

Abstract
BACKGROUND:
Giant Bowen’s disease is a rare and unusual clinical manifestation. Presenting as extensive scaly erythematous patch or plaque, it gives rise to a wide spectrum of dermatological differential diagnoses.
CASE PRESENTATION:
We report a patient with giant Bowen’s disease on the face that was successfully treated with topical 5 % imiquimod. A review of the literature was made with the aim to analyse and compare the findings in it with our observation.
CONCLUSION:
We present this case to draw attention to the importance of the self skin examination in the elderly population. Also, to prevent development to invasive squamous cell carcinoma from Bowen’s disease, we recommend mandatory dermoscopic examination on every long-standing erythemosquamous lesion.
Keywords: Giant Bowen’s disease, dermoscopy, histopathology
Introduction
Bowen’s disease is considered an intraepidermal/in situ squamous cell carcinoma (SCC) as long as it has not spread beyond the basal membrane. Spreading into the dermis is a time-consuming process, and when it happens, it grows as an invasive SCC [1]. This precancerous nature of Bowen’s disease was first recognised by John Templeton Bowen in 1912 [2]. The risk of progression to invasive SCC is estimated to be 3-5 % for extragenital lesions and 10% for genital lesions [3]. Referring to these assertions, its potential lateral spreading through the epidermis is expected. By this gradual progress, with time, Bowen’s disease gets an unusual giant dimension.
Clinical presentation as a large erythemosqamous patch or plaque can be mistaken with various other dermatological differential diagnoses [4], [5].
Chronic UV irradiation exposure (solar, iatrogenic and sunbeds) is considered the most obvious trigger of Bowen’s disease. Etiological causes also inspected are age, genetic factors, arsenic exposure and other carcinogens, human papilloma viruses (HPV), immunosuppression, trauma, x-ray irradiation etc. [4].
We present a case with giant Bowen’s disease on the face, a sun-exposed area, an elderly patient. Our observation prompted us to consult the literature concerning this unusual presentation of Bowen’s disease and compare the published findings with ours.
Case Report
An 85-year-old female was referred to our department with a history of slowly enlarging scaly erythematous lesion on the left cheek, developed over the last two years. Completely asymptomatic, it has caused an only cosmetic disturbance. Patient has reported unprotected exposition to the sun 5-6 months per year, in the last 30 years. She declined previous cutaneous carcinomas of any kind. The attempts to treat it with topical corticosteroids and antimycotic creams did not reveal any results. After careful clinical and dermoscopic examination of the total skin, no other suspected lesions were noticed.
Dermatological status showed scaly, slightly elevated erythematous plaque with dimension 9 x 7.5 centimetres and well-demarcated borders from the surrounding healthy skin (Fig. 1).
Figure 1.

Large scaly erythematous plaque on the left cheek
Dermoscopic findings through the surface of the entire lesion showed glomerular or dotted vessels and yellow-white opaque scales on an erythematous background, suggestive for Bowen’s disease (Fig. 2).
Figure 2.
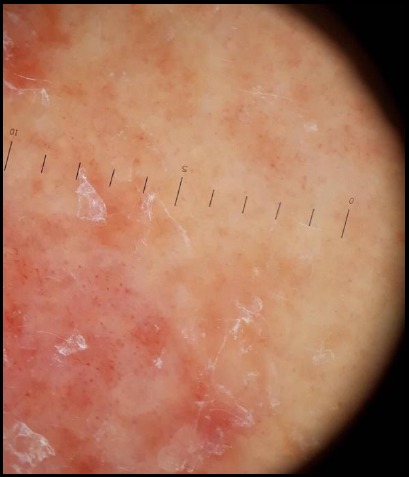
Dermoscopic findings: dotted vessels and yellow-white opaque scales on an erythematous background
Histopathological examination revealed parakeratosis in stratum corneum with atypia in cells throughout the epidermis. Individual dyskeratotic cells and increased mitotic figures were evident in the spinous layer. So, the diagnosis of Bowen’s disease was confirmed (Fig. 3).
