the prevention of esophageal stricture after endoscopic submucosal dissection. Dig Endosc. 2015;27:388–391. doi: 10.1111/den.12317. [DOI] [PubMed] [Google Scholar]
- 31.Kadota T, Yano T, Kato T et al. Prophylactic steroid administration for strictures after endoscopic resection of large superficial esophageal squamous cell carcinoma. Endosc Int Open. 2016;4:E1267–E1274. doi: 10.1055/s-0042-118291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Nagami Y, Ominami M, Shiba M et al. The five-year survival rate after endoscopic submucosal dissection for superficial esophageal squamous cell neoplasia. Dig Liver Dis. 2017;49:427–433. doi: 10.1016/j.dld.2016.12.009. [DOI] [PubMed] [Google Scholar]
- 33.Makazu M, Sakamoto T, So E et al. Relationship between indeterminate or positive lateral margin and local recurrence after endoscopic resection of colorectal polyps. Endosc Int Open. 2015;3:252–257. doi: 10.1055/s-0034-1391853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Matsuda K, Watanabe H, Kuwabara S et al. Esophageal submucosal tumor (SMT)-like carcinoma [Japanese with English abstract] Stomach Intestine. 1997;32:671–689. [Google Scholar]