Figure 3.
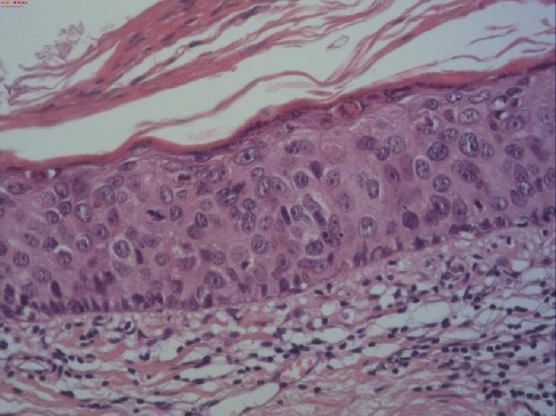
Histopathology, H&E: Parakeratosis in stratum corneum, atypia, pleomorphism, dyskeratotic cells and some mitotic figures in the epidermis
Treatment with 5% imiquimod cream was initiated 3 times weekly for 4 months. For the following 2 months, the application was reduced to 2 times per week. Impressive healing of the skin lesion was achieved [Fig.4. Ten months follow-up did not show recurrence of the lesion.
Figure 4.

Complete healing of the Bowen’s lesion after 6 months treatment with 5 % imiquimod
We aimed to review the literature and hence a Medline search was undertaken for the terms “Giant Bowen’s disease”, “Huge Bowen’s disease”, “Large Bowen’s disease” and “Extensive Bowen’s disease”. Additional articles were disclosed from the references given in the publications. All articles were methodically studied for the described clinical, dermoscopic and histopathological features. Clinical images and photomicrographs were reviewed and matched with those of our patient. All articles lacking any photomicrographs were excluded.
Table 1.
Data from the literature concerning giant Bowen’s disease, including our case
| Reference | Sex | Age | Localisation | Dimension | Course |
|---|---|---|---|---|---|
| Sotiriou E, et al.2011 [6] | Male | 79 | Right fronto-temporal area | 10 x 10 cm | 2 years |
| Park JY, et al. 2013 [7] | Male | 55 | Left Flank | 13 x 12 cm | ? |
| Female | 79 | Right breast | 21 x 14 cm | 40 years | |
| Bakardzhiev I, et al. 2015 [8] | Male | 56 | Above right flank | 26 x 22 cm | More than 15 years |
| Shankar AA, et al.2015 [9] | Male | 68 | Abdomen | 11 x 5 cm | 25 years |
| Baykal C, et al. 2016 [10] | Male | 67 | Abdomen | 15 x 15 cm | Since childhood |
| Akay BN, et al. 2016 [11] | Male | 44 | Abdomen | 32 x 25 cm | 10 years |
| Nagakeerthana S, et al. 2017 [12] | Male | 73 | Gluteal | 15 x 16 cm | 3 years |
| Ozlu E, et al. 2017 [13] | Male | 62 | Abdomen | 13 x 13 cm | 7 years |
| Caca-Biljanovska N, et al. 2019 [this paper] | Female | 85 | Left cheek | 9 x 7.5 cm | 2 years |
Discussion
Giant Bowen’s disease is rarely reported in the literature [8]. There is no consensus on an official definition of large, extensive or huge Bowen’s disease. Morton et al. made efforts in their study to define “large Bowen’s disease” as a lesion with a dimension more than 2 cm [14]. On the other hand, Lopez et al. used the term “extensive Bowen’s disease” for those lesions larger than 3 cm in diameter [15]. Our patient with 9 x 7.5 cm sized Bowen’s disease fulfilled the criteria proposed by Morton and Lopez [14], [15].
Although the clinical presentation can argue about plentiful of dermatological diseases, dermoscopic findings strongly suggestive for Bowen’s disease were recently defined [16]. Anyway, histopathology remains the ‘gold standard’ for an accurate diagnosis of Bowen’s disease [17].
The period for full expression of the Bowen’s lesion is variable, from 2 years to maximum 40 years, a finding which is strongly in favour of the slow, lateral spreading of Bowen’s disease.
Opposite to our patient, the most common position of giant Bowen’s disease in other published cases is the abdomen, followed by flanks. These are covered parts of the body, non- sun exposed. We could assume that this observation and the fact that most of the patients with giant Bowen’s disease are old males are the reasons for ignoring the lesion or delaying the dermatological consultation.
Only two of the patients from the literature, including our, have a lesion on the face, and both of them have the shortest history of 2 years duration of the disease. Upon that background, we can assume that cosmetically non-acceptance was the main motive to the patient to seek out dermatological help.
Asymptomatic as it is, the early lesions of Bowen’s disease are very subtle and overlap with clinical features seen in many other dermatological conditions (seborrheic keratosis, superficial basal cell carcinoma, actinic keratosis, eczema, tinea, psoriasis vulgaris, seborrhoeic dermatitis etc.) [5].
Although early dermatological consultation can be accessed by the patient, these clinically not specific changes of Bowen’s disease often mislead the dermatologist in making the correct diagnosis. Undiagnosed Bowen’s disease ultimately advances to invasive SCC [11].
Treatment modalities for Bowen’s disease are topical immunosuppressive/immunostimulating creams, cryotherapy, curettage, photodynamic therapy, radiotherapy, laser and finally surgical excision [18]. The therapeutic choice can be influenced by the age group, number, size and localisation of the lesion, preferable and comfortable solution by the patient and affordability of the therapeutic modalities [1].
In conclusion, the term “giant” is referred to clinical manifestation of the lesion, and it should not be used as a variant or distinctive form of Bowen’s disease. We suppose that giant manifestation of Bowen’s disease is due to neglecting the skin lesion by the patient, or not identifying it promptly by the dermatologist. Therefore, we strongly recommend self skin examination to be carried out, especially in older patients. Also, regular dermoscopy performed on every long-standing erythemosquamous skin lesion should be a rule. Early recognition of Bowen’s disease and prevention of its undeniable progression into an invasive SCC is very important.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
Reference
- 1.Bath-Hextall FJ, Matin RN, Wilkinson D, et al. Interventions for cutaneous Bowen's disease. Cochrane Database of Syst Rev. 2013;6:CD007281. doi: 10.1002/14651858.CD007281.pub2. https://doi.org/10.1002/14651858.CD007281.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bowen JT. Precancerous dermatosis:a study of two cases of chronic atypical epithelial proliferation. J Cutan Dis Syph. 1912:241–55. In:Arch Dermatol. 1983; 119(3):243-60. https://doi.org/10.1001/archderm.1983.01650270061020 PMid:6297414. [PubMed] [Google Scholar]
- 3.Kao GF. Carcinoma arising in Bowen's disease. Arch Dermatol. 1986;122:1124–1126. https://doi.org/10.1001/archderm.1986.01660220042010 PMid:3767398. [PubMed] [Google Scholar]
- 4.Kallini JR, Hamed N, Khachemoune A. Squamous cell carcinoma of the skin:epidemiology, classification, management, and novel trends. Int J Dermatol. 2015;54(2):130–40. doi: 10.1111/ijd.12553. https://doi.org/10.1111/ijd.12553 PMid:25428226. [DOI] [PubMed] [Google Scholar]
- 5.Wozniak Rito AM, Rudnicka L. Bowen's disease in dermoscopy. Acta Dermatovenerol Croat. 2018;26:157–161. https://doi.org./10.2340/00015555-1328 PMid:29989873. [PubMed] [Google Scholar]
- 6.Sotiriou E, Lallas A, Apalla Z, et al. Treatment of giant Bowen's disease with sequential use of photodynamic therapy and imiquimod cream. Photodermatology, Photoimmunology & Photomedicine. 2011;27:164–166. doi: 10.1111/j.1600-0781.2011.00586.x. https://doi.org/10.1111/j.1600-0781.2011.00586.x PMid:21535173. [DOI] [PubMed] [Google Scholar]
- 7.Park JY, Kim SK, Cho KH, et al. Huge Bowen's disease:A pitfall of topical photodynamic therapy. Photodiagnosis and Photodyn Ther. 2013;10(4):546–8. doi: 10.1016/j.pdpdt.2013.05.001. https://doi.org/10.1016/j.pdpdt.2013.05.001 PMid:24284109. [DOI] [PubMed] [Google Scholar]
- 8.Bakardzhiev I, Chokoeva AA, Tchernev G. Giant extragenital Bowen's disease. Wien Med Wochenschr. 2015;165(23-24):504–7. doi: 10.1007/s10354-015-0396-z. https://doi.org/10.1007/s10354-015-0396-z PMid:26542410. [DOI] [PubMed] [Google Scholar]
- 9.Shankar AA, Pinto M, Shenoy MM, et al. Giant pigmented Bowen's disease:A rare variant at a rare site. Indian Dermatol Online J. 2015;6:S63–4. doi: 10.4103/2229-5178.171048. https://doi.org/10.4103/2229-5178.171048 PMid:26904458 PMCid:PMC4738524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baykal C, Buyukbabani N, Babuna G, et al. Giant Bowen's disease histologically showing Borst- Jadassohn phenomenon and complicated with squamous cell carcinoma development. J Eur Acad Dermatol Venerol. 2016;30:88–89. doi: 10.1111/jdv.13335. https://doi.org/10.1111/jdv.13335 PMid:26373350. [DOI] [PubMed] [Google Scholar]
- 11.Akay BN, Maden A, Kocak O, et al. Development of poorly differentiated invasive squamous cell carcinoma in giant Bowen's disease:a case report with dermatoscopy. Dermatol Pract Concept. 2016;6(2):2. doi: 10.5826/dpc.0602a02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nagakeerthana S, Rajesh G, Madhavi S, et al. Bowen's disease:Two case reports of a giant and dwarf lesions. J Can Res Ther. 2017;13:371–3. doi: 10.4103/0973-1482.187237. https://doi.org/10.4103/0973-1482.187237 PMid:28643763. [DOI] [PubMed] [Google Scholar]
- 13.Ozlu E, Ertas R, Ozyurt K, et al. Giant neglected Bowen's disease lesion treated successfully with topical 5-fluorouracil. North Clin Istnb. 2017;10(4):77. doi: 10.14744/nci.2017.77598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Morton CA, Whithurst C, McColl J.H, et al. Photodynamic therapy for large or multiple patches of Bowen's disease and basal cell carcinoma. Arch Dermatol. 2001;137:319–324. PMid:11255332. [PubMed] [Google Scholar]
- 15.Lopez N, Meyer-Gonzales T, Herrera-Acosta E, et al. Photodynamic therapy in the treatment of extensive Bowen's disease. J Dermatol Treat. 2012;23:428–430. doi: 10.3109/09546634.2011.590789. https://doi.org/10.3109/09546634.2011.590789 PMid:21787214. [DOI] [PubMed] [Google Scholar]
- 16.Zalaudek I, Argenziano G, Leinweber B, et al. Dermoscopy of Bowen's disease. Br J Dermatol. 2004;150:1112–1116. doi: 10.1111/j.1365-2133.2004.05924.x. https://doi.org/10.1111/j.1365-2133.2004.05924.x PMid:15214896. [DOI] [PubMed] [Google Scholar]
- 17.Neagu TP, Tiglis M, Botezatu D, et al. Clinical, histological and therapeutic features of Bowen's disease. Rom J Morphol Embryol. 2017;58:33–40. PMid:28523295. [PubMed] [Google Scholar]
- 18.Morton CA, Birnie AJ, Eedy DJ. British Association of Dermatologists'guidelines for the management of squamous cell carcinoma in situ (Bowen's disease) 2014. British Journal of Dermatology. 2014;170:245–260. doi: 10.1111/bjd.12766. https://doi.org/10.1111/bjd.12766 PMid:24313974. [DOI] [PubMed] [Google Scholar]